
Abstract
Background
Research on the impact of metabolic abnormalities on breast cancer prognosis is limited by small samples and assessment of laboratory values at a single time point, often prior to cancer diagnosis and treatment. In this population-based cohort, time-updated laboratory values were adjusted for cancer treatment to assess the association between metabolic risk factors (glucose, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides) and breast cancer survival.
Methods
13,434 women diagnosed with stage I-III breast cancer from 2005-15 at Kaiser Permanente were included. All outpatient fasting glucose, HDL-C, LDL-C, and triglyceride values from diagnosis through 2019 or death were extracted from electronic medical records. Risk of breast cancer-specific mortality was evaluated with Cox proportional hazards models adjusted for metabolic labs, demographics, body mass index, diabetes, dyslipidemia and anti-hypertensive medications, tumor characteristics (stage, ER and HER2 receptor status) and cancer treatment (use of chemotherapy, tamoxifen, and aromatase inhibitors).
Results
Mean (SD) age at diagnosis was 62.3 (11.8) years. Over a median follow-up of 8.6 years, 2,876 patients died; 1,080 of breast cancer. Patients with low HDL-C (≤ 45 vs. > 45 mg/dL) had higher breast cancer-specific mortality (HR, 1.77; 95% CI, 1.53-2.05), as did those with elevated fasting glucose (> 99 vs. 60-99 mg/dL) (HR, 1.19; 95% CI, 1.03-1.37). Elevated levels of triglycerides and LDL-C were not associated with breast cancer-specific mortality.
Conclusions
High fasting glucose and low HDL-C evaluated over time after cancer diagnosis were associated with higher breast cancer mortality independent of cancer treatments and changes in other metabolic risk factors. Future studies should address whether pharmacologic or lifestyle treatment of glucose and lipids after breast cancer diagnosis can optimize survival outcomes.
Similar content being viewed by others

Background
Breast cancer is the second leading cause of cancer death among women in the United States [1]. Even after accounting for tumor characteristics, treatment, and other known risk factors for breast cancer mortality, there remains great heterogeneity in outcomes. Thus, identifying post-diagnosis modifiable risk factors may help improve prognosis [2,3,4].
Systemic metabolic dysregulation, including the highly prevalent conditions of dyslipidemia and hyperglycemia, has been implicated in breast cancer progression. Potential mechanisms include enhanced tumor cell reprogramming and chemoresistance, production of hormones and pro-inflammatory factors, and inhibited cancer cell apoptosis [4,5,6]. Yet, recent epidemiological studies assessing the association between hyperglycemia and breast cancer prognosis tend to focus on glucose values before or at diagnosis and often ignore the confounding influence of cancer treatment on glucose profiles and disease progression [6,7,8].
Dyslipidemia is also believed to influence cancer cell proliferation [2]. In particular, cholesterol’s role in cell membrane structure, cellular signaling pathways, and steroid hormone biosynthesis suggests it may be an important clinical factor in breast cancer development [9, 10]. Yet, the few studies that have assessed the relationship between lipids and prognosis have produced inconsistent results and been limited by small sample sizes and a focus on lipid profiles before lipid-altering cancer treatment [5, 11,12,13].
The role of metabolic dysregulation in breast cancer progression remains unclear, in part because prior studies have been conducted in small populations with assessment of laboratory values at a single time point, often at or before breast cancer diagnosis. Previous observational research often has not controlled for the influence of cancer treatments on metabolic dysregulation, even though emerging evidence suggests that chemotherapy may worsen glucose and lipid levels in breast cancer patients [14,15,16,17]. Endocrine therapies are also known to impact lipids, with prior research suggesting tamoxifen improves lipid profiles, while aromatase inhibitors worsen them [18].
This study of metabolic dysregulation and breast cancer survival is the first, to our knowledge, which assesses glucose, LDL-C, HDL-C, and triglycerides over time after breast cancer diagnosis controlling for cancer treatment.
