
Abstract
Background
In March 2020, the COVID-19 outbreak was declared a pandemic by the World Health Organization (WHO), generating stark economic and social repercussions that directly or indirectly affected families’ wellbeing and health status.
Aims
This review aims at mapping the existing evidence on the impact of the COVID-19 pandemic on maternal mental health, early childhood development, and parental practices, worldwide, to identify evidence gaps and better inform future delivery of care and health policy measures.
Methods
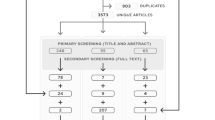
Following the protocol defined by PRISMA-ScR, this scoping review has searched for relevant studies published between January 2020 and June 2021, selecting evidence sources based on pre-established criteria. From a total of 2,308 articles, data were extracted from 537 publications from 35 countries on all three health domains.
Results
The combined stressors brought forth by the pandemic have exerted a heavy burden on the mental health of mothers and the development of young children, partly mediated by its impact on parental practices.
Conclusions
Despite remaining gaps, we have identified sufficient evidence pointing to an urgent need for more concerted global research efforts and rapid policy responses to timely address severe and pervasive negative impacts to the mental health of mothers and children at a key developmental stage.
Similar content being viewed by others


Background
Rationale
In March 2020, the COVID-19 outbreak was declared a pandemic by the World Health Organization (WHO). Following a complex interplay among social, cultural, and economic local contexts, regional-level infection rates developed differently, largely in response to administrative and public health measures. The economic and social impact of the pandemic on population wellbeing differed between and within countries, largely influenced by levels of employment insecurity, financial hardship, elevated morbidity and mortality burdens, requirement for prolonged social isolation measures, and overwhelmed health systems, contributing as significant stressor factors endured by families, globally.
Given the unprecedented nature of the COVID-19 pandemic, large evidence gaps exist on how the mental health of caregivers, as well as the early development of children, might have been impacted since the onset of the pandemic through various pathways—particularly through changes in key parental practices that directly affect children's wellbeing and the establishment of parental bonds. Prolonged adverse social conditions and family experiences, leading to toxic stress exposure, are particularly detrimental during the first years of children's lives, deeply affecting their present wellbeing as well as generating lifelong health consequences. The impact of the pandemic on these outcomes is, thus, deeply permeated by social determinants at play, which in turn delineates the unique cluster of social and biological factors interacting and jointly producing the impacts on health status and caregiving practices, captured by this review [227].
Objectives
The main goal of this review was to address the question: what is the current evidence of the effects of the COVID-19 pandemic on maternal mental health, early child development (ECD), parenting practices, and the establishment of parental bonds, worldwide?
This study employs the nurturing care framework [228] as the basis upon which the three areas of interest are conceptualized and defined, i.e., early childhood development (ECD), parental practices, and maternal mental health. Early childhood development, therefore, is defined as the group of processes comprised within the first years of life, consisting of several interdependent domains, including sensory-motor, cognitive, and social-emotional [229,230,231]. Such rapid and critical developmental processes are sustained by nurturing care dispensed to young children, here defined as inter-related behaviours, attitudes, and knowledge regarding caregiving practices; stimulation; responsiveness, and safety [228]. Parental practices, therefore, are conceptualized in our review as the group of caregiving practices that promote a stable environment sensitive to children’s health needs, offer opportunities for early learning, and provide security, support, and adequate stimulation [228]. Accordingly, maternal mental health is here defined as the wellbeing and mental health status of mothers, as primary caregivers to young children, and its role in fostering or hindering their capacity to adequately provide nurturing care. Under such assumptions, parental practices are hypothesized to impact ECD both directly, when primarily performed by either mothers or other caregivers, and indirectly, when its impact is moderated by maternal mental health [233,234,235].
Relevance
Defining the evidence gap around the possible effects of the pandemic on the mental health of mothers and on the development of children to better inform future delivery of care and health policy measures.
Materials and methods
We followed the protocol defined by the Preferred Reporting Items for Systematic Reviews extension for Scoping Reviews (PRISMA-ScR) [232]. This review was not registered in PROSPERO since the platform does not accept the registration of scoping reviews.
Importantly, scoping reviews differ from systematic reviews in design, purpose, and structure. Following this study’s goal of mapping existing evidence on the field of interest, a scoping review has been deemed a more appropriate choice. The PRISMA-ScR defines as potential goals of scoping reviews the following: examining the extent, range, and nature of the evidence on a topic or question; summarizing findings from a body of knowledge that is heterogeneous in methods or discipline; or identifying gaps in the literature to aid the planning and commissioning of future research, including systematic reviews [232]. Conversely, systematic reviews are the appropriate methodology for addressing questions that aim at informing clinical decision-making, such as determining the feasibility, appropriateness, meaningfulness, or effectiveness of a particular intervention, potentially employing risk-of-bias assessment and meta-analysis [232, 236].
Eligibility Criteria
Publications were eligible for inclusion if they contributed with scientific evidence regarding at least one of our three categories in relation to the COVID-19 pandemic, i.e., maternal mental health, early childhood development, and parental practices when concerning our population of interest, that is, mothers and/or caregivers, as well as children from 0–10 years old, worldwide. No age delimitation was defined for mothers and/or caregivers, and no specification was made for children and caregivers’ ethnicity and socioeconomic status. The lack of delimitations reflected the review aim of encompassing existing evidence regarding a broad range of populations, to better map gaps in the field. Peer-reviewed publications were included if they were published between January 1st, 2020, and June 9th, 2021. No language constraints were applied. Publications were required to comply with the following criteria:
-
(1)
Empirical studies that: (i) included our specified population of interest, and (ii) collected data and performed quantitative or qualitative analysis concerning at least one of the three outcome categories of our review.
-
(2)
Case reports describing health outcomes of neonates born to COVID-19 positive mothers.
-
(3)
Systematic reviews that: (i) included at least one of our outcome categories of interest, and (ii) presented detailed replicable search and selection methodology.
Given the unprecedented nature of the COVID-19 pandemic, case reports based on clinical records were included to assess initial documentation of its potential impact on early childhood development and the extent to which hypotheses raised by such reports were addressed by empirical research studies. Finally, rigorous systematic reviews aided our assessment of the evidence gap concerning our research question.
Regarding the age delimitation for studies concerning early childhood development, the choice for including children up to 10 years old reflects the goal of the scoping review to exhaustively identify relevant evidence concerning the outcomes of interest. The establishment of such a goal incurs a limitation to exclude studies that included in their sample children whose age exceeded the cutoff of 5 years old, which traditionally defines early childhood. This limitation is justified by the impossibility to derive from the findings of such studies those that pertained only to children 0–5 years old, given that findings were not always stratified by age sub-range. The choice for employing flexibility in the target age range addressed the characteristics of the nascent state of the field, which struggled to capture the rapid changes in population health status during the pandemic, incurring added difficulties in sampling, enrollment, and data collection procedures, prioritizing access to available studies’ subjects over rigor on sampling criteria.
Finally, while narrowing children’s age range was found to be unfeasible, the study opted for delimitating the analysis of caregivers’ mental health to mothers only. While examining the changes in the mental health status of fathers and other caregivers is undoubtedly relevant to better understanding the impact of the pandemic on ECD, parental practices, and family health, such delimitation reflected the need for processing available evidence on the initially settled outcomes on a pace that accompanied the articles production volume, over the inclusion of an additional outcome category which can be addressed by future research.
Information sources
A search strategy was constructed to retrieve studies addressing the following parameters about the COVID-19 pandemic: mental health of mothers and pregnant women; parenting; perinatal, infant, and childhood development. The following databases were searched: PubMed/Medline (National Library of Medicine, NCBI), Embase (Elsevier, Embase.com), PsycInfo (American Psychological Association), and CINAHL (CINAHL Plus with Full Text, Ebsco). Controlled vocabulary terms (i.e., MeSH, Emtree, APA Thesaurus of Psychological Index Terms, CINAHL subject headings) were included when available and appropriate. The search strategies were designed and executed by a librarian (Carol Mita) on December 8th, 2020. Subsequently, an updated search was conducted on June 9th, 2021, utilizing the same methods. The exact search terms used for each of the databases are provided in a supplementary document. The electronic database search was supplemented by searching the WHO Global Research on the COVID-19 database and scanning relevant reviews published within the pre-defined period.
Selection of publications
Search results were imported to the Covidence reference manager platform (Covid Systematic Review Software, Veritas Health Innovation, Melbourne Australia), and duplicates were removed. Initial selection by title and abstract and subsequent full-text review of remaining articles was conducted blindly by four independent reviewers with expert knowledge of the research area, following pre-established selection criteria as presented in the Eligibility Criteria section. Each selected publication was then individually appraised by two reviewers blindly. Divergent votes of inclusion based on pre-established criteria were settled through discussion and consensus among the reviewer’s team.
Articles excluded from either abstract or full-text selection were categorized as such:
-
1.
Empirical research, case reports, or systematic literature review with no inclusion of population of interest.
-
2.
Literature review not specifying the methodology for selection.
-
3.
Empirical research, case reports, or literature review with no inclusion of any of the outcome categories of interest.
-
4.
Clinical or hospital guidelines.
-
5.
Commentaries letters to the editors, or any other publication not complying with the categories of empirical research, case report, or systematic literature review.
-
6.
Study protocol.
Data charting
A data charting Microsoft Excel@ table was jointly developed by two reviewers to categorize the variables to extract from selected publications, concerning the three categories of interest of the review. The table was updated based on an iterative process as data extraction proceeded and new variables were deemed relevant. A separate table was created to categorize excluded publications. All charting tables can be found in the Supplementary material.
The selection of variables of empirical reports and systematic reviews followed an iterative process, which began by testing a simplified data charting form with 3 variables: outcome category, place, and date of study publication. This initial form was tested with a sample of 30 articles by two reviewers, independently, with the joint purpose of examining the adequacy of the 3 prespecified variables and identifying other key characteristics. After the initial testing, it was determined by consensus among the reviewers and the study team the following:
-
1.
While the three prespecified variables were adequate for assessing empirical reports, registering a place of publication for systematic reviews was deemed less relevant, given the collaborative nature of such works, often involving international research centers. The country of publication was used as a proxy for the country of data collection within empirical studies, informing about countries’ capacity for undertaking scientific research during the pandemic, data that were later examined against countries’ level of income, informing the relation between economic development and potential for undertaking scientific research, regardless of its quality or relevance. It also allowed direct mapping of evidence gaps concerning less studied populations given the data collection procedures. Systematic reviews did not allow for such approximations.
-
2.
While a formal risk-of-bias assessment lies within the goals of systematic rather than scoping reviews, the team concluded that it was necessary to register major study characteristics that could inform the internal validity of empirical studies, given the pace of publication and heightened interest of the scientific community for the field. Following this conclusion, variables concerning study design, sampling method, and utilization of validated instruments were included.
This evaluation process was repeated one more time with a larger sample of 60 articles, resulting in the addition of the variables concerning sample size and population. Throughout both piloting rounds, a third independent reviewer acted as an arbitrator when a lack of consensus occurred. During the data charting of included articles, 5 additional independent reviewers were included in the analysis team.
Similarly, data charting for evidence gaps was executed through an iterative process involving a team of 7 independent reviewers and a single arbitrator. During data charting reviewers were asked to register aspects of each paper that they found could be better developed or at least minimally addressed. After charting was concluded, reviewers gathered and presented their lists of such missing aspects, which were registered as single entries. Subsequently, the team jointly analyzed such entries to identify common themes within each outcome category. Lastly, themes were organized by domains following the conceptual framework that structured data charting of included articles. These data are presented as evidence gaps.
Data items
Nine variables were extracted from the final sample of selected studies: (i) inclusion criteria, i.e., primary research studies, case reports, or systematic reviews, (ii) country of publication, (iii) date of publication, (iv) study design, e.g., cross-sectional, prospective cohort, case–control, (v) type of sampling method, e.g., convenience sampling, open-access online form, (vi) utilization of validated instruments, e.g., scales measuring presence and severity of depressive symptoms, such as Edinburgh Postnatal Depression Scale (EPDS), (vii) primary outcome variables followed by scale utilized for measurement, if any, e.g., postnatal depression (EPDS), (viii) sample size of both reference and control groups when present, and (ix) study population, e.g., pregnant women, postnatal women, mothers of children 5–9 years old. Except for variables (i), (iii), (vii), and (ix), all apply to empirical research studies or case reports, not to systematic reviews.
Critical appraisal of publications
We have conducted a frequency assessment of three main characteristics that inform the strength of the evidence produced by the selected empirical research studies, concerning their design, sampling, and measurement. These data were extracted from the data charting table and were selected as a way of appraising the quality of evidence production within the context of heightened interest of the scientific community around COVID-19, reflected on the accelerated rate of publications as the pandemic unfolded. They especially help to inform the validity and reliability of evidence concerning etiologic questions around the research area. Furthermore, we conducted a detailed validity assessment of all included review papers according to the PRISMA 2020 Checklist, utilizing the PRISMA application (PRISMA Checklist). The checklist contains 42 items in total, which we have used to generate a quality score categorizing review publications' quality by score terciles: 0–14 indicates low quality, 15–28 medium quality, and 29–42 high quality. We only included findings from medium and high-quality reviews in our final analysis. Individual quality assessment reports can be found in the Supplementary material.
