
Abstract
Background
Peer victimization (PV) is one of the major causes of non-suicidal self-injury. Non-suicidal self-injury (NSSI), peer victimization, social anxiety, and mobile phone addiction are significantly related; however, the interaction mechanism and effect of sex differences remain to be determined.
Objective
Herein, we investigated the relationship between peer victimization and NSSI among Chinese high school students. We also explored the chain mediating roles of social anxiety and mobile phone addiction and the regulatory role of sex. The findings of this study provide insights for theoretical interventions based on internal mechanisms.
Method
A self-reported survey of 14,666 high school students from Sichuan County was conducted using a peer victimization scale, NSSI scale, social anxiety scale, and mobile phone addiction scale. A self-administered questionnaire was used to capture sociodemographic information.
Results
Peer victimization, social anxiety, and mobile phone addiction were positively correlated with NSSI. Peer victimization had significant direct predictive effects on NSSI (95% CI: 0.341, 0.385) and significant indirect predictive effects on NSSI through social anxiety (95% CI: 0.008, 0.019) or mobile phone addiction (95% CI: 0.036, 0.053). Peer victimization had significant indirect predictive effects on NSSI through social anxiety as well as mobile phone addiction (95% CI: 0.009, 0.014). The first stage (predicting the effect of peer victimization on NSSI) and the third stage (predicting the effect of mobile phone addiction on NSSI) were both moderated by sex.
Conclusions
Peer victimization could directly predict NSSI and indirectly predict NSSI through social anxiety and mobile phone addiction. Thus, social anxiety and mobile phone addiction exhibited chain mediating effects between peer victimization and NSSI in high school students; moreover, sex might be involved in the regulation of the mediation process.
Similar content being viewed by others


Introduction
Non-suicidal self-injury
Non-suicidal self-injury (NSSI) is the deliberate self-destruction of bodily tissue for purposes that are not socially sanctioned, without suicidal intent [1]. A survey encompassing 11 European countries showed that the prevalence of NSSI was 17.1–38.6% and that the most common form of self-injury was self-cutting [2]. A recent retrospective analysis showed that even in developing countries, the prevalence of NSSI was 11.5–33.8%, showing a continuously increasing trend, which is almost similar to that in developed countries [3]. According to Victor et al. [4], NSSI is more common in adolescence and early adulthood. This may be related to the gradual maturation of the prefrontal cortex area responsible for functions such as emotional regulation during adolescence; thus, adolescents are more susceptible to changes in the environment [5, 6]. NSSI may predict future suicide attempts and increase suicide risk [6,7,8]. It is also associated with mental health problems and substance use disorders in adulthood [9,10,11] and causes harms such as deteriorated physical health and decreased life expectancy [12]. A prospective cohort study suggested that NSSI in early adolescence indicates the emergence of a new psychiatric disorder [13]. Because of the widespread and harmful nature of NSSI and its specific influence on adolescents, NSSI behavior among adolescents has become a key issue to be addressed.
Peer victimization and NSSI
Peer victimization is defined as the experience of aggression, bullying, and social exclusion [14]. It is different from traditional bullying because in bullying, there is more emphasis on the imbalance of power [15]. Some researchers consider bullying to be a subtype of peer victimization [14]. Adolescence is a critical period during which peer victimization develops and forms roots in the mind of an adolescent [16]. The incidence of different forms of peer abuse among European adolescents is between 9.4% and 33.0% [17]. Peer victimization is typically considered a negative peer relationship [18]. Peer victimization is an important risk factor for NSSI, that is, people who experience peer victimization may be more likely to develop NSSI behaviors [19,20,21]. A cross-sectional survey of 2284 rural primary and secondary school students in China showed that students who had experienced peer victimization were more likely to engage in NSSI behaviors [22]. A meta-analysis of the relationship between peer victimization and NSSI showed a significant positive association between peer victimization and NSSI [20]. This may be understood in terms of the interpersonal reinforcement model of self-injury. In this case, the presence of distal risk factors that lead to problems such as interpersonal communication increases the risk of NSSI, and victims may seek help through NSSI behaviors; however, they may also avoid undesired social situations through NSSI behaviors [23]. As an important risk factor for NSSI, the internal mechanisms between peer victimization and self-injury should be urgently explored, and groups prone to these behaviors should be identified.
Mediating role of social anxiety
Social anxiety comprises emotions such as fear, uneasiness, and distress that one experiences in interpersonal situations, it can cause individuals to adopt avoidance behaviors, and they may be hesitant to participate in similar social situations in the future [24]. The level of social anxiety among Chinese adolescents increased significantly each year [25]. Some individuals with social anxiety exhibited highly impulsive and high-risk behaviors such as self-injury, suicide, and substance abuse [26]. Some people with NSSI exhibit specific behaviors for avoiding interpersonal interactions [27, 28]; 8% of borderline and avoidant personalities engage in NSSI behaviors for avoiding social interactions [29]. Peer victimization exhibits a close relationship with social anxiety [30, 31]. According to the social self-efficacy theory [32], peer victimization can significantly reduce adolescents’ social self-efficacy and lead to negative self-evaluations. Moreover, individuals with low social self-efficacy often develop social anxiety because they cannot cope with sudden changes in social situations. A meta-analysis showed a significant positive association between peer victimization and social anxiety, and it led to persistent or aggravated social anxiety [31]. In this study, we propose that adolescent NSSI behavior may be associated with social anxiety, and peer victimization predicts social anxiety levels; therefore, social anxiety may play a mediating role between peer aggression and NSSI.