Methods
Study population
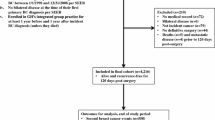
This study population drew from all female Kaiser Permanente Northern California (KPNC) patients 18 years and older who were diagnosed with a first primary invasive stage I-III breast cancer from 2005 through 2014 (n = 21,226). Women were included if they had at least one measurement of all four labs (fasting glucose, LDL-C, HDL-C, and triglycerides) between 24 months pre-diagnosis and 6 months post-diagnosis (n = 13,434). Women included and excluded because of insufficient metabolic data were similar with respect to race/ethnicity, body mass index (BMI) and estrogen receptor (ER) status but differed by stage (58% vs. 49% stage I) and diabetes status (18% vs. 9%). All methods in this retrospective, data-only study were conducted in accordance with relevant guidelines and regulations approved by the Kaiser Permanente Northern California Institutional Review Board with a waiver of written informed consent.
Metabolic measurements and start of follow-up
Outpatient fasting glucose, LDL-C, HDL-C, and triglycerides values were extracted from the electronic medical record (EMR). Baseline labs were selected as the lab value closest to diagnosis within the window of 24 months pre-diagnosis to 6 months post-diagnosis but prior to chemotherapy and radiation (baseline window). Of the four baseline laboratory values (glucose, LDL-C, HDL-C, triglycerides), the date of the most recent baseline lab measurement became the start of follow-up (follow-up start date). If all four baseline lab measurements occurred before breast cancer diagnosis, follow-up started at the diagnosis date. All metabolic measurements from baseline through follow-up were included and were dichotomized in accordance with KPNC’s clinical reference categories (see Table 1). The metabolic measurements were time-updated through follow-up and missing values were managed using last observation carried forward (LOCF) methodology. LOCF is a statistical approach to account for missing data in longitudinal studies in which a participant’s last observed value replaces their subsequent missing observations [19].
Breast cancer-specific mortality and survival time
Death data was obtained from the KPNC death file, comprising the National Death Index and the California Department of Vital Statistics. Patients with International Classification of Diseases (ICD)-10 diagnostic code C50: Malignant neoplasm of breast listed as their immediate or underlying cause of death were considered to have died from breast cancer. Follow-up continued from follow-up start date to death date or December 31, 2019, whichever was earlier.
Fixed and time-varying covariates
Age at diagnosis, race/ethnicity, tumor characteristics (stage, ER status, and human epidermal growth factor receptor 2 [HER2] status), and receipt of chemotherapy were identified from the EMR and KPNC Cancer Registry and treated as fixed covariates.
BMI, diabetes status, receipt of hormone therapies (tamoxifen and/or aromatase inhibitors), and use of dyslipidemia and anti-hypertensive medications were identified from the EMR and treated as time-varying covariates. Patients were identified as having diabetes at baseline if they had a diabetes diagnosis at any point prior to their follow-up start date. Baseline BMI was calculated using the weight measurement closest to diagnosis and the mode of the heights within the baseline window. Patients were classified as being on hormone therapies or medications at baseline if they had a prescription at any point during the baseline window. All time-varying covariates were updated from the follow-up start date through follow-up, utilizing LOCF methodology.
Statistical analysis
Cox proportional hazards models were used to estimate hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) for the association between metabolic dysregulation and breast cancer-specific mortality. Potential confounders were selected a priori and included age at diagnosis, race/ethnicity, BMI, diabetes status, tumor characteristics (stage and ER and HER2 status), cancer treatments (receipt of chemotherapy, tamoxifen and/or aromatase inhibitors), and usage of dyslipidemia and anti-hypertensive medications. A missing indicator was used for variables with missing data (see Table 1). The Cox proportional hazards assumption was assessed via visual examination of the Schoenfeld residuals. Stratified analyses were conducted for the following covariates: age at diagnosis (< 55 and ≥ 55 years); BMI (normal, overweight, class 1 obesity, and class 2/3 obesity as defined by the Centers for Disease Control and Prevention); diabetes status (no and yes); and ER status (negative and positive). Likelihood ratio tests were used to examine possible interactions between stratification variables and metabolic labs. A subsequent analysis of metabolic dysregulation and overall mortality was conducted to assess the potential for competing risks. All statistical analyses were performed using RStudio (version 4.0.2). Statistical significance was established with 2-sided tests with α = 0.05.