Synthesis of results
We present summarized publications` results by (1) main relevant characteristics, e.g., type, date, and country of publication, and (2) the three main outcome categories they refer to, i.e., maternal mental health, ECD, and parental practices. Supplementary systematic review findings, identified by scanning the WHO website, are included in the results as well.
Results
Selection of sources of evidence
Figure 1 shows the detailed publications selection flow diagram. Categories of exclusion are detailed in the Materials and Methods section, Selection of Publications sub-section.

Flow diagram of the selection process showing identification, screening, and final inclusion of publications
Characteristics and critical appraisal of evidence sources
Individual characteristics of each included publication can be found in the Supplementary material. Figure 2 displays the distribution of eligible publications by month, from January 1st, 2020, until June 9th, 2021. The accelerated growth of the publication rate from July 2020 on is distinguishable, being especially pronounced in November 2020, as well as in April and May 2021.

Distribution of publications by month, from January 1st, 2020, until June 9th, 2021
Summarized characteristics of interest of the selected empirical research studies (n = 442) and case reports (n = 55) are:
-
1.
Publication frequency by country-level income group, as categorized by the World Bank (2021): 63.19% of all selected publications were conducted in high-income countries, 28% in upper-middle-income countries, 5.23% in lower-middle, and 0.97% in low-income countries.
-
2.
Countries with the highest number of publications: U.S. (21.2%), China (13.8%), Italy (8.9%), Turkey (5.5%), U.K (5.5%).
-
3.
Main characteristics of empirical research studies: 67.4% employed a cross-sectional design, 34% utilized convenience sampling methods based on online open access links disseminated through social media platforms, and 52.2% used validated instruments of measurement concerning either maternal mental health, ECD, and/or parental practices.
-
4.
The most frequently utilized validated instruments/scales were the Edinburgh Postnatal Depression scale – EPDS (11,9%), General Anxiety Disorder-7 – GAD (7%), Parenting Stress Index – PSI (4.2%), State-Trait Anxiety Inventory- STAI (4%), Strengths and Difficulties Questionnaire – SDQ (3,2%), and Zung Self-Rating Anxiety Scale – SAS (2,4%).
-
5.
The most assessed variables concerning maternal mental health were stress (28,3%), depression (29,1%), and anxiety (30,1%).
Results by categories and domains
Summarized findings concerning the three main outcome categories analysed by this review are presented next. Table 1 displays the most reported factors, categorized by domains, impacting maternal mental health, early child development and parenting practices.
Maternal mental health
This analysis is based on an understanding that mental disorders exist in a spectrum. As such, a dimensional approach is assumed as the basis to inform the individual lived experience of suffering and resilience in the targeted population. The approach considers the differing resources that individuals may have at their disposal based on their unique developmental trajectories, as well as mediating protective factors such as different levels of social support, access to health services, or income stability.
The principle of convergence of evidence from multiple fields [150] oriented our analysis of the risk factors at play, largely informed by the sociological, economic, environmental, and medical perspectives on the impact of poverty and inequality on mental health. Risk factors are understood as potential moderators to the outcome, affecting it differently according to their severity level. Risk factors will be categorized by domains, informed by the Lancet Commission on Global Mental Health and Sustainable Development [150].
Table 2 Summarizes the findings of included systematic reviews with meta-analysis (n = 5) on the impact of the pandemic on maternal mental health. Table 3 shows evidence gaps, categorized by domains, concerning the impact of the COVID-19 pandemic on maternal mental health.
Protective factors identified in the selected studies were frequently related to individual emotional and psychological resources, namely latent constructs such as self-kindness, resilience, or perceived self-efficacy. The role of parental personality traits such as neuroticism or psychological flexibility were scrutinized as components of complex models correlating children and parental mental health, moderated, for instance, by family functioning impact or presence of other family members outside the maternal-infant dyad [44, 121].
Studies that analysed risk factors related to unbalanced caregiving and housework responsibilities were all conducted in high or upper-middle-income countries [11, 32, 39, 40, 47, 64, 70, 73, 79, 83, 110, 116, 122, 130, 157, 177, 202, 211, 212, 214, 215, 219] pointing to a large evidence gap concerning the exacerbation of gender inequities during lockdown measures and its impact on maternal well-being in low- and middle-income countries (LMICs).
Importantly, this gap extends to overall descriptive findings regarding the prevalence of elevated maternal stress, anxiety, and depressive symptoms, as well as associated risk factors across all areas as suggested by the low prevalence of included publications from low and lower-middle-income countries, 0.97% and 5.23%, respectively.
Disrupted sleeping and dietary patterns, as well as sleep deprivation, were as commonly reported as unbalanced and increased caregiving and housework responsibilities during the lockdown. This parallel suggests that the negative health impact on maternal wellbeing could be mitigated by a more balanced division of such responsibilities within households on lockdown, especially when considering children’s age as a relevant factor to maternal burnout. Equivalently, lack of support has often been directly associated with worsened maternal mental health status.
While access barriers to health services pose an obvious threat to maternal health, barriers to accessing clear, concise, and sufficient information regarding health risks related to COVID appeared as a major source of concern to mothers. Fear of infection and vertical transmission, as well as fear of adverse birth outcomes, were commonly registered risk factors. Conversely, effective public health communication efforts would be directly beneficial to maternal mental health, in diverse contexts.
Early childhood development
Our review indicated that robust, consistent, and up-to-date global/regional estimates of the pandemic's impact on children`s morbidity and mortality burdens are not yet consolidated in the literature.
Concerning summarized findings on health outcomes of neonates born to COVID-19 positive mothers, we found 8 systematic reviews without meta-analysis [1, 8, 81, 85, 88, 132, 149, 218] and 5 with meta-analysis, presented in Table 4. Table 5 shows evidence gaps, categorized by domains, concerning the impact of the COVID-19 pandemic on early childhood development.
Chmielewska et al. [32] identified an unchanged global prevalence in preterm birth and neonatal death, pointing out, however, that data suggest increased rates of both outcomes in LMICs and decreased in high-income countries (HICs), apparently driven by a reduction in spontaneous preterm birth in HICs. This finding stresses the role of insufficient capacity of healthcare systems to cope with the pandemic. Furthermore, despite large evidence gaps, the review shows that stillbirth rates might be particularly increased in LMICs. These findings highlight the urgent need for more contributions from LMICs regarding the differential impact of the pandemic and its interplay with local socioeconomic conditions, as well as pre-existing and exacerbated disease burdens concerning maternal and neonatal health. While the strong association between parental and children's mental health was pointed out in various studies [20, 31, 49, 72, 99, 151, 169, 183, 184] some sought to identify mediating mechanistic effects, such as parental emotion regulation capacity during lockdown [159, 160] or parental perceived manageability of the dyadic relationship [183, 184].
Most studies have either assessed worsened mental health states, such as the significantly higher prevalence of anxiety and depression symptoms [43, 100, 100, 174, 189, 195, 217] or changes in children’s behavioural patterns or developmental markers. Despite scarce evidence and particularly large evidence gaps concerning LMICs, few studies highlighted fundamental aspects of the pandemic's impact on ECD.
While reported changes in sleeping patterns were mixed [11, 24, 25, 84, 108, 137, 225] sedentarism during social isolation restrictions appears to be exceptionally high in one Canadian study [127], based on WHO recommendations. Additionally, a U.S. study utilized pre-existing longitudinal data on expected reading ability gain among kindergarten children to predict changes associated with school closures [13], concluding that in the absence of formal in-person education such gains would decrease by 31%. However, the model also predicted that the loss could be ameliorated by 42% if children had books read to them daily.
The impact of disrupted early childhood education undertaken in school and daycare centers that remained closed during lockdown was well documented in the literature. Equivalently, many studies sought to identify disrupted daily habits, such as sleeping and dietary patterns, as well as changes in screen time, regular physical activities, and loss of playing time outdoors. The potential associations between school closures and behavioral changes could be better explored, ideally through a careful examination of how factors such as socioeconomic status, the presence of welfare policies, or caregiving dynamics might inform these associations.
Overall, the review identified scattered initiatives in documenting the impact of the pandemic on developmental milestones and educational gaps. A more synthetic analytical approach would better inform how such impacts could differ by sociocultural context, gender, ethnicity, and socioeconomic status. Importantly, the acute paucity of longitudinal data on the impact of the pandemic on early childhood development is a considerable barrier to a more comprehensive understanding of its ongoing effects on the health and wellbeing of children worldwide, during a key developmental period. This scarcity of consistent information on the subject also hinders the analysis of its relationship with social determinants at play, which in turn is needed for the design and implementation of effective public health policies aiming at fostering healthier developmental paths.
Finally, most studies examined the multiple pathways through which the advent of the pandemic might have impacted ECD under scenarios that preserved the normal functioning of institutions to a considerable extent, but not much is known about such impact under ongoing humanitarian crises. Certainly, there is a large gap regarding the potential interaction between the pandemic and concomitant events that have likely acted as catalysts, magnifying the impact on ECD, such as natural and industrial disasters, war and conflict, climate change, forced migration, as well as trauma and violence on diverse scales.
Parenting practices
From the 497 empirical studies and case reports included in this review only 69 (14%) directly or indirectly assessed parental practices during the COVID-19 pandemic, comprising not only descriptive studies on children's mental health and behaviour patterns but also assessments of potential predictors and mechanistic effects mediating parental mental health and children’s wellbeing.
Table 6 shows evidence gaps, categorized by domains, concerning the impact of the COVID-19 pandemic on parenting practices.
A pressing matter concerning newborn care raised by a few studies [175, 195, 203] is whether COVID-19 positive mothers and their newborn babies should be separated to avoid vertical transmission. Recent guidelines by the WHO (World Health Organization, 2021) recommend maintaining close mother-baby contact as a fundamental measure to prevent newborn morbidity and mortality during the pandemic, stimulating practices such as kangaroo care and breastfeeding, especially among babies born preterm or at low birth weight. Accordingly, the number of mother-newborn separation days in one study [203] was found to be negatively associated with neurobehavioral development at 3 months old, after adjusting for preterm and NICU admission. Yet, evidence suggests that family visitations and receipt of developmental care activities were less frequent and shorter [175] among preterm infants admitted at a U.S. newborn intensive care unit (NICU).
Similarly, one review [199] found a stark misalignment between WHO recommendations and country-specific guidelines regarding breastfeeding and newborn care practices during the pandemic across 33 countries. The review points out that not only inconsistencies on guidelines were abundant (and none recommended all aspects of WHO guidance), but they also frequently included recommendations against practices supportive of breastfeeding, even in countries with high infant mortality rates. Despite a considerable evidence gap on the prevalence and change in breastfeeding practices by type—exclusive or complementary—few studies [18, 198] have found associations between breastfeeding cessation or non-initiation with lack of support and fear of vertical transmission.
Significant associations between specific parenting styles and children’s behaviours have been reported in the literature [127, 148, 152, 169, 183, 184] pointing to the detrimental effect of parental behavioural traits such as inconsistency and inflexibility [44, 148, 152]. Those studies describe a cycle where parental and infant mental suffering and burnout are bidirectionally associated with dysfunctional family dynamics. Correspondingly, they also suggest that greater use of constructive parenting strategies, such as supportive and consistent practices, are associated with greater family cohesion. Such strategies are predicted by parental emotion regulation capacity and psychological flexibility, which in turn was found to be highly associated with parental stress levels. Importantly, coercive practices were found to increase in situations of high parental stress [128, 152, 168, 171, 183, 184].
Finally, parental practices concerning children with disabilities or debilitating health conditions during the pandemic were reported in few studies [3, 12, 15, 17, 27, 30, 75, 123, 139, 143, 175] in which the main challenges identified by caregivers were routine disruptions accompanied by loss of access to stimulating activities, increased behavioural difficulties, health concerns regarding COVID-19 infection, loss of in-person rehabilitation support activities, and decreased access and quality of care services offered to children within overburdened health systems.
Discussion
Summary of evidence
Our findings suggest that there is a much larger body of evidence so far concerning the impact of the pandemic on maternal mental health than there is on early childhood development, and even less so on parental practices. We hypothesize that this imbalance is partially due to differing degrees of difficulty in accessing and enrolling participants in empirical studies. For instance, it might be overall easier to recruit women who attend health services based on convenience sampling, or to launch an online open survey through social media platforms, than it is to enroll children during periods of school and daycare center closures. Furthermore, in order to examine parental practices based on observed behavior it is often necessary to access households in person, which poses additional health risks of COVID contamination to both study participants and researchers.
Certainly, measuring the magnitude of the pandemic impact on each outcome category exceeds the scope of this review. However, some relevant findings synthesizing global burden estimates have been pointed out by specific studies. O'Driscoll et al. [144] estimated age-specific mortality and immunity patterns of SARS-CoV-2 across 45 countries, demonstrating that the age distribution of excess deaths due to COVID-19 in age groups younger than 65 years old was consistent across different settings. That study concluded that the infection fatality ratio (IFR) was lowest among children 5–9 years old (> 0.001), closely followed by children younger than five (> 0.01); male children’s IFR ranked slightly higher than females in both age groups [144].
