
Abstract
Background
The existing epidemiological data cannot represent the situation of undernutrition among Chinese children, particularly those in rural China. Hence, in this community-based cross-sectional study, the prevalence and associated factors of stunting, underweight and wasting among children (age < 6 years) from rural Hunan Province were analyzed.
Methods
Totally 5529 children aged 0 to 71 months and their caregivers were randomly chosen by multistage stratified cluster sampling from 72 villages from rural Hunan, which were distributed in 24 towns of 12 counties. Data about the children and their mothers, caregivers and family conditions was acquired using unified questionnaire, and the length/height and weight of each child were measured using unified instruments. The prevalence of undernutrition among children was evaluated using the length/height for age, weight for age, weight for length/height, and body mass index for age z scores, which were computed according to the 2006 and 2007 WHO Child Growth Standards.
Results
The prevalence of stunting, underweight, and wasting among the 5529 children were 4.4% (241), 3.9% (217), and 4.0% (221), respectively. The significant associated factors on higher risks of undernutrition in the children were low birth weight, maternal gestational weight gain <10 kg (stunting); low birth weight, maternal gestational weight gain <10 kg, ethnicity of caregivers being minority, large family size (underweight); low birth weight, ethnicity of caregivers being minority, large family size (wasting). High education level of caregivers and high family food expenditure were common protective factors for all three types of undernutrition, except that high family food expenditure was not protective against wasting.
Conclusions
The prevalence of stunting, underweight and wasting is low among rural children under age of 6 years in Hunan. As for the measures, the gestational care and reasonable diet of mothers should be strengthened, and nutritional deficiency during pregnancy be avoided, which will prevent low birth weight. The local economic development and the education level of caregivers need to be further improved, especially for minorities.
Similar content being viewed by others


Background
The malnutrition of children includes undernutrition, over-nutrition and micronutrient deficiency. Of them, undernutrition consists of three indices of stunting, underweight and wasting. In particular, stunting and wasting reflect the chronic or acute undernutrition of children, and underweight reveals the current undernutrition status, but cannot differentiate near-term or long-term undernutrition [1]. Different forms undernutrition may coexist in children. Preschool children are at a critical period of growth and development, and undernutrition occurring at this period may cause irreversible near-term and long-term effects on the health of children. Such effects include delayed physical and cognitional development [2,3,4], which even increase the risks of infection, death, hypertension, diabetes and other chronic diseases at adulthood [5].
About 149 million children under 5 years of age suffered stunting and about 49 million children had wasting in 2018 according to data from United Nations Children's Fund (UNICEF) and World Health Organization (WHO) [6]. Undernutrition of children is a major public health problem in developing countries, especially Africa and Southeast Asia. China is a developing country in East Asia. With the rapid socioeconomic development in the past 30 years, the significant increase in average disposable income, the optimization of dietary structure, the improvement of caregivers education level and the medical and health services, the nutrition status of children has been significantly improved [5, 7]. Nationwide nutrition surveys in China show that the prevalence of stunting and underweight among children under 5 years of age between 1990 and 2010 dropped from 33.1% to 9.9% and from 13.7% to 3.6% respectively, but were still up to 20.3% and 8.0% respectively in rural China [5, 7].
In China, the vast majority of poor areas are concentrated in the rural areas of the central and western provinces. Hunan province with medium economic development is located in central China, and the administrative region includes 123 districts/counties in 14 cities. Hunan is dominated by rural population, accounting for 65.1% [8]. Hunan is a multiracial province and is dwelt by 9.5% of minorities, including Miao, Tujia, and Dong. In rural Hunan, the economic development is relatively poor, and the caregivers have low education level and deficient nutritional knowledge, and many children receive unscientific feeding and suffer from undernutrition [9, 10]. A cross-sectional study conducted in 2009 showed that the prevalence of stunting and underweight among children aged 0-7 years in rural Hunan were 16.6% and 7.8%, respectively [11], which were obviously higher than the national average in 2010. Undernutrition of children can be caused by many factors. A number of observational studies show that poor socioeconomic development, inappropriate complementary feeding practices, household food insecurity, diseases of children (e.g. recurrent respiratory infections and diarrhea), inadequate maternal nutritional status, low education level of caregivers, and children left behind by internal migration are all associated with the undernutrition of children [12,13,14,15,16,17].
