
Abstract
Purpose
The credible data about the burden of early-onset colorectal cancer (EOCRC) in China when compared to other countries in the group of twenty (G20) remained unavailable. We aimed to assess the burden and trends of EOCRC and attributable risk factors in China. Meanwhile, the comparison in the burden and attributable risk factors between China and other G20 countries was also evaluated.
Methods
Data on the incidence, prevalence, mortality, disability-adjusted life years (DALYs), and attributable risk factors of EOCRC in China were obtained from Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019 and compared with other G20countries. Temporal trends of age-standardized rates for incidence, prevalence, mortality, and DALYs were evaluated by estimated annual percentage change (EAPC). The autoregressive integrated moving average (ARIMA) model was used to forecast the incidence, mortality, and DALY rates of EOCRC in China from 2020 to 2029.
Results
From 1990 to 2019, the age-standardized incidence rate (ASIR) and age-standardized prevalence rate (ASPR) of EOCRC in China increased with the EAPCs of 4.61 [95% confidence interval (CI): 4.45–4.77] and 5.82 (95% CI: 5.60–6.05). When compared to G20 countries, China was ranked 13th in the ASIR in 1990 and then increased to 2nd in 2019, second only to Japan. The ASPRs increased in all G20 countries, being highest in Saudi Arabia, followed by China and Mexico. Moreover, China had the highest age-standardized mortality rate and highest age-standardized DALY rate in 2019. In China, the five leading risk factors, for both sexes, were diet low in milk [18.54% (95% UI: 12.71–24.07)], diet low in calcium [15.06% (95% UI: 10.70–20.03)], alcohol use [12.16% (95% UI: 8.87–15.64)], smoking [9.08% (95% UI: 3.39–14.11)], and diet high in red meat [9.08% (95% UI: 3.39–14.11)] in 2019. Over the next 10 years, ASIR, ASMR, and age-standardized DALY rate of EOCRC will increase continuously in males and females.
Conclusion
The burden of EOCRC in China and other G20 countries is worrisome, indicating that coordinated efforts are needed to conduct high-quality researches, allocate medical resources, adjust screening guidelines, and develop effective treatment and prevention strategies in the G20 countries.
Similar content being viewed by others


Introduction
Globally, colorectal cancer (CRC) is one of the major reasons for the global burden of cancer, with more than 1.9 million new cases and 935,000 deaths in 2020 [1]. Overall, CRC ranks as the third most frequently diagnosed cancer and the second leading causes of cancer-associated deaths [1, 2]. In the past three decades, the age-standardized incidence and mortality rates of CRC either remained steady or declined in high Socio-demographic Index (SDI) countries such as the United States, Australia, and Germany [3]. However, large increases in the CRC incidence rates occurred in low and middle SDI countries [4]. It is noted that China has become the country with the largest number of new cases and deaths from CRC annually [5, 6]. The incidence rate of early-onset CRC (EOCRC) is increasing worldwide, which is defined as that diagnosed in individuals aged younger than 50 years. Up to 90% of all patients with newly diagnosed CRC are aged 50 years and over, namely, late-onset CRC (LOCRC), but EOCRC accounts for 10%-12% of CRC cases [7, 8]. A previous study revealed an increasing trend in the incidence of CRC in China from 1990 to 2016, with the most significant increase in the cases under the age of 50 [9]. Patients with EOCRC are prone to possess an underappreciation of symptoms, lack of awareness about CRC and early screening, have more reluctance to seek medical assistance, leading to delayed diagnosis and advanced stage at diagnosis [10]. In addition, EOCRC patients experienced significantly longer time to diagnosis and longer duration of symptoms compared to patients with LOCRC [10, 11]. Thus, EOCRC causes a large burden of disease among young adults.
It is reported that 70–75% of CRC cases are associated with modifiable risk factors such as smoking, alcohol use, high body-mass index, diet high in processed and red meat, whereas the remaining 25–30% of cases are related to non-modifiable risk factors including genetic factors, personal history of polyps or adenoma, or family history of CRC [4, 12]. The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019 has verified that 58.2% of cancer related-deaths and 57.6% of disability-adjusted life years (DALYs) due to CRC were approximately attributable to well recognized risk factors [13]. The reasons for the rapid increasing trends of EOCRC incidence and mortality are unclear, but they are likely to be affected a combination of modifiable and non-modifiable risk factors, such as excess body weight, lacking of physical activity, diabetes mellitus, male, black or Asian, family history of CRC, and personal history of inflammatory bowel disease [14,15,16]. However, whether known risk factors play similarly critical roles in EOCRC incidence is poorly understood. Also, identifying risk factors is essential to optimize guidelines for prevention and early detection for EOCRC.