Importantly, Hillis et al. [82] analysed global estimates of orphanhood associated with COVID-19, finding that between March 2020 and April 2021, approximately 1.134.000 children (95% CI: 884.000 – 1.185.000) experienced the death of primary caregivers, while 1.562.000 children (95% CI: 1.299.000 – 1.683.000) lost at least one primary or secondary caregiver. The study has identified countries with high rates of primary caregiver deaths per 1,000 children, including Peru (10.2), South Africa (5.1), Mexico (3.5), Brazil (2.4), Colombia (2.3), Iran (1.7), USA (1.5), Argentina (1.1), and Russia (1.0). It also estimated that between two to five more children experienced the death of fathers than mothers [82]. These alarming findings regarding orphanhood highlight the need for longitudinal studies that are capable of examining the compound impact of the pandemic on child development over time, across diverse sociocultural contexts.
This study addresses an evidence gap concerning the analysis of the impact of the COVID-19 pandemic on all three fields, namely, maternal mental health, early childhood development, and parental practices, globally. The breadth of our review lies not only in the diversity of themes explored by empirical research, case reports, and literature reviews within each field but also in the large period of publication determined by our inclusion criteria, from January 1st, 2020, until June 9th, 2021, capturing the development of relevant research efforts during diverse stages of the pandemic, across the world.
Regarding this global research effort, three points should be highlighted. Firstly, the deeply unequal contribution of evidence concerning countries’ income level groups, with as much as 63.19% of empirical research studies and case reports having been conducted in high-income countries, and as little as 0.97% originating from low-income countries. Secondly, the majority (67.4%) of primary research studies has employed a cross-sectional design, even when addressing etiologic questions concerning potential determinants of negatively impacted states of maternal mental health, childhood development, or parenting. Thirdly, convenience sampling methods have been utilized by almost half of all primary research studies (48.8%); specifically, 34% of studies recruited participants exclusively via open-access links disseminated through online social platforms.
Some considerations should be made based on these findings. Concerning the evidence gap based on country-level income group: there is relevant evidence [32] suggesting that stillbirth and maternal mortality rates have sharply increased in LMICs during the pandemic, and yet only 6% of the selected studies has been conducted within low and lower-middle income countries. The co-occurrence of inconsistent and misguided recommendations on key parental practices such as breastfeeding and neonatal care [199], and the general convergence of risk factors, sometimes within ongoing humanitarian crises, especially endangers the wellbeing of mothers and young children in LMICs. Without sufficient quality data it is impossible to estimate, and even more difficult to effectively act upon, this complex scenario which poses the threat of lifelong negative consequences on the health of young children currently experiencing toxic stress and deprivation during the first years of their life. The second consideration regards the overall quality and generalizability of evidence produced by most research efforts within all three fields, since the pandemic onset. The gap in longitudinal data is expected, considering the relative novelty of the phenomenon. However, it certainly hinders the possibility to grasp mechanistic effects better informing health outcomes, creating added difficulties to the timely monitoring of important changes on the magnitude of the pandemic impact on population health status. Finally, the massive employment of low-quality sampling methods, compromising internal and external validity of evidence across fields, clearly signals the need for more concerted research efforts to support the implementation of public policies that prioritize the most serious problems for maternal and child health. Importantly, there are considerable ethical and methodological difficulties in robustly assessing the pandemic impact on specific variables, such as intimate partner violence, abusive parental practices, or maternal-infant attachment quality. To minimize the risk of bias, the same population should be assessed before and during the pandemic, utilizing the same methods and instruments, which poses large limitations on research efforts. Additionally, there is the added barrier of assessing data on intrafamilial violence during periods where lockdowns have been imposed. In such times, not only do victims only do victims frequently havefrequently have no alternative except cohabitating with aggressors, but also pre-existing protective institutional resources may have been limited, for instance, by redirected investments to mitigate the burden of disease associated with COVID-19. Both conditions seem to stimulate participants’ hesitation of disclosing sensitive information regarding intrafamilial violence, even when anonymized. Unfortunately, even after considering these potential barriers to more accurate estimates, existing data on the subject show alarmingly increased rates of IPV and child abuse during the pandemic.
We would like to highlight four important findings from our study. First, because of the diverse and various pathways through which the mental health of caregivers might be directly correlated with the health and development of young children under their care, there are equivalently various measures that can be taken to foster a global improvement of outcomes within this relationship.
Second, even though certain social measures that are needed to mitigate the spread of COVID-19, such as physical isolation, might contribute as stressors to the wellbeing of caregivers and children [1759, 155, 319, 359, 639, 832, 879, 889, 1010, 1113, 1354, 1424, 1519, 171, 394, 1204, 1447, 1606, 1756, 1519, 234, 443, 324, 262, 361, 137, 343, 398, 1204, 1807, 2099, 639] this review found evidence that the added financial burden [831, 1515, 570, 517, 662, 692, 1073, 1140, 1377, 1519, 1462, 2107, 1351, 817, 928, 975, 186] and loss of access to health services [1354, 330, 879, 832, 176, 852, 1186, 398, 2174, 2192, 2123] seem to be component causes that are equally relevant in producing the reported negative outcomes in maternal mental health and ECD. More data is needed to estimate the differential impact of the pandemic on our outcome categories of interest in a scenario where physical distancing measures were adopted, within comparable populations, and that have experienced different levels of added financial hardship, employment, and food insecurity, and access barriers to health care throughout the pandemic.
Third, although the compound effect of various risk factors on the mental health and wellbeing of caregivers and children is highly dependent on local and dynamic circumstances during the pandemic, pre-existing socio-cultural conditions, such as gender inequality, seem to have been exacerbated in the absence of institutional and relational support resources, e.g., school and daycare centres closures [234, 443, 324, 262, 361, 145, 960, 1634, 1468, 1855, 1145]. The overburden created by unbalanced childcare and housework workloads performed by female caregivers appeared as one of the most influential risk factors for increased maternal stress, decreased maternal mental health, and parenting styles that are detrimental to ECD [466, 472, 775, 1743, 290, 384, 284, 774, 1409, 1920, 1143, 1473, 1059, 1056, 707, 582, 600, 662, 831, 186, 137, 1045, 1351, 1399].
Lastly, global estimates on orphanhood due to COVID-19 [82] identify the urgent need to map and timely address, both through international and local collaborations, this critical situation experienced by children in key developmental stages, especially regarding institutionalisation and immediate care needs.
Limitations
The assumption of mothers as the most frequent primary caregiver has implications on our findings. We have not systematically retrieved data on the impact of the pandemic on the mental health of alternative and/or secondary caregivers, which appears as an important component of constructive parenting practices and healthy family dynamics in the literature. Furthermore, even though the physical health of caregivers during the pandemic, especially pregnant and postpartum women, is intimately connected to their mental health status, such investigation surpasses the scope of this review. Finally, our search strategy did not include controlled vocabulary terms referring to specific parenting practices, such as “breastfeeding” or “home schooling”.
Overall, data on maternal mental health was more voluminous, structured, and easily accessible than on ECD, and even more so for parental practices. Most data concerning ECD was indirectly reported by caregivers, which poses a larger liability to information bias. These limitations, along with the frequent use of low-quality sampling methods, signal the added barriers to recruitment and selection of participants to research studies during the pandemic, particularly so during periods of lockdowns.
Conclusions
The central conclusion of this review is that the inherent interplay between the mental health of caregivers and the health and development of young children under their care, mediated by parenting practices, is deeply permeable to social determinants. While this finding is certainly echoed by a robust body of literature predating the pandemic, our review contributes to the understanding of the extent to which the pandemic has exacerbated previous conditions of vulnerability, frequently creating interactions between risk factors that deeply magnify the effects of inequality on the health and wellbeing of specific populations.
Availability of data and materials
Not applicable.
References
Abou Ghayda, R., Li, H., Lee, K. H., Lee, H. W., Hong, S. H., Kwak, M. Shin, J. I. (2020). COVID-19 and Adverse Pregnancy Outcome: A Systematic Review of 104 Cases. J Clin Med, 9(11). https://doi.org/10.3390/jcm9113441
Achterberg M, Dobbelaar S, Boer OD, Crone EA. Perceived stress as mediator for longitudinal effects of the COVID-19 lockdown on wellbeing of parents and children. Sci Rep. 2021;11(1):2971. https://doi.org/10.1038/s41598-021-81720-8.
AdemhanTural D, Emiralioglu N, TuralHesapcioglu S, Karahan S, Ozsezen B, Sunman B, Kiper N. Psychiatric and general health effects of COVID-19 pandemic on children with chronic lung disease and parents’ coping styles. Pediatr Pulmonol. 2020;55(12):3579–86. https://doi.org/10.1002/ppul.25082.
Ahorsu, D. K., Imani, V., Lin, C. Y., Timpka, T., Broström, A., Updegraff, J. A, Pakpour, A. H. (2020). Associations Between Fear of COVID-19, Mental Health, and Preventive Behaviours Across Pregnant Women and Husbands: An Actor-Partner Interdependence Modelling. Int J Ment Health Addict, 1–15. https://doi.org/10.1007/s11469-020-00340-x
AksoyDerya Y, Altiparmak S, AkÇa E, GÖkbulut N, Yilmaz AN. Pregnancy and birth planning during COVID-19: The effects of tele-education offered to pregnant women on prenatal distress and pregnancy-related anxiety. Midwifery. 2020;92:102877. https://doi.org/10.1016/j.midw.2020.102877.
Alsuhaibani M, Alaqeel A. Impact of the COVID-19 pandemic on routine childhood immunization in Saudi Arabia. Vaccines. 2020;8(4):581.
Altena E, Baglioni C, Espie CA, Ellis J, Gavriloff D, Holzinger B, Riemann D. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: Practical recommendations from a task force of the European CBT-I Academy. J Sleep Res. 2020;29(4):e13052.
Amaral, W. N. D., Moraes, C. L., Rodrigues, A., Noll, M., Arruda, J. T., & Mendonça, C. R. (2020). Maternal Coronavirus Infections and Neonates Born to Mothers with SARS-CoV-2: A Systematic Review. Healthcare (Basel), 8(4). https://doi.org/10.3390/healthcare8040511
Ares G, Bove I, Vidal L, Brunet G, Fuletti D, Arroyo Á, Blanc MV. The experience of social distancing for families with children and adolescents during the coronavirus (COVID-19) pandemic in Uruguay: Difficulties and opportunities. Child Youth Serv Rev. 2021;121:105906. https://doi.org/10.1016/j.childyouth.2020.105906.
Ashini A, Alsoufi A, Elhadi M. Parental perception of neonatal ICU visitation during the COVID-19 pandemic. Int J Gynaecol Obstet. 2021;153(3):554–5. https://doi.org/10.1002/ijgo.13650.
Auðardóttir AM, Rúdólfsdóttir AG. Chaos ruined the children’s sleep, diet and behaviour: Gendered discourses on family life in pandemic times. Gend Work Organ. 2020. https://doi.org/10.1111/gwao.12519.
Ayas, M., Ali Al Amadi, A. M. H., Khaled, D., & Alwaa, A. M. (2020). Impact of COVID-19 on the access to hearing health care services for children with cochlear implants: A survey of parents. F1000Research, 9. https://doi.org/10.12688/f1000research.24915.1
Bao, X., Qu, H., Zhang, R., & Hogan, T. P. (2020). Modeling Reading Ability Gain in Kindergarten Children during COVID-19 School Closures. International Journal of Environmental Research and Public Health, 17(17). https://doi.org/10.3390/ijerph17176371
Bender WR, Srinivas S, Coutifaris P, Acker A, Hirshberg A. The Psychological Experience of Obstetric Patients and Health Care Workers after Implementation of Universal SARS-CoV-2 Testing. Am J Perinatol. 2020;37(12):1271–9. https://doi.org/10.1055/s-0040-1715505.
Bentenuto A, Mazzoni N, Giannotti M, Venuti P, de Falco S. Psychological impact of Covid-19 pandemic in Italian families of children with neurodevelopmental disorders. Res Dev Disabil. 2021;109:103840. https://doi.org/10.1016/j.ridd.2020.103840.
Boivin J, Harrison C, Mathur R, Burns G, Pericleous-Smith A, Gameiro S. Patient experiences of fertility clinic closure during the COVID-19 pandemic: appraisals, coping and emotions. Hum Reprod. 2020;35(11):2556–66.
Brisca G, Vagelli G, Tagliarini G, Rotulo A, Pirlo D, Romanengo M, Piccotti E. The impact of COVID-19 lockdown on children with medical complexity in pediatric emergency department. Am J Emerg Med. 2021;42:225–7. https://doi.org/10.1016/j.ajem.2020.11.066.