Results
Patient characteristics are shown in Table 1. A majority (67%) were non-Hispanic white and mean (standard deviation (SD)) age at diagnosis was 62 (11.8) years. Most women were diagnosed with stage I (58%), ER-positive breast cancers (83%). A majority were overweight or obese (68%), and accordingly a considerable number had diagnosed diabetes (18%), were prescribed anti-hypertensives (57%) and/or dyslipidemia medications (43%) at baseline.
The number and temporal distribution of repeated measurements for each of the metabolic risk factors are shown in Supplemental Figures S1 and S2. The mean (SD) number of repeated measures for each metabolic risk factor (glucose, HDL-C, LDL-C, triglycerides) ranged from 5 (4) to 7 (5), and the mean (SD) time in years between first and last follow-up measurements ranged from 5 (3) to 6 (3). Categorical changes in glucose, HDL-C, LDL-C, and triglycerides from diagnosis (pre-treatment) into survivorship (the first measurement between 1.5- and 3.5-years post-diagnosis) stratified by treatment regimen are presented in supplemental Table S1. While most women remained in the same category over time, depending on the metabolic risk factor examined, up to 25% changed categories. For example, 15.2% of women moved from normal to high glucose and 7.2% from normal to low HDL-C over this period. Treatment type had little impact on these changes, except for tamoxifen where the expected decreases in LDL-C were observed.
Over a median follow-up of 8.6 years, 2,876 patients died, of whom 1,080 (37.6%) died of breast cancer. Hazard ratios and 95% CIs from Cox proportional hazards models are presented in Table 2 and supplemental Table S2. Patients with low HDL-C (≤ 45 vs. > 45 mg/dL) had higher breast cancer-specific mortality (HR, 1.77; 95% CI, 1.53–2.05) and overall mortality (HR, 1.87; 95% CI, 1.71–2.04) (Fig. 1). Those with high glucose (> 99 vs. 60–99 mg/dL) also had higher breast cancer-specific mortality (HR, 1.19; 95% CI, 1.03–1.37) and overall mortality (HR, 1.13; 95% CI 1.04–1.23). Elevated levels of LDL-C and triglycerides were not associated with breast cancer or overall mortality.

Time-Updated Metabolic Lab Values and Risk of Breast Cancer Mortality After. Stage I-III Breast Cancer Diagnosis (N = 13,434)1. 1High LDL (≥ 129 mg/dL); reference = normal (< 129 mg/dL). High triglycerides (≥ 199 mg/dL); reference = normal (< 199 mg/dL). High glucose (> 99 mg/dL); reference = normal (60—99 mg/dL). Low HDL (≤ 45 mg/dL); reference = normal (> 45 mg/dL)
In subgroup analyses, the associations of the metabolic labs with survival were similar across strata defined by age (as proxy for menopausal status), BMI, diabetes, and ER status (Table 3). However, the associations of high glucose with breast cancer mortality differed by diabetes status (HR, 1.41; 95% CI, 1.21–1.65 for no diabetes; HR, 0.77; 95% CI, 0.58–1.03 for diabetes).
Discussion
In this study of 13,434 women with non-metastatic breast cancer from a community-based cohort, low HDL-C and elevated fasting glucose were associated with an increased risk of breast cancer-specific morality, while abnormal LDL-C and triglycerides were not. To our knowledge, this is the first study of metabolic risk factors over time after a breast cancer diagnosis that also accounts for cancer treatments and dyslipidemia medications. Prior research on metabolic dysregulation and prognosis has been inconclusive and limited by small sample sizes, short follow-up, lack of serial measurements and adjustment for cancer treatments, making few studies directly comparable.