The Group of 20 (G20), which is widely recognized as one of the largest international economic cooperation fora, accounts for almost two-thirds of the world’s population [17]. The burden of diseases among G20 countries are inextricably related to their economic environment and medical condition [18]. Previous studies have identified the burden of EOCRC varied across geographic locations and socioeconomic statuses [19, 20]. However, a comprehensive analysis regarding disease burden and long-term trends along with attributable risk factors of EOCRC in China and other member countries of G20 has not been available. A better understanding of the current status and future trends of disease burden can promote effective prevention and aid policy decision-makers to allocate health care resources precisely and efficiently. Therefore, in this study, we utilized data from the GBD 2019 to quantify the trends in incidence, prevalence, mortality, DALYs of EOCRC in China and compared these indicators to other G20 countries from 1990 to 2019, and the contributions of risk factors. We also predicted the burden up to 2029 in China.
Methods
Study design and data sources
This study was designed as a secondary analysis of publicly available anonymized aggregate data from the GBD 2019, which comprehensively assessed the burden of 369 diseases and injuries, and 87 behavioral, environmental and occupational, and metabolic risk factors in 204 countries and territories from 1990 to 2019. The GBD 2019 was considered as a standardized framework for integrating, validating, analyzing, and disseminating the disease burden and for evaluating the burden of premature death, health loss, and disability due to disease, injury, and risk factors in diverse populations [21]. Data assembled in the GBD 2019 were derived from multiple sources, including the published literature reviews, cohort studies, cross-sectional studies, case reports, Global Health Databases, vital registration databases, sample registration systems, household surveys, censuses and health and demographic surveillance websites [21, 22]. The DisMod-MR 2.1, a Bayesian meta-regression tool, was used to pool the incidence and mortality data and generate location-year-age-sex-specific estimates in GBD 2019 [21]. More details about the methodology of GBD 2019 have been previously described [21, 22]. Herein, we obtained and analyzed the data on incidence, prevalence, mortality, DALYs, and related risk factors of EOCRC in China during 1990–2019, stratified by sex. In addition, we compared EOCRC estimates with other member countries of the G20 (an international forum for the governments from 20 major economies including Argentina, Australia, Brazil, Canada, European Union, France, Germany, India, Indonesia, Italy, Japan, Mexico, Republic of Korea, Russian Federation, Saudi Arabia, South Africa, Turkey, United Kingdom, and United States of America), and the European Union is considered as a whole in this analysis. DALYs are regarded as summary indicators to measure the disease burden due to disability and premature death in the GBD study [21]. DALYs are calculated as the sum of the YLLs and YLDs, and one DALY is comparable to one lost year of healthy life.The Global Health Data Exchange (GHDx) query tool (http://ghdx.healthdata.org/) was used to collect the data analyzed in this study. Our study followed the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) to ensure the transparency, reliability and replicability [23].
Definition of EOCRC
We regarded all cases coded C18-C21, D01.0-D01.2, and D12-D12.8 as CRC according to the 10th revision of International Classification of Diseases [4]. EOCRC were defined as CRC cases diagnosed at an age of 50 years or younger.
Risk factors
Disease burden attributable to each risk factor was estimated according to the comparative risk assessment framework in the GBD 2019. Ten risk factors that have a non-zero contribution to deaths and DALYs of CRC were selected, including five dietary factors (diet high in processed meat, diet high in red meat, diet low in calcium, diet low in fiber, and diet low in milk), three behavioral factors (alcohol use, smoking, and low physical activity), and two metabolic factors (high body-mass index and high fasting plasma glucose) [4]. Detailed definitions of these risk factors and methods for quantifying the proportions of the burden of EOCRC attributable to these risk factors have been described previously [22]. The percentage contribution of these ten risk factors to the DALYs of EOCRC in 2019 were assessed in this study.
Statistical analysis
The quantity of incidence, prevalence, mortality, and DALYs mainly covers the number, percent, and rate. The 95% uncertainty intervals (UIs) were demonstrated for each estimated quantity. Each estimate such as incident cases and age-standardized incidence rate in GBD study was calculated 1,000 times, with each time sampling from distributions for data inputs, data transformations, and model choice. The 95% UIs were determined by the 25th and 975th values of the 1,000 values after ordering them from smallest to largest [21]. Age-standardized rates for incidence, prevalence, mortality, and DALYs were computed by employing direct standardization to the World Health Organization (WHO) world standard population age-structure from 2000 to 2025 [24]. We calculated the estimated annual percentage change (EAPC) in the age-standardized rates for incidence, prevalence, mortality, and DALYs to assess the temporal trends in the burden of EOCRC during 1990–2019. EAPC was a widely accepted measure to quantificationally describe the trend of age-standardized rates over specific time intervals, and it was calculated based on the regression model fitted to the natural logarithm of the rates. The regression model was defined as: ln (rate) = α + β × (calendar year) + ε, and EAPC was calculated as 100 × (exp(β)-1). The 95% confidence interval (CI) was also determined by the linear regression model. When EAPC and the lower limit of 95% CI are positive, that age-standardized rate is considered to be in an increasing trend. Conversely, if EAPC and the upper limit of 95% CI are less than 0, the age-standardized rate shows a descending trend. The autoregressive integrated moving average (ARIMA) (p, d, q) model was selected to forecast the incidence, mortality, and DALY rates of EOCRC from 2020 to 2029. The letters p, d, q represented the orders of autoregression, degree of difference, and order of moving average, respectively. More details about ARIMA model were provided elsewhere [25, 26]. We constructed this model in the following steps: stationary test, model identification, parameter estimation, model diagnosis, and model prediction. The Augmented Dickey–Fuller (ADF) test is used to determine whether the series is stationary or not. If the rates were not stationary series, logarithmic transformation was performed to transform them into stationary series. The autocorrelation function (ACF) and the partial autocorrelation function (PACF) were used to determine the appropriate model parameters (p and q). The optimal ARIMA (p, d, q) model was evaluated by the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). We used the Ljung–Box Q test, ACF, and PACF of residuals to judge whether the residuals of the optimal model meet the requirements of white noise sequences. Then, the model was constructed and used to forecast the rates. All statistical analyses and graphics were performed by software package R version 4.1.1. P < 0.05 was considered statistically significant.