Brown, A., & Shenker, N. (2020). Experiences of breastfeeding during COVID-19: Lessons for future practical and emotional support. Maternal & Child Nutrition, e13088. https://doi.org/10.1111/mcn.13088
Brown, S. M., Doom, J. R., Lechuga-Peña, S., Watamura, S. E., & Koppels, T. (2020). Stress and parenting during the global COVID-19 pandemic. Child Abuse and Neglect, 104699. https://doi.org/10.1016/j.chiabu.2020.104699
Calvano, C., Engelke, L., Di Bella, J., Kindermann, J., Renneberg, B., & Winter, S. M. (2021). Families in the COVID-19 pandemic: parental stress, parent mental health and the occurrence of adverse childhood experiences-results of a representative survey in Germany. European Child and Adolescent Psychiatry, 1–13. https://doi.org/10.1007/s00787-021-01739-0
Cameron EE, Joyce KM, Delaquis CP, Reynolds K, Protudjer JLP, Roos LE. Maternal psychological distress & mental health service use during the COVID-19 pandemic. J Affect Disord. 2020;276:765–74. https://doi.org/10.1016/j.jad.2020.07.081.
Campagnaro R, Collet GO, Andrade MP, Salles J, CalvoFracasso ML, Scheffel DLS, Santin GC. COVID-19 pandemic and pediatric dentistry: Fear, eating habits and parent’s oral health perceptions. Child Youth Serv Rev. 2020;118:105469. https://doi.org/10.1016/j.childyouth.2020.105469.
Capobianco G, Saderi L, Aliberti S, Mondoni M, Piana A, Dessole F, Sotgiu G. COVID-19 in pregnant women: A systematic review and meta-analysis. Eur J Obstetrics, Gynecol Reprod Biol. 2020;252:543–58. https://doi.org/10.1016/j.ejogrb.2020.07.006.
Carroll N, Sadowski A, Laila A, Hruska V, Nixon M, Ma DW, Haines J. The impact of COVID-19 on health behavior, stress, financial and food security among middle to high income Canadian families with young children. Nutrients. 2020;12(8):2352.
Carroll, N., Sadowski, A., Laila, A., Hruska, V., Nixon, M., Ma, D. W. L., . . . On Behalf Of The Guelph Family Health, S. (2020). The Impact of COVID-19 on Health Behavior, Stress, Financial and Food Security among Middle to High Income Canadian Families with Young Children. Nutrients, 12(8). https://doi.org/10.3390/nu12082352
Cellini N, Di Giorgio E, Mioni G, Di Riso D. Sleep and Psychological Difficulties in Italian School-Age Children During COVID-19 Lockdown. J Pediatr Psychol. 2021;46(2):153–67. https://doi.org/10.1093/jpepsy/jsab003.
Chan, R. C. H., & Fung, S. C. (2021). Elevated Levels of COVID-19-Related Stress and Mental Health Problems Among Parents of Children with Developmental Disorders During the Pandemic. Journal of Autism and Developmental Disorders, 1–12. https://doi.org/10.1007/s10803-021-05004-w
Chapman GE, Ishlek I, Spoors J. Google search behaviour relating to perinatal mental wellbeing during the United Kingdom’s first COVID-19 lockdown period: a warning for future restrictions. Arch Womens Ment Health. 2021;24(4):681–6.
Chasson, M., Taubman-Ben-Ari, O., & Abu-Sharkia, S. (2020). Jewish and Arab pregnant women's psychological distress during the COVID-19 pandemic: the contribution of personal resources. Ethnicity and Health, 1–13. https://doi.org/10.1080/13557858.2020.1815000
Chen, S. Q., Chen, S. D., Li, X. K., & Ren, J. (2020). Mental Health of Parents of Special Needs Children in China during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 17(24). https://doi.org/10.3390/ijerph17249519
Cheng, Z., Mendolia, S., Paloyo, A. R., Savage, D. A., & Tani, M. (2021). Working parents, financial insecurity, and childcare: mental health in the time of COVID-19 in the UK. Rev Econ Househ, 1–22. https://doi.org/10.1007/s11150-020-09538-3
Chmielewska B, Barratt I, Townsend R, Kalafat E, van der Meulen J, Gurol-Urganci I, Khalil A. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: a systematic review and meta-analysis. Lancet Glob Health. 2021;9(6):e759–72. https://doi.org/10.1016/s2214-109x(21)00079-6.
Choi, J., Park, Y., Kim, H. E., Song, J., Lee, D., Lee, E., . . . Lee, Y. (2021). Daily Life Changes and Life Satisfaction among Korean School-Aged Children in the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(6). https://doi.org/10.3390/ijerph18063324
Chung, G., Lanier, P., & Wong, P. Y. J. (2020). Mediating Effects of Parental Stress on Harsh Parenting and Parent-Child Relationship during Coronavirus (COVID-19) Pandemic in Singapore. J Fam Violence, 1–12. https://doi.org/10.1007/s10896-020-00200-1
Cohodes EM, McCauley S, Gee DG. Parental Buffering of Stress in the Time of COVID-19: Family-Level Factors May Moderate the Association Between Pandemic-Related Stress and Youth Symptomatology. Res Child Adolesc Psychopathol. 2021;49(7):935–48. https://doi.org/10.1007/s10802-020-00732-6.
Congdon JL, Kair LR, Flaherman VJ, Wood KE, LoFrumento MA, Nwaobasi-Iwuh E, Phillipi CA. Management and Early Outcomes of Neonates Born to WoHospitals. Am J Perinatol. 2021;38(6):622–31.
Connell, C. M., & Strambler, M. J. (2021). Experiences With COVID-19 Stressors and Parents' Use of Neglectful, Harsh, and Positive Parenting Practices in the Northeastern United States. Child Maltreat, 10775595211006465. https://doi.org/10.1177/10775595211006465
Conti, M. G., Natale, F., Stolfi, I., Pedicino, R., Boscarino, G., Ajassa, C., . . . Terrin, G. (2021). Consequences of Early Separation of Maternal-Newborn Dyad in Neonates Born to SARS-CoV-2 Positive Mothers: An Observational Study. International Journal of Environmental Research and Public Health, 18(11). https://doi.org/10.3390/ijerph18115899
Costoya, V., Echeverría, L., Edo, M., Rocha, A., & Thailinger, A. (2021). Gender Gaps within Couples: Evidence of Time Re-allocations during COVID-19 in Argentina. J Fam Econ Issues, 1–14. https://doi.org/10.1007/s10834-021-09770-8
Craig L, Churchill B. Dual-earner Parent Couples’ Work and Care during COVID-19. Gend Work Organ. 2020. https://doi.org/10.1111/gwao.12497.
Cui S, Zhang C, Wang S, Zhang X, Wang L, Zhang L, Zhou X. Experiences and Attitudes of Elementary School Students and Their Parents Toward Online Learning in China During the COVID-19 Pandemic: Questionnaire Study. J Med Int Res. 2021;23(5):e24496. https://doi.org/10.2196/24496.
Cui Y, Li Y, Zheng Y. Mental health services for children in China during the COVID-19 pandemic: results of an expert-based national survey among child and adolescent psychiatric hospitals. Eur Child Adolesc Psychiatry. 2020;29(6):743–8. https://doi.org/10.1007/s00787-020-01548-x.
Cusinato, M., Iannattone, S., Spoto, A., Poli, M., Moretti, C., Gatta, M., & Miscioscia, M. (2020). Stress, Resilience, and Well-Being in Italian Children and Their Parents during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 17(22). https://doi.org/10.3390/ijerph17228297
Daks JS, Peltz JS, Rogge RD. Psychological flexibility and inflexibility as sources of resiliency and risk during a pandemic: Modeling the cascade of COVID-19 stress on family systems with a contextual behavioral science lens. J Contextual Behav Sci. 2020;18:16–27. https://doi.org/10.1016/j.jcbs.2020.08.003.
Daulay N. Home education for children with autism spectrum disorder during the COVID-19 pandemic: Indonesian mothers experience. Res Dev Disabil. 2021;114:103954. https://doi.org/10.1016/j.ridd.2021.103954.
de Sá, C. D. S. C., Pombo, A., Luz, C., Rodrigues, L. P., & Cordovil, R. (2020). Covid-19 social isolation in Brazil: Effects on the physical activity routine of families with children. Revista Paulista de Pediatria, 39. https://doi.org/10.1590/1984-0462/2021/39/2020159
Del Boca, D., Oggero, N., Profeta, P., & Rossi, M. (2020). Women's and men's work, housework and childcare, before and during COVID-19. Rev Econ Househ, 1–17. https://doi.org/10.1007/s11150-020-09502-1
Dellagiulia A, Lionetti F, Fasolo M, Verderame C, Sperati A, Alessandri G. Early impact of COVID-19 lockdown on children’s sleep: A 4-week longitudinal study. J Clin Sleep Med. 2020;16(9):1639–40. https://doi.org/10.5664/jcsm.8648.
DeYoung SE, Mangum M. Pregnancy, Birthing, and Postpartum Experiences During COVID-19 in the United States. Front Sociol. 2021;6:611212. https://doi.org/10.3389/fsoc.2021.611212.
Dhiman, S., Sahu, P. K., Reed, W. R., Ganesh, G. S., Goyal, R. K., & Jain, S. (2020). Impact of COVID-19 outbreak on mental health and perceived strain among caregivers tending children with special needs. Research in Developmental Disabilities, 107. https://doi.org/10.1016/j.ridd.2020.103790
Di Mascio D, Khalil A, Saccone G, Rizzo G, Buca D, Liberati M, D’Antonio F. Am J Obstet Gynecol MFM. 2020;2(2):100107. https://doi.org/10.1016/j.ajogmf.2020.100107.
Di Riso D, Spaggiari S, Cambrisi E, Ferraro V, Carraro S, Zanconato S. Psychosocial impact of Covid-19 outbreak on Italian asthmatic children and their mothers in a post lockdown scenario. Sci Rep. 2021;11(1):9152. https://doi.org/10.1038/s41598-021-88152-4.
Dickerson J, Kelly B, Lockyer B, Bridges S, Cartwright C, Willan K, Pickett KE. Experiences of lockdown during the Covid-19 pandemic: descriptive findings from a survey of families in the Born in Bradford study. Wellcome Open Res. 2020;5:228. https://doi.org/10.12688/wellcomeopenres.16317.2.
Ding W, Lu J, Zhou Y, Wei W, Zhou Z, Chen M. Knowledge, attitudes, practices, and influencing factors of anxiety among pregnant women in Wuhan during the outbreak of COVID-19: a cross-sectional study. BMC Pregnancy Childbirth. 2021;21(1):80. https://doi.org/10.1186/s12884-021-03561-7.
Diriba K, Awulachew E, Getu E. The effect of coronavirus infection (SARS-CoV-2, MERS-CoV, and SARS-CoV) during pregnancy and the possibility of vertical maternal-fetal transmission: a systematic review and meta-analysis. Eur J Med Res. 2020;25(1):39. https://doi.org/10.1186/s40001-020-00439-w.
Dumbre DU, Ramesh S, Chavan R, Jabade M. A descriptive study to assess the stress and coping mechanism due to lockdown among school going children. Indian J Forensic Med Toxicology. 2020;14(4):3590–7. https://doi.org/10.37506/ijfmt.v14i4.12186.
El-Osta A, Alaa A, Webber I, RiboliSasco E, Bagkeris E, Millar H, Majeed A. How is the COVID-19 lockdown impacting the mental health of parents of school-age children in the UK? BMJ Open. 2021;11(5):e043397. https://doi.org/10.1136/bmjopen-2020-043397.
Faccioli S, Lombardi F, Bellini P, Costi S, Sassi S, Pesci MC. How did italian adolescents with disability and parents deal with the covid-19 emergency? Int J Environ Res Public Health. 2021;18(4):1–13. https://doi.org/10.3390/ijerph18041687.
Fan S, Guan J, Cao L, Wang M, Zhao H, Chen L, Yan L. Psychological effects caused by COVID-19 pandemic on pregnant women: A systematic review with meta-analysis. Asian J Psychiatr. 2021;56:102533. https://doi.org/10.1016/j.ajp.2020.102533.
Farewell CV, Jewell J, Walls J, Leiferman JA. A Mixed-Methods Pilot Study of Perinatal Risk and Resilience During COVID-19. J Prim Care Community Health. 2020;11:2150132720944074. https://doi.org/10.1177/2150132720944074.
Farghaly MAA, Kupferman F, Castillo F, Kim RM. Characteristics of Newborns Born to SARS-CoV-2-Positive Mothers: A Retrospective Cohort Study. Am J Perinatol. 2020;37(13):1310–6. https://doi.org/10.1055/s-0040-1715862.
Farhadi R, Mehrpisheh S, Philip RK. Mobile-Assisted Virtual Bonding Enables Breast Milk Supply in Critically Ill Mothers With COVID-19: A Reflection on the Feasibility of Telelactation. Cureus. 2021;13(3):e13699. https://doi.org/10.7759/cureus.13699.
Fernandes DV, Canavarro MC, Moreira H. Postpartum during COVID-19 pandemic: Portuguese mothers’ mental health, mindful parenting, and mother-infant bonding. J Clin Psychol. 2021. https://doi.org/10.1002/jclp.23130.
Ferns SJ, Gautam S, Hudak ML. COVID-19 and Gender Disparities in Pediatric Cardiologists with Dependent Care Responsibilities. Am J Cardiol. 2021;147:137–42. https://doi.org/10.1016/j.amjcard.2021.02.017.