The current study utilized time-updated measurements after breast cancer diagnosis and found that elevated glucose may be an important prognostic factor in breast cancer-specific mortality. This adverse association is similar to the results of 2 prior studies on non-diabetics that assessed pre-diagnosis and chemotherapy-related hyperglycemia with overall survival (OS) and 5-year relapse-free survival (RFS) [7, 8]. 2 prior studies that found null associations between at-diagnosis hyperglycemia and various breast cancer outcomes did not adjust for diabetes status nor cancer treatment which may increase glucose levels and impact prognosis [7, 20, 21]. In contrast, this study’s stratified analyses adjusted for cancer treatment and found an adverse association of elevated glucose and breast cancer-specific mortality only among non-diabetics. The apparent inverse association observed among women with diabetes is potentially due to antidiabetic medications used to lower high glucose levels.
In addition to elevated glucose, low HDL-C evaluated over time was associated with breast cancer-specific mortality. This finding is consistent with 2 prior smaller studies that evaluated preoperative and at-diagnosis low HDL-C with overall survival, 1 of which only found a significant association among those with triple-negative breast cancers.[5, 20] In contrast to the current study’s findings, null associations with overall and breast-cancer specific mortality, as well as disease-free survival (DFS) and breast cancer recurrence have been reported [13, 22,23,24]. A potential explanation is that those studies were smaller and assessed HDL-C at a single time point. Moreover, only 1 of those studies adjusted for chemotherapy, whereas this study evaluated HDL-C over a long follow-up period and accounted for the effects of chemotherapy, tamoxifen, aromatase inhibitors, and dyslipidemia medications, all of which affect lipid profiles [18, 25].
Unlike elevated glucose and low HDL-C, high triglycerides and LDL-C were not associated with an increased risk of breast cancer-specific mortality. The null effect of triglycerides is in accordance with the majority of published studies on triglycerides and breast cancer outcomes, except for 1 that found high triglyceride levels to be protective and 1 other that suggested the opposite [4, 5, 13, 20,21,22,23,24]. Of the very few studies that have assessed LDL-C and prognosis, 2 have reported null associations with OS and DFS, while 1 found at-diagnosis high LDL-C was associated with worse DFS at 25 months follow-up [12, 23, 24]. The adverse association was reported in a study with a small sample size and short follow-up period that excluded women on dyslipidemia and/or anti-diabetic medications, yet, did not account for the lipid-altering effects of chemotherapy and endocrine therapy as the current study did [12, 18, 25]. Additionally, epidemiological evidence suggests that statin use among breast cancer patients can target cholesterol metabolism and decrease mortality risk, which could provide a potential explanation for why this study, which adjusted for use of statins over time, did not detect associations with LDL-C [26].
The exact mechanisms by which hyperglycemia and lipids affect breast cancer progression are still being studied. The adverse association found in this study between hyperglycemia and breast cancer-specific mortality is substantiated by current literature that hyperglycemia may promote tumor cell proliferation, invasion, and migration through various pathways, including the “Warburg” effect resulting in increased glucose consumption by cancer cells, activation of epidermal growth factor and insulin receptors, and production of pro-inflammatory factors. Hyperglycemia is also thought to alter the tumor microenvironment, inhibit cancer cell apoptosis, and increase the chemoresistance of tumor cells [6, 27].
Excess lipid biosynthesis may also influence tumor cell proliferation through increased tumor cell metabolic reprogramming, including increased: building materials for cell membrane components, energy via oxidation of fatty acids, and signaling molecules that influence oncogenic pathways [28,29,30,31]. Although hypotheses as to how HDL-C specifically impacts tumor progression are limited, this study’s findings that low HDL-C worsens breast cancer-specific mortality are in accordance with theories that low HDL-C increases activity of pro-inflammatory cytokines and decreases regulation of angiogenesis which could encourage tumor metastasis [4].