Results
Disease burden of EOCRC in China
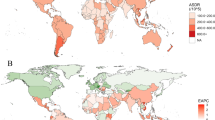
In China, there were 23,971 (95% UI: 20,744–27,552) incident cases of EOCRC in 1990 and 87,383 (95% UI: 72,880–103,288) cases in 2019, representing an increase of 264.54% from 1990 to 2019. Meanwhile, the global incident cases of EOCRC were 225,736 (95% UI: 207,658–246,756) in 2019, increasing from 94,707 (95% UI: 90,421–99,416) in 1990. The age-standardized incidence rates (ASIRs) of EOCRC in China were 3.59 (95% UI: 3.10–4.12) in 1990 and 12.12 (95% UI: 10.11–14.33) in 2019 per 100,000 population, which were higher than the global average of 3.49 (95% UI: 3.33–3.67) in 1990 and 5.74 (95% UI: 5.28–6.27) in 2019 per 100,000 population. When compared to G20 countries, China was ranked 13th in the ASIR in 1990 and then increased to 2nd in 2019, second only to Japan (Table 1). EOCRC accounted for 121,016 (95% UI: 105,534–138,358) prevalent cases in 1990 and 590,804 (95% UI: 494,021–697,827) cases in 2019 in China, comprising 23.08% of global prevalent cases in 1990 and 41.57% in 2019. Age-standardized prevalence rate (ASPR) of EOCRC in China jumped from the 13th in 1990 to the 3rd in 2019 (Table 2). It is worthwhile to point out China had the highest number of deaths caused by EOCRC in 1990 [14,851 (95% UI: 12,694–17,187)] and 2019 [26,274 (95% UI: 21,892–31,077)] among the G20 countries. Moreover, China had the highest age-standardized mortality rate (ASMR) [3.65 (95% UI: 3.04–4.31)] per 100,000 population in 2019 (Table 3). Worldwide, approximately 2.52 (95% UI: 2.37–2.66) million and 4.26 (95% UI: 3.94–4.59) million DALYs due to EOCRC were reported in 1990 and 2019, with more than 30% of global DALYs coming from China. Japan was the country with the highest age-standardized DALY rate [166.53 (95% UI: 162.97–169.95)] per 100,000 population in 1990, and China had the highest age-standardized DALY rate [181.04 (95% UI: 152.57–211.83)] per 100,000 population in 2019 (Table 4).
Temporal trends in EOCRC burden over time
With the exception of the Germany and South Africa, the ASIRs for EOCRC in all the other G20 member countries increased during 1990–2019. In China, the ASIR for EOCRC presented an increasing trend with an EAPC being 4.61 (95% CI: 4.45–4.77) (Table 1). The ASPRs increased in all G20 countries, being highest in Saudi Arabia (EAPC = 5.90, 95% CI: 5.67–6.14), followed by China (EAPC = 5.82, 95% CI: 5.60–6.05) and Mexico (EAPC = 4.04, 95% CI: 3.91–4.17) (Table 2). In terms of ASMRs for EOCRC during 1990–2019, China, Argentina, Brazil, India, Indonesia, Mexico, Saudi Arabia, and United States of America had upward trends, whereas the descending trends were observed in Australia, European Union, France, Italy, Japan, South Africa, Turkey, and United Kingdom. Meanwhile, the ASMRs in Canada, Germany, Republic of Korea, and Russian Federation remained stable (Table 3). The age-standardized DALY rate of EOCRC in China increased (EAPC = 1.64, 95% CI: 1.54–1.75), moreover, China’s upward trend ranked 4th in the G20 countries, followed by Mexico, Saudi Arabia, and Indonesia (Table 4).