Ferrante, M. J., Goldsmith, J., Tauriello, S., Epstein, L. H., Leone, L. A., & Anzman-Frasca, S. (2021a). Food Acquisition and Daily Life for U.S. Families with 4-to 8-Year-Old Children during COVID-19: Findings from a Nationally Representative Survey. International Journal of Environmental Research and Public Health, 18(4). https://doi.org/10.3390/ijerph18041734
Ferrante MJ, Goldsmith J, Tauriello S, Epstein LH, Leone LA, FrascaAnzman S. Food acquisition and daily life for U.S. families with 4-to 8-year-old children during COVID-19: Findings from a nationally representative survey [Article]. Int J Environ Res Public Health. 2021;18(4):1–15. https://doi.org/10.3390/ijerph18041734.
Ferrazzi E, Frigerio L, Savasi V, Vergani P, Prefumo F, Barresi S, Villa A. Vaginal delivery in SARS-CoV-2-infected pregnant women in Northern Italy: a retrospective analysis. BJOG. 2020;127(9):1116–21. https://doi.org/10.1111/1471-0528.16278.
Fisher, A. P., Patronick, J., Gerhardt, C. A., Radonovich, K., Salloum, R., & Wade, S. L. (2021). Impact of COVID-19 on adolescent and emerging adult brain tumor survivors and their parents. Pediatric Blood & Cancer, e29116. https://doi.org/10.1002/pbc.29116
Forbes, L. K., Lamar, M. R., Speciale, M., & Donovan, C. (2021). Mothers' and fathers' parenting attitudes during COVID-19. Current Psychology (New Brunswick, N.J.), 1–10. https://doi.org/10.1007/s12144-021-01605-x
Fosco GM, Sloan CJ, Fang S, Feinberg ME. Family vulnerability and disruption during the COVID-19 pandemic: prospective pathways to child maladjustment. J Child Psychol Psychiatry. 2021. https://doi.org/10.1111/jcpp.13458.
Franchi M, Del Piccolo L, Bosco M, Tosadori C, Casarin J, Laganà AS, Garzon S. COVID-19 and mental health in the obstetric population: a lesson from a case of puerperal psychosis. Minerva Ginecol. 2020;72(5):355–7. https://doi.org/10.23736/s0026-4784.20.04606-7.
Gadermann AC, Thomson KC, Richardson CG, Gagné M, McAuliffe C, Hirani S, Jenkins E. Examining the impacts of the COVID-19 pandemic on family mental health in Canada: findings from a national cross-sectional study. BMJ Open. 2021;11(1):e042871. https://doi.org/10.1136/bmjopen-2020-042871.
Gassman-Pines, A., Ananat, E. O., & Fitz-Henley, J., 2nd. (2020). COVID-19 and Parent-Child Psychological Well-being. Pediatrics, 146(4). https://doi.org/10.1542/peds.2020-007294
Gildner TE, Laugier EJ, Thayer ZM. Exercise routine change is associated with prenatal depression scores during the COVID-19 pandemic among pregnant women across the United States. PLoS ONE. 2020;15(12):e0243188. https://doi.org/10.1371/journal.pone.0243188.
Grumi, S., Provenzi, L., Gardani, A., Aramini, V., Dargenio, E., Naboni, C., . . . Borgatti, R. (2020). Rehabilitation services lockdown during the COVID-19 emergency: the mental health response of caregivers of children with neurodevelopmental disabilities. Disability and Rehabilitation, 1–6. https://doi.org/10.1080/09638288.2020.1842520
Guo, J., De Carli, P., Lodder, P., Bakermans-Kranenburg, M. J., & Riem, M. M. E. (2021). Maternal mental health during the COVID-19 lockdown in China, Italy, and the Netherlands: a cross-validation study. Psychological Medicine, 1–11. https://doi.org/10.1017/s0033291720005504
Gur RE, White LK, Waller R, Barzilay R, Moore TM, Kornfield S, Elovitz MA. The Disproportionate Burden of the COVID-19 Pandemic Among Pregnant Black Women. Psychiatry Res. 2020;293:113475. https://doi.org/10.1016/j.psychres.2020.113475.
Hailemariam S, Agegnehu W, Derese M. Exploring COVID-19 Related Factors Influencing Antenatal Care Services Uptake: A Qualitative Study among Women in a Rural Community in Southwest Ethiopia. J Prim Care Community Health. 2021;12:2150132721996892. https://doi.org/10.1177/2150132721996892.
Halley MC, Mathews KS, Diamond LC, Linos E, Sarkar U, Mangurian C, Jagsi R. The Intersection of Work and Home Challenges Faced by Physician Mothers During the Coronavirus Disease 2019 Pandemic: A Mixed-Methods Analysis. J Womens Health (Larchmt). 2021;30(4):514–24. https://doi.org/10.1089/jwh.2020.8964.
Hamadani JD, Hasan MI, Baldi AJ, Hossain SJ, Shiraji S, Bhuiyan MSA, Pasricha SR. Immediate impact of stay-at-home orders to control COVID-19 transmission on socioeconomic conditions, food insecurity, mental health, and intimate partner violence in Bangladeshi women and their families: an interrupted time series. Lancet Glob Health. 2020;8(11):e1380–9. https://doi.org/10.1016/s2214-109x(20)30366-1.
Hessami, K., Romanelli, C., Chiurazzi, M., & Cozzolino, M. (2020). COVID-19 pandemic and maternal mental health: a systematic review and meta-analysis. Journal of Maternal-Fetal & Neonatal Medicine, 1–8. https://doi.org/10.1080/14767058.2020.1843155
Hillis SD, et al. Global minimum estimates of children affected by COVID-19-associated orphanhood and deaths of caregivers: a modelling study. Lancet. 2021;398(10298):391–402. https://doi.org/10.1016/S0140-6736(21)01253-8.
Hjálmsdóttir, A., & Bjarnadóttir, V. S. (2020). "I have turned into a foreman here at home." Families and work-life balance in times of Covid-19 in a gender equality paradise. Gend Work Organ. https://doi.org/10.1111/gwao.12552
Horiuchi S, Shinohara R, Otawa S, Akiyama Y, Ooka T, Kojima R, Yamagata Z. Caregivers’ mental distress and child health during the COVID-19 outbreak in Japan. PLoS ONE. 2020;15(12):e0243702. https://doi.org/10.1371/journal.pone.0243702.
Islam MM, Poly TN, Walther BA, Yang HC, Wang CW, Hsieh WS, Jack Li YC. Clinical Characteristics and Neonatal Outcomes of Pregnant Patients With COVID-19: A Systematic Review. Front Med (Lausanne). 2020;7:573468. https://doi.org/10.3389/fmed.2020.573468.
Jafari, M., Pormohammad, A., Sheikh Neshin, S. A., Ghorbani, S., Bose, D., Alimohammadi, S., . . . Zarei, M. (2021). Clinical characteristics and outcomes of pregnant women with COVID-19 and comparison with control patients: A systematic review and meta-analysis. Reviews in Medical Virology, e2208. https://doi.org/10.1002/rmv.2208
Jansen E, Thapaliya G, Aghababian A, Sadler J, Smith K, Carnell S. Parental stress, food parenting practices and child snack intake during the COVID-19 pandemic. Appetite. 2021;161:105119. https://doi.org/10.1016/j.appet.2021.105119.
Juan J, Gil MM, Rong Z, Zhang Y, Yang H, Poon LC. Effect of coronavirus disease 2019 (COVID-19) on maternal, perinatal and neonatal outcome: systematic review. Ultrasound Obstet Gynecol. 2020;56(1):15–27. https://doi.org/10.1002/uog.22088.
Kahyaoglu Sut H, Kucukkaya B. Anxiety, depression, and related factors in pregnant women during the COVID-19 pandemic in Turkey: A web-based cross-sectional study. Perspect Psychiatr Care. 2020. https://doi.org/10.1111/ppc.12627.
Kassaw C, Pandey D. The prevalence of general anxiety disorder and its associated factors among women’s attending at the perinatal service of Dilla University referral hospital, Dilla town, Ethiopia, April 2020 in Covid pandemic. Heliyon. 2020;6(11):e05593. https://doi.org/10.1016/j.heliyon.2020.e05593.
Khoury JE, Atkinson L, Bennett T, Jack SM, Gonzalez A. COVID-19 and mental health during pregnancy: The importance of cognitive appraisal and social support. J Affect Disord. 2021;282:1161–9. https://doi.org/10.1016/j.jad.2021.01.027.
Kinser PA, Jallo N, Amstadter AB, Thacker LR, Jones E, Moyer S, Salisbury AL. Depression, Anxiety, Resilience, and Coping: The Experience of Pregnant and New Mothers During the First Few Months of the COVID-19 Pandemic. J Womens Health (Larchmt). 2021;30(5):654–64. https://doi.org/10.1089/jwh.2020.8866.
Kotlar B, Gerson E, Petrillo S, Langer A, Tiemeier H. The impact of the COVID-19 pandemic on maternal and perinatal health: a scoping review. Reprod Health. 2021;18(1):1–39.
Kovler, M. L., Ziegfeld, S., Ryan, L. M., Goldstein, M. A., Gardner, R., Garcia, A. V., & Nasr, I. W. (2020). Increased proportion of physical child abuse injuries at a level I pediatric trauma center during the Covid-19 pandemic. Child Abuse and Neglect, 104756. https://doi.org/10.1016/j.chiabu.2020.104756
Kracht CL, Katzmarzyk PT, Staiano AE. Household chaos, maternal stress, and maternal health behaviors in the United States during the COVID-19 outbreak. Womens Health (Lond). 2021;17:17455065211010656. https://doi.org/10.1177/17455065211010655.
Lawson, M., Piel, M. H., & Simon, M. (2020). Child Maltreatment during the COVID-19 Pandemic: Consequences of Parental Job Loss on Psychological and Physical Abuse Towards Children. Child Abuse and Neglect, 104709. https://doi.org/10.1016/j.chiabu.2020.104709
Lebel C, MacKinnon A, Bagshawe M, Tomfohr-Madsen L, Giesbrecht G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J Affect Disord. 2020;277:5–13. https://doi.org/10.1016/j.jad.2020.07.126.
Lee, S. J., Ward, K. P., Chang, O. D., & Downing, K. M. (2020). Parenting Activities and the Transition to Home-based Education During the COVID-19 Pandemic. Child Youth Serv Rev, 105585. https://doi.org/10.1016/j.childyouth.2020.105585
Lee, S. J., Ward, K. P., Lee, J. Y., & Rodriguez, C. M. (2021). Parental Social Isolation and Child Maltreatment Risk during the COVID-19 Pandemic. J Fam Violence, 1–12. https://doi.org/10.1007/s10896-020-00244-3
Leeb RT, Bitsko RH, Radhakrishnan L, Martinez P, Njai R, Holland KM. Mental Health-Related Emergency Department Visits Among Children Aged <18 Years During the COVID-19 Pandemic - United States, January 1-October 17, 2020. MMWR: Morb Mortal Wkly Rep. 2020;69(45):1675–80. https://doi.org/10.15585/mmwr.mm6945a3.
Lemieux, R., Garon-Bissonnette, J., Loiselle, M., Martel, É., Drouin-Maziade, C., & Berthelot, N. (2020). [Not Available]. Canadian Journal of Psychiatry. Revue Canadienne de Psychiatrie, 706743720963917. https://doi.org/10.1177/0706743720963917
Li C, Huo L, Wang R, Qi L, Wang W, Zhou X, Zhang X. The prevalence and risk factors of depression in prenatal and postnatal women in China with the outbreak of Corona Virus Disease 2019. J Affect Disord. 2021;282:1203–9. https://doi.org/10.1016/j.jad.2021.01.019.
Li W, Wang Z, Wang G, Ip P, Sun X, Jiang Y, Jiang F. Socioeconomic inequality in child mental health during the COVID-19 pandemic: First evidence from China. J Affect Disord. 2021;287:8–14. https://doi.org/10.1016/j.jad.2021.03.009.
Liang Z, Delvecchio E, Cheng Y, Mazzeschi C. Parent and Child’s Negative Emotions During COVID-19: The Moderating Role of Parental Attachment Style. Front Psychol. 2021;12:567483. https://doi.org/10.3389/fpsyg.2021.567483.
Limbers CA, McCollum C, Greenwood E. Physical activity moderates the association between parenting stress and quality of life in working mothers during the COVID-19 pandemic. Ment Health Phys Act. 2020;19:100358. https://doi.org/10.1016/j.mhpa.2020.100358.
Litmanovitz I, Silberstein D, Butler S, Vittner D. Care of hospitalized infants and their families during the COVID-19 pandemic: an international survey. J Perinatol. 2021;41(5):981–7. https://doi.org/10.1038/s41372-021-00960-8.
Liu W, Wang J, Li W, Zhou Z, Liu S, Rong Z. Clinical characteristics of 19 neonates born to mothers with COVID-19. Frontiers of Medicine. 2020;14(2):193–8. https://doi.org/10.1007/s11684-020-0772-y.
