
Abstract
Background
The mortality risk following COVID-19 diagnosis in men and women with common comorbidities at different ages has been difficult to communicate to the general public. The purpose of this study was to determine the age at which unvaccinated men and women with common comorbidities have a mortality risk which exceeds that of 75- and 65-year-old individuals in the general population (Phases 1b/1c thresholds of the Centre for Disease Control Vaccine Rollout Recommendations) following COVID-19 infection during the first wave.
Methods
We conducted a population-based retrospective cohort study using linked administrative datasets in Ontario, Canada. We identified all community-dwelling adults diagnosed with COVID-19 between January 1 and October 31st, 2020. Exposures of interest were age (modelled using restricted cubic splines) and the following conditions: major cardiovascular disease (recent myocardial infarction or lifetime history of heart failure); 2) diabetes; 3) hypertension; 4) recent cancer; 5) chronic obstructive pulmonary disease; 6) Stages 4/5 chronic kidney disease (CKD); 7) frailty. Logistic regression in the full cohort was used to estimate the risk of 30-day mortality for 75- and 65-year-old individuals. Analyses were repeated after stratifying by sex and medical condition to determine the age at which 30-day morality risk in strata exceed that of the general population at ages 65 and 75 years.
Results
We studied 52,429 individuals (median age 42 years; 52.5% women) of whom 417 (0.8%) died within 30 days. The 30-day mortality risk increased with age, male sex, and comorbidities. The 65- and 75-year-old mortality risks in the general population were exceeded at the youngest age by people with CKD, cancer, and frailty. Conversely, women aged < 65 years who had diabetes or hypertension did not have higher mortality than 65-year-olds in the general population. Most people with medical conditions (except for Stage 4–5 CKD) aged < 45 years had lower predicted mortality than the general population at age 65 years.
Conclusion
The mortality risk in COVID-19 increases with age and comorbidity but the prognostic implications varied by sex and condition. These observations can support communication efforts and inform vaccine rollout in jurisdictions with limited vaccine supplies.
Similar content being viewed by others

Background
It has been well-established that older age, male sex, and the presence of comorbidities are associated with higher mortality risks following diagnosis with the coronavirus disease of 2019 (COVID-19) [1,2,3,4,5,6,7,8,9,10,11,12]. Given COVID-19 incidence and mortality, and the precarious supply of COVID-19 vaccines globally [13,14,15,16,17,18], prioritization schemes will continue to be needed to triage vaccine delivery in early stages to people at the highest risk of death. When COVID-19 vaccines were first introduced in the United States, the Centre for Disease Control (CDC) Vaccine Rollout Recommendations [19] placed people aged 75 years and older in the Phase 1b stage, while Phase 1c extended eligibility to people aged 65–74 years and younger individuals with “underlying medical conditions which increase the risk of serious, life-threatening complications from COVID-19”.
However, this CDC approach treats “adults of any age” as being at increased risk of severe illness [20]. Thus, it does not account for differential risk between conditions, sex, or the multiplicative impact of older age on adverse outcomes among people with underlying medical conditions [21,22,23,24,25,26]. Other investigators have developed sophisticated risk prediction algorithms for mortality COVID-19 diagnosis [9, 27,28,29,30,31,32], but these do not lend themselves to simple implementation on a large scale by jurisdictions for vaccine prioritization. Furthermore, vaccine hesitancy remains an important stumbling block for vaccination in jurisdictions with adequate vaccine supplies. Unfortunately, the sociodemographic risk factors for chronic disease in the young overlap substantially with predictors of vaccine hesitancy [33,34,35,36,37,38,39,40]. Communication of risk for younger individuals can be hindered by lower absolute event rates, while relative risks can be harder to appreciate [41,42,43,44,45]. This has galvanized the development of alternate approaches for communication of risk for preventative intervention in younger patients [46,47,48,49].
Given these shortcomings, it would be desirable to provide relatively simple means to communicate how the risk of dying after being diagnosed with COVID-19 varies by age and sex for unvaccinated people living with comorbidity. Accordingly, we conducted a population-based cohort study of community-dwelling adults who developed COVID-19 before the availability of vaccines to quantify the incremental risk for death associated with underlying medical conditions as a function of age and sex. We specifically focused on cardiovascular disease, diabetes, hypertension, cancer, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD) and frailty. We hypothesized that chronic medical conditions could elevate the risk of some, but not all, younger individuals to equal that of individuals aged > 65 years.