Risk factors for DALYs of EOCRC in China
Although the DALYs of EOCRC in China was attributed to different individual risk factors, the five major risk factors in 2019 were diet low in milk [18.54% (95% UI: 12.71–24.07)], diet low in calcium [15.06% (95% UI: 10.70–20.03)], alcohol use [12.16% (95% UI: 8.87–15.64)], smoking [9.08% (95% UI: 3.39–14.11)], and diet high in red meat [9.08% (95% UI: 3.39–14.11)] (Fig. 1). The proportions of DALYs attributable to risk factors differed by sex and country. The five most common risk factors for males were diet low in milk, alcohol use, diet low in calcium, smoking, and high body-mass index, whereas diet low in milk, diet low in calcium, diet high in red meat, high body-mass index, and high fasting plasma glucose were the five risk factors that contributed most to DALYs in females (Figs. S1 and S2). At the national level, the highest percentage of DALYs for alcohol use was in Germany [19.55% (95% UI: 14.93–24.34)], for diet high in processed meat was in United States of America [7.76% (95% UI: 2.90–13.38)], for diet high in red meat was in Australia [12.77% (95% UI: 6.34–18.92)], for diet low in calcium was in Indonesia [24.29% (95% UI: 19.73–29.01)], for diet low in fiber was in Republic of Korea [4.41% (95% UI: 1.74–7.36)], for diet low in milk was in India [19.17% (95% UI: 13.68–24.61)], for high body-mass index was in Saudi Arabia [17.31% (95% UI: 10.89–23.84)], for high fasting plasma glucose was in United Kingdom [5.13% (95% UI: 1.14–11.50)], for low physical activity was in Saudi Arabia [11.49% (95% UI: 3.71–19.37)], and for smoking was in United Kingdom [12.73% (95% UI: 4.65–19.60)] (Fig. 1).

The proportion of DALYs due to EOCRC attributable to risk factors in China and other G20 countries in 2019. DALYs: Disability-adjusted life years; EOCRC: Early-onset colorectal cancer; G20: Group of 20
Predictions of incidence, mortality and DALYs of EOCRC in China from 2020 to 2029
We used the ARIMA model to fit the ASIR, ASMR, and age-standardized DALY rate of EOCRC stratified by sex, from 1990 to 2019 and predict them in 2029. The selected optimal model parameters and corresponding AIC and BIC were presented in the Table S1. By 2029, the ASIR in males will increase to 21.91 (95% CI: 16.18–27.64) per 100,000 population with an EAPC of 2.63 (95% CI: 2.47–2.79) (Table 5, Fig. 2A). The ASIR in females will reach 8.23 (95% CI: 7.14–9.32) per 100,000 population, which means a slight increase with an EAPC of 0.95 (95% CI: 0.76–1.15) (Table 5, Fig. 2B). Men are anticipated to have a steeper increase than women in the ASMR during 2020–2029, with EAPCs of 1.73 (95% CI: 1.70–1.76) and 1.45 (95% CI: 1.42–1.49), respectively (Table 5, Fig. 2C, D). Meanwhile, the increasing speed of rise in the age-standardized DALY rate in males with an EAPC of 1.92 (95% CI: 1.89–1.96) will be higher than in females with an EAPC of 0.51 (95% CI: 0.41–0.61) (Table 5, Fig. 2E, F).

The temporal trends in the age-standardized rates for incidence, mortality, and DALY of EOCRC from 1990 to 2019 and projections from 2020 to 2029 in China, stratified by gender. A The temporal trends in the age-standardized incidence rate of EOCRC from 1990 to 2019 and projections from 2020 to 2029 in males. B The temporal trends in the age-standardized incidence rate of EOCRC from 1990 to 2019 and projections from 2020 to 2029 in females. C The temporal trends in the age-standardized mortality rate of EOCRC from 1990 to 2019 and projections from 2020 to 2029 in males. D The temporal trends in the age-standardized mortality rate of EOCRC from 1990 to 2019 and projections from 2020 to 2029 in females. E The temporal trends in the age-standardized DALY rate of EOCRC from 1990 to 2019 and projections from 2020 to 2029 in males. F The temporal trends in the age-standardized DALY rate of EOCRC from 1990 to 2019 and projections from 2020 to 2029 in females. DALYs: Disability-adjusted life years; EOCRC: Early-onset colorectal cancer
Discussion
The present study provided the up-to-date estimates on incidence, prevalence, mortality, DALYs, and leading risk factors associated with EOCRC in China and compared these rates to other G20 countries over a 30-year period during 1990–2019, while utilizing data collected from the GBD 2019. The G20 is an international economic cooperation forum composed of 20 developed and developing countries. Similar to people in other countries around the world, the burden of diseases in G20 countries is inseparable from their specific economic circumstances and health conditions [27, 28]. It is estimated that 71% of the world’s elderly live in G20 countries, and most G20 member countries have experienced the high level of mortality attributed to non-communicable diseases including EOCRC. Thus, G20 countries should play a crucial role in helping to improve global health due to member countries have been confronted with many issues associated with aging society and increased burden of non-communicable diseases.
