
Abstract
Introduction
Globally, drowning is a significant cause of preventable mortality and morbidity. The Eastern Mediterranean region (EMR) comprises 22 countries of extreme disparity in income and is a region impacted by conflict and migration. We systematically review literature published on drowning in the EMR.
Methods
Peer-reviewed literature (limited to original research) was identified using Embase, PubMed, Scopus, SportsDiscus, and Web of Science databases. Literature was independently dual screened at title/abstract and full text stages with dual data extraction (20% of included studies). Studies were included if they reported epidemiology, risk/protective factors and/or prevention strategies for drowning (unintentional and intentional; fatal and non-fatal) of residents, tourists or migrants in the EMR. Literature was assessed against the [Australian] National Health and Medical Research Council’s Levels of Evidence.
Results
Seventy-two studies were included in this review (epidemiology 68 studies; risk/protective factor 13 studies; prevention strategies 19 studies). Iran (n = 27), Saudia Arabia (n = 11) and Pakistan (n = 10) recorded the largest number of dedicated studies. Studies predominately focused on unintentional drowning. Ninety-two percent of included studies (n = 66) were ranked as being low evidence (level IV). The majority of studies explored drowning among children and adolescents (0–19 years). All-age fatal drowning rates varied from a low of 0.48 per 100,000 (United Arab Emirates; 2002; Ministry of Health death registry data) to a high of 18.5 per 100,000 (Egypt; 2014–15; WHO mortality database). Commonly identified risk factors included being male, young age, submersion time and resident status. Common prevention strategies public education, lifeguard supervision, and cardiopulmonary resuscitation.
Discussion
Gaps in understanding of drowning burden in some countries within the region, as well as region-wide risk factor identification for adult drowning, intentional and migration-related drowning, impair the ability of nations to advance drowning prevention. There is a need for investment in implementation and evaluation of drowning prevention interventions in the EMR.
Conclusion
Drowning is a significant cause of mortality and morbidity in the EMR. The recent UN declaration on global drowning prevention may provide the impetus to invest in drowning prevention research, policy, and advocacy with the aim of reducing drowning-related harms in the EMR.
Trial registration
Registration number: #CRD42021271215.
Similar content being viewed by others


Introduction
Globally, drowning is a significant cause of preventable harm [1] which has recently been acknowledged in a United Nations (UN) General Assembly resolution [2]. In 2017, the Global Burden of Disease (GBD) Study estimated 295,000 lives lost to drowning [3]. More recently, the World Health Organization (WHO) estimated 236,000 lives lost globally in 2019 [4]. However, both estimates are likely to be significant underreports due to the exclusion of fatal unintentional drowning due to transportation and disaster-related causes. The exclusion of such cases is shown to underreport drowning by between 40 and 60% in some high-income countries (HICs) [5,6,7], with the impact likely to be significantly higher in low- and middle-income countries (LMICs). In addition, there is limited global data on the impact of intentional drowning as a cause of death [8, 9].
Our understanding of drowning is further limited due to a lack of data globally on non-fatal drowning. Drowning is defined as the process of experiencing respiratory impairment due to submersion or immersion in liquid, with outcomes being death, morbidity or no morbidity [10]. However, a lack of uniform classifications for non-fatal drowning and a lack of data has hampered global estimates [11].
The Eastern Mediterranean Region (EMR) of the WHO comprises 21 member states and the occupied Palestinian territory (including East Jerusalem), with a population of nearly 679 million people [12]. The EMR spans countries from North Africa to Western Asia and the unique geographical, social and economic characteristics of each country yield differing burden of injuries and violence [13]. It is a region that has significant disparities in income levels and has been heavily impacted by conflict [14] and migration, with untold loss of life at sea [15].
Drowning has been identified as an issue in the EMR. A previous review exploring injuries and violence in the EMR reported that unintentional drowning accounted for 6% of all injury deaths in 2012, slightly lower than the global burden at 7% [13]. Unintentional drowning appeared in the top 10 causes of years of life lost in 2013 for EMR countries of Jordan (ranked 7th), Oman (ranked 9th) and Qatar (ranked 10th) [16]. Suicidal drowning has also been identified as an issue of concern in the EMR, accounting for 3.1% of all suicide deaths in the region, with a slightly higher proportion among females (5.0%) than males (4.5%) [17].
Despite previously published location-based literature reviews exploring drowning in low and middle income countries [18], the African continent [19] and individual countries such as India [20] and Singapore [21], no previous systematic literature review has explored drowning in the EMR. As such, the aim of this literature review is to identify the published literature exploring fatal and non-fatal drowning (regardless of intent) in the EMR, with a focus on the epidemiology reported, risk factors identified, and prevention strategies recommended.
Methods
The protocol for this systematic review was prospectively registered with PROSPERO (#CRD42021271215) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines to identify, screen, determine eligibility and include studies [22].
Peer-reviewed literature, limited to original research, was identified via searches of the Embase, PubMed, Scopus, SportsDiscus and Web of Science databases. In addition, we also searched the Google Scholar website to identify additional articles not found through database searches. Google Scholar results were searched until 10 pages of nil results. Database searches were run on 11 August 2021, with the Google Scholar search run on 19 September 2021. The full search strategies used for each database and Google Scholar can be found in Table S1. Additionally, reference lists of relevant excluded studies were searched for additional literature that may not have been identified prior. As a result of this process four additional studies were identified.
Studies were included if they explored drowning in the EMR as defined by the World Health Organization (WHO) [12]. The EMR is comprised of the following member states and territories: Afghanistan, Bahrain, Djibouti, Egypt, (Islamic Republic of) Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Pakistan, Palestine (Occupied Palestinian Territory), Qatar, Saudi Arabia, Somalia, Sudan, Syrian Arab Republic, Tunisia, United Arab Emirates, and Yemen. Studies exploring drowning were included if they reported fatal or non-fatal drowning of any intent (i.e., unintentional, intentional, undetermined intent). We included in this broad definition drowning that was recreational in nature, occupational-related drowning, conflict-related drowning and migration-related drowning. We included studies reporting drowning of non-residents of the EMR if drowning occurred in EMR. We excluded non-human studies, studies focused on the forensic diagnosis of drowning, or the pathophysiology of drowning. We also excluded studies exploring drowning among EMR-born people who reside (and drowned) in non-EMR countries (e.g., EMR residents who emigrated to Scandinavia). Literature published from inception to 11 August 2021 was included in the study.