Methods
Study design and population
Residents of Ontario (Canada’s most populous province) receive universal coverage for essential physician services and hospital-based care through the Ontario Health Insurance Plan (OHIP). This facilitates the conduct of population-based cohort studies using administrative health datasets that are linked using unique encoded identifiers and are analyzed at ICES (formerly Institute for Clinical Evaluative Sciences). Multiple algorithms have been validated to ascertain medical diagnoses using these administrative databases [50]. ICES is an independent, non-profit research institute funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC), and a prescribed entity under Ontario’s Personal Health Information Protection Act (PHIPA), Sect. 45 of PHIPA. As such, the use of the data in this project is authorized under Sect. 45, approved by ICES’ Privacy and Legal Office, exempt from Research Ethics Board review, and does not require patient consent. All methods were carried out in accordance with locally relevant guidelines and regulations.
The Ontario Laboratories Information System (OLIS) was used to identify individuals aged ≥ 18 years with a positive reverse-transcription SARS-CoV-2 polymerase chain reaction (RT-PCR) test in Ontario between January 1 and October 31st, 2020, prior to the availability of vaccines. For people with more than one positive test, we retained the first positive test. The index date was that of collection of the qualifying SARS-CoV-2 swab. We excluded people with missing/invalid key data (age, sex, OHIP number), non-Ontario residents, OHIP coverage < 1 year before the SARS-CoV-2 test (for ascertainment of medical history), or an index positive SARS-CoV-2 test that was collected on a date when the individual was hospitalized (to limit our study to outpatients). We also excluded 5740 long-term care (LTC) residents (minimum age 20 years; maximum age 107 years) since they are already prioritized in the highest risk category globally (e.g., Phase 1a of the CDC framework). The remaining patients constituted our cohort of community-dwelling outpatients with COVID-19.
Our primary exposure was age. We also studied underlying medical conditions that have been shown to increase mortality risk in COVID-19 [1,2,3,4,5,6,7,8,9,10,11,12], affect a substantial proportion of the population, and are objective enough to be implemented by governments in vaccine prioritization policies: (1) major cardiovascular disease, defined as a recent (in past 5 years) myocardial infarction [51] or lifetime history of heart failure [52]; (2) diabetes [53]; (3) hypertension [54]; (4) cancer diagnosed within 5 years [55]; (5) COPD [56]; and (6) Stages 4/ 5 CKD (defined as dialysis-dependence or estimated glomerular filtration rate (eGFR) < 30ml/min/m2) [57]. For the analysis of CKD, we excluded individuals who were not dialysis-dependent and did not have creatinine measurements in the 2 years before contracting COVID-19. We also studied the Johns Hopkins ACG System binary frailty indicator [58] as a marker of global illness that can be applied widely across multiple health systems.
Outcome
The primary outcome was death within 30 days of the positive SARS-Cov-2 test; this follow-up period after a positive PCR test is expected to capture most deaths directly attributable to COVID-19 [59, 60] while decreasing the likelihood of incorporating deaths due to other illnesses (which may be more likely for older patients with comorbidities).
Statistical analysis
We fit univariable logistic regression models using Firth’s penalized likelihood approach to address potential bias in parameter estimates due to small sample and outcomes sizes in some age/condition strata [61, 62]. In these models, age was the only predictor, and modelled using a restricted cubic spline with knots at the 5th, 35th, 65th, and 95th percentiles, as suggested by Harrell to account for the non-linear relationship between age and our outcome [63] . Since separate curves are fit to each segment (i.e., range of ages), the model better reflects the relationship between age and death. The fitted model was used to estimate the risk of death within 30 days for 75- and 65-year-old individuals. These two probabilities were used as benchmarks against which to compare other subjects, since these are the age cut-offs used in Phases 1b and 1c respectively of the CDC’s COVID-19 Vaccine Rollout Recommendations. We then repeated the same logistic regression analyses, this time stratifying the cohort by sex and presence of the underlying medical conditions described above [62]. For each sex/comorbidity stratum, we determined the predicted risk of death within 30 days at all ages and identified the age at which individuals with the medical condition exceed the predicted benchmarks risk in the general population at age 65 years and 75 years. The age at which the benchmark risks were crossed were rounded up to the next integer for ease of presentation. All analyses were performed using SAS Enterprise Guide 7.1 (SAS Institute Inc., Cary, NC).