Liu, Z., Tang, H., Jin, Q., Wang, G., Yang, Z., Chen, H., . . . Owens, J. (2020). Sleep of preschoolers during the coronavirus disease 2019 (COVID-19) outbreak. Journal of Sleep Research, e13142. https://doi.org/10.1111/jsr.13142
Mahmoud AB, Hack-Polay D, Fuxman L, Nicoletti M. The Janus-faced effects of COVID-19 perceptions on family healthy eating behavior: Parent’s negative experience as a mediator and gender as a moderator. Scand J Psychol. 2021. https://doi.org/10.1111/sjop.12742.
Malkawi, S. H., Almhdawi, K., Jaber, A. F., & Alqatarneh, N. S. (2020). COVID-19 Quarantine-Related Mental Health Symptoms and their Correlates among Mothers: A Cross Sectional Study. Matern Child Health J, 1–11. https://doi.org/10.1007/s10995-020-03034-x
Mangiavacchi L, Piccoli L, Pieroni L. Fathers matter: Intrahousehold responsibilities and children’s wellbeing during the COVID-19 lockdown in Italy. Econ Hum Biol. 2021;42:101016. https://doi.org/10.1016/j.ehb.2021.101016.
Mangolian Shahrbabaki, P., Dehghan, M., Maazallahi, M., & Asadi, N. (2021). Fear and anxiety in girls aged 7 to 11 years old and related factors during the coronavirus pandemic. Clinical Child Psychology and Psychiatry, 13591045211013873. https://doi.org/10.1177/13591045211013873
Manja SA, Mohamad I, Ismail H, Yusof NI. COVID-19: The investigation on the emotional parental burnout during movement control order in Malaysia. Eur J Mol Clin Med. 2020;7(2):4912–29.
Mappa I, Distefano FA, Rizzo G. Effects of coronavirus 19 pandemic on maternal anxiety during pregnancy: a prospectic observational study. J Perinat Med. 2020;48(6):545–50. https://doi.org/10.1515/jpm-2020-0182.
Marchetti D, Fontanesi L, Di Giandomenico S, Mazza C, Roma P, Verrocchio MC. The Effect of Parent Psychological Distress on Child Hyperactivity/Inattention During the COVID-19 Lockdown: Testing the Mediation of Parent Verbal Hostility and Child Emotional Symptoms. Front Psychol. 2020;11:567052. https://doi.org/10.3389/fpsyg.2020.567052.
Marchetti D, Fontanesi L, Mazza C, Di Giandomenico S, Roma P, Verrocchio MC. Parenting-Related Exhaustion During the Italian COVID-19 Lockdown. J Pediatr Psychol. 2020;45(10):1114–23. https://doi.org/10.1093/jpepsy/jsaa093.
Marshall J, Kihlström L, Buro A, Chandran V, Prieto C, Stein-Elger R, Hood K. Statewide implementation of virtual perinatal home visiting during COVID-19. Matern Child Health J. 2020;24(10):1224–30.
Martins-Filho PR, Damascena NP, Lage RCM, Sposato KB. Decrease in child abuse notifications during COVID-19 outbreak: A reason for worry or celebration? J Paediatr Child Health. 2020;56(12):1980–1. https://doi.org/10.1111/jpc.15213.
Masters GA, Asipenko E, Bergman AL, Person SD, Brenckle L, Moore Simas TA, Byatt N. Impact of the COVID-19 pandemic on mental health, access to care, and health disparities in the perinatal period. J Psychiatr Res. 2021;137:126–30. https://doi.org/10.1016/j.jpsychires.2021.02.056.
Mayopoulos GA, Ein-Dor T, Dishy GA, Nandru R, Chan SJ, Hanley LE, Dekel S. COVID-19 is associated with traumatic childbirth and subsequent mother-infant bonding problems. J Affect Disord. 2021;282:122–5. https://doi.org/10.1016/j.jad.2020.12.101.
Mazza, C., Ricci, E., Marchetti, D., Fontanesi, L., Di Giandomenico, S., Verrocchio, M. C., & Roma, P. (2020). How Personality Relates to Distress in Parents during the Covid-19 Lockdown: The Mediating Role of Child's Emotional and Behavioral Difficulties and the Moderating Effect of Living with Other People. International Journal of Environmental Research and Public Health, 17(17). https://doi.org/10.3390/ijerph17176236
Miller KA, Mannix R, Schmitz G, Monuteaux MC, Lee LK. Impact of COVID-19 on professional and personal responsibilities of Massachusetts physicians. Am J Emerg Med. 2020;38(11):2365–7. https://doi.org/10.1016/j.ajem.2020.08.051.
Mirlashari J, Ebrahimpour F, Salisu WJ. War on two fronts: Experience of children with cancer and their family during COVID-19 pandemic in Iran. J Pediatr Nurs. 2020;57:25–31. https://doi.org/10.1016/j.pedn.2020.10.024.
Mizrak Sahin B, Kabakci EN. The experiences of pregnant women during the COVID-19 pandemic in Turkey: A qualitative study. Women Birth. 2020. https://doi.org/10.1016/j.wombi.2020.09.022.
Mo PKH, Fong VWI, Song B, Di J, Wang Q, Wang L. Association of Perceived Threat, Negative Emotions, and Self-Efficacy With Mental Health and Personal Protective Behavior Among Chinese Pregnant Women During the COVID-19 Pandemic: Cross-sectional Survey Study. J Med Internet Res. 2021;23(4):e24053. https://doi.org/10.2196/24053.
Molgora S, Accordini M. Motherhood in the Time of Coronavirus: The Impact of the Pandemic Emergency on Expectant and Postpartum Women’s Psychological Well-Being. Front Psychol. 2020;11:567155. https://doi.org/10.3389/fpsyg.2020.567155.
Moore SA, Faulkner G, Rhodes RE, Brussoni M, Chulak-Bozzer T, Ferguson LJ, Tremblay MS. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: a national survey. Int J Behav Nutr Phys Act. 2020;17(1):85. https://doi.org/10.1186/s12966-020-00987-8.
Morelli M, Cattelino E, Baiocco R, Trumello C, Babore A, Candelori C, Chirumbolo A. Parents and Children During the COVID-19 Lockdown: The Influence of Parenting Distress and Parenting Self-Efficacy on Children’s Emotional Well-Being. Front Psychol. 2020;11:584645. https://doi.org/10.3389/fpsyg.2020.584645.
Moscardino, U., Dicataldo, R., Roch, M., Carbone, M., & Mammarella, I. C. (2021). Parental stress during COVID-19: A brief report on the role of distance education and family resources in an Italian sample. Current Psychology (New Brunswick, N.J.), 1–4. https://doi.org/10.1007/s12144-021-01454-8
Mousavi SF. Psychological Well-Being, Marital Satisfaction, and Parental Burnout in Iranian Parents: The Effect of Home Quarantine During COVID-19 Outbreaks. Front Psychol. 2020;11:553880. https://doi.org/10.3389/fpsyg.2020.553880.
Moyer CA, Sakyi KS, Sacks E, Compton SD, Lori JR, Williams JEO. COVID-19 is increasing Ghanaian pregnant women’s anxiety and reducing healthcare seeking. Int J Gynaecol Obstet. 2020. https://doi.org/10.1002/ijgo.13487.
Muhidin S, Behboodi Moghadam Z, Vizheh M. Analysis of Maternal Coronavirus Infections and Neonates Born to Mothers with 2019-nCoV; a Systematic Review. Arch Acad Emerg Med. 2020;8(1):e49.
Mulale, U. K., Kashamba, T., Strysko, J., & Kyokunda, L. T. (2021). Fatal SARS-CoV-2 and Mycobacterium tuberculosis coinfection in an infant: insights from Botswana. BMJ Case Reports, 14(4). https://doi.org/10.1136/bcr-2020-239701
Muldoon KA, Denize KM, Talarico R, Boisvert C, Frank O, Harvey ALJ, El-Chaar D. COVID-19 and perinatal intimate partner violence: a cross-sectional survey of pregnant and postpartum individuals in the early stages of the COVID-19 pandemic. BMJ Open. 2021;11(5):e049295. https://doi.org/10.1136/bmjopen-2021-049295.
Naeem F, Husain MO, Husain MI, Javed A. Digital psychiatry in low-and middle-income countries post-COVID-19: Opportunities, challenges, and solutions. Indian J Psychiatry. 2020;62(Suppl 3):S380.
Naghizadeh S, Mirghafourvand M, Mohammadirad R. Domestic violence and its relationship with quality of life in pregnant women during the outbreak of COVID-19 disease. BMC Pregnancy Childbirth. 2021;21(1):88. https://doi.org/10.1186/s12884-021-03579-x.
Nassar MF, Allam MF, Shata MO. Effect of COVID-19 Lockdown on Young Egyptian Soccer Players. Glob Pediatr Health. 2021;8:2333794x211012980. https://doi.org/10.1177/2333794x211012980.
Naurin, E., Markstedt, E., Stolle, D., Enström, D., Wallin, A., Andreasson, I., . . . Sengpiel, V. (2020). Pregnant under the pressure of a pandemic: a large-scale longitudinal survey before and during the COVID-19 outbreak. European Journal of Public Health. https://doi.org/10.1093/eurpub/ckaa223
Neece C, McIntyre LL, Fenning R. Examining the impact of COVID-19 in ethnically diverse families with young children with intellectual and developmental disabilities. J Intellect Disabil Res. 2020;64(10):739–49. https://doi.org/10.1111/jir.12769.
Nguyen PH, Kachwaha S, Pant A, Tran LM, Ghosh S, Sharma PK, Menon P. Impact of COVID-19 on household food insecurity and interlinkages with child feeding practices and coping strategies in Uttar Pradesh, India: a longitudinal community-based study. BMJ Open. 2021;11(4):e048738. https://doi.org/10.1136/bmjopen-2021-048738.
Nodoushan, R. J., Alimoradi, H., & Nazari, M. (2020). Spiritual Health and Stress in Pregnant Women During the Covid-19 Pandemic. SN Compr Clin Med, 1–7. https://doi.org/10.1007/s42399-020-00582-9
Nomura, R., Tavares, I., Ubinha, A. C., Costa, M. L., Opperman, M. L., Brock, M., . . . Br, A. P. S. C. B. A. D. P. S. G. I. C. (2021). Impact of the COVID-19 Pandemic on Maternal Anxiety in Brazil. J Clin Med, 10(4). https://doi.org/10.3390/jcm10040620
Odeh R, Gharaibeh L, Daher A, Kussad S, Alassaf A. Caring for a child with type 1 diabetes during COVID-19 lockdown in a developing country: Challenges and parents’ perspectives on the use of telemedicine. Diabetes Res Clin Pract. 2020;168:108393. https://doi.org/10.1016/j.diabres.2020.108393.
O’Driscoll M, Ribeiro Dos Santos G, Wang L, et al. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature. 2021;590:140–5. https://doi.org/10.1038/s41586-020-2918-0.
Oncel, M. Y., Akın, I. M., Kanburoglu, M. K., Tayman, C., Coskun, S., Narter, F., . . . Koc, E. (2020). A multicenter study on epidemiological and clinical characteristics of 125 newborns born to women infected with COVID-19 by Turkish Neonatal Society. European Journal of Pediatrics, 1–10. https://doi.org/10.1007/s00431-020-03767-5
Oskovi-Kaplan, Z. A., Buyuk, G. N., Ozgu-Erdinc, A. S., Keskin, H. L., Ozbas, A., & Moraloglu Tekin, O. (2020). The Effect of COVID-19 Pandemic and Social Restrictions on Depression Rates and Maternal Attachment in Immediate Postpartum Women: a Preliminary Study. Psychiatric Quarterly, 1–8. https://doi.org/10.1007/s11126-020-09843-1
Overbeck, G., Graungaard, A. H., Rasmussen, I. S., Andersen, J. H., Ertmann, R. K., Kragstrup, J., & Wilson, P. (2020). Pregnant women's concerns and antenatal care during COVID-19 lock-down of the Danish society. Danish Medical Journal, 67(12).
Ozturk Eyimaya A, Yalçin Irmak A. Relationship between parenting practices and children’s screen time during the COVID-19 Pandemic in Turkey. J Pediatr Nurs. 2020;56:24–9. https://doi.org/10.1016/j.pedn.2020.10.002.
Papapanou, M., Papaioannou, M., Petta, A., Routsi, E., Farmaki, M., Vlahos, N., & Siristatidis, C. (2021). Maternal and Neonatal Characteristics and Outcomes of COVID-19 in Pregnancy: An Overview of Systematic Reviews. International Journal of Environmental Research and Public Health, 18(2). https://doi.org/10.3390/ijerph18020596
Patel V, et al. The Lancet Commission on global mental health and sustainable development. Lancet. 2018;392(10157):1553–98. https://doi.org/10.1016/S0140-6736(18)32624-2.
Patrick, S. W., Henkhaus, L. E., Zickafoose, J. S., Lovell, K., Halvorson, A., Loch, S., . . . Davis, M. M. (2020). Well-being of Parents and Children During the COVID-19 Pandemic: A National Survey. Pediatrics, 146(4). https://doi.org/10.1542/peds.2020-016824
Peltz JS, Daks JS, Rogge RD. Mediators of the association between COVID-19-related stressors and parents’ psychological flexibility and inflexibility: The roles of perceived sleep quality and energy. J Contextual Behav Sci. 2020;17:168–76. https://doi.org/10.1016/j.jcbs.2020.07.001.