Literature was screened using Covidence literature screening software [23]. Independent dual screening was performed at title and abstract stage, and again at full text stage, with conflicts resolved via consensus between the two authors. Data extraction was performed using a custom-built Microsoft Excel spreadsheet. Independent data extraction was conducted by both authors, with dual extraction of 20% of included studies.
Studies reporting the epidemiology of drowning were extracted as numbers, proportions or rates per 100,000 for each population reported (i.e., overall, by sex, by age group, by year etc). Where drowning rates were not presented but could be derived (i.e., drowning cases and population data presented), these were manually calculated. Drowning was characterised by outcome (fatal, non-fatal, both, not specified), and intent (unintentional, intentional, both, not specified) and explored at a total population level, as well as by age group and sex. Trends in all-age drowning rates were calculated using the linear trend function in Excel.
Risk/protective factors were defined if statistical tests identified a significant link between the factor and risk of drowning or drowning outcome (i.e., chi square tests of significance, odds ratio, relative risk). The free text description of risk/protective factors was coded by both authors via consensus (see Table S2 for method). Free text of prevention strategies was coded by both authors via consensus (see Table S3 for method). Prevention strategies were extracted if proposed, implemented and/or evaluated. Prevention strategies were coded as primary, secondary or tertiary prevention [24] and against the corresponding level within the Hierarchy of Control [25]. We also recorded if the prevention strategy involved multi-sectoral action (as recommended by the WHO [26]) and if so, which sectors were involved (i.e., health, transport, maritime safety, tourism, disaster preparedness etc). We also assessed whether the prevention strategy mentioned in the literature, aligned to the six selected interventions and four cross-cutting implementation strategies for the prevention of drowning, as recommended by the WHO [26].
Included studies were assessed against the [Australian] National Health and Medical Research Council’s Levels of Evidence [27]. Levels of evidence range from Level I (a systematic review of Level II studies [randomised controlled trial]) to Level IV (case studies with either post-test or pre-test/post-test outcomes) [27]. Income levels of countries represented in included studies were assessed using the World Bank open data country profiles [28].
Results
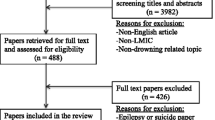
A total of 1806 studies were identified via database searches and Google Scholar. After the removal of duplicates (n = 641), 1165 studies were screened for inclusion by title and abstract. Of these, 1016 studies were deemed irrelevant (87.2%). A total of 149 full text studies were screened for eligibility. After the removal of 77 (51.7%) studies at full text review, a total of 72 studies were included for data extraction (Fig. 1).

PRISMA flow chart
Study characteristics
Included studies were published between 1975 [29] and 2021 [30,31,32]. Studies most commonly reported data on drowning from Iran (27 studies [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59]), Saudia Arabia (11 studies [31, 32, 60,61,62,63,64,65,66,67,68]) and Pakistan (10 studies [69,70,71,72,73,74,75,76,77,78]). There were 3 studies which reported on multiple countries within the EMR [79,80,81] and 3 studies which reported on the EMR as a whole [3, 82, 83] (Table 1).
Twenty-seven studies (37.5% of all included studies) reported data on a national level, with the remaining studies exploring data at a sub-national level. Thirty-six studies (50.0%) reported data from both urban and rural areas, 18 studies (25.0%) reported data from urban areas only and 18 studies (25.0%) examined drowning in rural areas only. When exploring outcome, 42 studies (58.3%) explored fatal drowning, 10 studies (13.9%) explored non-fatal drowning and 20 studies (27.8%) explored both fatal and non-fatal drowning. Twenty-eight (38.9%) studies reported unintentional drowning, 3 studies (4.2%) reported intentional drowning and 9 studies (12.5%) reported drowning regardless of intent. The remaining 32 studies (44.4%) did not specify the intent of the drowning cases reported. The majority of included studies were ranked as being of low evidence (level IV; 66 studies; 91.7%). The characteristics of all included studies can be viewed in full in Table S4.
Epidemiology
Sixty-eight (94.4%) included studies reported the epidemiology of drowning in the EMR. There were 10 studies [3, 34, 40, 43, 50, 54,55,56, 80, 98] which reported all-age fatal drowning rates. Data sources ranged from GBD study [3] and WHO mortality database [80], to death registry and newspaper reports [98] and the majority of studies reported unintentional drowning (Fig. 2).

Rate and trends over time of all-age fatal drowning by country, Eastern Mediterranean Region. GBD Global Burden of Disease, N National, S Sub-national, U Unknown. U Unintentional, I Intentional, Unk Unknown
All-age fatal drowning rates ranged from a low of 0.48 per 100,000 in the United Arab Emirates in 2002 as per Ministry of Health death registry data [98], to a high of 18.5 per 100,000 population in Egypt in 2014–15 [80]. Drowning rates in all countries reported a downward trend, with the exception of Morocco and Egypt, which WHO mortality data indicated an increasing trend in fatal unintentional drowning between 2004 and 05 and 2014–15 [80] (Fig. 2).
There were a further 11 studies [35, 40, 43, 44, 50, 52, 54,55,56, 83, 93] which reported fatal drowning rates by sex and/or age group, the majority of these studies came from Iran. When exploring the EMR as a whole, data from 2004 for children and adolescents aged 0–19 years indicated the highest fatal drowning rate among 1–4 year-olds (9.0 / 100,000 population). For females, the rate was highest among those aged < 1 year of age (7.0 per 100,000) and for males, in the 1–4 years age group (11.0 per 100,000) [83]. Outside of the child and adolescent (0–19 years) age group, the highest drowning rates were reported in Iran among 20–24 year-olds between 2002 and 2007 (17.0 per 100,000 population) [35] (Table 2).