Results
We studied 52,429 community-dwelling individuals who tested positive for SARS-CoV-2 between January 1 and October 31st, 2020 (Tables 1and Supplemental Fig. 1). Median age of our study population was 42 years [minimum, Q1, Q3, maximum 18, 29, 56, 104] years with 5,962 and 2,596 individuals 65- and 75 years and older, respectively; and 27,535 [52.5%] were women. A total of 1,185 individuals (2.3%) had major cardiovascular disease, 7,336 (14.0%) had been diagnosed with diabetes, 12,275 (23.4%) with hypertension, 966 (1.8%) with recent cancer, and 2,466 (4.7%) with COPD. Of 34,724 people (66.2% of cohort) whose CKD status could be ascertained, 350 (0.7%) were classified as having advanced CKD, of whom 146 (0.3%) were dialysis dependent. Using the Johns Hopkins indicator, 1,794 individuals (3.4%) were classified as frail.
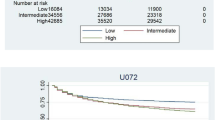
Within 30 days following their positive SARS-CoV-2 test, 417 (0.8%) people died, with the greatest death rates for both men and women among those with hypertension (78,7% and 85.9%, respectively) or classified as frail (45.8% and 60.4%, respectively) (Table 2). The predicted risk of death in the general population was 1.1% at age 65 years and 3.4% at 75 years. The estimated 30-day mortality risk increased with age (1.7% among 65–74 year olds, and 11.5% among those 75 years and older), and was generally higher in men (Fig. 1). After stratifying by presence of underlying medical conditions, the estimated risk of death was generally higher in those with a comorbidity.

Predicted risk of 30-day death by age and sex. The shaded region indicates 95% confidence intervals. The blue curves depict estimated risk in men, while the red curves depict risk in women
Figures 2 and 3 illustrate the differences in risk of death at 30 days for men and women with and without underlying medical conditions. Overall, both men and women with a medical condition had higher 30-day death rates than those without, though a few exceptions were observed (i.e., among middle-aged men with versus without COPD and older women with versus without diabetes).

Predicted risk of 30-day mortality for men by presence of underlying medical conditions. Horizontal lines indicate the predicted risk of death in the general population at age 65 years and 75 years. Vertical lines highlight the age at which the risk for men with the medical conditions is equivalent to the general population aged 65- or 75- years

Predicted risk of 30-day mortality for women by presence of underlying medical conditions. Horizontal lines indicate the predicted risk of death in the general population at ages 65 years and 75 years. Vertical lines highlight the age at which the risk for women with the medical conditions is equivalent to the general population aged 65- or 75- years
Table 3 summarizes the age (rounded up to the next integer) at which men and women with a particular comorbidity had the same predicted risk of death at 30-days as the general population aged 65 years and 75 years of age. The benchmark risks were exceeded at the earliest age by people with CKD, cancer, and frailty. For example, the risk of death at 30 days in men with CKD at age < 40 years and women with CKD at age 45 years equalled the risk of 75-year-olds from the general population. In contrast, the risk of death at 30 days for women aged < 65 years who had diabetes or hypertension was not higher than the 30-day mortality risk of 65-year-olds in the general population.
Discussion
In this population-based cohort study, we determined the estimated age at which a community-dwelling man or woman with underlying medical conditions will exceed the 30-day mortality risk of the typical person included in Phase 1b or 1c of the CDC recommendations based on age alone. While the risk of death after COVID-19 was higher in people with underlying medical conditions, the prognostic implications varied by sex and condition. The risk of 30-day death was generally higher in men than in women. The increase in risk incurred by the presence of CKD and recent cancer was higher than isolated diabetes or hypertension. Thus, it would be inappropriate to treat hypertension and diabetes as being equivalent to the other comorbidities studied when triaging vaccine rollout. The Johns Hopkins ACG System binary frailty indicator was a useful composite measure which can be applied by large health systems using administrative data for identification of individuals at higher risk for death with COVID-19 despite younger age.