We observed that the increase in ASIR and ASPR over the past 30 years occurred in most G20 countries, which was consistent with previous studies [29,30,31]. In China, the incidence, prevalence, mortality, and DALYs of EOCRC have been on the rise from 1990 to 2019. Indeed, the estimated number of incident and prevalent EOCRC cases was 87,383 and 590,804 in 2019, which accounted for 38.71% and 41.57% of all EOCRC cases globally. Compared with the global average levels and other members of the G20 countries, the ASIR and ASPR of EOCRC increased significantly with EAPCs of 4.61 (95% CI: 4.45 to 4.77) and 5.82 (95% CI: 5.60 to 6.05) in China during the study period. The reasons underlying this rise of EOCRC are unclear. One possible hypothesis is that early-life exposure to established CRC risk factors including westernized diet, high body-mass index, and physical inactivity might result in genetic and epigenetic changes in colorectal epithelial cells, gut microbiota, and host immunity [10]. Although the role of genetic factors in the pathogenesis of EOCRC is more evident than that of LOCRC, most EOCRC patients are still sporadic [32]. Our findings indicated that proportions of EOCRC DALYs attributable to dietary, behavioral, and metabolic risk factors in China were 76.25% in 2019 (Fig. 1), while attributable risk proportions of dietary, behavioral, and metabolic factors in males were higher than those in females (86.27% vs. 52.58%) (Figs. S1 & S2). Therefore, the increase in incidence rate is mainly due to the increased exposure of risk factors. We further found that diet low in milk and diet low in calcium were the top two risk factors for EOCRC in 2019. High dietary milk and calcium intakes were reported to be associated with the reduced risk of CRC and EOCRC, possibly due to vitamin D and calcium may activate signaling pathways that are involved in regulating the inhibition of epithelial cell proliferation, induction of target tissue differentiation, regulation of antioxidant enzyme gene expression, and induction of carcinoma cell apoptosis via calcium-sensing receptor through promoting of E-cadherin expression, suppressing of β-catenin/T cell factor activation, and activating of p38 mitogen-activated protein kinase cascade [33,34,35]. Alcohol use and smoking contributed considerably to the burden of EOCRC. Many epidemiologic investigations have identified that alcohol use and smoking are associated with increased risks of EOCRC in a dose-dependent manner [36,37,38]. Ethanol and related metabolites initiate multiple signaling cascades augmenting the cancer progression, such as DNA-adduct formation, oxidative stress and lipid peroxidation, epigenetic alterations, epithelial barrier dysfunction, and immune modulatory effects [39]. Moreover, smoking promotes colon carcinogenesis possibly through impairing the phagocytic function of macrophages and augmenting the function of M2-like macrophages, which were associated with worse cancer-specific survival of CRC [40, 41]. A positive association between diet high in red meat and alkylating signatures was found in the distal colorectum. These alkylating signatures targeted cancer driver mutations KRAS p.G12D, KRAS p.G13D, and PIK3CA p.E545K, as well as predicted poor survival in CRC patients [42]. Additionally, changes in lifestyle and dietary habits such as high sugar-sweetened beverage consumption in adolescence and young adulthood are also associated with increased risk of EOCRC [10, 43].
From 1990 to 2019, the trends of age-standardized DALY rates for EOCRC showed patterns similar to those of ASMRs in the G20 countries. In contrast to the increasing trends of ASIR and ASPR in most G20 countries, ASMR and age-standardized DALY rate due to EOCRC declined or increased at a relatively low pace. This was consistent with a recent study, which revealed that mortality rates of EOCRC showed a downward trend in the high SDI countries, particularly in Australia, France, Germany, Japan, and the United Kingdom [19]. The amelioration in ASMR is possibly attributed to the continuous progression of early screening and efficient treatment approaches for CRC, coupled with the popularization of multidisciplinary comprehensive treatment concepts, including surgery, radiotherapy, chemotherapy, targeted therapy, and immunotherapy [44]. Although EOCRC patients were associated with a higher risk of malignancy and late staging compared to the LOCRC, EOCRC patients had fewer complications and higher tolerance and acceptance of cancer therapy, which was also beneficial for improving the treatment effectiveness and survival [45]. In most countries, early screening for CRC is currently performed in individuals over 50 years old. However, due to the rising incidence of EOCRC, some expert panels such as US Preventive Services Task Force recommended to lower the screening initiation age to 45 years [46, 47]. China has initiated some population-based CRC screening programs, such as a large-scale screening for high-risk populations in Haining County in the 1970s and the Cancer Screening Program in Urban China (CanSPUC) in 2012, which effectively inhibit the substantial increase of mortality of CRC in China [48]. However, according to the forecast results of ARIMA model, the ASIR, ASMR, and age-standardized DALY rate of EOCRC will still increase over the next 10 years in China. Moreover, men will experience higher ASIR, ASMR, and age-standardized DALY rate and have more significantly increasing trends of the rates compared with women. Thus, promising approaches to optimize prevention and early detection of EOCRC including the screening of high-risk populations such as young adults with family history of CRC in first-degree relatives should be emphasized.