Data on non-fatal drowning were limited. Several studies identified the significant non-fatal drowning burden among young children less than five [32, 51, 67]. By contrast, a study from Saudi Arabia reported almost half (43.1%) of all non-fatal drowning cases in children 1–14, occurring among school age children (7–14 years of age) [64]. While males typically report significantly higher fatal drowning rates, among the non-fatal cases reported, the sex split was proportionately more similar. A study of non-fatal drowning among children 0–14 years of age in Saudi Arabia identified 40% of cases were of girls [32]. Among the all-age population, a study from northern Iran highlighted females accounted for 20.2% of all non-fatal drownings from 2007 to 2008 [42]. A study from Pakistan reported similar findings, with females accounting for 27.9% of all emergency department (ED) presentations for non-fatal drowning [69]. A study of hospital admissions in Iran between 1995 and 2005, found females accounted for 33% of non-fatal drowning-related admissions [51].
Two studies also reported fatal drowning rates by rurality. An all-age study of drowning in Iran between 2005 and 2006, found a higher rate of fatal drowning in rural areas (2.6 per 100,000 population) than in urban areas (1.8) [50]. A study of drowning in Iran among children 0–14 years in 2005 found even higher differences in fatal drowning rates by rurality (rural residence: 4.7; urban residence: 1.3) [52]. One study also reported rates of fatal drowning by aquatic location. In northern Iran, fatal drowning in coastal locations occurred at a rate of 2.48 per 100,000 population, compared with 1.5 for rivers, 0.15 for canals and 0.35 for other natural water locations [50].
Risk/protective factors
There were 13 studies which reported on 18 unique risk/protective factors associated with drowning in the EMR. The majority of studies were conducted among children and adolescents, with just 4 studies examining the all-age population, all from Iran [40, 42, 55, 59]. One study identified factors associated with the self-reported behaviours of parents of infants in Saudi Arabia [68] (Table 3).
The majority (15 factors including low Glasgow Coma Scale [GCS] score) were identified as factors which increased risk of both fatal or non-fatal drowning with poor outcomes (such as severe neurological disease or brain death). Commonly identified risk factors included being male [31, 40, 42, 51, 55, 58, 94], young age [30, 31, 58], submersion time [60, 63] and resident status (both tourists and local residents) [59]. There were several factors identified in the literature as being protective for drowning outcome. These were a high GCS score upon admission and upon end of care [32], decreased length of hospital stay [32], shorter length of time submersed [32] and a body temperature of ≥36 degrees [51] (Table 3).
Prevention of drowning
A total of 19 studies reported 17 unique strategies for the prevention of drowning in the EMR (Table 4). Common strategies detailed in included studies were public education (mentioned in 7 studies across 4 countries), lifeguard supervision (mentioned in 6 studies across 3 countries), and cardiopulmonary resuscitation (CPR) and first aid (mentioned in 6 studies across 4 countries).
Of the 17 unique prevention strategies identified in the literature, the vast majority were proposed, with just five strategies (CPR and First Aid and signage in Jordan [90] and vehicle modification, vehicle operational procedures and vehicle-related water safety training for US troops in Afghanistan and Iraq [79] (Table 4).
Two studies reported the evaluation of drowning prevention interventions. One study in Saudi Arabia assessed parental knowledge of first aid. This study indicated 64.3% knew to lay the victim in a left lateral position. In a nonresponsive not breathing drowning victim, 90.5% knew to start chest compressions and mouth to mouth ventilation. Sixty-six percent (65.6%) knew not to slap a victim on the back [66]. Another study explored the impact on fatal drowning rates of a package of interventions in two coastal areas of Iran, including CPR and first aid training, public education, elimination of water reservoirs and increased lifeguard supervision. This study found the fatal drowning rate fell from 4.24 / 100,000 residents at baseline to 3.04 at end line [40] (Table 4).
The majority of the prevention strategies in the included literature were low on the hierarchy of control, with all but three (signage and vehicle modification [engineering] and restricting access to water [elimination or isolation]) being administrative in nature. Several strategies were identified as being multi-sectoral in nature involving sectors such as education, maritime, health, police, defence, media and tourism, as well as land managers such as local and provincial government (Table 4).
Six of the strategies proposed align with the six selected interventions and four cross-cutting implementation strategies outlined by the WHO. These include the provision of safe places away from water for pre-school children with capable childcare, train bystanders in safe rescue and resuscitation, develop a national water safety plan, strengthen public awareness of drowning through strategic communications, install barriers controlling access to water and teach school-aged children swimming and water safety skills (Table 4).
Discussion
Drowning is a preventable cause of mortality and morbidity in all regions of the world [3], including in the EMR. While significant research has been undertaken to date in countries such as Iran, Saudia Arabia and Pakistan, there remains a dearth of literature on drowning in Yemen, Syria, Somalia, Oman, Libya, Kuwait, and Djibouti, aside from modelled data available via the GBD Study. This review has also identified the need for further research quantifying drowning among adults, intentional drowning burden and migration-related drowning. Risk factor identification was predominately limited to children and there is extremely limited data on the implementation and evaluation of prevention strategies.
The EMR is a diverse region comprising a mix of high and low-and middle-income countries [28]. As such, there was wide variation in the rates of all-age fatal drowning across the region reported in included studies. Rates varied from a low of 0.48 per 100,000 population for unintentional drowning via national Ministry of Health data in the United Arab Emirates in 2002 [98], to a high of 18.5 per 100,000 population for national unintentional drowning in Egypt in 2014–15 [80], using the WHO Mortality Database. Similarly, systematic reviews of drowning in the African region [19] and in low and middle income countries [18] have also reported large variation in rates of fatal drowning. Inconsistencies in data collection makes data synthesis extremely challenging. In addition, there were several countries in the EMR where no studies had been conducted and no data on drowning were available in the peer reviewed literature beyond GBD study modelled data. We echo the call of others, on the need for further research on the issue of drowning in low- and middle-income countries [100, 101].
The existence and availability of accurate and timely data on drowning in many countries in the region is likely impacting country-level analyses of drowning [65]. Several studies included in this review highlighted data challenges such as differences in reporting between data sources in Iran [50] and underreporting of drowning in Ministry of Health death data in the United Arab Emirates, when compared to newspaper reports [98]. Such findings underscore the importance of strengthening existing surveillance systems or developing new systems for consistent and detailed capture of drowning cases [19]. There is a need for prioritisation and investment in, country level drowning registries [102] to aid in the quantification of burden, identification of at risk groups and development, implementation and evaluation of drowning prevention interventions, within the framework of a National Water Safety Plan as recommended by the WHO [26]. This should include all cases of fatal and non-fatal drowning, regardless of intent.