Chain mediating role of social anxiety and mobile phone addiction
Individuals with social anxiety tend to exhibit negative cognitive patterns [33], and they tend to be negativize pessimistic about the social cues expressed by others. In online interactions such as on mobile phones and web platforms, socially anxious individuals are involved in a non-face-to-face form of social interaction, which, considering the aforementioned social self-efficacy theory, avoids the timely feedback associated with traditional face-to-face interactions. Social anxiety can predict mobile phone addiction levels [34, 35] Although mobile phone addiction has not yet been included in the DSM-V(American Handbook of Mental Disorders, Fifth Edition) and there is no consolidated definition, it is a prevalent health problem, mainly manifested by excessive use; it can disrupt social activities and when mobile phone use is prohibited, it can lead to mood swings [36]. A survey conducted by Lopez-Fernandez et al. [37] showed that the prevalence of mobile phone addiction among UK teenagers is 10%. A cross-sectional survey also demonstrated that peer victimization and mobile phone addiction are related [38]. Another longitudinal study showed that levels of peer victimization predicted levels of mobile phone addiction after six months and one year [39]. In contrast, unmonitored/unchecked mobile phone usage can cause headaches, insomnia, anxiety, depression, self-injury, and so on [40, 41]. A cross-sectional survey of 2,719 adolescents in China showed that those with higher mobile phone addiction scores were more likely to experience severe, repeated NSSI [42]. In summary, peer victimization may lead to social anxiety, smart phone addiction, and NSSI, and social anxiety positively predicts the levels of smart phone addiction and NSSI. In addition, smart phone addictive behaviors exhibit a latent association with NSSI. Therefore, in the present study, we hypothesize that smart phone addiction and social anxiety may play a chain mediating role in peer aggression and NSSI.
The moderating role of sex in this mediation model
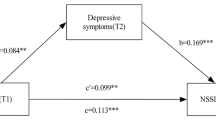
Sex differences affect the prevalence of NSSI; however, the findings of previous studies in this regard have been inconsistent. Female students are also considered to be at risk of NSSI [2, 43, 44]. Conversely, a meta-analysis of self-injurious behavior in children and adolescents between 1989 and 2018 indicated that sex was not a significant moderator for explaining heterogeneity when suicidal and self-harming behaviors are prevalent [45]. This shows inconsistencies in the findings of studies on the incidence of self-harm between male and female students, which may be related to the differences in regions and samples, with some studies reporting that sex differences are more common in clinical samples than in community samples [46] and that sex differences are more common at younger ages [47]. Several studies have also investigated the relationship between peer victimization and NSSI as a function of sex. A cross-sectional survey of 578 adolescents in China showed that sex moderated the relationship between negative peer relationships and NSSI [48]. According to social role theory, this may be related to the fact that female students attach more importance to interpersonal relationships [49]. However, a 2022 meta-analysis could not verify the sex relationship between victimization and self-injury because fewer articles were included to increase the amount of sex difference between victimization and self-injury [50]. This study proposes an alternative hypothesis that sex plays a moderating role between peer victimization and NSSI. A survey on smart phone addiction found that boys tend to use gaming functions, whereas female students tend to use social functions, with female students having higher levels of addiction than male students(Yang et al., 2010). We speculate that sex may play a moderating role in cell phone addiction and NSSI. A study on adolescent social anxiety found that male students showed higher levels of social avoidance [51]; however, according to the above NSSI-mentioned interpersonal model, whether sex plays a moderating role remains to be clarified. Therefore, this study examined the moderating effect of sex between peer aggression and smart phone addiction. The integrated conceptual model of this study is presented in Fig. 1.

Model diagram for the chain mediating role of social anxiety and mobile phone addiction between peer victimization and NSSI and the moderating role of sex in peer victimization, social anxiety, and mobile phone addiction
Materials and methods
Procedures and participants
All high schools in Zizhong County, a rural area, in central Sichuan were selected for this study, and all students enrolled in the school from April 13, 2022, to April 15, 2023 were surveyed. A total of 14,666 high school students were invited to participate in our anonymous survey, which was administered in classrooms. Informed consent was obtained from school administrators, students, and their parents prior to data collection. Classroom teachers or classroom leaders were first trained by trained leaders in the five high schools in Zizhong County to distribute the survey questionnaires. Students were informed that the collected data would be confidential and that they had the right to withdraw at any time. To ensure completeness and accuracy of data, students were given 1 h to answer the questionnaire questions centrally, all questionnaires were conducted in the Chinese language. To prevent any potential influence from teachers, alternative staff members were tasked with distributing and collecting the questionnaires. During the next 1 month, all participants were educated about emotion management and provided a free psychological hotline service. This study was approved by the Ethics Committee of Mianyang Third People’s Hospital-Sichuan Provincial Mental Health Center (Approval Document No: 2022 Annual Review;Ethics approval number:12510600451210007X.).
Measures
Demographic characteristics
We used a self-administered questionnaire to collect sociodemographic information from the students, including sex, age, grade, class, and parents’ marital status (married, divorced, other), whether they were left behind (unable to live with both parents or either of them for more than six months due to work and other reasons).
Adolescent NSSI questionnaire
The NSSI scale [52] for adolescents was used to measure the self-injurious behaviors of secondary school students. Homogeneity reliability in a sample of Chinese adolescents was reported to be 0.85 [52]. It comprised two parallel paired parts: the number of self-injurious behaviors was assessed into four levels: 0, 1, 2–4, and ≥ 5, and the degree of physical injury was assessed into five levels: none, mild, moderate, severe, and very severe. This included 18 types of self-inflicted wounds such as intentionally scratching one’s skin with glass and knives and intentionally poking open wounds to prevent healing. The total score of the questionnaire was taken as the sum of the product of the number score and the grade score; as long as one of the scores was not zero, it was considered self-injurious behavior. A higher score indicated more serious self-injurious behavior. The value of Cronbach’s alpha and construct validity of the scale were 0.899 and 0.742, respectively [52].