Several limitations should be acknowledged in the present study. First, the data provided in GBD 2019 were based on estimation and mathematical modelling, which may affect the accuracy and reliability of the burden estimates. Second, due to detailed data about burden and trends of EOCRC stratified by histological subtype were not available, we were unable to assess the burden of colon cancer and rectal cancer respectively. Third, some potential risk factors of EOCRC such as antibiotic usage and changes in the gut microbiome were not analyzed due to the limitations of relevant data sources. Fourth, the absence of provincial-level data regarding the burden of EOCRC may not reflect the regional and provincial disparities of disease burden in China.
Conclusion
The present study carried out a comprehensive and in-depth analysis regarding the burden and long-term trend of EOCRC in China and other G20 countries. The ASIR, ASPR, ASMR, and age-standardized DALY rate of EOCRC increased from 1990 to 2019 in China. There were substantial differences in these rates among G20 countries. Diet low in milk, diet low in calcium, alcohol use, smoking, and diet high in red meat were the five leading risk factors for DALYs of EOCRC in 2019, which should be paid more attention to. The burden of EOCRC is predicted to increase continuously over the next 10 years in China. The huge burden of EOCRC calls for close collaboration and cooperation amongst G20 countries to implement interventions for improving early detection, optimizing early-stage diagnosis, and developing effective treatment and prevention strategies to reduce the burden of EOCRC.
Availability of data and materials
Publicly available datasets were analyzed in this study. The data can be found here: http://ghdx.healthdata.org/gbd-results-tool.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Song M. Global epidemiology and prevention of colorectal cancer. Lancet Gastroenterol Hepatol. 2022;7(7):588–90.
Morgan E, Arnold M, Gini A, Lorenzoni V, Cabasag CJ, Laversanne M, Vignat J, Ferlay J, Murphy N, Bray F. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut. 2023;72(2):338–44.
GBD 2019 Colorectal Cancer Collaborators. Global, regional, and national burden of colorectal cancer and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol Hepatol. 2022;7(7):627–47.
Li N, Lu B, Luo C, Cai J, Lu M, Zhang Y, Chen H, Dai M. Incidence, mortality, survival, risk factor and screening of colorectal cancer: a comparison among China, Europe, and northern America. Cancer Lett. 2021;522:255–68.
Wang W, Yin P, Liu YN, Liu JM, Wang LJ, Qi JL, You JL, Lin L, Meng SD, Wang FX, et al. Mortality and years of life lost of colorectal cancer in China, 2005–2020: findings from the national mortality surveillance system. Chin Med J (Engl). 2021;134(16):1933–40.
Siegel RL, Miller KD, Goding Sauer A, Fedewa SA, Butterly LF, Anderson JC, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70(3):145–64.
Burnett-Hartman AN, Lee JK, Demb J, Gupta S. An update on the epidemiology, molecular characterization, diagnosis, and screening strategies for early-onset colorectal cancer. Gastroenterology. 2021;160(4):1041–9.
Zhang L, Cao F, Zhang G, Shi L, Chen S, Zhang Z, Zhi W, Ma T. Trends in and predictions of colorectal cancer incidence and mortality in China from 1990 to 2025. Front Oncol. 2019;9:98.
Akimoto N, Ugai T, Zhong R, Hamada T, Fujiyoshi K, Giannakis M, Wu K, Cao Y, Ng K, Ogino S. Rising incidence of early-onset colorectal cancer - a call to action. Nat Rev Clin Oncol. 2021;18(4):230–43.
Willauer AN, Liu Y, Pereira AAL, Lam M, Morris JS, Raghav KPS, Morris VK, Menter D, Broaddus R, Meric-Bernstam F, et al. Clinical and molecular characterization of early-onset colorectal cancer. Cancer. 2019;125(12):2002–10.
Li Q, Wu H, Cao M, Li H, He S, Yang F, Yan X, Zhang S, Teng Y, Xia C, et al. Colorectal cancer burden, trends and risk factors in China: a review and comparison with the United States. Chin J Cancer Res. 2022;34(5):483–95.
GBD 2019 Cancer Risk Factors Collaborators. The global burden of cancer attributable to risk factors, 2010–19: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2022;400(10352):563–91.
Islami F, Goding Sauer A, Miller KD, Siegel RL, Fedewa SA, Jacobs EJ, McCullough ML, Patel AV, Ma J, Soerjomataram I, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin. 2018;68(1):31–54.