The drowning literature for the EMR published to date identified in this review, has largely explored unintentional fatal drowning. The two key data sources included in this review, the GBD Study [3] and the WHO Mortality Database [80], define unintentional drowning using ICD codes W65–74 (accidental drowning and submersion). This narrow definition of drowning does not capture unintentional drowning due to water transport and disaster events, which has been shown to underreport drowning by between 40 and 60% in selected high-income countries [5,6,7]. Therefore, the declining rates of all-age drowning fatalities reported in this review must be interpreted with caution. Broader inclusion of drowning cases is another benefit of establishing national or regional drowning registries. Included studies also overwhelmingly focused on drowning among children and adolescents, with a need to identify drowning burden, risk factors and prevention strategies for adults and older adults, given an ageing population globally [103, 104].
There were no studies exploring migration-related drowning and only one study exploring conflict-related drowning [79] despite the EMR being a region that is significantly impacted by both issues [105]. Migration in particular is likely to be a significant contributor to the drowning burden in the EMR, with the Missing Migrant project indicating drowning is a leading cause of death during travel along migratory routes [15]. In addition, several studies conducted in countries outside the EMR were identified in initial searches, which pointed to an increased drowning risk among migrants from EMR countries [106, 107]. Although outside the scope of this review, such studies highlight a lack of drowning prevention interventions within the EMR, increasing drowning risk for both residents of the EMR and migrants originating from the EMR.
Being male was a commonly identified risk factor for drowning in the EMR, as has been found elsewhere [108,109,110]. The exception being an all-age study from Iran, which found females aged ≤14 years to be at increased risk of fatal drowning [59]. There may be cultural or other reasons behind this anomalous finding that should be further explored. Little research on the impact of seasonality has been conducted in the EMR, although one study from Saudi Arabia, identified the Winter and Autumn months as being a risk factor for drowning [60]. This differs from many other studies reporting increased drowning risk with periods of warmer weather [111,112,113]. This may be due to extreme summer temperatures in Saudi Arabia impacting patterns of exposure with water. With a changing climate forecast to have significant impacts on drowning risk [114], the differing profile of drowning risk for countries already prone to extreme temperatures in the EMR will likely need to be considered when developing preventive approaches in the near future.
Overwhelmingly however, risk factors for drowning in the EMR were identified based on studies of drowning in children and adolescents. While young people account for a significant proportion of the global burden of drowning [1, 3], there is a need to better understand risk factors for adult and older adult drowning, as well as deeper exploration of location and activity-based risk factors to inform prevention efforts. Such challenges in the identification of risk factors have been previously highlighted in systematic reviews of drowning in the African region [19] and in low and middle income countries [18]. The authors of these studies, as do we, call for detailed data to enable risk factor identification to target preventive approaches.
Evidence surrounding prevention interventions identified in the literature was extremely poor, with extremely limited implementation and evaluation of proposed interventions. Of note however, a study exploring the effect of a package of interventions in coastal regions of Iran, indicated positive reductions in fatal drowning rates [40]. The study does, however, highlight the complexity of implementation with a diversity of sectors and organisations involved, as well as the need for accurate and timely data to evaluate impact [40]. Other literature reviews of drowning have also highlighted the dearth of studies exploring the prevention of drowning, compared to the larger bodies of literature on drowning epidemiology and risk factors [18, 19, 104, 115]. Although conducting studies to identify the effectiveness of drowning prevention interventions are challenging, it represents one of the greatest needs for the drowning prevention sector globally [26]. In the absence of data to identify effectiveness of prevention interventions, validation of expert opinion on drowning prevention interventions via a Delphi process, may be an option, as has been used in other areas of drowning where evidence is lacking [116, 117].
This study is the first of its kind to systematically report on literature exploring the epidemiology, risk factors and prevention strategies for drowning in the EMR. However, the finding of this systematic literature review should be considered within the context of some limitations. This review was conducted in the English language only and may have therefore excluded studies published in languages other than English. This review included primary studies published in peer-reviewed literature only. There may also be relevant information on the issue of drowning and its prevention within the EMR published in the grey literature. The identification of studies is based on the search strategy used. A different search strategy would yield differing results. The resulting included literature is based on the two authors application of the inclusion and exclusion criteria, though dual screening and partial dual extraction methods were utilised to reduce any bias or human error. The World Bank income level attributed to the country is from data from 2019, a country’s income level may have been changed since the included study was conducted. There is a paucity of data on drowning in the EMR outside of Iran, Saudi Arabia, and Pakistan (66.7% of all included articles). It is not known if the risk factors and prevention strategies identified in included studies can be extrapolated to the broader EMR.
Conclusion
Drowning is a significant cause of mortality and morbidity in the EMR; a diverse region that faces significant conflict and migration-related public health challenges. Although many included studies report declining drowning rates, there is a need to examine the full burden of drowning to determine if reductions in unintentional drowning (i.e., ICD codes W65–74) also hold true for water transport and disaster-related drowning. Despite reported reductions, drowning rates remain significant in countries such as Egypt, Afghanistan, and Iran, and among young children and adolescents. However, there is a dearth of research on drowning in the region outside of Iran, Saudia Arabia and Pakistan and on drowning in adults. Additionally, intentional drowning, non-fatal drowning, and the drowning burden associated with migration are poorly researched within the region. Data gaps impair understanding of risk factors and the ability of nations to develop water safety plans to reduce drowning, as recommended by the WHO. Many included studies rely on a single source of data (GBD Study) which exclude water transport and disaster-related drowning. Investment in the establishment of national (or regional) drowning registries will enhance accurate surveillance and monitoring as well as facilitate research to better understand causal factors and impact of preventive approaches. The recent UN Declaration on Global Drowning Prevention provides an opportunity to invest in drowning prevention research, policy, and advocacy with the aim of reducing the drowning-related burden in the EMR. Such efforts must be prioritized to end this preventable loss of life in the region.