Peer victimization questionnaire
The multidimensional peer victimization scale developed by Mynard and Joseph [53] and revised by Zhang [54] was used for measuring peer victimization levels. The internal consistency reliability of the physical aggression subscale in the Chinese adolescent sample reported in a previous study was 0.71, with the internal consistency reliability of the relationship aggression subscale being 0.85 [54]. It comprises two subscales of physical victimization and relational victimization, with 11 entries, and a 4-point Likert scale, with 0 indicating never and 3 indicating frequently. This included items such as other students threatening to beat me up in the last six months, other students deliberately ignoring me, etc. Higher scores indicated more severe peer victimization. The value of Cronbach’s alpha for this scale was 0.873, and the construct validity of the scale was 0.909.
Social anxiety questionnaire
The interaction anxiousness scale (IAS) questionnaire [55] uses a clinical empirical approach and specifically measures subjective feelings of anxiety about interpersonal interactions. Homogeneity reliability in a sample of Chinese adolescents was reported to be 0.87 [56]. It contains questions about everyday social situations that may provoke feelings of anxiety. For example, I feel nervous even in informal situations; I feel nervous when I must talk to teachers, etc. The IAS is a measure of the tendency to experience subjective social anxiety independently of behavior. The value of Cronbach’s alpha for this scale was 0.787, and the construct validity of the scale was 0.919.
Mobile phone addiction questionnaire
The mobile phone addiction index (MPAI) [55], developed at the Chinese University of Hong Kong, was used to diagnose mobile phone addiction in adolescents and college students. Homogeneity reliability reported previously in a sample of Chinese adolescents was 0.86 [57]. It included 17 questions, for example, you have been told you spend too much time on your phone; your friends and family have complained about your use of your phone, etc. The total score was in the range of 17–85, with higher scores indicating a higher tendency of mobile phone addiction. A higher score indicated a higher tendency for mobile phone addiction. For scoring, a 5-point Likert scale was used, where 1 meant never and 5 meant always. The value of Cronbach’s alpha for this scale was 0.892, and the construct validity of the scale was 0.896.
Statistical analyses
All data in this study were analyzed using SPSS 26.0; continuous variables are expressed as mean ± standard deviation, whereas categorical variables are expressed as frequencies. To analyze the relationship between variables, Pearson correlation was used for data variables that conformed to a normal distribution, and Spearman correlation was used for variables that did not conform to a normal distribution. First, Model 6 in PROCESS macro was used to test the chain mediating effect. Bootstrap 95% confidence intervals (CIs) were used to examine whether the estimates of the chain mediating effect of the regression coefficients on 5000 samples were significant. The indirect effect was considered statistically significant if the 95% CI did not contain 0. Next, the moderating role of sex in the chain mediating effect was tested using Model 89, and bootstrap analysis was conducted using a heavy sample of 5000 95% CIs to analyze the significance of the mediating model with moderation. The Harman single-factor test was used for determining the common method bias [58]. Overall, there were 24 factors > 1 without rotation, and the first factor had an explanatory rate of 15.476%, which was less than the critical criterion of 40%, indicating that there was no significant common method bias in this study.
Result
Baseline information
Out of 14,666 questionnaires that were distributed, professionals proofread and selected 14,036 valid questionnaires after excluding non-response questionnaires (recovery rate: 95.7%). These valid questionnaires were collected from 6326 (45.1%) male students and 7710 (54.9%) female students, with participants’ age ranging from 15 to 18 (M = 16.40) years.
Detection rates and sex differences
The detection rate of NSSI behaviors was 25.5%, with females having a higher detection rate (14.8%) than males (10.7%), and the difference was statistically significant (P < 0.001). Of these, 4.02% committed self-injury in only one way, 15.90% scored in the range 2–10, and 5.54% scored ≥ 10. The detection rate of peer victimization in this study was 65.1%, and the detection rate of physical victimization was 38.3%, with that for males being 21.8% and that for females being 16.6%, and the difference was statistically significant (p < 0.001). The detection rate of relationship victimization in this study was 56.6%, with that in males being 25.6% and that in females being 31.0%, indicating a non-significant sex difference (p = 0.63).
Relevance analysis
Correlation analysis was performed on the variables of peer victimization, adolescent NSSI, social anxiety, and mobile phone addiction, and the results are presented in Table 1. A significant positive correlation was observed between peer victimization, NSSI, social anxiety, and mobile phone addiction (P < 0.001). Additionally, a significant positive correlation between sex (0 = male, 1 = female) and NSSI (P < 0.001).
Chain mediated outcome test
Based on the results of the correlation analysis, after controlling for variables including grade level, whether the adolescent was left behind, and parental marital status, we considered peer victimization as a predictor variable, adolescent NSSI as an outcome variable, and social anxiety and mobile phone addiction as mediating variables. A chain mediated effects test was conducted using Model 6 in the SPSS PROCESS macro program. The results of the regression analysis are presented in Table 2. Peer victimization positively predicted adolescent NSSI (β = 0.363, t = 32.213, 95%, CI = [0.341, 0.385]), social anxiety (β = 0.328, t = 20.912, 95%, CI = [0.297, 0.359]), and mobile phone addiction (β = 0.723, t = 35.737, 95%, CI = [0.683, 0.763]). Social anxiety positively predicted mobile phone addiction (β = 0.551, t = 51.3523, 95%, CI = [0.530, 0.572]) and NSSI (β = 0.395, t = 6.338, 95%, CI = [0.0273, 0.052]). Mobile phone addiction positively predicted NSSI behavior (β = 0.062, t = 13.702, 95%, CI = [0.053, 0.071]). Mediated effects analysis revealed (Table 3) that social anxiety and mobile phone addiction significantly mediated the relation between peer victimization and NSSI, and social anxiety and mobile phone addiction serve as the chain mediators between peer victimization and NSSI. The total indirect effect value was 0.069, accounting for 19.01% of the total effect of peer victimization on NSSI.