Low EE, Demb J, Liu L, Earles A, Bustamante R, Williams CD, Provenzale D, Kaltenbach T, Gawron AJ, Martinez ME, et al. Risk factors for early-onset colorectal cancer. Gastroenterology. 2020;159(2):492-501.e7.
Gausman V, Dornblaser D, Anand S, Hayes RB, O’Connell K, Du M, Liang PS. Risk factors associated with early-onset colorectal cancer. Clin Gastroenterol Hepatol. 2020;18(12):2752-2759.e2.
Dente MG, Riccardo F, Declich S, Milano A, Robbiati C, Agrimi U, Mantovani A, Morabito S, Scavia G, Cubadda F, et al. Strengthening preparedness against global health threats: a paradigm shift based on One Health approaches. One Health. 2022;14:100396.
McBride B, Hawkes S, Buse K. Soft power and global health: the sustainable development goals (SDGs) era health agendas of the G7, G20 and BRICS. BMC Public Health. 2019;19(1):815.
Gu WJ, Pei JP, Lyu J, Akimoto N, Haruki K, Ogino S, Zhang CD. The burden of early-onset colorectal cancer and its risk factors from 1990 to 2019: a systematic analysis for the global burden of disease study 2019. Cancers (Basel). 2022;14(14):3502.
Shao B, Zhu M, Shen K, Luo L, Du P, Li J, Xu J, Deng Y, Lin N, Wu J, et al. Disease burden of total and early-onset colorectal cancer in China from 1990 to 2019 and predictions of cancer incidence and mortality. Clin Epidemiol. 2023;15:151–63.
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–22.
GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1223–49.
Stevens GA, Alkema L, Black RE, Boerma JT, Collins GS, Ezzati M, Grove JT, Hogan DR, Hogan MC, Horton R, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. PLoS Med. 2016;13(6):e1002056.
Bilal U, Hessel P, Perez-Ferrer C, Michael YL, Alfaro T, Tenorio-Mucha J, Friche AAL, Pina MF, Vives A, Quick H, et al. Life expectancy and mortality in 363 cities of Latin America. Nat Med. 2021;27(3):463–70.
Wei J, Chen L, Huang S, Li Y, Zheng J, Cheng Z, Xie Z. Time trends in the incidence of spinal pain in China, 1990 to 2019 and its prediction to 2030: the global burden of disease study 2019. Pain Ther. 2022;11(4):1245–66.
Wu Y, Xia F, Chen M, Zhang S, Yang Z, Gong Z, Zhou X, Chen L, Wang T. Disease burden and attributable risk factors of neonatal disorders and their specific causes in China from 1990 to 2019 and its prediction to 2024. BMC Public Health. 2023;23(1):122.
Liu M, Gan H, Lin Y, Lin R, Xue M, Zhang T, Cheng ZJ, Sun B. Prevalence and disability-adjusted life year rates of asthma in China: findings from the GBD study 2019 of the G20. Int J Environ Res Public Health. 2022;19(22):14663.
Akashi H, Ishizuka A, Lee S, Irie M, Oketani H, Akashi R. The role of the G20 economies in global health. Glob Health Med. 2019;1(1):11–5.
Siegel RL, Torre LA, Soerjomataram I, Hayes RB, Bray F, Weber TK, Jemal A. Global patterns and trends in colorectal cancer incidence in young adults. Gut. 2019;68(12):2179–85.
Vuik FE, Nieuwenburg SA, Bardou M, Lansdorp-Vogelaar I, Dinis-Ribeiro M, Bento MJ, Zadnik V, Pellisé M, Esteban L, Kaminski MF, et al. Increasing incidence of colorectal cancer in young adults in Europe over the last 25 years. Gut. 2019;68(10):1820–6.
Pan H, Zhao Z, Deng Y, Zheng Z, Huang Y, Huang S, Chi P. The global, regional, and national early-onset colorectal cancer burden and trends from 1990 to 2019: results from the Global Burden of Disease Study 2019. BMC Public Health. 2022;22(1):1896.
Hofseth LJ, Hebert JR, Chanda A, Chen H, Love BL, Pena MM, Murphy EA, Sajish M, Sheth A, Buckhaults PJ, et al. Early-onset colorectal cancer: initial clues and current views. Nat Rev Gastroenterol Hepatol. 2020;17(6):352–64.
Zhang X, Fang YJ, Feng XL, Abulimiti A, Huang CY, Luo H, Zhang NQ, Chen YM, Zhang CX. Higher intakes of dietary vitamin D, calcium and dairy products are inversely associated with the risk of colorectal cancer: a case-control study in China. Br J Nutr. 2020;123(6):699–711.
Yang W, Liu L, Masugi Y, Qian ZR, Nishihara R, Keum N, Wu K, Smith-Warner S, Ma Y, Nowak JA, et al. Calcium intake and risk of colorectal cancer according to expression status of calcium-sensing receptor (CASR). Gut. 2018;67(8):1475–83.