Numerous publications have demonstrated that individuals with comorbidities are at higher risk for adverse outcomes following COVID-19 infection [1,2,3,4,5,6,7,8,9,10,11,12]. The comorbidities studied in our analysis have been among the most studied and most consistently linked to higher mortality with COVID-19 [1, 2, 6, 11]. In meta-analyses of studies prior to vaccine availability, reported risk estimates have ranged from 3.07 to 4.90 for CKD, 1.47 to 1.90 for cancer, and 2.25–3.05 for cardiovascular disease [1, 6, 11]. Male sex has also been consistently shown to increase the risk of adverse outcomes following COVID-19 infection [5, 8, 9], which may be related, in part, to the X-linked nature of the SARS-CoV-2 receptor [64]. The combination of multiple comorbidities increase risk even further, and this has been utilized to develop comprehensive models which predict the risk of death following COVID-19 infection with high accuracy [9, 27,28,29,30,31,32]. In a study of Veteran Affairs data in the United States, a model of nine risk factors including age, sex, diabetes, CKD and heart failure demonstrated a discriminative ability of 83.4% compared to 74.0% in a model using age alone, as in the CDC approach [65]. Furthermore, once population vaccination rates reach 50%, vaccine prioritization based on the model was estimated to result in 21.5% fewer deaths than prioritization on the CDC phased approach [65].
However, while these studies have provided valuable information about factors associated with increased COVID-19 mortality, we are not aware of studies reporting their age-equivalent mortality risk. Additionally, the inferences from these studies about the impact of comorbidity and sex on the risk of dying from COVID-19 at different ages are challenging to communicate to the public in a transparent and easily understood manner [41,42,43]. The communication gap is expected to be largest for demographic groups that are at higher risk for COVID-19 and more susceptible to misinformation [66,67,68]. The profound impact of some comorbidities on mortality is important to communicate to younger individuals with vaccine hesitancy, which remains an important issue among people with comorbidity, particularly those living in communities in which medical comorbidity is more likely to emerge at a younger age [33,34,35,36,37,38,39,40]. Provision of visual cues and expressing risk in terms of relative age (e.g., “heart age”) improves communication of cardiovascular risk for younger individuals and is more likely to promote behaviour change than traditional methods of communicating cardiovascular risk [42,43,44,45,46,47,48,49, 69]. We present our data in an analogous approach, which we believe can be helpful for vaccine-hesitant individuals with comorbidities that confer higher risk of adverse outcomes following COVID-19.
Importantly, we showed that regardless of underlying medical condition, the mortality risk rises substantially with age, meaning that age should continue to be a key factor in the triage process. The presence of most underlying medical conditions in individuals under the age of 45 years did not elevate their risk to that of the general population at age 65 years, with the notable exception of Stage 4–5 CKD, and among men, recent cancer and frailty. In other words, the protective effects of younger age persisted despite the presence of underlying medical conditions for most people aged < 45 years.
Several limitations to our study are noted. By design, we adopted an approach prioritizing parsimony and simplicity by focusing on the presence/ absence of comorbidity without accounting for the severity of disease. Although 12.8% of our study population had more than one of the conditions studied, we also did not study the combined impact of multiple comorbidities outside the frailty indicator for the same reasons. As a result, in our comparisons of risk among men and women with specific conditions versus without, it is possible that some differences may be attenuated because those without the condition have other conditions which also increase their risk. Another limitation was the small event counts for sex-specific strata of patients with cancer and CKD, which decreases precision of our estimates for these groups. Our results also do not apply to LTC residents, who should already be considered at highest risk regardless of age or comorbidities. Finally, since our study population was identified during the first eight months of the pandemic and prior to the appearance of variants of concern, such as Delta and Omicron, the absolute risk estimates by age may not be applicable to patients diagnosed with these newer variants; however, the higher mortality risks associated with CKD, cancer and frailty compared with hypertension and diabetes are likely applicable beyond the first wave though the relative risk associated with variant types differs.[70, 71] Additionally, the relative ages reported from our analyses remain valuable for communication of relative risks.