Results of the moderated chained mediated effects test
After controlling for grade, whether left behind, and parental marital status, the measures were data-centered and tested for moderating effects using Model 89 in the SPSS PROCESS macro program. Sampling was repeated 5000 times to test the moderating role of sex in the chain mediated model (Fig. 1), and the results are presented in Table 4. After sex was given as input to the model, the product term of peer victimization and sex significantly affected NSSI (β = 0.114, t = 5.039, 95% CI = [0.070, 0.168]), and the product of mobile phone addiction and sex (β = 0.025, t = 2,710, 95% CI = [0.007, 0.042]) were significant predictors of NSSI. However, the product term of social anxiety and sex was not a significant predictor of NSSI (β = 0.004, t = 0.342, 95% CI = [− 0.203, 0.029]). Thus, sex can play a moderating role in the direct effect of peer victimization on adolescents’ NSSI behavior and can also moderate the predictive effect of smart smartphone addiction on NSSI behavior.
Further simple slope analysis showed that the level of peer victimization in female positively predicted NSSI behavior (β = 0.418, t = 27.629, 95% CI = [0. 389, 0.448]), and the positive prediction effect was weaker in male (β = 0.305, t = 18.162, 95% CI = [0. 271, 0.337]). A simple slope analysis is shown in Fig. 2. Similarly, smart smartphone addiction levels among female students positively predicted their NSSI behavior (β = 0.072, t = 12.280, 95% CI = [0. 061, 0.084]), and smart smartphone addiction level among males also positively predicted NSSI behavior but with a smaller predictive effect (β = 0.048, t = 6.933, 95% CI = [0. 034, 0.061]). A simple slope analysis is shown in Fig. 3. Finally, we examined the Index of moderated mediation, and the results showed that in the model of chained mediated effects of social anxiety and smart phone addiction, the mediator index of moderation was 0.0044, (CI = [0.001, 0.009]).

Model of the test for simple slopes showing the moderating role of sex in the association between peer victimization and NSSI

Model of the test for simple slopes showing the moderating role of sex in the association
Thus, the chain mediation model constructed in this paper was verified, indicating the moderating role of sex in peer victimization and smart smartphone addiction for predicting NSSI; moreover, social anxiety does not play a role in predicting NSSI.
Discussion
In this study, we developed a moderated chain mediation model to explore the relationship between peer victimization and NSSI and the internal mechanisms of peer victimization and NSSI, as well as to identify priority populations. In addition, we report the detection rates and sex differences in peer victimization and NSSI, which helped us better understand the levels of peer victimization and NSSI in western China.
Detection rates and sex differences in peer victimization and NSSI
In this study, we noticed that the detection rate of NSSI behaviors was 25.5%, which is similar to the results of a cross-sectional study in China (23.2%) [59] and another Chinese meta-analysis pooling the prevalence of 26 surveys, which showed an increase in NSSI prevalence from 2008 to 2016 with a pooled prevalence of (22.37%) [60]. In terms of sex, we found that females were more likely to engage in NSSI than males (P < 0.001), which is consistent with the results of a previous META and multiple cross-sectional survey analysis [43, 44, 61, 62]. In contrast, a previous study showed no significant difference in the prevalence of self-injury in the general population (N = 1442) sample [63]. Our finding supports the notion that the rate of detection of NSSI is higher in female students than in male students, which may be explained by the fact that the subjects of these students were adolescents studying in high schools. Previous studies have shown that the sex difference in NSSI is not a static process but may expand in adolescence and disappears in early adulthood [64]. The detection rate of peer victimization in this study was 65.1%, and the prevalence of different forms of peer aggression among European adolescents was reported to be 9.4– 33.0% [17]. A meta-analysis in China showed that the prevalence of peer victimization in mainland China was 2–66% [65]. and the detection rate of peer victimization in this study was at a higher level, While the high level of detection of peer victimization in this study is consistent with our conjecture that our sample originated from counties in western China, a less economically developed rural area with more left-behind children, which is consistent with previous findings, however, this inference needs more data to be verified. The detection rate of physical victimization was 38.3%, among these, the proportion of males was significantly larger than females, which is consistent with the findings of most previous studies, where the level of physical victimization was reported to be higher in males than in females [53, 66, 67]. The detection rate of relationship victimization in males and females showed non-significant sex difference, this may be because males focus more on physical aggression and may underestimate the level of relational victimization when they are subjected to physical versus relational aggression [67]; as a result, even if they are subjected to the same level of relational aggression, it is more likely that they will ignore it, compared to physical aggression.
Social anxiety and the chain mediating role of cell phone addiction
Bourgeoning literature implied a positive correlation between social anxiety and high-risk behaviors [26]; [30, 31]. In the present study, among several indicators such as grade, marital status of parents, stay behind or not, sex, peer victimization, social anxiety, mobile phone addiction and NSSI, most significant positive correlation between peer victimization and NSSI was found, indicating that a high level of peer victimization increases the probability and frequency of self-injury, which is consistent with the findings of previous studies [20, 21]. As expected, peer victimization was positively correlated with NSSI. Here, our findings suggest that social anxiety plays a mediating role between peer victimization and NSSI. Nock indicated that individuals whose NSSI is influenced by interpersonal environments may engage in NSSI behaviors to avoid socialization [23]; in other words, these individuals may avoid socialization and engage in NSSI behaviors.