To further improve the nutrition status of children in poor rural areas, National Health Commission of China extensively implemented children nutrition improvement projects in poor rural areas including Hunan province since 2012, including food supplements and nutrition education [18]. So far, children nutrition improvement projects have been implemented in rural areas of Hunan for eight years. Hence, previous epidemiological investigations are already unable to reflect the current undernutrition levels of children in rural Hunan. Though several children undernutrition investigations have been conducted in rural Hunan recently, the investigated age ranges are narrow and concentrated on under age of 3 years [19,20,21]. In particular, relevant research on preschool children is insufficient [22].
In the new era, systematic study on the undernutrition of children under 6 years of age in rural areas, and discovery of key associated factors are critical for prevention and treatment of undernutrition among children in rural areas. Hence, in this study, a community-based cross-sectional survey was conducted to clarify the status and associated factors of undernutrition among children under 6 years of age in rural Hunan. Some targeted interventions were proposed to improve the nutrition status of rural children.
Materials and methods
Subjects
The subjects were children under 6 years of age (0 to 71 months) and their caregivers from rural Hunan investigated between August and November 2019. The sample size was determined according to relevant equations for cross-sectional studies [23]. Since the stunting prevalence among rural children was estimated to be 16 %[11], the size of a test α was 0.05, permissible error d was 0.10, the designed effect of complex samples was 2 and the non-response rate was 20%, the final sample size was determined to be 5040 (= 2100×2× 1.2).
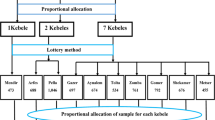
Subjects were selected by multistage stratified cluster sampling. In China, one province consists of several cities, and one city consists of several districts and several counties (districts and counties are urban and rural, respectively); one county contains several towns, and one town has several villages [22]. The 14 cities in Hunan were divided by economic development into three levels: high, moderate and low. Then 2 cities from each economic level, 2 counties from each selected city, 2 towns from each selected county, and 3 villages from each selected town were randomly selected. From each village, all eligible children were included into our subjects. Totally, 5529 children from 72 villages covering 24 towns in 12 counties were involved.
Data collection
This study consisted of a questionnaire survey and anthropometric measurements. The questionnaire included children’s factors (gender, age, birth weight, preterm birth, left-behind children, only child, passive smoking, regular physical examination), maternal gestational factors (age at delivery, gestational gain weight, moderate/severe anemia, pregnancy comorbidity), and factors of caregivers and family (type of caregivers, ethnicity, education level, occupation, family size, family income, family food expenditure). All children received anthropometric measurements, including length/height, and weight.
Definition of variables
Birth weight referred to the infant’s net weight within 1 hour of birth, and did not include any wear or wraps, which can be obtained from the child’s vaccination certificate or medical certificate of birth. If there was no vaccination certificate or medical certificate of birth, the birth weight of the child was obtained from the recalling by the caregivers. The birth weight <2500 g, 2500-3999 g, and ≥ 4000 g were considered as low birth weight, normal birth weight, and macrosomia, respectively. Birth at <37 gestational weeks was regarded as premature birth. Left-behind children referred to those children whose parents (both or either) worked in other places and did not live together with the children [22]. Only child was the only child born by one couple, and had no siblings. Passive smoking meant a nonsmoker inhaled at least 15 minutes every day the smoke exhaled by smokers for at least 1 day within 1 week. Maternal gestational weight gain was determined by the final weight of the mother measured in late pregnancy before delivery subtracted by the weight in early pregnanc y[24] and was divided into four groups of <10.00, 10.00-14.99, 15.00-19.99, and ≥20.00 kg. Maternal moderate/severe anemia was defined as a hemoglobin level <100 g/ L[25]. The maternal hemoglobin concentration in this study was the concentration in the third trimester of pregnancy. The maternal weights in early pregnancy and in late pregnancy before delivery, and the hemoglobin concentration in the third trimester of pregnancy can be obtained from the clinical medical records of maternal health handbook. If there was no maternal health handbook, the maternal weights and hemoglobin concentration during pregnancy were obtained from the recalling by the caregivers. The maternal pregnancy comorbidities included gestational diabetes mellitus, gestational hypertension, pregnancy associated with cardiac diseases, gestational liver diseases, and thyroid dysfunction. Caregivers were those who took care of the diets, living and personal security of children and were divided into two types: parents, and grandparents/others. Ethnicity of caregivers was divided into Han and minorities. The education level of caregivers was classified into primary school or below, junior high school, senior high school, and college or above. The occupation of caregivers was divided into housework, government agencies staff, business service staff, farmer, and others. Family size was defined as the total number of family members and involved the members with economic relations and joint budget and diets, and was separated into ≤4, 5-6, and ≥7.