Availability of data and materials
All data generated or analysed during this study are included in this published article (and its Supplementary information files).
References
World Health Organization. Global report on drowning: preventing a leading killer Geneva: World Health Organization; 2014.
United Nations. Resolution on Global Drowning Prevention: United Nations; 2021 Available from: https://www.undocs.org/en/A/75/L.76.
Franklin RC, Peden AE, Hamilton EB, Bisignano C, Castle CD, Dingels ZV, et al. The burden of unintentional drowning: global, regional and national estimates of mortality from the global burden of disease 2017 study. Injury Prevention. 2020;26(Supp 1):i83–95.
World Health Organisation. Fact sheets - Drowning 2020 [Date cited: 30-11-2020]. Available from: https://www.who.int/news-room/fact-sheets/detail/drowning.
Lunetta P, Penttilä A, Sajantila A. Drowning in Finland: "external cause" and "injury" codes. Injury Prevention. 2002;8:342–4.
Passmore JW, Smith JO, Clapperton A. True burden of drowning: compiling data to meet the new definition. Int J Inj Control Saf Promot. 2007;14(1):1–3.
Peden A, Franklin RC, Mahony A, Barnsley P, Scarr J. Using a retrospective cross-sectional study to analyse unintentional fatal drowning in Australia: ICD-10 coding-based methodologies verses actual deaths. BMJ Open. 2017;7(e019407).
Haw C, Hawton K. Suicide and self-harm by drowning: a review of the literature. Archives of Suicide Research. 2016;20(2):95–112.
Cenderadewi M, Franklin RC, Peden AE, Devine S. Fatal intentional drowning in Australia: a systematic literature review of rates and risk factors. PLoS One. 2020;15(5):e0231861.
van Beeck E, Branche CM, Szpilman D, Modell JH, Bierens J. A new definition of drowning: towards documentation and prevention of a global public health problem. Bull World Health Organ. 2005;83(11):853–6.
Beerman SB, Bierens, JJLM., Clemens, T., Meddings, D., Rahman, A., Szpilman, D. Clarification and categorization of non-fatal drowning: a draft position statement for review and input by the global drowning community: World Health Organization; 2018 . Available from: https://www.who.int/docs/default-source/documents/drowning/non-fatal-drowning-categorization.pdf?sfvrsn=44d18cc1_2. [7-01-2021]
World Health Organization. World Health Organization Regional Office for the Eastern Mediterranean 2021 Available from: http://www.emro.who.int/index.html.
Bachani AM, Zhang XJ, Allen KA, Hyder AA. Injuries and violence in the eastern Mediterranean region: a review of the health, economic and social burden. East Mediterr Health J. 2014;20(10):643–52.
Brennan R, Hajjeh R, Al-Mandhari A. Responding to health emergencies in the eastern Mediterranean region in times of conflict. Lancet. 2020.
The Missing Migrant Project. Missing Migrants - Tracking Deaths Along Migratory Routes 2021 [Available from: https://missingmigrants.iom.int/.
Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;385(9963):117–71.
Morovatdar N, Moradi-Lakeh M, Malakouti SK, Nojomi M. Most common methods of suicide in eastern Mediterranean region of WHO: a systematic review and Meta-analysis. Arch Suicide Res. 2013;17(4):335–44.
Tyler MD, Richards DB, Reske-Nielsen C, Saghafi O, Morse EA, Carey R, et al. The epidemiology of drowning in low- and middle-income countries: a systematic review. BMC Public Health. 2017;17(1):413.
Miller L, Alele FO, Emeto TI, Franklin RC. Epidemiology, risk factors and measures for preventing drowning in Africa: a systematic review. Medicina. 2019;55(10):637.
Lukaszyk C, Ivers RQ, Jagnoor J. Systematic review of drowning in India: assessment of burden and risk. Injury Prevention. 2018;24(6):451–8.
Tan RMK. The epidemiology and prevention of drowning in Singapore. Singap Med J. 2004;45(7):324–9.
Moher D LA, Tetzlaff J, Altman DG,. Preferred reporting items for systematic reviews and Meta-analyses: the PRISMA statement. Br Med J 2009;339:2535.
Veritas Health Innovation. Covidence systematic review software Melbourne, Australia: Veritas Health Innovation,; 2021 [Available from: www.covidence.org.
Pless IB, Hagel B. Injury prevention: a glossary of terms. J Epidemiol Community Health. 2005;59(3):182.
National Safety Council. The Hierarchy of Controls: National Safety Council; 2019 [Available from: https://www.safetyandhealthmagazine.com/articles/16790-the-hierarchy-of-controls.
World Health Organization. Preventing drowning: an implementation guide: World Health Organization; 2017.
Australian Government National Health and Medical Research Council (NHMRC). NHMRC additional levels of evidence and grades for recommendations for developers of guidelines. 2005.
The World Bank. World Bank Open Data Country Profiles 2021 [Available from: https://data.worldbank.org/country.
Malik MOA. Some aspects of the mortality pattern in the Sudan. Med Sci Law. 1975;15(4):246–60.
Liu JC, Ismael AA, Zaidi A, Sha’ban BW, Almutawa SE, Chatha AA, et al. Epidemiology of pediatric trauma in the Kingdom of Bahrain: a national pediatric trauma registry pilot study. Injury. Epidemiology. 2021;8(1):42.
Almuneef M, Saleheen H, AlBuhairan F, Al-Eissa M, Al Muntaser M, Al Alem H, et al. Child mortality in Saudi Arabia: time for action at all levels. Int J Pediatr Adolesc Med. 2021;8(3):165–71.
Alkhalaf H, Zuraie M, Alqahtani Ryan N, Alghamdi M, Afif Abdulrahman B, Alqahtani Faisal J, et al. The epidemiology of drowning among Saudi children: results from a large trauma center. Ann Saudi Med. 2021;41(3):157–64.
Aghajani MH, Haddadi M, Saadat S. Epidemiological pattern of injuries in Iran; a nationwide review of seven million emergency department admissions. Arc Acad Emer Med. 2019;7(1).
