
Abstract
Introduction
Drowning is a public health problem in Türkiye, as in the rest of the world. This study aims to systematically review the literature on drowning in Türkiye with a focus on data sources, epidemiology, risk factors and prevention strategies. Methods: Literature searches were conducted using PubMed, SPORTSDiscus, Scopus, Web of Science, Turk MEDLINE, Google Scholar and Google Akademik (Turkish language). Studies (limited to original research written in English and Turkish) reporting drowning (unintentional and intentional; fatal and non-fatal) of residents and tourists in Türkiye were independently dual screened at the title and abstract and full text stages. Study quality was assessed using JBI checklists and evidence level assessed based on study design. Results: From a total of 917 studies, 49 met the inclusion criteria. Most (51%) focused on unintentional fatal drowning. Included studies were most commonly analytical cross-sectional studies (n = 23) and case series (n = 20) meaning the evidence level was low or very low for 48 (98%) studies. Fifteen studies examined drowning at the national level, while sub-national studies (n = 30) focused on urban areas across three provinces: Antalya (n = 6), Istanbul (n = 6), Izmir (n = 4). There was little consensus on risk factors beyond male drowning risk, and no data reported on implemented or evaluated drowning prevention interventions. Discussion: There is a need for more national-level studies to identify the causes of drowning and to guide intervention implementation and evaluation to inform policy makers and donors. Currently official data is limited in its detail, providing age and gender data only, hampering efforts to identify, and thus address, causal factors for drowning. Practical applications: There is currently very little evidence to inform investment in effective drowning prevention interventions in Türkiye. To improve this, data collection systems on drowning in Türkiye need to be strengthened via the development a national drowning registry.
Trial Registration
#CRD42022382615.
Similar content being viewed by others

Introduction
Drowning is recognised as a serious public health problem worldwide. In 2019, more than 230,000 people died due to drowning, mostly in low- and middle-income countries, making drowning the third leading cause of unintentional injury death globally (accounting for 7% of all injury-related deaths) [1]. Studies from several countries identify that such figures likely underreport the true burden of drowning due to the exclusion of water transport and disaster-related drowning [2,3,4], as well as intentional drowning [5]. Drowning can occur in any type of water, such as rivers, lakes, oceans, pools, bathtubs or buckets, and can be classified as fatal or non-fatal depending on whether the outcome of the initial drowning incident [6].
Türkiye, a Eurasian country with 783,577 km2 of land, is surrounded by four seas (the Mediterranean, the Aegean, the Black Sea, and the Marmara) and has many lakes, streams and rivers [7]. The country’s total coastline is 8,592 km long and the area of the coastal provinces accounts for 30% of the whole country. Türkiye’s most populous provinces are generally along the coast [8]. This gives more people access to the sea, thus increasing drowning risk. Moreover, with the rising temperatures in the summer months, more people participate in aquatic activities such as swimming, boating, etc. This leads to fatal and non-fatal drowning incidents in Türkiye [9]. Although there are lifeguards on all major beaches, people may choose to enter the water in more rural areas. Also, in rural areas, irrigation canals, lakes, dams, rivers and streams are seen as significant risk factors for drowning. It is thought that the number of drownings increases in these areas due to the lack of protective measures (such as warning signs and rescue equipment) [10].
Drowning is a significant issue across the European region [11], including in Türkiye, where the prevention of drowning is challenging due to a lack of reliable and comprehensive data on its burden and risk factors [7]. The number of drowning deaths and crude mortality rate in Türkiye is uncertain due to different data sources (media data, clinic reports and autopsy records) which use different definitions thus affect the accuracy of estimates of drowning mortality in Türkiye. Further, the exclusion of flood-related drowning deaths and water transportation-related drownings [10] also risks underrepresenting the true burden. Further, there is no total population level data capture on non-fatal drowning in Türkiye. Therefore, more comprehensive and consistent data on drowning in Türkiye are needed to inform prevention strategies and policies [7].
Given of the lack of consolidated information on drowning in Türkiye, this systematic literature review aimed to identify and synthesise the published literature on drowning burden, data sources, risk factors and prevention strategies in Türkiye, with the aim of informing next steps for drowning prevention in the country.
Materials and methods
The protocol for this systematic review was prospectively registered with PROSPERO (#CRD42022382615) and conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [12].
Literature search
Searches were conducted using PubMed, SPORTSDiscus, Scopus, Web of Science, and Turk MEDLINE from inception to 9th December 2022. The inclusion and exclusion criteria are presented in Table 1. Search terms included drown*, immers*, submers*, swim*, a variety of aquatic locations (i.e., river, lake, sea, beach, pool) and Turk*. Full search strategies can be found in Table S1. These were tailored to suit each journal and based on consultations with a specialist librarian and a previous literature review of drowning [13]. Search strings were also devised in such a way as to capture more relevant information, for example, cases classified as drowning not just deaths or incidents in water, and swimming as it pertains to drowning prevention and not competitive swimming or the biomechanics of swimming.