Anthropometric measurements
The investigators used unified instruments to measure the length/heights and weights of children according to standardized methods, which were described by the Technical Specification for Children Health Check Service (China Ministry of Health, 2012). The lengths and weights of children aged 0-23 months were measured by using an FSG-25-YE lying-form infants and young children precision medical examination meter (Shanghai Betterren Medical Tech Co., Ltd.). The heights and weights of children aged 24-71 months were measured using an HX-200 stadiometer and an HCS-50-RT electronic scale respectively (Liheng Instrumentation LTD., Shanghai, China). The accuracies of instruments for length/heights and weights were 0.1 cm and 0.05 kg, respectively.
Evaluation criteria for children physical development
The commonly-used indices for children physical development are length/height for age, weight for age, weight for length/height, and body mass index (BMI) for age. BMI was calculated using the ratio between a child's weight in kilograms and length/height in meters squared (kg/m2): BMI = weight (kg)/ height2 (m2). A child’s physical development was evaluated using Z-score recommended by WHO: Z score = (analyzed index - median of reference standard)/standard deviation of reference standard. The WHO Child Growth Standards involve two age groups: 0-5 years (0-60 months) and 5-19 years (61-228 months), which are 2006 Child Growth Standar d[26] and 2007 Child Growth Standar d[27]. Hence, the physical development of children was evaluated according to the two age groups above.
-
(1)
Children aged 0-60 months: length/height for age z score (HAZ), weight for age z score (WAZ) and weight for length/height z score (WHZ) were calculated according to WHO 2006 Child Growth Standard. HAZ <-2, WAZ <-2 and WHZ <-2 were defined as stunting, underweight, and wasting respectively.
-
(2)
Children aged 61-71 months: HAZ, WAZ, and BMI for age z score (BMIZ) were calculated according to WHO 2007 Child Growth Standard. HAZ <-2, WAZ <-2 and BMIZ <-2 were defined as stunting, underweight, and wasting respectively.
Quality control
The investigators were the child health care doctors selected from the county-level maternal and child health care hospitals of the corresponding counties. The investigators conducted a face-to- face interview with children’s caregivers. Prior to the survey, all the investigators were trained unifiedly, and only the qualified ones were allowed to take part in on-site survey. The instruments were calibrated before and during investigations. The physique measuring staff measured the length/height and weight of children in strict accordance with the specifications of the instruments. During the survey, all copies of the questionnaire were checked by a quality controller. Each copy should be filled in in a complete and standard way. Any illogical or missed response should be corrected in time. Data were double-inputted on Epidata 3.1 and tested in terms of consistency. For any inconsistent data, the original copy should be checked to ensure the high quality of any inputted data.
Statistical analysis
HAZ, WAZ, WHZ and BMIZ were computed using WHO anthropometric macros in SPSS (igrowup_SPSS and WHO2007_SPSS) [28, 29], and statistical analyses were conducted on SPSS 25.0 (IBM, Chicago, IL, USA). Categorical data was statistically described as proportion or rate. The prevalence of stunting, underweight and wasting among children with different characteristics was compared by Chi-square test. With undernutrition status (stunting, underweight, wasting) as dependent variables (No=0, Yes=1), all 19 factors related to the characteristics of children, mothers, caregivers and families were used as independent variables, and multivariate logistic regression models were developed to identify the associated factors of children’s undernutrition. Variables were selected using a backward selection method. Multivariate logistic regression models were developed separately for each undernutrition status: stunting, underweight, and wasting. The strength of association between significant variables and undernutrition was evaluated by using odds ratios (ORs) with 95% confidence interval (CI). All statistical tests were two-tailed, and the significant level was P<0.05.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Hunan Provincial Maternal and Child Health Care Hospital (No.2019-S036). The study was conducted in accordance with the Declaration of Helsinki. Written informed consents were obtained from all the caregivers of children involved in this study.