Strengths of the study include being the first large study evaluating multiple metabolic exposures and breast cancer-specific survival with a long follow-up time, and incorporation of time-varying exposures post cancer diagnosis. Furthermore, robust multivariate models were used to control for multiple potential confounders, including cancer characteristics and treatment and dyslipidemia medications. Limitations include exclusion of women with insufficient metabolic data; while women in the study were more likely to be diabetic, other notable differences in their characteristics were not detected and stratified analyses by diabetes status were conducted. In addition, clinically collected EMR data was used to characterize metabolic risk factors; thus, the timing of data collection was not perfectly aligned with diagnosis or at regular follow-up intervals. However, the analytic approach enabled us to update metabolic risk factors over time, a novel strength.
Conclusions
The results of this study indicate that elevated glucose and low HDL-C evaluated over time after breast cancer diagnosis is associated with worse breast cancer-specific mortality, after controlling for cancer treatments, dyslipidemia medications, and changes in other metabolic risk factors. Although this study did not detect differences in associations by ER status, future studies by breast cancer subtype are necessary to understand the impact of metabolic dysregulation on the metabolic reprogramming of different tumor types [3, 32]. Given the preclinical literature indicating metabolism may influence tumor progression and the current study’s findings of the significant role of elevated glucose and low HDL-C on breast cancer specific-mortality, future studies should address whether pharmacologic or lifestyle treatment of glucose and lipids after breast cancer diagnosis can optimize survival outcomes.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to being generated based on information collected during clinical care but are available in de-identified form from the corresponding author on reasonable request at the study’s close.
Abbreviations
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- KPNC:
-
Kaiser permanente Northern California
- BMI:
-
Body mass index
- ER:
-
Estrogen receptor
- EMR:
-
Electronic medical record
- ICD:
-
International classification of diseases
- HER2:
-
Human epidermal growth factor receptor 2
- LOCF:
-
Last observation carried forward
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- SD:
-
Standard deviation
- OS:
-
Overall survival
- RFS:
-
Relapse-free survival
- DFS:
-
Disease-free survival
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30.
Cedo L, Reddy ST, Mato E, Blanco-Vaca F, Escola-Gil JC. HDL and LDL: Potential New Players in Breast Cancer Development. J Clin Med 2019;8(6):853.
Song JL, Chen C, Yuan JP, Sun SR. Progress in the clinical detection of heterogeneity in breast cancer. Cancer Med. 2016;5(12):3475–88.
Lofterod T, Mortensen ES, Nalwoga H, Wilsgaard T, Frydenberg H, Risberg T, Eggen AE, McTiernan A, Aziz S, Wist EA, et al. Impact of pre-diagnostic triglycerides and HDL-cholesterol on breast cancer recurrence and survival by breast cancer subtypes. BMC Cancer. 2018;18(1):654.
Li X, Tang H, Wang J, Xie X, Liu P, Kong Y, Ye F, Shuang Z, Xie Z, Xie X. The effect of preoperative serum triglycerides and high-density lipoprotein-cholesterol levels on the prognosis of breast cancer. Breast. 2017;32:1–6.
Qiu J, Zheng Q, Meng X. Hyperglycemia and Chemoresistance in Breast Cancer: From Cellular Mechanisms to Treatment Response. Front Oncol. 2021;11:628359.
Monzavi-Karbassi B, Gentry R, Kaur V, Siegel ER, Jousheghany F, Medarametla S, Fuhrman BJ, Safar AM, Hutchins LF, Kieber-Emmons T. Pre-diagnosis blood glucose and prognosis in women with breast cancer. Cancer Metab. 2016;4:7.
Ahn HR, Kang SY, Youn HJ, Jung SH. Hyperglycemia during Adjuvant Chemotherapy as a Prognostic Factor in Breast Cancer Patients without Diabetes. J Breast Cancer. 2020;23(4):398–409.
Dong S, Wang Z, Shen K, Chen X. Metabolic Syndrome and Breast Cancer: Prevalence, Treatment Response, and Prognosis. Front Oncol. 2021;11:629666.