According to recent studies, there is a positive correlation between mobile phone addiction and NSSI among adolescents. Also, it was found that smartphone addiction could positively predict NSSI, particularly in pre-adolescence as compared to adolescents, which was related to low self-control and emotion dysregulation(Wang et al., 2022; Xu et al., 2023). Here, our data showed that mobile phone addiction mediates the relationship between peer victimization and NSSI behavior. First, we found that the level of peer aggression was significantly and positively associated with cell phone addiction. A longitudinal study showed that the level of peer victimization can predict the level of mobile phone addiction [39]. According to the Internet compensation theory, upon experiencing psychosocial problems, individuals may turn to the Internet or cell phones to escape the predicament they are in, which may be one of the reasons for the high level of cell phone addiction in peer-victimized individuals [68]. The results of this study showed that the higher the level of cell phone addiction, the higher the levels of NSSI. This is consistent with the findings of some studies, pointing out that cell phone addiction can lead to a range of problems such as anxiety, depression, and self-injury [69, 70]. The risk of self-injury induced by smart phone addiction may be related to the sleep problems caused by it. Sleep problems seriously affect adolescents’ mental health, and previous studies have indicated a significant positive correlation between sleep problems and NSSI [71], while smart phone use has been shown to significantly reduce sleep quality and decrease sleep length, among other issues. Our study also reports the establishment of a chain mediating effect in the same social anxiety and cell phone addiction in peer victimization and NSSI, suggesting that there is an association between these variables. Among these, mobile phone addiction showed the highest R2 of 0.263. The results of previous studies between social anxiety and cell phone addiction have been inconsistent, with some studies showing a strong positive correlation, whereas others reporting weak to no correlation between the two. This discrepancy in the findings may be related to differences in the study population; this study was conducted among high school students in Western China, and research suggests that Easterners exhibit a stronger sense of community and tend to experience more social anxiety, with Eastern culture involving communication through non-verbal language. Possibly, social anxiety and cell phone addiction are more closely linked in the aforementioned cultural context.
The moderating role of sex in this mediation model
We finally investigated the moderating relationship of sex with the aforementioned issues and self-injury, indicating that sex moderated the relationship between peer victimization and NSSI, with female students’ peer victimization having a greater direct effect on their NSSI behavior. This phenomenon can be explained by the sociological theory, according to which female students tend to be more easily influenced by interpersonal relationships than male counterparts [49]. In other words, female students are more likely to experience adverse emotions when exposed to the same level of victimization. A previous study showed that female students exhibit lower emotional regulation than male students when experiencing negative peer relationships [72]. Another study found regional gray matter volume in the right dorsolateral prefrontal cortex in male students and in the left brainstem extending into anatomical clusters in the left hippocampus, left amygdala, and insular cortex in female students, which implies that male students may be more likely to withdraw from negative emotions [73]. The emotion regulation model of self-injury also states that negative emotions and the ability to regulate them play a crucial role in self-injury. In addition, the results suggest that the direct effect of mobile phone addiction levels on NSSI behavior is greater in female students than in male students. This may also be related to female’s poor ability to regulate negative emotions, as studies have found that cell phone addiction increases the risk of self-harm possibly because of the negative emotions it brings(Yang et al., 2010). This may be explained as differences in how mobile phone addiction manifests in male and female students, resulting in different addiction patterns. Males consider their mobile phones to be tools, whereas females use them mostly for social functions. Studies have also concluded that females are more dependent on smart mobile phones than males, which may explain the potential moderating role of sex in the aforementioned chain-mediated model [74, 75]. Female’s mobile phone addiction levels are more responsive to social problems than those of males. Another study also showed that the negative consequences of mobile phone addiction were more pronounced among females [76].
Limitations and practical implications
This study has several limitations. First, the cross-sectional survey we used does not allow us to establish causal inferences about the observed associations, warranting longitudinal studies to validate our theoretical model in the future. Second, this study used a self-report approach that may have concealed self-injurious behavior, and in the future, multiple assessment methods, such as conversation method, observation method, and family report questionnaire, can be designed to make the theoretical model more reliable. Finally, relationship victimization and physical victimization in peer victimization were not viewed separately, and the theoretical model of this study counted the total victimization score, which can be refined in future experimental designs so that the intervention can be justified according to different types of victimization.
The present study has important practical implications. Although we did not involve the clinical population, the study findings provide insights for practice. First, the detection rate of peer victimization in western China is high; therefore, reducing a series of psychological problems brought about by peer victimization in the region is essential. This study is the first to include social anxiety and cell phone addiction in the model of peer victimization and NSSI, which provides new intervention methods to reduce the self-injury problems caused by peer victimization, such as group counseling and individual counseling to reduce social anxiety, or cell phone use management to reduce the length of cell phone use. We also established the relationship between social anxiety and cell phone addiction due to cultural differences and differences in communication styles [77, 78]. Furthermore, we analyzed the role of sex difference in peer victimization and NSSI and examined its moderating effect, which helped us better understand the relationship between these variables. Teachers and parents should focus more on adolescent female students who are peer victimized. More importantly, cognitive behavioral therapy should be provided to adolescents with peer problems with NSSI, which may reduce their levels of social anxiety, eventually alleviating their internalized psychological problems.