Peng S, Zhang Y, Liu H, Huang X, Noble DJ, Yang L, Narayan A. A multi-center survey on the postpartum mental health of mothers and attachment to their neonates during COVID-19 in Hubei Province of China. Ann Transl Med. 2021;9(5):382. https://doi.org/10.21037/atm-20-6115.
Peng S, Zhu H, Yang L, Cao L, Huang X, Dynes M, Xia S. A study of breastfeeding practices, SARS-CoV-2 and its antibodies in the breast milk of mothers confirmed with COVID-19. Lancet Reg Health West Pac. 2020;4:100045. https://doi.org/10.1016/j.lanwpc.2020.100045.
Perzow SED, Hennessey EP, Hoffman MC, Grote NK, Davis EP, Hankin BL. Mental health of pregnant and postpartum women in response to the COVID-19 pandemic. J Affect Disord Rep. 2021;4:100123. https://doi.org/10.1016/j.jadr.2021.100123.
Philippe K, Chabanet C, Issanchou S, Monnery-Patris S. Child eating behaviors, parental feeding practices and food shopping motivations during the COVID-19 lockdown in France: (How) did they change? Appetite. 2021;161:105132. https://doi.org/10.1016/j.appet.2021.105132.
Pınar Senkalfa B, Sismanlar Eyuboglu T, Aslan AT, Ramaslı Gursoy T, Soysal AS, Yapar D, İlhan MN. Effect of the COVID-19 pandemic on anxiety among children with cystic fibrosis and their mothers. Pediatr Pulmonol. 2020;55(8):2128–34. https://doi.org/10.1002/ppul.24900.
Poulain T, Meigen C, Sobek C, Ober P, Igel U, Körner A, Vogel M. Loss of childcare and classroom teaching during the Covid-19-related lockdown in spring 2020: A longitudinal study on consequences on leisure behavior and schoolwork at home. PLoS ONE. 2021;16(3):e0247949. https://doi.org/10.1371/journal.pone.0247949.
Preuss H, Capito K, van Eickels RL, Zemp M, Kolar DR. Cognitive reappraisal and self-compassion as emotion regulation strategies for parents during COVID-19: An online randomized controlled trial. Internet Interv. 2021;24:100388. https://doi.org/10.1016/j.invent.2021.100388.
Prikhidko A, Long H, Wheaton MG. The Effect of Concerns About COVID-19 on Anxiety, Stress, Parental Burnout, and Emotion Regulation: The Role of Susceptibility to Digital Emotion Contagion. Front Public Health. 2020;8:567250. https://doi.org/10.3389/fpubh.2020.567250.
Protudjer JLP, Golding M, Salisbury MR, Abrams EM, Roos LE. High anxiety and health-related quality of life in families with children with food allergy during coronavirus disease 2019. Ann Allergy Asthma Immunol. 2020;126(1):83-88.e81. https://doi.org/10.1016/j.anai.2020.09.010.
Quandt, S. A., LaMonto, N. J., Mora, D. C., Talton, J. W., Laurienti, P. J., & Arcury, T. A. (2020). COVID-19 Pandemic Among Immigrant Latinx Farmworker and Non-farmworker Families: A Rural-Urban Comparison of Economic, Educational, Healthcare, and Immigration Concerns. medRxiv. https://doi.org/10.1101/2020.10.30.20223156
Quenzer-Alfred C, Schneider L, Soyka V, Harbrecht M, Blume V, Mays D. No nursery ‘til school–the transition to primary school without institutional transition support due to the COVID-19 shutdown in Germany. Eur J Spec Needs Educ. 2021;36(1):127–41. https://doi.org/10.1080/08856257.2021.1872850.
Ren J, Li X, Chen S, Nie Y. The Influence of Factors Such as Parenting Stress and Social Support on the State Anxiety in Parents of Special Needs Children During the COVID-19 Epidemic. Front Psychol. 2020;11:565393. https://doi.org/10.3389/fpsyg.2020.565393.
Rhodes A, Kheireddine S, Smith AD. A mixed methods investigation into the experiences, attitudes and needs of Baby Buddy pregnancy and parenting app users during the COVID-19 pandemic. JMIR Mhealth Uhealth. 2020. https://doi.org/10.2196/23157.
Rocha HA, Sudfeld CR, Leite ÁJ, Rocha SG, Machado MM, Campos JS, Correia LL. Coronavirus disease 2019, food security and maternal mental health in Ceará, Brazil: a repeated cross-sectional survey. Public Health Nutr. 2021;24(7):1836–40. https://doi.org/10.1017/s1368980021000628.
Rogers, G., Perez-Olivas, G., Stenfert Kroese, B., Patel, V., Murphy, G., Rose, J., . . . Willner, P. (2021). The experiences of mothers of children and young people with intellectual disabilities during the first COVID-19 lockdown period. J Appl Res Intellect Disabil. https://doi.org/10.1111/jar.12884
Romero, E., López-Romero, L., Domínguez-Álvarez, B., Villar, P., & Gómez-Fraguela, J. A. (2020). Testing the Effects of COVID-19 Confinement in Spanish Children: The Role of Parents' Distress, Emotional Problems and Specific Parenting. International Journal of Environmental Research and Public Health, 17(19). https://doi.org/10.3390/ijerph17196975
Romero-Gonzalez B, Puertas-Gonzalez JA, Mariño-Narvaez C, Peralta-Ramirez MI. Confinement variables by COVID-19 predictors of anxious and depressive symptoms in pregnant women. Med Clin. 2020. https://doi.org/10.1016/j.medcli.2020.10.002.
Ronchi A, Pietrasanta C, Zavattoni M, Saruggia M, Schena F, Sinelli MT, Pugni L. Evaluation of Rooming-in Practice for Neonates Born to Mothers With Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Italy. JAMA Pediatr. 2021;175(3):260–6. https://doi.org/10.1001/jamapediatrics.2020.5086.
Russell BS, Hutchison M, Tambling R, Tomkunas AJ, Horton AL. Initial Challenges of Caregiving During COVID-19: Caregiver Burden, Mental Health, and the Parent-Child Relationship. Child Psychiatry Hum Dev. 2020;51(5):671–82. https://doi.org/10.1007/s10578-020-01037-x.
Sabharwal V, Bartolome R, Hassan SA, Levesque BM, Camelo IY, Wachman EM, Parker MG. Mother-Infant Dyads with COVID-19 at an Urban, Safety-Net Hospital: Clinical Manifestations and Birth Outcomes. Am J Perinatol. 2021;38(7):741–6. https://doi.org/10.1055/s-0041-1726429.
Sakalidis, V. S., Rea, A., Perrella, S. L., McEachran, J., Collis, G., Miraudo, J., . . . Geddes, D. T. (2021). Wellbeing of Breastfeeding Women in Australia and New Zealand during the COVID-19 Pandemic: A Cross-Sectional Study. Nutrients, 13(6). https://doi.org/10.3390/nu13061831
Sama BK, Kaur P, Thind PS, Verma MK, Kaur M, Singh DD. Implications of COVID-19-induced nationwide lockdown on children’s behaviour in Punjab, India. Child Care Health Dev. 2020. https://doi.org/10.1111/cch.12816.
Scala, M., Marchman, V. A., Brignoni-Pérez, E., Morales, M. C., & Travis, K. E. (2020). Impact of the COVID-19 pandemic on developmental care practices for infants born preterm. medRxiv. https://doi.org/10.1101/2020.11.25.20238956
Scarpellini F, Segre G, Cartabia M, Zanetti M, Campi R, Clavenna A, Bonati M. Distance learning in Italian primary and middle school children during the COVID-19 pandemic: a national survey. BMC Public Health. 2021;21(1):1035. https://doi.org/10.1186/s12889-021-11026-x.
Shafer K, Scheibling C, Milkie MA. The Division of Domestic Labor before and during the COVID-19 Pandemic in Canada: Stagnation versus Shifts in Fathers’ Contributions. Can Rev Sociol. 2020;57(4):523–49. https://doi.org/10.1111/cars.12315.
Shah R, Raju VV, Sharma A, Grover S. Impact of COVID-19 and Lockdown on Children with ADHD and Their Families-An Online Survey and a Continuity Care Model. Journal of Neurosciences in Rural Practice. 2021;12(1):71–9. https://doi.org/10.1055/s-0040-1718645.
Shinomiya, Y., Yoshizaki, A., Murata, E., Fujisawa, T. X., Taniike, M., & Mohri, I. (2021). Sleep and the General Behavior of Infants and Parents during the Closure of Schools as a Result of the COVID-19 Pandemic: Comparison with 2019 Data. Children (Basel), 8(2). https://doi.org/10.3390/children8020168
Shockley KM, Clark MA, Dodd H, King EB. Work-family strategies during COVID-19: Examining gender dynamics among dual-earner couples with young children. J Appl Psychol. 2020. https://doi.org/10.1037/apl0000857.
Shorey, S. Y., Ng, E. D., & Chee, C. Y. I. (2021). Anxiety and depressive symptoms of women in the perinatal period during the COVID-19 pandemic: A systematic review and meta-analysis. Scand J Public Health, 14034948211011793. https://doi.org/10.1177/14034948211011793
Silverman ME, Burgos L, Rodriguez ZI, Afzal O, Kalishman A, Callipari F, Loudon H. Postpartum mood among universally screened high and low socioeconomic status patients during COVID-19 social restrictions in New York City. Sci Rep. 2020;10(1):22380. https://doi.org/10.1038/s41598-020-79564-9.
Spinelli M, Lionetti F, Pastore M, Fasolo M. Parents’ Stress and Children’s Psychological Problems in Families Facing the COVID-19 Outbreak in Italy. Front Psychol. 2020;11:1713. https://doi.org/10.3389/fpsyg.2020.01713.
Spinelli M, Lionetti F, Setti A, Fasolo M. Parenting Stress During the COVID-19 Outbreak: Socioeconomic and Environmental Risk Factors and Implications for Children Emotion Regulation. Fam Process. 2020. https://doi.org/10.1111/famp.12601.
Steinberg S, Liu T, Lense MD. Musical Engagement and Parent-Child Attachment in Families With Young Children During the Covid-19 Pandemic. Front Psychol. 2021;12:641733. https://doi.org/10.3389/fpsyg.2021.641733.
Suzuki, S. (2020). Psychological status of postpartum women under the COVID-19 pandemic in Japan. Journal of Maternal-Fetal & Neonatal Medicine, 1–3. https://doi.org/10.1080/14767058.2020.1763949
Sánchez-Luna, M., Fernández Colomer, B., de Alba Romero, C., Alarcón Allen, A., Baña Souto, A., Camba Longueira, F., . . . Zamora Flores, E. (2021). Neonates Born to Mothers With COVID-19: Data From the Spanish Society of Neonatology Registry. Pediatrics, 147(2). https://doi.org/10.1542/peds.2020-015065
Talbot, J., Charron, V., & Konkle, A. T. (2021). Feeling the Void: Lack of Support for Isolation and Sleep Difficulties in Pregnant Women during the COVID-19 Pandemic Revealed by Twitter Data Analysis. International Journal of Environmental Research and Public Health, 18(2). https://doi.org/10.3390/ijerph18020393
Tang S, Xiang M, Cheung T, Xiang YT. Mental health and its correlates among children and adolescents during COVID-19 school closure: The importance of parent-child discussion. J Affect Disord. 2020;279:353–60. https://doi.org/10.1016/j.jad.2020.10.016.
Taubman-Ben-Ari O, Ben-Yaakov O. Distress and apprehension among new parents during the COVID-19 pandemic: The contribution of personal resources. Am J Orthopsychiatry. 2020;90(6):810–6. https://doi.org/10.1037/ort0000497.
Taubman-Ben-Ari O, Chasson M, Abu-Sharkia S. Childbirth anxieties in the shadow of COVID-19: Self-compassion and social support among Jewish and Arab pregnant women in Israel. Health Soc Care Community. 2020. https://doi.org/10.1111/hsc.13196.
TG, W. M., Kassie, B. A., Asratie, M. H., & Abate, A. T. The Effects of Fear and Knowledge of COVID-19 on Preventive Practice Among Pregnant Women Who Attend Antenatal Care in Northwest Ethiopia, 2020: Institution-Based Cross-Sectional Study. Int J Womens Health. 2021;13:95–100. https://doi.org/10.2147/ijwh.S286088.
Thayer, Z. M., & Gildner, T. E. (2020). COVID-19-related financial stress associated with higher likelihood of depression among pregnant women living in the United States. American Journal of Human Biology, e23508. https://doi.org/10.1002/ajhb.23508
Thompson, K. A., & Bardone-Cone, A. M. (2021). 2019-nCOV distress and depressive, anxiety and OCD-type, and eating disorder symptoms among postpartum and control women. Arch Womens Ment Health, 1–10. https://doi.org/10.1007/s00737-021-01120-9
Tso, W. W. Y., Wong, R. S., Tung, K. T. S., Rao, N., Fu, K. W., Yam, J. C. S., . . . Lp, P. (2020). Vulnerability and resilience in children during the COVID-19 pandemic. European Child and Adolescent Psychiatry, 1–16. https://doi.org/10.1007/s00787-020-01680-8
Valero-Moreno S, Lacomba-Trejo L, Tamarit A, Pérez-Marín M, Montoya-Castilla I. Psycho-emotional adjustment in parents of adolescents: A cross-sectional and longitudinal analysis of the impact of the COVID pandemic. J Pediatr Nurs. 2021. https://doi.org/10.1016/j.pedn.2021.01.028.