Jung SM, Kang D, Guallar E, Yu J, Lee JE, Kim SW, Nam SJ, Cho J, Lee SK. Impact of Serum Lipid on Breast Cancer Recurrence. J Clin Med. 2020;9(9):2846.
Guan X, Liu Z, Zhao Z, Zhang X, Tao S, Yuan B, Zhang J, Wang D, Liu Q, Ding Y. Emerging roles of low-density lipoprotein in the development and treatment of breast cancer. Lipids Health Dis. 2019;18(1):137.
Rodrigues dos Santos C, Fonseca I, Dias S, Mendes de Almeida J. Plasma level of LDL-cholesterol at diagnosis is a predictor factor of breast tumor progression. BMC Cancer. 2014;14(132):1–10.
Emaus A, Veierod MB, Tretli S, Finstad SE, Selmer R, Furberg AS, Bernstein L, Schlichting E, Thune I. Metabolic profile, physical activity, and mortality in breast cancer patients. Breast Cancer Res Treat. 2010;121(3):651–60.
Qi A, Li Y, Yan S, Sun H, Zhao M, Chen Y. Effect of postoperative chemotherapy on blood glucose and lipid metabolism in patients with invasive breast cancer. Gland Surg. 2021;10(4):1470–7.
Lu Q, Wu X, Zhu Y, Yang J, Wang X, Ye C, Cai R, Zhang K, Xu T, Wang B, et al. Effects of Chemotherapy on Serum Lipids in Chinese Postoperative Breast Cancer Patients. Cancer Manag Res. 2020;12:8397–408.
He T, Wang C, Tan Q, Wang Z, Li J, Chen T, Cui K, Wu Y, Sun J, Zheng D, et al. Adjuvant chemotherapy-associated lipid changes in breast cancer patients: A real-word retrospective analysis. Medicine (Baltimore). 2020;99(33):e21498.
Hickish T, Astras G, Thomas P, Penfold S, Purandare L, Hickish TF, Kerr D. Glucose intolerance during adjuvant chemotherapy for breast cancer. J Natl Cancer Inst. 2009;101(7):537.
Esteva FJ, Hortobagyi GN. Comparative assessment of lipid effects of endocrine therapy for breast cancer: implications for cardiovascular disease prevention in postmenopausal women. Breast. 2006;15(3):301–12.
LOCF Method and Application in Clinical Data Analysis. 2009. https://www.lexjansen.com/nesug/nesug09/po/PO12.pdf. Accessed 21 November 2022.
Fan Y, Ding X, Wang J, Ma F, Yuan P, Li Q, Zhang P, Xu B. Decreased serum HDL at initial diagnosis correlates with worse outcomes for triple-negative breast cancer but not non-TNBCs. Int J Biol Markers. 2015;30(2):e200-207.
Wulaningsih W, Vahdaninia M, Rowley M, Holmberg L, Garmo H, Malmstrom H, Lambe M, Hammar N, Walldius G, Jungner I, et al. Prediagnostic serum glucose and lipids in relation to survival in breast cancer patients: a competing risk analysis. BMC Cancer. 2015;15:913.
Oh S, Park C, Lee E, Yoon Y, Lee E, Park S, Kim Y, Sung N, Yun Y, Lee K et al: Adipokines, insulin resistance, metabolic syndrome, and breast cancer recurrence: a cohort study. Breast Cancer Research 2011;13:1–10.
His M, Dartois L, Fagherazzi G, Boutten A, Dupre T, Mesrine S, Boutron-Ruault MC, Clavel-Chapelon F, Dossus L. Associations between serum lipids and breast cancer incidence and survival in the E3N prospective cohort study. Cancer Causes Control. 2017;28(1):77–88.
Bahl M, Ennis M, Tannock IF, Hux JE, Pritchard KI, Koo J, Goodwin PJ. Serum lipids and outcome of early-stage breast cancer: results of a prospective cohort study. Breast Cancer Res Treat. 2005;94(2):135–44.