Aghamohamadi S, Jahangiri K, Kavousi A, Sayah MA. Analysis and forecasting the accident mortality trends in the Islamic Republic of Iran applying lee-Carter model during the years 2006 to 2035. Bulletin Emerg Trauma. 2018;6(4):341–8.
Anary SHS, Sheikhazadi A, Ghadyani MH. Epidemiology of drowning in Mazandaran Province, north of Iran. Am J Forensic Med Pathol. 2010;31(3):236–42.
Astaraki P, Mahmoudi G, Ahadi M, Almasi V. The reasons of death among children and adolescents in Lorestan Province, west of Iran, from 2007 to 2014. Int J Med Toxicol Forensic Med. 2016;6(2):65–70.
Barzegar A, Ghadipasha M, Aram S, Khademi A. Suicides, homicides, and fatal occupational accidents in Iran: a cross-sectional, retrospective study based on autopsy reports; need to develop preventive strategies. Iran Red Crescent Med J. 2019;21(4):e65672.
Bazeli J, Aryankhesal A, Khorasani-Zavareh D. Epidemiology of special incidents: results from national mortality and morbidity registry and the associated factors in Iran in 2014. Electron Physician. 2017;9(8):5113–21.
Bozorgi F, Derakhshanfar H, Hoseininejad SM, Abbasi A, AbolghasemLali MT. Cogitation on routine drowned cases in Mazandaran Province: a CaseStudyinbetweentheYear2008to2013. Ambient Science. 2016;3(2):61–3.
Davoudi-kiakalayeh A, Mohammadi R, Yousefzade-Chabok S, Jansson B. Evaluation of a community-based drowning prevention programme in northern Islamic Republic of Iran. East Mediterr Health J. 2013;19(7):629–37.
Davoudi-Kiakalayeh A, Mohammadi R, Yousefzadeh-Chabok S. Prevention of drowning by community-based intervention: implications for low- and middle-income countries. Arch Trauma Res. 2012;1(3):112–7.
Davoudi-Kiakalayeh A, Dalal K, Yousefzade-Chabok S, Jansson B, Mohammadi R. Costs related to drowning and near drowning in northern Iran (Guilan province). Ocean Coast Manag. 2011;54(3):250–5.
Davoudi-Kiakalayeh A, Mohammadi R, Yousefzade-Chabok S. Maternal beliefs and socioeconomic correlated factors on child mortality from drowning in Caspian Sea coastline. Bull Emerg Trauma. 2014;2(2):86–91.
Derakhshan P, Saeedi Moghaddam S, Saadat S, Ghanbari A, Rezaei N, Khosravi S, et al. Trends in the drowning mortality rate in Iran. Injury Prevention. 2020;26(4):351–9.
Ghodsi Z, Saadat S, Barzegar A, Alaeddini F, Rahimi-Movaghar V, Zafarghandi M, et al. The completeness of the registration system and the economic burden of fatal injuries in Iran. Turkish J Trauma Emerg Surg. 2020;26(5):671–7.
Hajebi A, Ahmadzad-Asl M, Davoudi F, Ghayyomi R. Trend of suicide in Iran during 2009 to 2012: epidemiological evidences from national suicide registration. Iran J Psychiatr. Behav Sci. 2016;10(4).
Hooshangi Z, Salehi S, Amini-Rarani M. Explanatory social variables of under-5 mortality caused by injury in Isfahan Province, Islamic Republic of Iran. East Mediterr Health J. 2020;26(6):660–7.
Khazaei S, Ayubi E, Sanaei Z, Jenabi E, Khazaei L, Amiri J. Epidemiologic characteristics of injuries among 1-5 year-old children in Hamadan Province: analysis of 4523 hospitalized children over a 6-year period. Archives of Trauma Research. 2020;9(1):3–7.
Kiakalayeh AD, Mohammadi R, Ekman DS, Chabok SY, Janson B. Unintentional drowning in northern Iran: a population-based study. Accid Anal Prev. 2008;40(6):1977–81.
Kiakalayeh AD, Mohammadi R, Ekman DS, Yousefzade-Chabok S, Behboudi F, Jansson B. Estimating drowning deaths in northern Iran using capture-recapture method. Health Policy. 2011;100(2–3):290–6.
Mosayebi Z, Movahedian A, Mousavi G. Drowning in children in Iran: outcomes and prognostic factors. Med J Malaysia. 2011;66(3):187–90.
Naghavi M, Pourmalek F, Shahraz S, Jafari N, Delavar B, Motlagh ME. The burden of injuries in Iranian children in 2005. Popul Health Metrics. 2010;8(1):5.
Roudsari BS, Shadman M, Ghodsi M. Childhood trauma fatality and resource allocation in injury control programs in a developing country. BMC Public Health. 2006;6(1):117.
Samaneh A, Samaneh A, Hamid S, Ardeshir K, Khosro G. Years of potential life lost due to unintentional drowning mortality in Mazandaran province. Iran World Appl Sci J. 2012;20(10):1433–8.
Shahbazi F, Mirtorabi SD, Mahdavi SAH, Nazari SSH. Trend of mortality rate due to drowning in Iran (2013-2018). Arch Trauma Res. 2020;9(3):111–5.
Sheikhazadi A, Ghadyani MH. Epidemiology of drowning in Isfahan province, center of Iran. J Res Med Sci. 2009;14(2):79–87.
Soori H, Naghavi M. Deaths from unintentional injuries in rural areas of the Islamic Republic of Iran. East Mediterr Health J. 1999;5(1):55–60.
Vahhab E, Gholamzadeh S, Zarenezhad M. Injury-related pediatric mortality in shiraz, Iran: a community-based survey. Shiraz E Med J. 2019;20(2).
Zolala F, Nasehi MM, Moosazadeh M, Azadeh H, Mirzajani M. Epidemiology of drowning in Mazandaran, Iran: a population based study. Middle-East J Sci Res. 2012;11.
Al-Fifi S, Shabana M, Zayed M, Al-Binali A, Al-Shehri M. Drowning in children: Aseer central hospital experience, southwestern Saudi Arabia. J Fam Community Med. 2011;18(1):13–6.