After database searches were run, additional searches of boğulma* AND Türk were run using Google Akademik (Turkish language by author AI) and drown* AND Turk* in Google Scholar (English language by author AP) to identify any articles not found via database searches. Authors screened results until 10 pages of nil results. As a result of these searches, no new articles were identified. Databases were chosen based on their relevance to drowning from a previous review of drowning in a neighbouring region [13], in addition to the use of Turk MEDLINE and Google Akademik to capture Turkish literature not indexed in the other databases.
Study selection
Two authors (AI and AP) conducted a dual independent review of the title and abstract followed by full-text screening with conflicts resolved via consensus. One Turkish-speaking author (AI) reviewed Turkish language literature, clarifying any concerns with author (AP). Study screening was performed using Covidence literature screening software [14].
Data extraction
Data extraction was undertaken by one author (AI) with an independent quality check of 20% of included records undertaken by a second author (AP). Data extraction was undertaken using a Microsoft Excel Spreadsheet custom-built for this purpose. Data were extracted on the following aspects: Study characteristics (which included author name, year published, years of study, study population, study design and data source(s)), epidemiology, risk factors, and prevention strategies.
The epidemiology of drowning was reported as numbers, proportions, or rates per 100,000 for each population reported (overall, by age group, by year, by gender, etc.) in the included studies. No inferred rates were calculated. Drowning was described by outcome (fatal, non-fatal, both, not specified), and intent (unintentional, intentional, both, not specified) and examined at a total population level, as well as by age group and gender.
We coded the free text description of data sources, risk/protective factors, and prevention strategies by consensus. Risk/protective factors were those that had a significant association with the risk of drowning or drowning outcome (e.g., chi square tests of significance [p < 0.05], odds ratio, relative risk). We extracted prevention strategies that were proposed, implemented and/or evaluated. We classified prevention strategies as being primary (before the drowning occurs), secondary (reduce the impact of a drowning which has already occurred), or tertiary prevention (reduce the ongoing effects of a drowning incident) [15] and also aligned strategies to the Hierarchy of Control [16]. We also noted if the prevention strategy involved multi-sectoral action (as recommended by the WHO [17]) and which sectors were involved.
Quality appraisal
Quality assessment of included studies was performed by two members of the review team using the Joanna Briggs Institute (JBI) Critical Appraisal Tools based on study type. The first author (X1) assessed all articles and then the other author (X2) randomly assessed 20% of the articles. Disagreements between the two authors were resolved by discussion. Checklists provide a score based on assessment of a range of study design criteria. Study design of the included studies were graded according to the National Health and Medical Research Council's (NHMRC) levels of evidence, which range from level I (a systematic review of Level II studies [randomised controlled trial]) to level IV (case studies with either post-test or pre-test/post-test outcomes) (Table S2).
Results
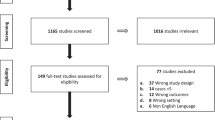
Database searching yielded 917 studies. After removal of 79 duplicates, 838 studies were screened by title and abstract for inclusion. Of these, 735 studies were deemed irrelevant and excluded. The remaining 103 full text studies were screened for eligibility. In total, 54 studies were removed at full text review and data were extracted from the remaining 49 studies which satisfied the inclusion criteria (Fig. 1).

PRISMA flow chart
Study characteristics
Among the 49 included studies, the publication dates ranged from 2004 to 2022. The included studies were predominately analytical cross-sectional studies (n = 23; 47%) and case series (n = 20; 41%). The remaining studies comprised four prevalence studies, one qualitative study and one quasi-experimental study. Included studies mostly used autopsy data (n = 21; 43%) or medical reports (n = 13; 27%), followed by media reports (n = 8; 16%). Based on study design, the overall level of evidence was low, with almost all studies (n = 48) ranked as low or very low on the NHMRC Levels of Evidence criteria (Table S2). When assessed using JBI checklists based on study type, 23 studies (47%) recorded a score of 7 or above.