Conclusion
The mortality risk in COVID-19 increases with age and comorbidity but the prognostic implications varied by sex and condition. The risk was generally higher for men, and the increase in risk associated with CKD, cancer, and frailty was higher than what was observed with hypertension and diabetes. We hope to improve communication by presenting the combined impact of patient age, sex, and comorbidity using visual scales and reporting the “equivalent age” at which individuals would have the same mortality risk as the average 65- and 75-year-old with COVID-19. We believe these observations can inform vaccine rollout and support communication efforts in jurisdictions with limited vaccine supplies.
Data Availability
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS (or email Data Analytic Services at das@ices.on.ca). The full dataset creation plan and underlying analytic code are available from the corresponding author, Douglas S. Lee (Douglas.Lee@ices.on.ca) upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Abbreviations
- CDC:
-
Centre for Disease Control
- CKD:
-
Chronic kidney disease
- COPD:
-
Chronic obstructive pulmonary disease
- eGFR:
-
Estimated glomerular filtration rate
- LTC:
-
Long-term care
- OHIP:
-
Ontario Health Insurance Plan
- OLIS:
-
Ontario Laboratories Information System
- RT-PCR:
-
Reverse-transcription SARS-CoV-2 polymerase chain reaction
References
Ssentongo P, Ssentongo AE, Heilbrunn ES, Ba DM, Chinchilli VM. Association of cardiovascular disease and 10 other pre-existing comorbidities with COVID-19 mortality: a systematic review and meta-analysis. PLoS ONE. 2020;15(8):e0238215.
Sanyaolu A, Okorie C, Marinkovic A et al. Comorbidity and its impact on patients with COVID-19.SN Compr Clin Med2020:1–8.
Reilev M, Kristensen KB, Pottegård A, et al. Characteristics and predictors of hospitalization and death in the first 11 122 cases with a positive RT-PCR test for SARS-CoV-2 in Denmark: a nationwide cohort. Int J Epidemiol. 2020;49(5):1468–81.
Poblador-Plou B, Carmona-Pírez J, Ioakeim-Skoufa I, et al. Baseline chronic comorbidity and mortality in laboratory-confirmed COVID-19 cases: results from the PRECOVID study in Spain. Int J Environ Res Public Health. 2020;17(14):5171.
Parra-Bracamonte GM, Lopez-Villalobos N, Parra-Bracamonte FE. Clinical characteristics and risk factors for mortality of patients with COVID-19 in a large data set from Mexico. Ann Epidemiol. 2020;52:93–98e2.
Luo L, Fu M, Li Y, et al. The potential association between common comorbidities and severity and mortality of coronavirus disease 2019: a pooled analysis. Clin Cardiol. 2020;43(12):1478–93.
Imam Z, Odish F, Gill I, et al. Older age and comorbidity are independent mortality predictors in a large cohort of 1305 COVID-19 patients in Michigan, United States. J Intern Med. 2020;288(4):469–76.
Harrison SL, Fazio-Eynullayeva E, Lane DA, Underhill P, Lip GY. Comorbidities associated with mortality in 31,461 adults with COVID-19 in the United States: a federated electronic medical record analysis. PLoS Med. 2020;17(9):e1003321.
Clift AK, Coupland CA, Keogh RH, et al. Living risk prediction algorithm (QCOVID) for risk of hospital admission and mortality from coronavirus 19 in adults: national derivation and validation cohort study. BMJ. 2020;371:m3731.
Cho SI, Yoon S, Lee H-J. Impact of comorbidity burden on mortality in patients with COVID-19 using the korean health insurance database. Sci Rep. 2021;11(1):1–9.
Biswas M, Rahaman S, Biswas TK, Haque Z, Ibrahim B. Association of sex, age, and comorbidities with mortality in COVID-19 patients: a systematic review and meta-analysis. Intervirology. 2021;64(1):36–47.
Bajgain KT, Badal S, Bajgain BB, Santana MJ. Prevalence of comorbidities among individuals with COVID-19: a rapid review of current literature. Am J Infection Control. 2021;49(2):238–46.
Wouters OJ, Shadlen KC, Salcher-Konrad M, et al. Challenges in ensuring global access to COVID-19 vaccines: production, affordability, allocation, and deployment. Lancet. 2021;397(10278):1023–34.
Katz IT, Weintraub R, Bekker L-G, Brandt AM. From vaccine nationalism to vaccine equity—finding a path forward. N Engl J Med. 2021;384(14):1281–3.