Vasilevski, V., Sweet, L., Bradfield, Z., Wilson, A. N., Hauck, Y., Kuliukas, L., . . . Wynter, K. (2021). Receiving maternity care during the COVID-19 pandemic: Experiences of women's partners and support persons. Women Birth. https://doi.org/10.1016/j.wombi.2021.04.012
Vazquez-Vazquez A, Dib S, Rougeaux E, Wells JC, Fewtrell MS. The impact of the Covid-19 lockdown on the experiences and feeding practices of new mothers in the UK: Preliminary data from the COVID-19 New Mum Study. Appetite. 2021;156:104985. https://doi.org/10.1016/j.appet.2020.104985.
Vu Hoang D, Cashin J, Gribble K, Marinelli K, Mathisen R. Misalignment of global COVID-19 breastfeeding and newborn care guidelines with World Health Organization recommendations. BMJ Nutr Prev Health. 2020;3(2):339–50. https://doi.org/10.1136/bmjnph-2020-000184.
Waller, R., Powell, T., Rodriguez, Y., Corbett, N., Perlstein, S., White, L. K., . . . Wagner, N. J. (2021). The Impact of the COVID-19 Pandemic on Children's Conduct Problems and Callous-Unemotional Traits. Child Psychiatry and Human Development, 1–12. https://doi.org/10.1007/s10578-020-01109-y
Wang Q, Song B, Di J, Yang X, Wu A, Lau J, Mo PK. Intentions to Seek Mental Health Services During the COVID-19 Pandemic Among Chinese Pregnant Women With Probable Depression or Anxiety: Cross-sectional Web-Based Survey Study. JMIR Ment Health. 2021;8(2):e24162. https://doi.org/10.2196/24162.
Wang SD, Devjani S, Chillakanti M, Dunton GF, Mason TB. The COMET study: Examining the effects of COVID-19-related perceived stress on Los Angeles Mothers’ dysregulated eating behaviors, child feeding practices, and body mass index. Appetite. 2021;163:105209. https://doi.org/10.1016/j.appet.2021.105209.
Wang Y, Chen L, Wu T, Shi H, Li Q, Jiang H, Qiao J. Impact of Covid-19 in pregnancy on mother’s psychological status and infant’s neurobehavioral development: a longitudinal cohort study in China. BMC Med. 2020;18(1):347. https://doi.org/10.1186/s12916-020-01825-1.
Wimberly CE, Towry L, Caudill C, Johnston EE, Walsh KM. Impacts of COVID-19 on caregivers of childhood cancer survivors. Pediatr Blood Cancer. 2021;68(4):e28943. https://doi.org/10.1002/pbc.28943.
Wu, Q., Xu, Y., & Jedwab, M. (2021). Custodial Grandparent's Job Loss During the COVID-19 Pandemic and Its Relationship With Parenting Stress and Mental Health. Journal of Applied Gerontology, 7334648211006222. https://doi.org/10.1177/07334648211006222
Xie M, Wang X, Zhang J, Wang Y. Alteration in the psychologic status and family environment of pregnant women before and during the COVID-19 pandemic. Int J Gynaecol Obstet. 2021;153(1):71–5. https://doi.org/10.1002/ijgo.13575.
Xu K, Zhang Y, Xu Q, Lv L, Zhang J. Mental health among pregnant women under public health interventions during COVID-19 outbreak in Wuhan. China Psychiatry Research. 2021;301:113977. https://doi.org/10.1016/j.psychres.2021.113977.
Xu, Y., Wu, Q., Jedwab, M., & Levkoff, S. E. (2020). Understanding the Relationships between Parenting Stress and Mental Health with Grandparent Kinship Caregivers' Risky Parenting Behaviors in the Time of COVID-19. J Fam Violence, 1–13. https://doi.org/10.1007/s10896-020-00228-3
Xu, Y., Wu, Q., Levkoff, S. E., & Jedwab, M. (2020). Material hardship and parenting stress among grandparent kinship providers during the COVID-19 pandemic: The mediating role of grandparents' mental health. Child Abuse and Neglect, 104700. https://doi.org/10.1016/j.chiabu.2020.104700
Xue, A., Oros, V., Marca-Ghaemmaghami, P., Scholkmann, F., Righini-Grunder, F., Natalucci, G., . . . Restin, T. (2021). New Parents Experienced Lower Parenting Self-Efficacy during the COVID-19 Pandemic Lockdown. Children (Basel), 8(2). https://doi.org/10.3390/children8020079
Xue B, McMunn A. Gender differences in unpaid care work and psychological distress in the UK Covid-19 lockdown. PLoS ONE. 2021;16(3):e0247959. https://doi.org/10.1371/journal.pone.0247959.
Yamamura, E., & Tsustsui, Y. (2021). The impact of closing schools on working from home during the COVID-19 pandemic: evidence using panel data from Japan. Rev Econ Househ, 1–20. https://doi.org/10.1007/s11150-020-09536-5
Yan H, Ding Y, Guo W. Mental Health of Pregnant and Postpartum Women During the Coronavirus Disease 2019 Pandemic: A Systematic Review and Meta-Analysis. Front Psychol. 2020;11:617001. https://doi.org/10.3389/fpsyg.2020.617001.
Yerkes MA, André SCH, Besamusca JW, Kruyen PM, Remery C, van der Zwan R, Geurts SAE. “Intelligent” lockdown, intelligent effects? Results from a survey on gender (in)equality in paid work, the division of childcare and household work, and quality of life among parents in the Netherlands during the Covid-19 lockdown. PLoS ONE. 2020;15(11):e0242249. https://doi.org/10.1371/journal.pone.0242249.
Yildirim TM, Eslen-Ziya H. The Differential Impact of COVID-19 on the Work Conditions of Women and Men Academics during the Lockdown. Gend Work Organ. 2020. https://doi.org/10.1111/gwao.12529.
Yirmiya, K., Yakirevich-Amir, N., Preis, H., Lotan, A., Atzil, S., & Reuveni, I. (2021). Women's Depressive Symptoms during the COVID-19 Pandemic: The Role of Pregnancy. International Journal of Environmental Research and Public Health, 18(8). https://doi.org/10.3390/ijerph18084298
Yue, J., Zang, X., Le, Y., & An, Y. (2020). Anxiety, depression and PTSD among children and their parent during 2019 novel coronavirus disease (COVID-19) outbreak in China. Current Psychology (New Brunswick, N.J.), 1–8. https://doi.org/10.1007/s12144-020-01191-4
Zaigham M, Andersson O. Maternal and perinatal outcomes with COVID-19: A systematic review of 108 pregnancies. Acta Obstet Gynecol Scand. 2020;99(7):823–9. https://doi.org/10.1111/aogs.13867.
Zamarro, G., & Prados, M. J. (2021). Gender differences in couples' division of childcare, work and mental health during COVID-19. Rev Econ Househ, 1–30. https://doi.org/10.1007/s11150-020-09534-7
Zanardo, V., Tortora, D., Guerrini, P., Garani, G., Severino, L., Soldera, G., & Straface, G. (2020). Infant feeding initiation practices in the context of COVID-19 lockdown. Early Human Development, 152, 105286. https://doi.org/10.1016/j.earlhumdev.2020.105286
Zeng X, Li W, Sun H, Luo X, Garg S, Liu T, Zhang Y. Mental Health Outcomes in Perinatal Women During the Remission Phase of COVID-19 in China. Front Psychiatry. 2020;11:571876. https://doi.org/10.3389/fpsyt.2020.571876.
Zhang Y, Deng R, Chen M, Cao R, Chen S, Chen K, Tian K. Association of Sleep Duration and Screen Time With Anxiety of Pregnant Women During the COVID-19 Pandemic. Front Psychol. 2021;12:646368. https://doi.org/10.3389/fpsyg.2021.646368.
Zhang, Y., & Ma, Z. F. (2020). Psychological responses and lifestyle changes among pregnant women with respect to the early stages of COVID-19 pandemic. International Journal of Social Psychiatry, 20764020952116. https://doi.org/10.1177/0020764020952116
Zhou Y, Wang R, Liu L, Ding T, Huo L, Qi L, Dai G. The impact of lockdown policy on depressive symptoms among pregnant women in China: mediating effects of internet use and family support. Glob Health Res Policy. 2021;6(1):11. https://doi.org/10.1186/s41256-021-00193-4.
Zreik, G., Asraf, K., Haimov, I., & Tikotzky, L. (2020). Maternal perceptions of sleep problems among children and mothers during the coronavirus disease 2019 (COVID-19) pandemic in Israel. Journal of Sleep Research, e13201. https://doi.org/10.1111/jsr.13201
Çolak S, Gürlek B, Önal Ö, Yılmaz B, Hocaoglu C. The level of depression, anxiety, and sleep quality in pregnancy during coronavirus disease 2019 pandemic. J Obstet Gynaecol Res. 2021. https://doi.org/10.1111/jog.14872.
Singer M, Nicola B, Ostrach B, Emily M. Syndemics and the biosocial conception of health. The Lancet (British Edition). 2017;389(10072):941–50. https://doi.org/10.1016/S0140-6736(17)30003-X.
Britto PR, et al. Nurturing care: promoting early childhood development. The Lancet (British Edition). 2016;389(10064):91–102. https://doi.org/10.1016/S0140-6736(16)31390-3.
Shonkoff JP, Ritcher L, van der Gaag J, Bhutta ZA. An Integrated Scientific Framework for Child Survival and Early Childhood Development. Pediatrics (Evanston). 2012;129(2):E460–72. https://doi.org/10.1542/peds.2011-0366.
Black MM, et al. Early childhood development coming of age: science through the life course. The Lancet (British Edition). 2016;389(10064):77–90. https://doi.org/10.1016/S0140-6736(16)31389-7.
Grantham-McGregor C, Cueto YB, Glewwe S, Richter PL, Strupp B. Child development in developing countries 1 - Developmental potential in the first 5 years for children in developing countries. The Lancet (British Edition). 2007;369(9555):60–70. https://doi.org/10.1016/S0140-6736(07)60032-4.
Tricco LE, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–73. https://doi.org/10.7326/M18-0850.
Neamah HH, McCoy DC, Fink G, Fawzi WW, Masanja H, Danaei G, Muhihi A, Kaaya S, Fawzi MCS. Intimate Partner Violence, Depression, and Child Growth and Development. Pediatrics (Evanston). 2018;142(1):1. https://doi.org/10.1542/peds.2017-3457.
Landry SH, Smith KE, Swank PR, Zucker T, Crawford AD, Solari E. The effects of a responsive parenting intervention on parent-child interactions during shared book reading. Dev Psychol. 2011;48:969–86.
Young KS, Stein A, Vuust P, Craske MG, Kringelbach ML. The neural basis of responsive caregiving behavior: Investigating temporal dynamics within the parental brain. Behav Brain Res. 2017;325(Pt B):105–16. https://doi.org/10.1016/j.bbr.2016.09.012.
Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, McInerney P, Godfrey CM, Khalil H. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis. 2020;18(10):2119–26.
Acknowledgements
We acknowledge the support of Fundação de Apoio à Pesquisas no Ceará e Nordeste (ASTEF) and the Federal University of Ceará (UFC).
Funding
This study was funded by Fundação Maria Cecília Souto Vidigal (FMCSV). The funding source had no role in the design, data collection, analysis of results, or manuscript elaboration.
Author information
Authors and Affiliations
Contributions
Authors’ abbreviations: Ana Luiza Penna (AP); Camila Machado de Aquino (CA), Maria Suelly Nogueira Pinheiro (MP), Rodrigo Leão Ferreira do Nascimento (RN), Simone Farias-Antúnez (SF), David Augusto Batista Sá Araújo (DA), Carol Mita (CM), Marcia Maria Tavares Machado (MM) and Marcia C. Castro (MC).
MC and AP conceptualized the work; MC, AP, and CM designed the data search criteria; AP and CA designed the analysis plan; CM was responsible for data acquisition; AP, CA, MP, RN, SF, and DA analysed the data and produced data charts; AP and CA interpreted the data; AP synthesized the data and wrote the manuscript; AP, SF and DA formatted the manuscript and Supplementary materials; MM and MC revised the final documents, including all Supplementary materials. All authors read and approved the final manuscript and have agreed to both be personally accountable for their contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
All data generated or analyzed during this study are included in this published article and its supplementary information files. The code necessary to reproduce the analyses presented here are available from the first author.
Competing interests
The authors declare that they have no financial or non-financial competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Penna, A.L., de Aquino, C.M., Pinheiro, M.S.N. et al. Impact of the COVID-19 pandemic on maternal mental health, early childhood development, and parental practices: a global scoping review. BMC Public Health 23, 388 (2023). https://doi.org/10.1186/s12889-023-15003-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15003-4