Alghnam S, Alkelya M, Al-Bedah K, Al-Enazi S. Burden of traumatic injuries in Saudi Arabia: lessons from a major trauma registry in Riyadh. Saudi Arabia Ann Saudi Med. 2014;34(4):291–6.
Alghnam S, Towhari JA, Al Babtain I, Al Nahdi M, Aldebasi MH, Alyami M, et al. The associations between injury mechanism and extended hospital stay among pediatric patients: findings from a trauma Center in Saudi Arabia. BMC Pediatr. 2019;19(1):177.
Al-Mofadda SM, Nassar A, Al-Turki A, Al-Sallounm AA. Pediatric Near Drowning: The Experience of King Khalid University Hospital. 2001;21(5–6):300–3.
Al-Qurashi FO, Yousef AA, Aljoudi A, Alzahrani SM, Al-Jawder NY, Al-Ahmar AK, et al. A review of nonfatal drowning in the pediatric-age group: a 10-year experience at a university hospital in Saudi Arabia. Pediatr Emerg Care. 2019;35(11).
Alsaif DM, Almadani OM, Ali Almoghannam S, Hamdi D, Al-Farayedhi MA, Kharosha MA. Child fatalities in Dammam: a call for child fatality reviews in Arab countries. J Forensic Sci. 2018;63(4):1171–5.
Habeeb KA, Alarfaj G. Saudi parents awareness regarding burn, choking, and drowning first aid in children. J Family Med Primary Care. 2020;9(3).
Hijazi OM, Shahin AA, Haidar NA, Sarwi MF, Musawa ES. Effect of submersion injury on water safety practice after the event in children, Saudi Arabia. Saudi Med J. 2007;28(1):100.
Jan MM. Pediatric near-drowning and drowning. Saudi Med J. 2013;34(2):119–22.
He S, Lunnen JC, Zia N, Khan UR, Shamim K, Hyder AA. Pattern of presenting complaints recorded as near-drowning events in emergency departments: a national surveillance study from Pakistan. BMC Emergency Medicine. 2015;15(2):S4.
Khalil ZH, Naeem M, Adil M, Khan MZ-u-I, Abbas SH. Analysis of autopsy record of unnatural deaths in Peshawar district. J Postgrad Med Inst. 2013;27(4).
MAL S, SZA TIRMIZI, WASEEM F, MAKHDOOM PA, IMRAN S, MIRZA FH, et al. Medicolegal analysis of fatal drowning in Karachi: an autopsy based study. PAKISTAN J Med Health Sci. 2020;14(4):1212–5.
Pal MI, Qasim AP, Naeem M, Arshad H, Saeed A. Profile of Asphyxial deaths in Faisalabad: a 10-year study. J Coll Physicians Surg Pak. 2018;28:266+.
Razzak JA, Khan UR, Zia N, Azam I. A child an hour: burden of injury deaths among children under 5 in Pakistan. Arch Dis Child. 2013;98(11):867.
Razzak JA, Luby SP, Laflamme L, Chotani H. Injuries among children in Karachi, Pakistan—what, where and how. Public Health. 2004;118(2):114–20.
Shaikh MA. Risks of drowning and safety concerns at the beaches of Karachi--perspective from lifeguards. J Pakistan Med Assoc 2014;64(5):576–578.
Shaikh MA. Epidemiology of drowning and near drowning at Karachi beaches from 2012 to 2014. J Pakistan Med Assoc. 2016;66(5):602–5.
Siddiqui E, Ejaz K, Siddiqui U. Unintentional, paediatric domestic injury in a semi rural area of Karachi. J Pakistan Med Assoc. 2012;62(7):638.
Waseem H, Carenzo L, Razzak J, Naseer R. Epidemiology of major incidents: an EMS study from Pakistan. Int J Emerg Med. 2011;4(1):48.
Hammett M, Pearse L, Naito N, Watts D, Hooper T. Drowning deaths of U.S. service personnel associated with motor vehicle accidents occurring in operation Iraqi freedom and operation enduring freedom, 2003–2005. Mil Med. 2007;172(8):875–8.
Lin C-Y, Wang L-Y, Lu T-H. Changes in drowning mortality rates and quality of reporting from 2004–2005 to 2014–2015: a comparative study of 61 countries. BMC Public Health. 2019;19(1):1391.
Mavridou A, Pappa O, Papatzitze O, Blougoura A, Drossos P. An overview of pool and spa regulations in Mediterranean countries with a focus on the tourist industry. J Water Health. 2014;12(3):359–71.
Azzopardi P, Cini K, Kennedy E, Sawyer S, El Bcheraoui C, Charara R, et al. Adolescent health in the eastern Mediterranean region: findings from the global burden of disease 2015 study. Int J Public Health. 2018;63(1):79–96.
Soori H, Khodakarim S. Child unintentional injury prevention in eastern Mediterranean region. Int J Crit Illness Injury Sci. 2016;6(1):33–9.
Al Awadhi MA, Abulfateh NM, Board A. Drowning epidemiology in Bahrain. Bahrain Med Bull. 2018;2003-2015, 40(1).
Ruehsen MM, Abdul-Wahab A-WM. The epidemiology of trauma in an intensive care unit in Bahrain. Journal of trauma and acute care. Surgery. 1989;29(1).
Gad ElHak SA, El-Ghazali AM, Salama MM, Aboelyazeed AY. Fatal suicide cases in Port Said city, Egypt. J Forensic Legal Med. 2009;16(5):266–8.
Halawa EF, Barakat A, Rizk HII, Moawad EMI. Epidemiology of non-fatal injuries among Egyptian children: a community-based cross-sectional survey. BMC Public Health. 2015;15(1):1248.
Al-Sammak NI. Types of accidents in Nineveh governorate/Iraq. International journal of psychosocial. Rehabilitation. 2020;24(05).
Bilukha OO, Sultan ASS, Hassan A, Hussain SJ, Leidman E. Injury-related fatalities in selected governorates of Iraq from 2010 to 2013: prospective surveillance. Am J Disaster Med. 2016;11(1):49–58.
Abdullah S, Sharkas G, Sabri N, Iblan I, Abdallat M, Jriesat S, et al. Mass gathering in Aqaba, Jordan, during Eid Al Adha, 2010. East Mediterr Health J. 2013;19.