Asundi A, O’Leary C, Bhadelia N. Global COVID-19 vaccine inequity: the scope, the impact, and the challenges. Cell Host Microbe. 2021;29(7):1036–9.
Hassan F, London L, Gonsalves G. Unequal global vaccine coverage is at the heart of the current covid-19 crisis. BMJ. 2021;375:n3074.
Kim JH, Hotez P, Batista C, et al. Operation Warp Speed: implications for global vaccine security. Lancet Glob Health. 2021;9(7):e1017–21.
Kim SY, Yeniova A. Global, regional, and national incidence and mortality of COVID-19 in 237 countries and territories, January 2022: a systematic analysis for World Health Organization COVID-19 dashboard. Life Cycle. 2022;2:e10.
Centers for Disease Control and Prevention. CDC’s COVID-19 Vaccine Rollout Recommendations. Available online at https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations.html. Accessed March 27, 2021.
Centers for Disease Control and Prevention. Certain Medical Conditions and Risk for Severe COVID-19 Illness. Available online at https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html. Accessed on March 27, 2021.
Dehingia N, Raj A. Sex differences in COVID-19 case fatality: do we know enough? Lancet Glob Health. 2021;9(1):e14–5.
Yanez ND, Weiss NS, Romand J-A, Treggiari MM. COVID-19 mortality risk for older men and women. BMC Public Health. 2020;20(1):1–7.
Bhopal SS, Bhopal R. Sex differential in COVID-19 mortality varies markedly by age. Lancet. 2020;396(10250):532–3.
Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052–9.
Grasselli G, Greco M, Zanella A, et al. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern Med. 2020;180(10):1345–55.
Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–62.
Yan L, Zhang H-T, Goncalves J, et al. An interpretable mortality prediction model for COVID-19 patients. Nat Mach Intell. 2020;2(5):283–8.
Yadaw AS, Yan-Chak L, Bose S, Iyengar R, Bunyavanich S, Pandey G. Clinical features of COVID-19 mortality: development and validation of a clinical prediction model. Lancet Digit Health. 2020;2(10):e516–25.
Nafilyan V, Humberstone B, Mehta N, et al. An external validation of the QCovid risk prediction algorithm for risk of mortality from COVID-19 in adults: a national validation cohort study in England. Lancet Digit Health. 2021;3(7):e425–33.
Knight SR, Ho A, Pius R, et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: development and validation of the 4 C mortality score. BMJ. 2020;370:m3339.
Jimenez-Solem E, Petersen TS, Hansen C, et al. Developing and validating COVID-19 adverse outcome risk prediction models from a bi-national european cohort of 5594 patients. Sci Rep. 2021;11(1):3246.
Gao Y, Cai G-Y, Fang W, et al. Machine learning based early warning system enables accurate mortality risk prediction for COVID-19. Nat Commun. 2020;11(1):1–10.
Tsai R, Hervey J, Hoffman K, et al. COVID-19 vaccine hesitancy and acceptance among individuals with cancer, autoimmune diseases, and other serious comorbid conditions: cross-sectional, internet-based survey. JMIR Public Health Surveill. 2022;8(1):e29872.
Savoia E, Piltch-Loeb R, Goldberg B, et al. Predictors of COVID-19 vaccine hesitancy: socio-demographics, co-morbidity, and past experience of racial discrimination. Vaccines (Basel). 2021;9(7):767.
Robertson E, Reeve KS, Niedzwiedz CL, et al. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav Immun. 2021;94:41–50.
Mejri N, Berrazega Y, Ouertani E, et al. Understanding COVID-19 vaccine hesitancy and resistance: another challenge in cancer patients. Support Care Cancer. 2022;30(1):289–93.
Bleser WK, Miranda PY, Jean-Jacques M. Racial/ethnic disparities in influenza vaccination of chronically-ill us adults: the mediating role of perceived discrimination in healthcare. Med Care. 2016;54(6):570.
Grumbach K, Judson T, Desai M, et al. Association of race/ethnicity with likeliness of COVID-19 vaccine uptake among health workers and the general population in the San Francisco Bay Area. JAMA Intern Med. 2021;181(7):1008–11.
Malik AA, McFadden SM, Elharake J, Omer SB. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine. 2020;26:100495.