Results
Characteristics of children
Totally 5800 copies of the questionnaire were sent out, and 5645 copies were returned, with a reply rate of 97.3%. Of them, 5529 copies were valid, with a valid rate of 97.9%. Of the 5529 children investigated, 50.8% were boys and 49.2% were girls (Table 1). The major age groups were 48- 59 and 60-71 months old, which accounted for 20.8% and 20.1% respectively. The proportions of low birth weight, preterm birth, left-behind children, only child, passive smoking and regular physical examination were 3.7%, 4.8%, 42.4%, 24.7%, 43.8% and 88.5% respectively.
Gestational conditions of mothers
The maternal age at delivery was mainly 25-29 years and 30-34 years, accounting for 30.8% and 40.8% respectively (Table 2). The proportions of maternal gestational weight gain <10.00 kg, moderate/severe anemia, and pregnancy comorbidity were 19.1%, 4.9% and 9.9% respectively.
Characteristics of caregivers and family
As shown in Table 3, the caregivers were mostly parents (67.1%). The ethnicity of caregivers was mostly Han (90.5%), the education level was mainly junior middle school (38.4%), and the dominant occupation was housework (57.4%). The family size was mostly 5-6 members (53.6%), the family annual income was mainly ≥60000 (61.6%), and the family annual food expenditure was mostly ≥6000 Yuan (72.9%).
Prevalence of stunting, underweight, and wasting among children
The prevalence of stunting, underweight, and wasting among the children were 4.4% (241/5529), 3.9% (217/5529), and 4.0% (221/5529) respectively. Table 4 shows a comparison of prevalence of stunting, underweight, and wasting in children with different characteristics. The prevalence of stunting significantly differed with birth weight, preterm birth, maternal gestational weight gain, ethnicity of caregivers, education level of caregivers, and family food expenditure groups (P<0.05). The prevalence of underweight significantly differed with birth weight, preterm birth, maternal gestational weight gain, ethnicity of caregivers, education level of caregivers, family income, and family food expenditure groups (P<0.05). The prevalence of wasting significantly differed with birth weight, preterm birth, regular physical examination, ethnicity of caregivers, education level of caregivers, family size, and family food expenditure (P<0.05).
Associated factors of stunting, underweight, and wasting among children
Multivariate logistic regression analyses showed that low birth weight (<2500 g) and maternal gestational weight gain <10.00 kg were significantly associated with an increased risk of stunting in the children (AOR=3.44, 95%CI: 2.23-5.31; AOR=1.74, 95%CI: 1.04-2.90). High education level of caregivers and high family food expenditure were protective factors against stunting in the children (AOR=0.80, 95%CI: 0.69-0.92; AOR=0.85, 95%CI: 0.73-0.99). Low birth weight (<2500 g), maternal gestational weight gain < 10.00 kg, ethnicity of caregivers being minority and large family size were significantly associated with an increased risk of underweight in the children (AOR=2.86, 95%CI: 1.67-4.90; AOR=1.83, 95%CI: 1.03-3.26; AOR=1.97, 95%CI: 1.35-2.86; AOR=1.26, 95%CI: 1.03-1.55). High education level of caregivers and high family food expenditure were protective factor against underweight in the children (AOR=0.80, 95%CI: 0.69-0.93; AOR=0.86, 95%CI: 0.73-0.98). Low birth weight (<2500 g), ethnicity of caregivers being minority and large family size were significantly associated with an increased risk of wasting in the children (AOR=2.22, 95%CI: 1.24-3.98; AOR=3.45, 95%CI: 2.50-4.77; AOR=1.23, 95%CI: 1.01-1.50). High education level of caregivers was a protective factor against wasting in the children (AOR=0.81, 95%CI: 0.70-0.93) (Table 5).
Discussion
Undernutrition status of children
This study shows that the prevalence of stunting, underweight and wasting among children under 6 years of age in rural Hunan are 4.4%, 3.9% and 4.0% respectively, which are lower compared with the majority of developing countries, especially Southeast Asia (e.g. Pakistan, Bhutan, Myanmar, India), and are close to those of developed countries, such as the US A[15, 30,31,32,33]. A national family health investigation in India during 2015-2016 showed that the prevalence of stunting and underweight among children under 5 years of age were up to 38% and 35% respectivel y[33]. The prevalence of stunting and underweight among children under 6 years of age in rural Hunan reached the requirements of the China Children Development Outline (2011-2020) (be lower than 7% and 5%, respectively).