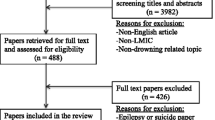
Fifteen included studies reported drowning at the national level, while 16 studies reported drowning at the provincial level, most commonly in Antalya (n = 6), Istanbul (n = 6) and Izmir (n = 4) (Fig. 2). More than half of the included studies reported data at the sub-national level (n = 30; 61%), followed by 16 studies (33%) reporting national data and 3 studies (6%) reporting on foreign visitors to Türkiye. No studies examined drowning among migrants, either once they had arrived in Türkiye or while in transit. Most of the studies (27 out of 49; 55%) reported data from urban areas, while two studies (4%) reported data from rural areas. Some studies (20 out of 49; 41%) reported data from both urban and rural areas. Fatal drownings were the focus of 36 studies, while both fatal and non-fatal drownings were included in 12 studies. While 18 of these studies examined unintentional drownings only, seven examined both intentional and unintentional drownings. The remaining 24 studies did not distinguish between intentional and unintentional drownings (Table 2).

Heatmap of sub-national studies by location
Burden and risk factors
One of the more commonly reported risk factors for drowning in Türkiye was gender [7, 10, 27, 31, 34]. Three studies presented drowning mortality rates per 100,000 people [7, 9, 34]. In these studies, the drowning rates for males were 1.8 (between 2005 and 2017), 0.52 (2015–2019) and 1.44 (2007–2011), respectively, while the corresponding rates for females were 0.48, 0.06 and 0.28 (Table 3). Only one study reported a higher proportion of females drowning (60%) than males (40%), though case numbers were small [47].
Studies showed different rates in different age groups, with different data sources, and focusing on different regions. However, the general trend was that about 70% of drowning cases were male. Işın et al. (2020) reported that the drowning rate for children under 18 years of age was 1.18 per 100,000 for males and 0.48 for females. It also showed that the risk of fatal drowning was almost four times higher for males (relative risk: 3.98) than females [7].
Few and varied mortality rates were reported in the included studies because of differences in data sets and populations. Turgut and Turgut (2014) found that drowning rate of 0.89 per 100,000 people in Türkiye based on media reports [9]. A similar study by Işın et al. (2020) found a rate of 1.17 per 100,000 children aged 0–18 years [7]. Çaylan et al. [27] found that the rate in children under 5 years of age decreased from 1.1 per 100,000 population in 2014 to 0.7 in 2017. In another study also conducted in children [7], it was reported that the rate of drowning, which was in an upward trend from 2005 to 2010, decreased every year until 2017 to 0.78 per 100,000 children after peaking in 2010. In a study conducted on the whole population [10], it was found that the drowning rate has been on a downward trend every year since 2015 (1.24 per 100,000 people) and decreased to 0.64 in 2019 (Table 3).
Out of 16 studies that reported number of deaths in age groups, only 10 presented data for the 0–19 years age group. The total number of deaths reported varied from 1 to 1,086. There was no consensus on the age group with the highest burden of drowning; a population-based study showed the 65 + years age group as recording the highest number of drowning cases [10], while a population-based drowning study showed high drowning numbers in the 10–14 years age group [7] (Table 4). A study focusing on child drowning found that the drowning rate per 100,000 children by age group varied from a low of 0.73 for 0–4 year-olds, increasing with age to a high of 2.11 for adolescents aged 15–17 years [7]. According to a study of rescue-related drowning, the age group with the highest risk of drowning per 100 000 persons was 15–24 years (1.28), followed by 25–34 years with 0.78 [34].
Fatal drownings by water location were reported in 16 studies. In Türkiye, the most common environments where fatal drownings occur were Beach/Sea, Stream/River/Creek, and Irrigation channel, respectively. The Beach/Sea was the most common drowning location in 5 studies, followed by Stream/River/Creek in 4 studies and lake in 2 studies. Bucket, Irrigation Channel, Hole/Well and Pool were each the most frequent drowning location in 1 study (Table 5). The sea/beach was the most common place for drowning across all age groups, but buckets were the main cause of drowning for children aged 0–4 years, while streams/rivers/creeks and irrigation channels were more prevalent for older children. Among rescuers, lakes/ponds and rivers were frequent drowning sites (Table 6).
Beyond gender, age and water location, several other drowning risk and protective factors were identified in the included literature. Results differed with respect to season, with winter found to have statistically significant lower drowning risk than Summer [27], while in Summer drowning rescues were more likely to be successful when compared to other seasons [34]. Among fatal and non-fatal drowning of children < 18 years, receipt of CPR and Noninvasive ventilation (NIV) treatment were associated with survival to hospital admission and a shorter stay in hospital respectively, whereas poorer vital signs led to poorer outcomes [44] (Table 6).
Prevention strategies
Identified prevention strategies included supervision for children aged ≤ 18 years, first aid education, data/research, rescue skills education (including throw rescues) and training, and swimming education. All were proposed strategies with no implementation or evaluation reported. All were classified as administrative on the Hierarchy of Control, representing lower order strategies in terms of likely effectiveness. Strategies were reasonably evenly spread across primary (four strategies), secondary (four strategies), and tertiary (three strategies) prevention. Most of the strategies (nine out of 11) involved more than one sector, with education and health being the most commonly co-occurring sectors (Table 7).