Szilagyi PG, Thomas K, Shah MD, et al. National trends in the US public’s likelihood of getting a COVID-19 vaccine—April 1 to December 8, 2020. JAMA. 2021;325(4):396–8.
Stone ER, Yates JF, Parker AM. Risk communication: absolute versus relative expressions of low-probability risks. Organ Behav Hum Decis Process. 1994;60(3):387–408.
Gordon-Lubitz RJ. Risk communication: problems of presentation and understanding. JAMA. 2003;289(1):95–5.
Edwards A, Elwyn G. Understanding risk and lessons for clinical risk communication about treatment preferences. Qual Health Care. 2001;10(suppl 1):i9–i13.
Freemen A. The strange world of risk perception, and communicating risks. 2020. Available online at: https://blogs.bmj.com/bmj/2020/11/18/alexandra-freeman-the-strange-world-of-risk-perception-and-communicating-risks/. Accessed December 4, 2021.
Fagerlin A, Zikmund-Fisher BJ, Ubel PA. Helping patients decide: ten steps to better risk communication. J Natl Cancer Inst. 2011;103(19):1436–43.
Bonner C, Bell K, Jansen J, et al. Should heart age calculators be used alongside absolute cardiovascular disease risk assessment? BMC Cardiovasc Disord. 2018;18(1):1–8.
Bonner C, Raffoul N, Battaglia T, Mitchell JA, Batcup C, Stavreski B. Experiences of a national web-based heart age calculator for cardiovascular disease prevention: user characteristics, heart age results, and behavior change survey. J Med Internet Res. 2020;22(8):e19028.
Damman OC, Vonk SI, Van den Haak MJ, van Hooijdonk CM, Timmermans DR. The effects of infographics and several quantitative versus qualitative formats for cardiovascular disease risk, including heart age, on people’s risk understanding. Patient Educ Couns. 2018;101(8):1410–8.
Lopez-Gonzalez AA, Aguilo A, Frontera M, et al. Effectiveness of the Heart Age tool for improving modifiable cardiovascular risk factors in a southern european population: a randomized trial. Eur J Prev Cardiol. 2015;22(3):389–96.
Lee DS, Ma S, Chu A, et al. Predictors of mortality among long-term care residents with SARS-CoV-2 infection. J Am Geriatr Soc. 2021;69(12):3377–88.
Vermeulen MJ, Tu JV, Schull MJ. ICD-10 adaptations of the Ontario Acute Myocardial Infarction Mortality Prediction Rules performed as well as the original versions. J Clin Epidemiol. 2007;60(9):971–4.
Schultz SE, Rothwell DM, Chen Z, Tu K. Identifying cases of congestive heart failure from administrative data: a validation study using primary care patient records. Chronic Dis Inj Can. 2013;33(3):160–6.
Lipscombe LL, Hwee J, Webster L, Shah BR, Booth GL, Tu K. Identifying diabetes cases from administrative data: a population-based validation study. BMC Health Serv Res. 2018;18(1):316.
Tu K, Campbell NR, Chen ZL, Cauch-Dudek KJ, McAlister FA. Accuracy of administrative databases in identifying patients with hypertension. Open Med. 2007;1(1):e18–e26.
Robles SC, Marrett LD, Clarke EA, Risch HA. An application of capture-recapture methods to the estimation of completeness of cancer registration. J Clin Epidemiol. 1988;41(5):495–501.
Gershon AS, Warner L, Cascagnette P, Victor JC, To T. Lifetime risk of developing chronic obstructive pulmonary disease: a longitudinal population study. Lancet. 2011;378(9795):991–6.
Fleet JL, Dixon SN, Shariff SZ, et al. Detecting chronic kidney disease in population-based administrative databases using an algorithm of hospital encounter and physician claim codes. BMC Nephrol. 2013;14:81.
Abrams C, Lieberman R, Weiner JP. Development and evaluation of the Johns Hopkins University risk adjustment models for Medicare + Choice plan payment. Final report to Centers for Medicare and Medicaid Services, US Department of Health and Human Services. Baltimore, MD, USA: Johns Hopkins University. Published June 6, 2003.
Jung S-M, Akhmetzhanov AR, Hayashi K, et al. Real-time estimation of the risk of death from novel coronavirus (COVID-19) infection: inference using exported cases. J Clin Med. 2020;9(2):523.