The possible reason for the low undernutrition prevalence in this study is that the Chinese government has implemented child nutrition improvement projects in poor rural areas recently. As one of the few provinces to first implement the national child nutrition improvement project in poor rural areas of China, the project in 2012 covered 20 counties of Hunan, expanded to 25 counties in 2014, and adjusted to 53 counties in 2018, which covered all poor villages of Hunan. Specifically, all children aged 6-23 months in poor rural areas were provided for free with 1 bag/day of complementary food supplement (Yingyangbao, YYB for short) containing 6 vitamins and 3 minerals (Ca, Fe, Zn), and childhood nutrition knowledge was propagandized to the caregiver s[18].
Associated factors of undernutrition in children
Birth weight
Birth weight is a key indicator about the intrauterine nutrition status of the fetus, and is one of the critical factors that decide postnatal growth and development. A cross-sectional study in Iran demonstrates that the physical development levels (e.g. length, weight, head circumference) of infants with low or extremely low birth weight are significantly lower at the 18-th month compared with infants with normal birth weight [34]. Several observational studies confirm that low birth weight is an independent risk factor of undernutrition in children [15, 35, 36]. The present study finds that low birth weight is the most important influence factor on the undernutrition of children in rural Hunan, and the risks of children with low birth weight to suffer stunting, underweight and wasting are 3.44, 2.86 and 2.22 times those of children with normal birth weight, respectively. Infants with low birth weight more commonly suffer preterm birth or intrauterine growth retardation, and the functions of their organs/systems are undeveloped, such as imperfect sucking and swallowing abilities, poor digestion and absorption, and difficulties in feeding. Moreover, these infants have low autoimmunity and are susceptible to the harmful external environment and diseases, which can lead to the delayed growth and development [37].
Maternal gestational weight gain
The gestational nutrition of the mother is closely related to the child's growth and development [15, 24, 38]. A retrospective cohort study in China shows that the pre-pregnant BMIs and gestational weight gains of mothers are both positively correlated with the WAZ and HAZ of the children aged 12 month s[38]. Data analysis of a National Demographic and Health Survey in Myanmar during 2015-2016 shows that maternal nutritional inadequacy will raise the risks of underweight and wasting among children under 5 years of ag e[15]. Similarly, our study demonstrates that maternal gestational weight gain is related to the undernutrition of children, and weight gain <10.00 kg will increase the risks of stunting and underweight in children by 74% and 83% respectively, but we report no association between maternal gestational weight gain and wasting of children. Though studies show that the increase of maternal gestational weight gain will reduce the risk of undernutrition in children [24], it does not mean the larger weight gain is better, which is because excessive gestational weight gain will in turn increase the risk of overweight/obesity in children [39, 40]. Hence, providing mothers with regular prenatal care and reasonable diet to avoid gestational excessive or insufficient weight gain is significant for malnutrition prevention in children.
Ethnicity of caregivers
Hunan is a multiracial province in Central China and is dwelt by 9.5% of minorities, including Miao, Tujia, and Dong. Though previous studies show the ethnicity of the mother or caregivers is related to the undernutrition of children, the findings are inconsistent [19, 22]. Zhou et al. show that the ethnicity of Miao or Tujia is a protective factor against undernutrition in children, as the prevalence of undernutrition in Miao and Tujia children is lower than that of Han children [19]. A cross-sectional study in rural poor areas of China suggests that ethnicity of Tibetan, Yi or other minorities is a risk factor of stunting in children, as the risks of stunting are 2.35, 1.95 and 1.42 times higher compared with Han childre n[22]. Our findings are different from the above two studies and indicate that ethnicity of minority is a risk factor of underweight and wasting in children, but is not related to stunting. These differences may be attributed to two reasons. Firstly, the economy, cultures, religions, living conditions and life customs are all different among ethnics. Secondly, the sample sizes, definitions of indices, and data analyses are all different among studies, as Zhou et al. concerned the total prevalence of undernutrition, but ignored the types of undernutrition. In our study, the education level of caregivers with minority ethnicity is significantly lower than that of Han caregivers, and the family income and family food expenditure of minority ethnicity are also significantly lower than those of Han. Caregivers with low education level often lack nutritional knowledge, and families under poor socio-economic status have low food consumption capacity, both of which will directly affect the quality of children’s diet, thereby increasing the risk of undernutrition in children.