Chang VC, Cotterchio M, De P, Tinmouth J. Risk factors for early-onset colorectal cancer: a population-based case-control study in Ontario, Canada. Cancer Causes Control. 2021;32(10):1063–83.
Kim NH, Jung YS, Yang HJ, Park SK, Park JH, Park DI, Sohn CI. Prevalence of and risk factors for colorectal neoplasia in asymptomatic young adults (20–39 years old). Clin Gastroenterol Hepatol. 2019;17(1):115–22.
O’Sullivan DE, Sutherland RL, Town S, Chow K, Fan J, Forbes N, Heitman SJ, Hilsden RJ, Brenner DR. Risk factors for early-onset colorectal cancer: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022;20(6):1229-1240.e5.
Puzzono M, Mannucci A, Grannò S, Zuppardo RA, Galli A, Danese S, Cavestro GM. The role of diet and lifestyle in early-onset colorectal cancer: a systematic review. Cancers (Basel). 2021;13(23):5933.
Rossi M, Jahanzaib Anwar M, Usman A, Keshavarzian A, Bishehsari F. Colorectal cancer and alcohol consumption-populations to molecules. Cancers (Basel). 2018;10(2):38.
Ugai T, Väyrynen JP, Haruki K, Akimoto N, Lau MC, Zhong R, Kishikawa J, Väyrynen SA, Zhao M, Fujiyoshi K, et al. Smoking and incidence of colorectal cancer subclassified by tumor-associated macrophage infiltrates. J Natl Cancer Inst. 2022;114(1):68–77.
Väyrynen JP, Haruki K, Lau MC, Väyrynen SA, Zhong R, Dias Costa A, Borowsky J, Zhao M, Fujiyoshi K, Arima K, et al. The prognostic role of macrophage polarization in the colorectal cancer microenvironment. Cancer Immunol Res. 2021;9(1):8–19.
Gurjao C, Zhong R, Haruki K, Li YY, Spurr LF, Lee-Six H, Reardon B, Ugai T, Zhang X, Cherniack AD, et al. Discovery and features of an alkylating signature in colorectal cancer. Cancer Discov. 2021;11(10):2446–55.
Hur J, Otegbeye E, Joh HK, Nimptsch K, Ng K, Ogino S, Meyerhardt JA, Chan AT, Willett WC, Wu K, et al. Sugar-sweetened beverage intake in adulthood and adolescence and risk of early-onset colorectal cancer among women. Gut. 2021;70(12):2330–6.
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394(10207):1467–80.
Manjelievskaia J, Brown D, McGlynn KA, Anderson W, Shriver CD, Zhu K. Chemotherapy use and survival among young and middle-aged patients with colon cancer. JAMA Surg. 2017;152(5):452–9.
Shaukat A, Levin TR. Current and future colorectal cancer screening strategies. Nat Rev Gastroenterol Hepatol. 2022;19(8):521–31.
Ladabaum U, Mannalithara A, Meester RGS, Gupta S, Schoen RE. Cost-effectiveness and national effects of initiating colorectal cancer screening for average-risk persons at age 45 years instead of 50 years. Gastroenterology. 2019;157(1):137–48.
Chen H, Li N, Ren J, Feng X, Lyu Z, Wei L, Li X, Guo L, Zheng Z, Zou S, et al. Participation and yield of a population-based colorectal cancer screening programme in China. Gut. 2019;68(8):1450–7.
Acknowledgements
The authors appreciate the works by the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019 collaborators.
Funding
The study was supported by the Tai’an Science and Technology Innovation Development Project (Grant No. 2021NS335, 2021ZC524). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
QL and HY conceived of and designed the project. QL, MY, and HL collected the data. LZ and YD analyzed and interpreted the data. QL drafted the manuscript. HY revised of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval and consent to participate The Second Hospital affiliated to Shandong University Institutional Review Board determined that the study did not require ethics approval and consent to participate because it used publicly available data.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
The proportion of DALYs due to EOCRC attributable to risk factors in China and other G20 countries in males in 2019. DALYs: Disability-adjusted life years; EOCRC: Early-onset colorectal cancer; G20: Group of 20.
Additional file 2: Figure S2.
The proportion of DALYs due to EOCRC attributable to risk factors in China and other G20 countries in females in 2019. DALYs: Disability-adjusted life years; EOCRC: Early-onset colorectal cancer; G20: Group of 20.
Additional file 3: Table S1.
ARIMA model parameters and their corresponding AIC and BIC for prediction of age-standardized rate (per 100 000) of all three measures for early-onset colorectal cancer for the next 10 years in China.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, Q., Yu, M., Lv, H. et al. Burden of early-onset colorectal cancer along with attributable risk factors from 1990 to 2019: a comparative study between China and other G20 countries. BMC Public Health 23, 1463 (2023). https://doi.org/10.1186/s12889-023-16407-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16407-y