Kang YK, Wang X, Hu NL, Yue J, Si YR, Ju J, Gao SL, Yuan P. The Effects of Endocrine Therapies on Lipid Profiles in Chinese Young Women With Early Breast Cancer. Front Oncol. 2021;11:759595.
Lv H, Shi D, Fei M, Chen Y, Xie F, Wang Z, Wang Y, Hu P. Association Between Statin Use and Prognosis of Breast Cancer: A Meta-Analysis of Cohort Studies. Front Oncol. 2020;10:556243.
Li W, Zhang X, Sang H, Zhou Y, Shang C, Wang Y, Zhu H. Effects of hyperglycemia on the progression of tumor diseases. J Exp Clin Cancer Res. 2019;38(1):327.
Fu Y, Zou T, Shen X, Nelson PJ, Li J, Wu C, Yang J, Zheng Y, Bruns C, Zhao Y, et al. Lipid metabolism in cancer progression and therapeutic strategies. MedComm (2020). 2021;2(1):27–59.
Guo R, Chen Y, Borgard H, Jijiwa M, Nasu M, He M, Deng Y. The Function and Mechanism of Lipid Molecules and Their Roles in The Diagnosis and Prognosis of Breast Cancer. Molecules. 2020;25(20):4864.
Butler LM, Perone Y, Dehairs J, Lupien LE, de Laat V, Talebi A, Loda M, Kinlaw WB, Swinnen JV. Lipids and cancer: Emerging roles in pathogenesis, diagnosis and therapeutic intervention. Adv Drug Deliv Rev. 2020;159:245–93.
Luo X, Cheng C, Tan Z, Li N, Tang M, Yang L, Cao Y. Emerging roles of lipid metabolism in cancer metastasis. Mol Cancer. 2017;16(1):76.
Patra S, Elahi N, Armorer A, Arunachalam S, Omala J, Hamid I, Ashton AW, Joyce D, Jiao X, Pestell RG. Mechanisms Governing Metabolic Heterogeneity in Breast Cancer and Other Tumors. Front Oncol. 2021;11:700629.
Acknowledgements
Not applicable.
Funding
This work was supported by grant R01CA251589 from the National Cancer Institute, and by the American Institute for Cancer Research, Grant Number 632996.
Author information
Authors and Affiliations
Contributions
ECF obtained funding and oversaw the study management, design, analysis, and manuscript writing. AZ led data management, statistical analysis, and writing. BC, WC, EM, and DD helped obtain study funding, reviewed the manuscript for clinical and epidemiological content, and contributed to writing. CQ provided statistical analysis expertise and edited the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Kaiser Permanente Northern California Institutional Review Board. The need for written informed consent to participate in the study was waived by the Kaiser Permanente Northern California Institutional Review Board.
Consent for publication
Not applicable.
Competing interests
Dr. Elizabeth Mittendorf discloses consulting fees, advisory board membership and/or sponsored research agreements from Exact Sciences, Merck, and Roche/Genentech. These were unrelated to this work. Dr. Deborah Dillon discloses contracted research from Canon, Inc and advisory board membership with Oncology Analytics, Inc. These were unrelated to this work. Ms. Zimbalist and Drs. Caan, Chen, Quesenberry, and Cespedes Feliciano have no competing interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Table S1. Change in laboratory values from diagnosis to post-treatment (1.5-3.5 years post-diagnosis).
Additional file 2: Table S2.
Time-Updated Metabolic Labs and Overall Survival in Women With Stage I-III Breast Cancer (N = 13,434; Events = 2,876).
Additional file 3:
Figure S1. Number of Repeated Measurements by Metabolic Risk Factor.
Additional file 4:
Figure S2. Distribution of time between first and last follow-up measurements among women with at least 2 follow-up measurements.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zimbalist, A.S., Caan, B.J., Chen, W.Y. et al. Metabolic abnormalities and survival among patients with non-metastatic breast cancer. BMC Cancer 22, 1361 (2022). https://doi.org/10.1186/s12885-022-10430-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-022-10430-9