Education levels and family incomes
Many observational studies confirm that high education level of mothers or caregivers and high family income are two protective factors against undernutrition of childre n[7, 32, 35, 36, 41, 42]. Our study shows that as the education level of caregivers and the family food expenditure increase, the risk of undernutrition in children is lowered, which is consistent with other studies. This is because the increased education level of caregivers can largely improve their acceptance of nutrition and health knowledge, which thereby promotes the scientific feeding and diet balancing of children [5]. Generally, family food expenditure will not increase unless the family incomes rise, and thus is the most direct and objective reflection of family incomes. Since family incomes and family food expenditure are collinear, the variable of family income was not involved in our multivariate logistic regression models. Nevertheless, the protective effect of family food expenditure on undernutrition among children directly reflects the protective effect of family incomes on undernutrition.
Family size
In addition, this study also finds that as the family size increases, the risk of underweight and wasting in children is increased. This finding is consistent with the study conducted in Ethiopi a[13] which shows that the risk of wasting is 1.22 times higher among children who have lived in family members of 6-10 than children who have lived in family members of 1-5. The increase in family size will increase the financial burden of the whole family, and therefore inevitably affect the nutritional status of children.
Limitations
This cross-sectional study has some limitations. First, the relationship between investigated factors and undernutrition is statistical association, rather than causality. Second, some data about the birth weights of children and the maternal gestational weight gain were acquired from the recalling of caregivers, which inevitably resulted in recall bias. To reduce the recall bias, the clinical medical records of child’s vaccination certificate, medical certificate of birth, and maternal health handbook should be taken as the standard, and the subjective recall of the caregivers should be avoided as much as possible. Nonetheless, this large-size epidemiological study involves 5529 children randomly selected from 72 villages across 24 towns in 12 counties of Hunan, and covers the whole preschool age group. Hence, our findings reflect the undernutrition statuses and associated factors of children (age <6 years) in rural Hunan and will help health administrations to lower undernutrition-caused burdens in rural areas.
Conclusions
The prevalence of stunting, underweight and wasting is low among rural children under age of 6 years in Hunan. Undernutrition of children in this region is affected by birth weight, maternal gestational weight gain, ethnicity of caregivers, education level of caregivers, family size, and family food expenditure. Attention must be focused on strengthening the gestational care and reasonable diet of mothers, and on avoiding nutritional deficiency during pregnancy, which will reduce the occurrence of low birth weight. The local economic development and the education level of caregivers need to be further improved, especially for minorities.
Availability of data and materials
The datasets generated during and/or analysed during the current study are not publicly available duo to the personal privacy of subjects but are available from the corresponding author on reasonable request.
Abbreviations
- WHO:
-
World Health Organization
- HAZ:
-
Length/height for Age Z Score
- WAZ:
-
Weight for Age Z Score
- WHZ:
-
Weight for Length/height Z Score
- BMIZ:
-
Body Mass Index for Age Z Score
- AOR:
-
Adjusted Odds Ratio
- CI:
-
Confidence Interval
References
Shi SH, Dai YH. Child Health (third edition). Beijing: People's Medical Publishing House; 2014. (In Chinese)
Kang Y, Aguayo VM, Campbell RK, West KP Jr. Association between stunting and early childhood development among children aged 36-59 months in South Asia. Matern Child Nutr. 2018; Suppl 4:e12684.
Olsen MF, Iuel-Brockdorff AS, Yaméogo CW, Cichon B, Fabiansen C, Filteau S, et al. Early development in children with moderate acute malnutrition: a cross-sectional study in Burkina Faso. Matern Child Nutr. 2019:e12928.
Emerson E, Savage A, Llewellyn G. Prevalence of underweight, wasting and stunting among young children with a significant cognitive delay in 47 low-income and middle-income countries. J Intellect Disabil Res. 2020;64(2):93–102.
Ministry of Health. The nutrition development report of Chinese children aged 0-6 (2012). Beijing: Ministry of Health; 2012. (In Chinese)
World Health Organization. Child malnutrition. https://www.who.int/data/gho/data/themes/theme -details/GHO/child-malnutrition. Accessed 15 December 2019.
Wu L, Yang Z, Yin SA, Zhu M, Gao H. The relationship between socioeconomic development and malnutrition in children younger than 5 years in China during the period 1990 to 2010. Asia Pac J Clin Nutr. 2015;24(4):665–73.
Hunan Provincial Bureau of Statistics, Survey Office of the National Bureau of Statistics in Hunan. Hunan Statistical Yearbook 2019. Beijing: China Statistics Press; 2020. (In Chinese).