Faes C, Abrams S, Van Beckhoven D, Meyfroidt G, Vlieghe E, Hens N. Time between symptom onset, hospitalisation and recovery or death: statistical analysis of belgian COVID-19 patients. Int J Environ Res Public Health. 2020;17(20):7560.
Firth D. Bias reduction of maximum likelihood estimates. Biometrika. 1993;80(1):27–38.
LaValley MP, Logistic, Regression. Circulation. 2008;117(18):2395–9.
Harrell FE. Regression modeling strategies: with applications to Linear Models, logistic and ordinal regression, and Survival Analysis. Springer International Publishing; 2015.
Tukiainen T, Villani AC, Yen A, et al. Landscape of X chromosome inactivation across human tissues. Nature. 2017;550(7675):244–8.
Ioannou GN, Green P, Fan VS, et al. Development of COVIDVax model to estimate the risk of SARS-CoV-2–related death among 7.6 million US veterans for use in vaccination prioritization. JAMA Netw Open. 2021;4(4):e214347–7.
Roozenbeek J, Schneider CR, Dryhurst S, et al. Susceptibility to misinformation about COVID-19 around the world. R Soc Open Sci. 2020;7(10):201199.
Ali SH, Foreman J, Tozan Y, Capasso A, Jones AM, DiClemente RJ. Trends and predictors of COVID-19 information sources and their relationship with knowledge and beliefs related to the pandemic: nationwide cross-sectional study. JMIR Public Health Surveill. 2020;6(4):e21071.
Petrova D, Kostopoulou O, Delaney BC, Cokely ET, Garcia-Retamero R. Strengths and gaps in physicians’ risk communication: a scenario study of the influence of numeracy on cancer screening communication. Med Decis Making. 2018;38(3):355–65.
Kurz-Milcke E, Gigerenzer G, Martignon L. Transparency in risk communication: graphical and analog tools.Ann N Y Acad Sci2008:18–28.
Centers for Disease Control and Prevention. COVID-19 Data Review: Update on COVID-19–Related Mortality. Available online at https://www.cdc.gov/coronavirus/2019-ncov/science/data-review/index.html. Last updated Jan. 27, 2023. Accessed January 31, 2023.
Ward IL, Bermingham C, Ayoubkhani D, et al. Risk of COVID-19 related deaths for SARS-CoV-2 Omicron (B.1.1.529) compared with Delta (B.1.617.2): retrospective cohort study. BMJ. 2022;378:e070695.
Acknowledgements
This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and information compiled and provided by the Ontario Ministry of Health, CIHI and Ontario Health. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Funding
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and Ministry of Long-Term Care (MLTC), and by a grant from the Canadian Frailty Network (to DSL). The funding sources had no role in the design of this study, collection, analysis and interpretation of data, or in the writing of this manuscript.
Author information
Authors and Affiliations
Contributions
HAQ contributed to the conception of this work, analysis and interpretation of data and drafted the manuscript. PCA, HCW and DSL contributed to the conception of this work, and analysis and interpretation of data. AS and AC contributed to the analysis and interpretation of the data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
ICES is an independent, non-profit research institute funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). As a prescribed entity under Ontario’s Personal Health Information Protection Act (PHIPA), Sect. 45 of PHIPA authorizes ICES to collect and use personal health information and health care data, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system Ontario’s privacy legislation. Secure access to these data is governed by policies and procedures that are approved by the Information and Privacy Commissioner of Ontario. Projects that use data collected by ICES under Sect. 45 of PHIPA, and use no other data, are exempt from Research Ethics Board review. The use of the data in this project is authorized under Sect. 45 and approved by ICES’ Privacy and Legal Office. All methods were carried out in accordance with locally relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
HA is supported by a National New Investigator Award from the Heart and Stroke Foundation of Canada. PA was supported by a Mid-Career Investigator Award from the Heart and Stroke Foundation of Ontario. DSL is supported by the Ted Rogers Chair in Heart Function Outcomes. All other authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Abdel-Qadir, H., Austin, P.C., Sivaswamy, A. et al. Comorbidity-stratified estimates of 30-day mortality risk by age for unvaccinated men and women with COVID-19: a population-based cohort study. BMC Public Health 23, 482 (2023). https://doi.org/10.1186/s12889-023-15386-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15386-4