Discussion
This study aimed to identify and synthesise the studies that have addressed drowning in Türkiye to date, examining data sources, epidemiology, risk factors and prevention strategies. Despite being a public health concern across Europe [11], our review identifies limited literature on drowning in Türkiye and low consensus on drowning risk factors. This lack of understanding on causal factors for drowning in Türkiye is thus manifest with no implementation or evaluation of drowning prevention strategies identified in the included literature [7, 64].
Little is known about the crude drowning rate in Türkiye. The most important reason for this is that most of the conducted studies in Türkiye were based on autopsy or clinical/medical reports. Studies using these sources are not generalisable as they usually focus on a single centre (hospital, forensic medicine) or a province/region. This was insufficient data presented in many of the included studies to calculate mortality rates. In addition, many population-based studies used media reports of drowning as their source of data. While media reporting can be useful in the absence of routinely collected data, and in Türkiye supplements the meagre detail provided from the national statistics authority [10], it is not without its limitations. Previous research has indicated a bias towards more newsworthy incidents and incidents which occurred in urban settings [65]. Therefore, such data must be interpreted with caution and provides further support for the establishment of detailed and timely routine data collection on drowning such as via a national registry [66].
Where drowning mortality rates were reported, the rates among children were lower than those of neighbouring countries such as Iran, albeit with different data capture methods used [13].
Studies presenting crude drowning rates of different years and populations in Türkiye showed that drowning in Türkiye has been on a decreasing trend recently. Declining drowning rates in Türkiye appear to mirror those reported globally [67], as greater effort and funding is directed toward the issue [68], particularly investment in those interventions known to be effective in young children [69]. However, there is a need to expand this investment into the adolescent age group who experience high drowning rates with relatively lower investment [70]. Additionally, there is a need to ensure drowning fatalities across both urban and rural settings are captured [10], as well as better exploration of the impact of non-fatal drowning, particularly on the Turkish health system.
There was little consensus on risk factors for drowning in Türkiye, within the identified literature, aside from the consensus regarding male drowning risk being greater than female [7, 10, 34]. This is broadly consistent with many other studies globally [67, 71,72,73].Based on the included studies, three possible reasons may account for the higher drowning rates among male in Türkiye; first, being males are more exposed to water than female. Thus, they spend more time in the water doing activities such as fishing, swimming, cooling off, boating, etc. [7, 9, 38]. Another reason could be that males are less likely to wear life jackets than female [7]. Finally, it is believed that male’s participation in the above activities under the influence of alcohol and drugs increases the risk of drowning in favour of male. Although the data didn’t meet the criteria to be included as a risk factor in our analysis, three studies suggested that alcohol consumption may be a preventable risk factor for drowning in Türkiye [37, 46, 59], particularly among males [37]. However, studies examining the impact of alcohol on drowning in Türkiye should consider the use of objective measures of alcohol consumption and intoxication such as recording blood alcohol concentration.
Another risk factor was age [7, 10, 27, 34]. Most of the included studies focused on children and adolescents, but some also evaluated all age groups. The results of these studies showed that children, adolescents, and individuals over 65 years of age had a higher risk of drowning than other ages. Effective drowning prevention interventions for young children are well understood, comprising active supervision, restricting access to water, water familiarisation [7] and cardiopulmonary resuscitation (CPR) as a tertiary response [44]. It may be that greater public education on strategies to reduce child drowning risk are needed within Türkiye [51], though the baseline knowledge is not currently known. The results of a study on drowning in swimming pools in Türkiye highlight the need to provide safer environments to prevent drowning in swimming pools. It is stated that lack of adequate safety measures and supervision is the cause of a significant proportion of child drownings. It was concluded that there is a need to close the pool edges with safety fences and to raise awareness of public by hanging information and warning signs at the edge of the pool [64], although such legislation is yet to have been implemented. While such approaches are likely to reduce drowning among young children, globally there is little evidence regarding effective drowning prevention interventions for adolescents and older people [70, 74].
Seasons were another risk factor for drownings in Türkiye. Fatal drowning cases increased in summer and decreased in winter [7, 27, 34]. People attended water environments for activities such as cooling off, swimming, fishing, boat trips, etc. [7]. Especially in the summer months, when the temperatures rose and the schools closed, people visited water environments such as sea, dam, lake, etc. more often [9, 64]. This led to more drownings due to a lack of supervision [7], inability to swim [64], swimming in areas without lifeguards [49], etc. Therefore, the authors recommended swimming education as a prevention strategy [51]. In addition, we recommend increased public education and awareness campaigns regarding drowning risk reduction strategies ahead of high-risk periods such as summer and school holidays.