Atallah AI. Epidemiology of trauma injuries in the districts of Amman, Jordan: problems and suggestions. JEMTAC. 2008;8(1):35–7.
Al Talafieh A, Al Majali R, Al DG. Clinical, laboratory and X-ray findings of drowning and near-drowning in the Gulf of Aqaba. East Mediterr Health J. 1999;5(4):706–9.
Shaheen A, Edwards P. Flying bullets and speeding cars: analysis of child injury deaths in the Palestinian territory. East Mediterr Health J. 2008;14(2):406–14.
Al-Thani M, Al-Thani A-A, Toumi A, Khalifa S, Ijaz MA, Akram H. Trends in the leading causes of childhood mortality from 2004 to 2016 in Qatar. Central Asian J Global Health. 2018;7(1):334.
Al-Mannai L, Selim NAA, Al-kuwari MG, Ismail MFS. Unintentional injuries among preschool children in Qatar: cross sectional study. World Family Medicine Journal. 2014;12(1):36–44.
Bener A, Hussain SJ, Ghaffar A, Abou-Taleb H, El-Sayed HF. Trends in childhood trauma mortality in the fast economically developing State of Qatar. World J Pediatr. 2011;7(1):41–4.
Mlayeh S, Ben Abderrahim S, Haggui F, Ghzel R, Jedidi M. Deadly falls into wells: a retrospective study of 72 autopsy cases from Kairouan. Tunisia J Forensic Sci. 2021;66(3):934–9.
Barss P, Subait OM, Ali MHA, Grivna M. Drowning in a high-income developing country in the Middle East: newspapers as an essential resource for injury surveillance. J Sci Med Sport. 2009;12(1):164–70.
Bener A, Al-Salman KM, Pugh RNH. Injury mortality and morbidity among children in the United Arab Emirates. Eur J Epidemiol. 1998;14(2):175–8.
Borse NN, Hyder AA. Call for more research on injury from the developing world: results of a bibliometric analyss. Indian J Med Res. 2009;129(3):321–6.
Scarr J-P, Jagnoor J. Mapping trends in drowning research: a bibliometric analysis 1995–2020. Int J Environ Res Public Health. 2021;18(8).
Queiroga AC, Seabra R, Franklin RC, Peden AE. Trends in drowning mortality in Portugal from 1992 to 2019: comparing Global Burden of Disease and national data. Injury Prevention. 2021; Published Online First: 31 December 2021.
Clemens T, Peden AE, Franklin RC. Exploring a hidden epidemic: drowning among adults aged 65 years and older. J Aging Health. 2021;8982643211014770.
Peden AE, Franklin RC, Queiroga AC. Epidemiology, risk factors and strategies for the prevention of global unintentional fatal drowning in people aged 50 years and older: a systematic review. Injury Prevention. 2018;24(3):240–7.
Adler-Nissen R, Andersen KE, Hansen L. Images, emotions, and international politics: the death of Alan Kurdi. Rev Int Stud. 2020;46(1):75–95.
Karimi N, Beiki O, Mohammadi R. Risk of fatal unintentional injuries in children by migration status: a nationwide cohort study with 46 years' follow-up. Injury Prevention. 2015;21(e1):e80–7.
Janson S, Schyllander J, Hansson C, Eriksson UB. Children with a single parent are a risk group for drowning. Also immigrant children from the Middle East and Iran are at risk according to a descriptive study. Lakartidningen. 2010;107(24–25):1618–22.
Howland J, Hingson R, Mangione T, Bell N, Bak S. Why are most drowning victims men? Sex differences in aquatic skills and behaviors. Am J Public Health. 1996;86(1):93–6.
Peden AE, Scarr J-P, Mahony AJ. Analysis of fatal unintentional drowning in Australia 2008–2020: implications for the Australian water safety strategy. Aust N Z J Public Health. 2021;45(3):248–54.
Croft JL, Button C. Interacting factors associated with adult male drowning in New Zealand. PLoS One. 2015;10(6):e0130545.
Chauvin M, Kosatsky T, Bilodeau-Bertrand M, Gamache P, Smargiassi A, Auger N. Hot weather and risk of drowning in children: opportunity for prevention. Prev Med. 2020;130:105885.
Fralick MDC, Redelmeier DA. Drowning and the influence of hot weather. PLoS One. 2013;8(8):e71689.
Peden AE, Franklin RC, Willcox-Pidgeon S. Media reporting of summer drowning: a partial picture, useful for advocacy. Health Promotion J Australia. 2020;31(3):491–6.
Sindall R, Mecrow T, Queiroga AC, Boyer C, Koon W, Peden AE. Drowning risk and climate change: a state-of-the-art review. Injury Prevention. 2022;injuryprev-2021-044486.
Peden A, Franklin RC, Leggat PA. Fatal River drowning: identification of research gaps through a systematic literature review. Injury Prevention. 2016;22:202–9.
Peden AE, Franklin RC, Leggat PA. Developing drowning prevention strategies for rivers through the use of a modified Delphi process. Injury Prevention. 2020;26(3):240–7.
Quan L, Bennett E, Moran K, Bierens JJLM. Use of a consensus-based process to develop international guidelines to decrease recreational open water drowning deaths. Int J Health Promot Educ. 2012;50(3):135–44.
Acknowledgements
Not applicable.
Funding
There was no funding associated with this research.
Author information
Authors and Affiliations
Contributions
AP led the design and coordination of the review. AP and AI screened literature and extracted data. AP led the data visualisation and writing of the study. AI reviewed the data visualisation and manuscript. AP and AI revised the manuscript. Both authors approve the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Search Strategy. Table S2. Description of risk/protective factors, their measure of significance and coding methodology. Table S3. Prevention strategies as described in included studies and coding methodology used, Eastern Mediterranean Region. Table S4. Characteristics of included studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Peden, A.E., Işın, A. Drowning in the Eastern Mediterranean region: a systematic literature review of the epidemiology, risk factors and strategies for prevention. BMC Public Health 22, 1477 (2022). https://doi.org/10.1186/s12889-022-13778-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13778-6