Conclusion
In this cross-sectional study of 14,036 Chinese high school students, the detection rate of self-injury was on par with those reported in previous studies, and the detection rate of peer victimization was found to be higher. Peer victimization directly predicted NSSI and was indirectly predicted through social anxiety and mobile phone addiction. Further, according to simple slope analysis, peer victimization and mobile phone addiction levels among female students showed a less significant predictors of NSSI than among males.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Nock MK. Self-injury. Annu Rev Clin Psychol. 2010;6:339–63.
Brunner R, Kaess M, Parzer P, Fischer G, Carli V, Hoven CW, et al. Life-time prevalence and psychosocial correlates of adolescent direct self-injurious behavior: a comparative study of findings in 11 European countries. J Child Psychol Psychiatry. 2014;55:337–48.
Mannekote Thippaiah S, Shankarapura Nanjappa M, Gude JG, Voyiaziakis E, Patwa S, Birur B, et al. Non-suicidal self-injury in developing countries: a review. Int J Soc Psychiatry. 2021;67:472–82.
Victor SE, Muehlenkamp JJ, Hayes NA, Lengel GJ, Styer DM, Washburn JJ. Characterizing gender differences in nonsuicidal self-injury: evidence from a large clinical sample of adolescents and adults. Compr Psychiatry. 2018;82:53–60.
Caballero A, Granberg R, Tseng KY. Mechanisms contributing to prefrontal cortex maturation during adolescence. Neurosci Biobehav Rev. 2016;70:4–12.
Hawton K, Bale L, Brand F, Townsend E, Ness J, Waters K, et al. Mortality in children and adolescents following presentation to hospital after non-fatal self-harm in the Multicentre Study of Self-harm: a prospective observational cohort study. Lancet Child Adolesc Health. 2020;4:111–20.
Ribeiro JD, Franklin JC, Fox KR, Bentley KH, Kleiman EM, Chang BP, et al. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: a meta-analysis of longitudinal studies. Psychol Med. 2016;46:225–36.
Ohlis A, Bjureberg J, Lichtenstein P, D’Onofrio BM, Fruzzetti AE, Cederlöf M, et al. Comparison of suicide risk and other outcomes among boys and girls who self-harm. Eur Child Adolesc Psychiatry. 2020;29:1741–6.
Mars B, Heron J, Crane C, Hawton K, Lewis G, Macleod J, et al. Clinical and social outcomes of adolescent self harm: population based birth cohort study. BMJ. 2014;349:g5954.
Borschmann R, Becker D, Coffey C, Spry E, Moreno-Betancur M, Moran P, et al. 20-year outcomes in adolescents who self-harm: a population-based cohort study. Lancet Child Adolesc Health. 2017;1:195–202.
Steeg S. Self-harm in adolescence: a marker for psychosocial problems in early adulthood. Lancet Child Adolesc Health. 2017;1:163–4.
Bergen H, Hawton K, Waters K, Ness J, Cooper J, Steeg S, et al. Premature death after self-harm: a multicentre cohort study. Lancet. 2012;380:1568–74.
Wilkinson PO, Qiu T, Neufeld S, Jones PB, Goodyer IM. Sporadic and recurrent non-suicidal self-injury before age 14 and incident onset of psychiatric disorders by 17 years: prospective cohort study. Br J Psychiatry. 2018;212:222–6.
Hunter SC, Boyle JM, Warden D. Perceptions and correlates of peer-victimization and bullying. Br J Educ Psychol. 2007;77:797–810.
Cuadrado-Gordillo I. Repetition, power imbalance, and intentionality: do these criteria conform to teenagers’ perception of bullying? A role-based analysis. J Interpers Violence. 2012;27:1889–910.
Arseneault L. Annual Research Review: the persistent and pervasive impact of being bullied in childhood and adolescence: implications for policy and practice. J Child Psychol Psychiatry. 2018;59:405–21.
Burke T, Sticca F, Perren S. Everything’s gonna be alright! The longitudinal interplay among social support, peer victimization, and depressive symptoms. J Youth Adolesc. 2017;46:1999–2014.
Yurkowski K, Martin J, Levesque C, Bureau JF, Lafontaine MF, Cloutier P. Emotion dysregulation mediates the influence of relationship difficulties on non-suicidal self-injury behavior in young adults. Psychiatry Res. 2015;228:871–8.
van Geel M, Vedder P, Tanilon J. Relationship between peer victimization, cyberbullying, and suicide in children and adolescents: a meta-analysis. JAMA Pediatr. 2014;168:435–42.
van Geel M, Goemans A, Vedder P. A meta-analysis on the relation between peer victimization and adolescent non-suicidal self-injury. Psychiatry Res. 2015;230:364–8.
Esposito C, Bacchini D, Affuso G. Adolescent non-suicidal self-injury and its relationships with school bullying and peer rejection. Psychiatry Res. 2019;274:1–6.
Li X, Chen F, Lin Y, Jia Z, Tucker W, He J, et al. Research on the relationships between psychological problems and school bullying and non-suicidal self-injury among rural primary and middle school students in developing areas of China. Int J Environ Res Public Health. 2020;17:3371.
Nock MK. Why do people Hurt themselves? New insights into the Nature and functions of Self-Injury. Curr Dir Psychol Sci. 2009;18:78–83.
Heimberg RG, Hofmann SG, Liebowitz MR, Schneier FR, Smits JAJ, Stein MB, et al. Social anxiety disorder in DSM-5. Depress Anxiety. 2014;31:472–9.
Xin S, Peng H, Sheng L. Changes of social anxiety in Chinese adolescents during 2002∼ 2020: an increasing trend and its relationship with social change. Child Youth Serv Rev. 2022;142:106614.
Binelli C, Muñiz A, Sanches S, Ortiz A, Navines R, Egmond E, et al. New evidence of heterogeneity in social anxiety disorder: defining two qualitatively different personality profiles taking into account clinical, environmental and genetic factors. Eur Psychiatry. 2015;30:160–5.