Aquatic location was also identified as a risk factor for drowning, although there was little consensus in the included studies. Türkiye has many natural water bodies including four seas, numerous lakes, dams, and rivers [7], leading to natural water bodies being a leading location for all-age drowning. Results of this review show that drownings in areas close to the coastline were mostly in the sea [19, 24, 31], while lake, rivers and irrigation canals were the main drowning places in landlocked or inland areas [58]. the findings of the current systematic review showed that most studies focused on drownings in a single province or region. This resulted in different locations being the leading sites for drowning cases/deaths for children and adults, based on their geographical location. Drowning prevention interventions in Türkiye must be tailored to the accessible water bodies and practices around interaction with water in the different localities.
Although still facing drowning risk from natural waterbodies where adults drown, such as the sea and rivers, creeks and streams, this review also highlight the drowning risk for children posed by buckets [18] and irrigation channels [7, 28]. Updated research is needed to determine whether water storage practices have changed over time since Asurdizer et al.’s analysis of cases between 1996 and 2000 [18], including the potential role of water and sanitation hygiene advancements in changing child drowning risk profile. An absence of adult supervision combined with a lack of swimming ability contribute to drowning risk in irrigation channels. Therefore, parental education campaigns on supervision, as well as the provision of basic swimming and water safety education at the primary school level in Türkiye may assist in preventing future drowning incidents [50].
With respect to the ocean, Işın et al. [34] analysed the drownings of rescuers and found that rescues were more successful in the sea. The main reason for this is that seas are places where lifeguards are present and are visited by more people than other water environments. This increases the chance of rescue when more professionals intervene to save drowning people. Therefore, Işın et al. [34] suggested that rescue skill training and education would be an important prevention strategy, especially to prevent multiple drowning deaths.
Finally, lack of official data and limited data are considered as a barrier to the calculation of the burden of drowning in Türkiye [7]. Failure or limited determination of the burden of drowning and its underlying causes delays the planning of drowning prevention strategies. Previous studies in Türkiye have reported inadequate official records on drowning [7, 9, 34, 64]. Due to the limited availability of official sources, most studies on drowning in Türkiye have obtained data either from autopsy reports [19, 59] or medical reports (patient information form, electronic medical records, medical charts, and nursing records, etc.) [24, 43, 44]. However, such studies investigated drowning by analysing patient records or autopsy data from a region, a province, or one or more hospitals. Therefore, these studies were not successful in providing generalisable data on the total population burden of drowning in Türkiye due to their relatively small samples. Due to the lack of official records or limited information available to analyse the burden of drowning, researchers have analysed drowning in Türkiye from cases obtained from media reports [7, 9, 34, 64]. Although this type of research has some reported limitations, it has provided important findings because of its generalisable conclusions and its contribution to revealing the main gaps in Türkiye to prevent drowning. Official mortality data, triangulated with police and media reports, are needed to identify causal factors to inform, and in future evaluate, risk reduction initiatives. Although Işın and Peden (2022) obtained data from TurkSTAT, which use the death notification system, only gender and age group were analysed in the study because TurkSTAT provides very limited information [10]. While this contributes to the epidemiology of drowning in Türkiye, it is insufficient to formulate prevention strategies. As has been proposed in other European countries, a National Drowning Registry needs to be developed in Türkiye in order to collect drowning data efficiently [66]. The adoption of a non-fatal drowning definition that is consistently applied to capture non-fatal drowning cases in Türkiye in this registry would also be advisable.
Strengths and limitations
To the best of our knowledge, this is the first systematic review of the published literature on drowning in Türkiye in terms of data sources, epidemiology, risk factors and prevention strategies. It is bolstered by examining publications in both English and Turkish language, as well as exploring publications from inception. However, it is not without its limitations. Turkish language studies could only be screened by one author due to the native language of the second author, which may have weakened the rigour around article screening and data extraction. Search strategies using different terms or combinations of terms, may have produced different results in terms of literature yielded. This review included primary studies published in peer-reviewed literature only. There may also be relevant information on the issue of drowning and its prevention within Türkiye published in the grey literature. The heterogenous nature of the studies made comparison difficult and a meta-analysis not possible.