Tan C, Luo JY, Wang Z, Mou JS, Zhang LL, Fu CH, et al. Knowledge, attitude, practice and related determinants on nutrition among caregivers of rural standed children under 7 years olds in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2009;30(6):588–91 (In Chinese).
Zhou X, Fang JQ, Luo JY, Wang H, Du QY, Huang GW, et al. Status of, and factors associated with, complementary feeding among infants and young children aged 6-23 months in poor rural areas of Hunan province, China. Zhonghua Yu Fang Yi Xue Za Zhi. 2017; 51(1):58-64. (In Chinese).
Zeng R, Mou JS, Luo JY, Du QY, Wu H, Zhang L, et al. Prevalence and risk factors for malnutrition among 15142 children aged 0-7 in rural areas. Wei Sheng Yan Jiu. 2009;38:624–7 (In Chinese).
Tanaka J, Yoshizawa K, Hirayama K, Karama M, Wanjihia V, Changoma MS, et al. Relationship between dietary patterns and stunting in preschool children: a cohort analysis from Kwale. Kenya. Public Health. 2019;173:58–68.
Tekile AK, Woya AA, Basha GW. Prevalence of malnutrition and associated factors among under-five children in Ethiopia: evidence from the 2016 Ethiopia Demographic and Health Survey. BMC Res Notes. 2019;12(1):391.
Ansuya, Nayak BS, Unnikrishnan B, George A, N SY, Mundkur SC, et al. Risk factors for malnutrition among preschool children in rural Karnataka: a case-control study. BMC Public Health. 2018; 18(1):283.
Khaing HT, Nomura S, Yoneoka D, Ueda P, Shibuya K. Risk factors and regional variations of malnutrition among children under 5 in Myanmar: cross-sectional analyses at national and subnational levels. BMJ Open. 2019;9(9):e030894.
Hintsa S, Gereziher K. Determinants of underweight among 6-59 months old children in Berahle, Afar, North East Ethiopia: a case control study 2016. BMC Res Notes. 2019;12(1):753.
Mou JS, Luo JY, Li YP, Shuai ZR, Liu XH. Study on the nutritional status and determinants among rural stranded children in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2009;30(5):439–43 (In Chinese).
Huo J. Ying Yang Bao: improving complementary feeding for Chinese infants in poor regions. Nestle Nutr Inst Workshop Ser. 2017;87:131–8.
Zhou X, Fang JQ, Luo JY, Wang H, Du QY, Huang GW, et al. Factors associated with malnutrition among infants and young children aged 6-23 months in poor rural areas in Hunan Province, China. Zhonghua Yu Fang Yi Xue Za Zhi. 2017;51(8):751–5 (In Chinese).
Ban L, Guo S, Scherpbier RW, Wang X, Zhou H, Tata LJ. Child feeding and stunting prevalence in left-behind children: a descriptive analysis of data from a central and western Chinese population. Int J Public Health. 2017;62(1):143–51.
Wang J, Wang H, Chang S, Zhao L, Fu P, Yu W, et al. The influence of malnutrition and micronutrient status on anemic risk in children under 3 years old in poor areas in China. PLoS One. 2015;10(10):e0140840.
Zhang Y, Huang X, Yang Y, Liu X, Yang C, Wang A, et al. Double burden of malnutrition among children under 5 in poor areas of China. PLoS One. 2018;13(9):e0204142.
Li LM. Epidemiology (sixth editon). Beijing: People's Medical Publishing House; 2008. (In Chinese)
Li C, Zhu N, Zeng L, Dang S, Zhou J, Pei L, et al. Effect of maternal pre-pregnancy underweight and average gestational weight gain on physical growth and intellectual development of early school-aged children. Sci Rep. 2018;8(1):12014.
World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva: World Health Organization; 2011. https://www.who.int/vmnis/indicators/haemoglobin.pdf. Accessed 29 Mar 2015.
WHO Multicentre Growth Reference Study Group. WHO child growth standards: length/height-for-age, weight-for-age, weight-for length, weight-for-height and body mass index-for-age: methods and development. Geneva: WHO; 2006.
de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85(9):660–7.
World Health Organization. WHO anthro survey analyser and other tools. https://www.who.int/ childgrowth/software/en/. Accessed 6 Jul 2016.
World Health Organization. Growth reference 5-19 years: application tools. https://www.who.int/ growthref/tools/en/. Accessed 6 Jul 2016.