Nock MK, Prinstein MJ, Sterba SK. Revealing the form and function of self-injurious thoughts and behaviors: a real-time ecological assessment study among adolescents and young adults. J Abnorm Psychol. 2009;118:816–27.
Turner BJ, Cobb RJ, Gratz KL, Chapman AL. The role of interpersonal conflict and perceived social support in nonsuicidal self-injury in daily life. J Abnorm Psychol. 2016;125:588–98.
Glassman LH, Weierich MR, Hooley JM, Deliberto TL, Nock MK. Child maltreatment, non-suicidal self-injury, and the mediating role of self-criticism. Behav Res Ther. 2007;45:2483–90.
Wu L, Zhang D, Cheng G, Hu T. Bullying and social anxiety in Chinese children: moderating roles of Trait Resilience and Psychological Suzhi. Child Abuse Negl. 2018;76:204–15.
Pontillo M, Tata MC, Averna R, Demaria F, Gargiullo P, Guerrera S et al. Peer victimization and onset of social anxiety disorder in children and adolescents. Brain Sci. 2019;9.
Betz NE. Self-efficacy theory as a basis for career assessment. J Career Assessment. 2000;8:205–22.
Blöte AW, Miers AC, Van den Bos E, Westenberg PM. Negative social self-cognitions: how shyness may lead to social anxiety. J Appl Dev Psychol. 2019;63:9–15.
Pera A. The psychology of addictive smartphone behavior in young adults: problematic use, social anxiety, and depressive stress. Front Psychiatry. 2020;11:573473.
Li X, Li W, Liu M, Xiao W, Zhou H. How does shyness affect Chinese College Students’ tendency to Mobile phone addiction? Testing the mediating roles of social anxiety and self-control. Front Public Health. 2022;10:902425.
Panova T, Carbonell X. Is smartphone addiction really an addiction? J Behav Addict. 2018;7:252–9.
Lopez-Fernandez O, Honrubia-Serrano L, Freixa-Blanxart M, Gibson W. Prevalence of problematic mobile phone use in British adolescents. Cyberpsychol Behav Soc Netw. 2014;17:91–8.
Jia J, Li D, Li X, Zhou Y, Wang Y, Sun W, et al. Peer victimization and adolescent internet addiction: the mediating role of psychological security and the moderating role of teacher-student relationships. Comput Hum Behav. 2018;85:116–24.
Chen Y, Zhu J, Zhang W. Reciprocal longitudinal relations between peer victimization and mobile phone addiction: the explanatory mechanism of adolescent depression. J Adolesc. 2021;89:1–9.
Yang YS, Yen JY, Ko CH, Cheng CP, Yen CF. The association between problematic cellular phone use and risky behaviors and low self-esteem among Taiwanese adolescents. BMC Public Health. 2010;10:217.
Augner C, Hacker GW. Associations between problematic mobile phone use and psychological parameters in young adults. Int J Public Health. 2012;57:437–41.
Wang R, Yang R, Ran H, Xu X, Yang G, Wang T, et al. Mobile phone addiction and non-suicidal self-injury among adolescents in China. Peer J. 2022;10:e14057.
Ang RP, Ooi YP. Impact of gender and parents’ marital status on adolescents’ suicidal ideation. Int J Soc Psychiatry. 2004;50:351–60.
Brown RC, Plener PL. Non-suicidal Self-Injury in Adolescence. Curr Psychiatry Rep. 2017;19:20.
Lim KS, Wong CH, McIntyre RS, Wang J, Zhang Z, Tran BX et al. Global lifetime and 12-Month prevalence of suicidal behavior, Deliberate Self-Harm and Non-suicidal Self-Injury in Children and adolescents between 1989 and 2018: a Meta-analysis. Int J Environ Res Public Health. 2019;16.
Heath N, Toste J, Nedecheva T, Charlebois A. An examination of nonsuicidal self-injury among college students. J Ment Health Couns. 2008;30:137–56.
Sornberger MJ, Heath NL, Toste JR, McLouth R. Nonsuicidal self-injury and gender: patterns of prevalence, methods, and locations among adolescents. Suicide Life Threat Behav. 2012;42:266–78.
Xu JB, Jiang N, Qin Q, Jiang Q. The relationship between negative peer relationship and non-suicidal self-injury in Chinese adolescents: a moderated-mediation model. Front Psychol. 2022;13:913872.
Eagly AH, Wood W. Social role theory. Handbook of theories of social psychology. London: SAGE Publications Ltd.; 2012. pp. 458–76.
Huang H, Ding Y, Wan X, Liang Y, Zhang Y, Lu G, et al. A meta-analysis of the relationship between bullying and non-suicidal self-injury among children and adolescents. Sci Rep. 2022;12:17285.
La Greca AM, Ingles CJ, Lai BS, Marzo JC. Social anxiety scale for adolescents: factorial invariance across gender and age in Hispanic American adolescents. Assessment. 2015;22:224–32.
Feng Y. The relationship between adolescent self-harming behavior and individual emotional and family environmental factors. Central China Normal University; 2008.
Mynard H, Joseph S. Development of the multidimensional peer-victimization scale. Aggressive Behav. 2000;26:169–78.
Zhang W, Chen L, Ji L, Zhang L, Chen G, Wang S. Physical aggression, relational aggression, and children’s emotional adjustment in mid-childhood. Psychol News. 2009;41:433–43.
Leung L. Impacts of net-generation attributes, seductive properties of the internet, and gratifications-obtained on internet use. Telemat Inf. 2003;20:107–29.