Conclusion
This research has highlighted the need for more generalised studies to better understand and estimate the burden of drowning deaths in Türkiye. Most of the studies were autopsy-based and focused on specific regions, or cities, which limited their generalisability. Thus, the burden of drowning in Türkiye was mostly calculated with media reports, which had some limitations and biases. There is a need for more research to support greater consensus on risk factors, to inform prevention interventions. However, the lack of accurate and comprehensive data remains a significant barrier to advancing drowning prevention efforts in Türkiye. We recommend the establishment of a national drowning data registry to capture fatal drowning incidents, before considering the inclusion of non-fatal drowning events. The consistent collection and timely analysis of such data are vital to saving lives from drowning in Türkiye.
Availability of data and materials
All data generated or analysed during this study are included in this published article (and its Supplementary information files).
References
World Health Organization. Drowning. 2021 [cited 2023 January 27, 2023]; Available from: https://www.who.int/news-room/fact-sheets/detail/drowning.
Peden AE, et al. Using a retrospective cross-sectional study to analyse unintentional fatal drowning in Australia: ICD-10 coding-based methodologies verses actual deaths. BMJ Open. 2017;7(12): e019407.
Lunetta P, Penttilä A, Sajantila A. Drowning in Finland:“external cause” and “injury” codes. Inj Prev. 2002;8(4):342–4.
Passmore J, Ozanne-Smith J, Clapperton A. True burden of drowning: compiling data to meet the new definition. Int J Inj Contr Saf Promot. 2007;14(1):1–3.
Haw C, Hawton K. Suicide and self-harm by drowning: a review of the literature. Arch Suicide Res. 2016;20(2):95–112.
Peden AE, et al. Understanding the full burden of drowning: a retrospective, cross-sectional analysis of fatal and non-fatal drowning in Australia. BMJ Open. 2018;8(11):e024868.
Işın A, Akdağ E, Turgut A. The epidemiology of fatal drowning in children: a 13-year retrospective study in Turkey. Int J Inj Contr Saf Promot. 2020;27(4):465–71.
Uzun B, Celik N. Sustainable management of coastal lands: A new approach for Turkish Coasts. Ocean Coast Manag. 2014;95:53–62.
Turgut A, Turgut T. A population-based study on deaths by drowning incidents in Turkey. Int J Inj Contr Saf Promot. 2014;21(1):61–7.
Işın A, Peden AE. Assessing variations in estimates of drowning mortality in Turkey from 2013 to 2019. Archives of public health. 2022;80(1):178.
Peden AE, et al. Closing the gap for drowning prevention across Europe. Lancet Public Health. 2022;7(9):e728–9.
Moher D, et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ. 2009;339:2535.
Peden AE, Işın A. Drowning in the Eastern Mediterranean region: a systematic literature review of the epidemiology, risk factors and strategies for prevention. BMC Public Health. 2022;22(1):1477.
Veritas Health Innovation. Covidence systematic review software. 2021 19–09–2021]; Available from: www.covidence.org.
Pless IB, Hagel B. Injury prevention: a glossary of terms. J Epidemiol Community Health. 2005;59(3):182.
National Safety Council. The Hierarchy of Controls. 2019 03–02–2019]; Available from: https://www.safetyandhealthmagazine.com/articles/16790-the-hierarchy-of-controls.
World Health Organization, Preventing drowning: an implementation guide. Geneva: World Health Organization; 2017.
Aşırdizer M, et al. Infant and adolescent deaths in Istanbul due to home accidents. Turk J Pediatr. 2005;47:141–9.
Atilgan M, et al. Deadly stays: A 10-year autopsy study of deaths in hotels in Antalya. Turkey Journal of forensic sciences. 2022;67(3):1116–23.
Azmak D. Asphyxial deaths: a retrospective study and review of the literature. Am J Forensic Med Pathol. 2006;27(2):134–44.
Barlas B, Beji S. Rip current fatalities on the Black Sea beaches of Istanbul and effects of cultural aspects in shaping the incidents. Nat Hazards. 2016;80:811–21.
Başol N, Baydın A, Yardan T. A retrospective evaluation of patients admitted emergency department due to drowning. Journal of Experimental and Clinical Medicene. 2012;29:121–5.
Beydilli I, et al. Mortality across drowning in the view of the meteorological parameters: Relative humudity and sea wavelength. Biomed Res. 2017;28(1):61–5.
Çakmakcı S, et al. Therapeutic Approaches and Mortality in Acute Respiratory Failure due to Drowning. Turkish Thoracic Journal. 2021;22(6):477.
Canturk N, et al. Evaluation of the deaths due to drowning autopsied between 2003 and 2006 in Ankara. TURKIYE KLINIKLERI TIP BILIMLERI DERGISI. 2009;29(5):1198–205.
Canturk N, et al. Medico-legal child deaths in Istanbul: data from the Morgue Department. Pediatr Int. 2007;49(1):88–93.