Akombi BJ, Chitekwe S, Sahle BW, Renzaho AMN. Estimating the double burden of malnutrition among 595,975 children in 65 low- and middle-income countries: a meta-analysis of demographic and health surveys. Int J Environ Res Public Health. 2019; 16(16):pii: E2886.
Khan S, Zaheer S, Safdar NF. Determinants of stunting, underweight and wasting among children < 5 years of age: evidence from 2012-2013 Pakistan Demographic and Health Survey. BMC Public Health. 2019;19(1):358.
Kang Y, Aguayo VM, Campbell RK, Dzed L, Joshi V, Waid JL, et al. Nutritional status and risk factors for stunting in preschool children in Bhutan. Matern Child Nutr. 2018;Suppl 4:e12653.
Singh S, Srivastava S, Upadhyay AK. Socio-economic inequality in malnutrition among children in India: an analysis of 640 districts from National Family Health Survey (2015-16). Int J Equity Health. 2019;18(1):203.
Abdeyazdan Z, Ehsanpour S, Hemmati E. Evaluation of growth and development pattern in normal, low and very low birth weight neonatesat 18 months of age. J Educ Health Promot. 2014;3:102.
Nshimyiryo A, Hedt-Gauthier B, Mutaganzwa C, Kirk CM, Beck K, Ndayisaba A, et al. Risk factors for stunting among children under five years: a cross-sectional population-based study in Rwanda using the 2015 Demographic and Health Survey. BMC Public Health. 2019;19(1):175.
Berhe K, Seid O, Gebremariam Y, Berhe A, Etsay N. Risk factors of stunting (chronic undernutrition) of children aged 6 to 24 months in Mekelle City, Tigray Region, North Ethiopia: an unmatched case-control study. PLoS One. 2019;14(6):e0217736.
Li HX, Zheng JF, Huang GW, Xiao J, Wang AH, Feng N, et al. Effects of birth weight on growth and development and anemia among 6-23 months old infants in rural Hunan. Chin J Public Health. 2019;35(6):726–30 (In Chinese).
Zhang W, Niu F, Ren X. Association of maternal pre-pregnancy body mass index and gestational weight gain with Chinese infant growth. J Paediatr Child Health. 2019;55(6):673–9.
Liang JJ, Hu Y, Xing YF, Ma Y, Jiang L, Liu HY, et al. Association between both maternal pre-pregnancy body mass index/gestational weight gain and overweight/obesity children at preschool stag. Zhonghua Liu Xing Bing Xue Za Zhi. 2019;40(8):976–81 (In Chinese).
Josey MJ, McCullough LE, Hoyo C, Williams-DeVane C. Overall gestational weight gain mediates the relationship between maternal and child obesity. BMC Public Health. 2019;19(1):1062.
Jiang Y, Su X, Wang C, Zhang L, Zhang X, Wang L, et al. Prevalence and risk factors for stunting and severe stunting among children under three years old in mid-western rural areas of China. Child Care Health Dev. 2015;41(1):45–51.
Hein AK, Hong SA, Puckpinyo A, Tejativaddhana P. Dietary diversity, social support and stunting among children aged 6-59 months in an internally displaced persons camp in Kayin State. Myanmar. Clin Nutr Res. 2019;8(4):307–17.
Acknowledgements
We would like to thank all the researchers from local county-level maternal and child health care hospital as well as to all caregivers of children who participated in this study from the 12 counties in Hunan Province.
Funding
This study was supported by the Hunan Provincial Health Commission (No.20201924) and Hunan Provincial Natural Science Foundation (No.2020JJ5285).
Author information
Authors and Affiliations
Contributions
HXL, GWH and HW conceived the research idea. HXL participated in the data collection, statistical analysis and preparation of the manuscript. SY and AWH performed the data collection and statistical analysis. SY, HLF and QH performed the data collection. GWH and HW provided the critical review of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Hunan Provincial Maternal and Child Health Care Hospital (No.2019-S036). The study was conducted in accordance with the Declaration of Helsinki. Written informed consents were obtained from all the caregivers of children involved in this study.
Consent for publication
Not applicable
Competing interests
The authors declared that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, H., Yuan, S., Fang, H. et al. Prevalence and associated factors for stunting, underweight and wasting among children under 6 years of age in rural Hunan Province, China: a community-based cross-sectional study. BMC Public Health 22, 483 (2022). https://doi.org/10.1186/s12889-022-12875-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-12875-w