Liu Y, Yu Y, Zhang P, Meng X. Relationship between social anxiety and aggressive behavior in children and adolescents. School Health in China. 2011;32:909–11.
Shi M, Zhai X, Li S, Shi Y, Fan X. The relationship between physical activity, mobile phone addiction, and irrational procrastination in Chinese college students. Int J Environ Res Public Health. 2021;18:5325.
Malhotra NK, Kim SS, Patil A. Common method variance in IS research: a comparison of alternative approaches and a reanalysis of past research. Manage Sci. 2006;52:1865–83.
Liang S, Yan J, Zhang T, Zhu C, Situ M, Du N, et al. Differences between non-suicidal self injury and suicide attempt in Chinese adolescents. Asian J Psychiatr. 2014;8:76–83.
Taylor PJ, Jomar K, Dhingra K, Forrester R, Shahmalak U, Dickson JM. A meta-analysis of the prevalence of different functions of non-suicidal self-injury. J Affect Disorders. 2018;227:759–69.
Laye-Gindhu A, Schonert-Reichl KA. Nonsuicidal self-harm among community adolescents: understanding the whats and whys of self-harm. J Youth Adolesc. 2005;34:447–57.
Bresin K, Schoenleber M. Gender differences in the prevalence of nonsuicidal self-injury: a meta-analysis. Clin Psychol Rev. 2015;38:55–64.
Briere J, Gil E. Self-mutilation in clinical and general population samples: prevalence, correlates, and functions. Am J Orthopsychiat. 1998;68:609–20.
Wilkinson PO, Qiu T, Jesmont C, Neufeld SAS, Kaur SP, Jones PB, et al. Age and gender effects on non-suicidal self-injury, and their interplay with psychological distress. J Affect Disorders. 2022;306:240–5.
Chan HCO, Wong DSW. Traditional school bullying and cyberbullying in Chinese societies: prevalence and a review of the whole-school intervention approach. Aggress Violent Beh. 2015;23:98–108.
Crick NR, Bigbee MA. Relational and overt forms of peer victimization: a multiinformant approach. J Consult Clin Psych. 1998;66:337–47.
Phelps CE. Children’s responses to overt and relational aggression. J Clin Child Psychol. 2001;30:240–52.
Kardefelt-Winther D. A conceptual and methodological critique of internet addiction research: towards a model of compensatory internet use. Comput Hum Behav. 2014;31:351–4.
Oshima N, Nishida A, Shimodera S, Tochigi M, Ando S, Yamasaki S, et al. The suicidal feelings, self-injury, and mobile phone use after lights out in adolescents. J Pediatr Psychol. 2012;37:1023–30.
Xu H, Xiao W, Xie Y, Xu S, Wan Y, Tao F. Association of parent-child relationship quality and problematic mobile phone use with non-suicidal self-injury among adolescents. BMC Psychiatry. 2023;23:1–11.
Goldstein TR, Bridge JA, Brent DA. Sleep disturbance preceding completed suicide in adolescents. J Clin Child Psychol. 2008;76:84–91.
Adrian M, Zeman J, Erdley C, Lisa L, Sim L. Emotional dysregulation and interpersonal difficulties as risk factors for nonsuicidal self-injury in adolescent girls. J Abnorm Child Psychol. 2011;39:389–400.
Kong F, Zhen Z, Li J, Huang L, Wang X, Song Y, et al. Sex-related neuroanatomical basis of emotion regulation ability. PLoS ONE. 2014;9:e97071.
Chiu SI, Hong FY, Chiu SL. An analysis on the correlation and gender difference between College Students’ internet addiction and Mobile Phone Addiction in Taiwan. ISRN Addict. 2013;2013:360607.
Roberts JA, Yaya LH, Manolis C. The invisible addiction: cell-phone activities and addiction among male and female college students. J Behav Addict. 2014;3:254–65.
Beranuy M, Oberst U, Carbonell X, Chamarro A. Problematic internet and mobile phone use and clinical symptoms in college students: the role of emotional intelligence. Comput Hum Behav. 2009;25:1182–7.
Kayan S, Fussell SR, Setlock LD. Cultural differences in the use of instant messaging in Asia and North America. in Proceedings of the 2006 20th anniversary conference on Computer supported cooperative work. 2006.
Woody SR, Miao S, Kellman-McFarlane K. Cultural differences in social anxiety: a meta-analysis of Asian and European heritage samples. Asian Am J Psychol. 2015;6:47–55.
Acknowledgements
The authors thank all the students and schools who participated in this study.
Funding
This study was supported by The Primary Health Development Research Center of the Sichuan Province Program (SWFZ22-C-89) and Mianyang Social Science Foundation (MY2023YB127).
Author information
Authors and Affiliations
Contributions
Qianmei Long participated in the formulation of research concepts, research design, data analysis and statistics, and drafting manuscripts. Bin Huang, Junlin Wu, Jia Yu, Junlin Qiu, Yanqing Huang, and Yiyu Tang participated in the data collection, entry, and completion of the manuscript revision. Guoping Huang contributed to the review, revision, and supervision of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this study was provided by the Medical Ethics Review Committee of The Third Hospital of Mianyang, Sichuan Mental Health Center Health Research Ethics Committee of China (Approval Document No.:2022 Annual Review (10)), conducted by the Declaration of Helsinki. Informed consent was obtained from school administrators, students, and their parents prior to data collection.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Long, Q., Huang, B., Tang, Y. et al. Peer victimization and non-suicidal self-injury among high school students: the mediating role of social anxiety, mobile phone addiction, and sex differences. BMC Psychiatry 24, 25 (2024). https://doi.org/10.1186/s12888-024-05495-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-024-05495-8