Çaylan N, et al. Evaluation of injury-related under-five mortality in Turkey between 2014–2017. Turk J Pediatr. 2021;63(1):37–47.
Dirlik M, Bostancıoğlu B. Child drowning deaths in Aydin province, western Turkey, 2002–2012. Eur J Trauma Emerg Surg. 2015;41:683–8.
Dogan KH, et al. Dead bodies found in wells. Am J Forensic Med Pathol. 2010;31(3):208–12.
Esiyok B, Balci Y, Ozbay M. Bodies recovered from wells, sewerage systems and pits: what is the cause of death? Annals-Academy of Medicine Singapore. 2006;35(8):547.
Güzel A, et al. Drowning and near-drowning: experience of a university hospital in the Black Sea region. Turk J Pediatr. 2013;55(6):620.
Hsieh W-H, Wang C-H, Lu T-H. Drowning mortality by intent: a population-based cross-sectional study of 32 OECD countries, 2012–2014. BMJ Open. 2018;8(7):e021501.
Işik M, Eşitti Ş. Content analysis of printed news media related to drowning incidents in Turkey. Hum Ecol Risk Assess Int J. 2015;21(4):1050–61.
Işın A, Turgut A, Peden AE. Descriptive epidemiology of Rescue-Related fatal drowning in turkey. Int J Environ Res Public Health. 2021;18(12):6613.
Ketenci HÇ, et al. Drowning in submerged cars caused by traffic accidents. Turk J Trauma Emerg Surg/Ulusal Travma ve Acil Cerrahi Dergisi. 2022;28(8):1115–21.
Koca E, et al. Evaluation of fatal diving accidents in Turkey. Undersea Hyperb Med. 2019;45(6):633–8.
Lakadamyalı H, Doğan T. Türkiye’de bir turizm yöresinde suda boğulma olgularının irdelenmesi. Türkiye Klinikleri Tıp Bilimleri Dergisi. 2008;28(2):143–8.
Lapa TY, Turgut A, Turgut T. Deaths by drowning incidents during recreational boating and similar activities. World Appl Sci J. 2012;17(2):233–8.
Lin C-Y, et al. Unintentional drowning mortality, by age and body of water: an analysis of 60 countries. Inj Prev. 2015;21(e1):e43–50.
Mollaoğlu M, Bolayir E. Injuries in patients with epilepsy and some factors associated with injury. Nöro Psikiyatri Arşivi. 2013;50(3):269.
Orhan İ. Sinking or Swimming: The Need for Water Safety and Swimming Education in the 21st Century. International Journal of Applied Exercise Physiology. 2020;9(6):263–9.
Petrucci O, et al. Flood fatalities in Europe, 1980–2018: Variability, features, and lessons to learn. Water. 2019;11(8):1682.
Şık N, et al. Early application of non-invasive ventilation for children with pulmonary edema after drowning. Pediatr Int. 2022;64(1): e14858.
Şık N, et al. A reappraisal of childhood drowning in a pediatric emergency department. Am J Emerg Med. 2021;41:90–5.
Şimşek Y, Satar S, Suda Boğulma ve Acil Servis. Turk J Emerg Med. 2013;13(2):81–5.
Söyüncü S, et al. Acil servise suda boğulma veya boğulayazma nedeniyle başvuran hastaların prognozunun belirlenmesinde GKS ve REMS skorlarının değerliliği. Turkish Journal of Emergency Medicine. 2008;8(2):067–72.
Taskesen M, Pirinççioglu AG, Yaramis A. Drowning and near-drowning in children in the southeast of Turkey. Eurasian Journal of Emergency Medicine. 2015;14(1):16.
Tunçez FT, et al. Evaluation of autopsied refugee deaths in Izmir, Turkey. Med Sci Law. 2022;62(3):199–205.
Turgut A. A study on multiple drowning syndromes. Int J Inj Contr Saf Promot. 2012;19(1):63–7.
Turgut A, Turgut T. A study on rescuer drowning and multiple drowning incidents. J Safety Res. 2012;43(2):129–32.
Turgut T, Yaman M, Turgut A. Educating children on water safety for drowning prevention. Soc Indic Res. 2016;129:787–801.
Uzun I, et al. Foreigners dying in Istanbul. J Forensic Sci. 2009;54(5):1101–4.
Yayci N, et al. The review of autopsy cases of accidental childhood deaths in Istanbul. J Forensic Leg Med. 2011;18(6):253–6.
Balcı Y, et al. Muğla’da Otopsisi Yapılan Gençlik Yaş Grubuna Ait Olguların Değerlendirilmesi. Adli Tıp Bülteni. 2018;23(3):156–61.
Yıldırım A, Polater E, Bütün C. 0–6 Yaşlar Arası Adli Nitelikli Çocuk Çağı Medikolegal Ölümlerinin Retrospektif Olarak Değerlendirilmesi. Adli Tıp Bülteni. 2020;25(2):65–71.
Küçük MP, et al. Yoğun Bakımda İzlenen Boğulma Olgularında Sonlanımı Etkileyen Parametreler: Sekiz Yıllık Retrospektif Hasta Verileri. Turk J Intensive Care. 2020;18(1):13–20.
Cömert SŞ, et al. Suda boğulma nedeniyle hastanede yatan olgularin özellikleri ve prognostik bulgular. İzmir Göğüs Hastanesi Dergisi. 2014;28(3):161–9.
Türkoğlu A, et al. Elazığ’da 2005–2012 yılları arasında meydana gelen suda boğulma olgularının retrospektif değerlendirilmesi. Fırat Tıp Derg. 2014;19(3):145–50.
Beydilli I, et al. Factors affecting drowning-related mortality of elderly foreigners according to autopsy results. Turk J Geriatr/Türk Geriatri Dergisi. 2016;19(2):81–6.
Demir U, et al. Beş yaşın altındaki çocukların kazayla ölümlerinin analizi. J Forensic Med. 2017;31:1.
Tutanç M, et al. Çocuk yoğun bakım ünitesine yatan hastaların değerlendirilmesi. Duzce Medical Journal. 2011;13(3):18–22.
Tutanç M, et al. Çocuk yoğun bakım ünitesinde takip edilen suda boğulma ve boğulayazma olguları. Adli Tıp Dergisi. 2011;25(3):177–82.
Arslan MM, et al. Adana’da 1997–2001 yılları arasında otopsisi yapılan çocukluk çağı ölüm olgularının retrospektif olarak değerlendirilmesi. Adli Tıp Bülteni. 2004;9(2):37–42.
Turgut A, Işın A, Akdağ E. Yüzme havuzlarındaki suda boğulma vakalarının incelenmesi. İstanbul Üniversitesi Spor Bilimleri Dergisi. 2018;8(1):69–76.
Peden AE, Franklin RC, Willcox-Pidgeon S. Media reporting of summer drowning: A partial picture, useful for advocacy. Health Promot J Austr. 2020;31(3):491–6.
Queiroga AC, et al. Trends in drowning mortality in Portugal from 1992 to 2019: comparing Global Burden of Disease and national data. Inj Prev. 2022;28(4):318–24.
Franklin RC, et al. The burden of unintentional drowning: global, regional and national estimates of mortality from the Global Burden of Disease 2017 Study. Inj Prev. 2020;26(Supp 1):i83–95.
United Nations. Resolution on Global Drowning Prevention. 2021; Available from: https://www.undocs.org/en/A/75/L.76. (Date cited: 24-05-2023)
Rahman A, et al. Drowning: Global Burden, Risk Factors, and Prevention Strategies. Oxford Research Encyclopedia of Global Public Health. 2021. Retrieved 18 Feb. 2024 from https://oxfordre.com/publichealth/view/10.1093/acrefore/9780190632366.001.0001/acrefore-9780190632366-e-307.
Peden AE, et al. A systematic review of the evidence for effectiveness of interventions to address transport and other unintentional injuries among adolescents. J Saf Res. 2023;85:21–338.
Peden AE, et al. Adolescent transport and unintentional injuries: a systematic analysis using the Global Burden of Disease Study 2019. The Lancet Public Health. 2022;7(8):e657–69.
Howland J, et al. Why are most drowning victims men? Sex differences in aquatic skills and behaviors. Am J Public Health. 1996;86(1):93–6.
Koon W, et al. Burden of fatal drowning in California, 2005–2019. Inj Prev. 2023;29:371–7.
Peden AE, Franklin RC, Queiroga AC. Epidemiology, risk factors and strategies for the prevention of global unintentional fatal drowning in people aged 50 years and older: a systematic review. Inj Prev. 2018;24(3):240–7.
Funding
There was no funding associated with this research. Author AP is supported by an [Australian] National Health and Medical Research Council Emerging Leadership Fellowship (Grant ID: APP2009306).
Author information
Authors and Affiliations
Contributions
AI and AP designed and coordinated of the review. AI and AP screened literature and extracted data. AI led the data visualisation and writing of the study. AP reviewed the data visualisation and manuscript. AI and AP revised the manuscript. Both authors approve the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Işın, A., Peden, A.E. The burden, risk factors and prevention strategies for drowning in Türkiye: a systematic literature review. BMC Public Health 24, 528 (2024). https://doi.org/10.1186/s12889-024-18032-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18032-9