
Abstract
Background
There has long been clinical disagreement over the resumption of antiplatelet therapy in patients with primary intracranial hemorrhage (ICH). This meta-analysis aimed to systematically evaluate the efficacy and safety of restarting antiplatelet therapy after ICH among different races and ethnicities.
Methods
All relevant medical studies involving adults with antiplatelet-associated ICH published in PubMed, The Cochrane Library and Chinese National Knowledge Infrastructure from inception to March 2024 were sourced. Outcome measures were thromboembolic events (stroke and myocardial infarction) and recurrence of ICH. After assessing study heterogeneity and publication bias, we performed a meta-analysis using random-effects model to assess the strength of association between resumption of antiplatelet therapy and our outcomes.The review was not registered and the review protocol was not prepared.
Results
Thirty-five studies were included, with 9758 ICH patients. Subgroup analysis revealed that restarting antiplatelet therapy was associated with a significantly higher risk of recurrence or aggravation of cerebral hemorrhage in Asians[OR = 1.48, 95% CI (1.13–1.94), P = 0.004]; in Caucasians, on the contrary, reinitiation of antiplatelet therapy was not associated with a significantly higher risk of recurrence or aggravation of cerebral hemorrhage [OR = 0.85, 95% CI (0.67–1.06), P = 0.149]. Reinitiation of antiplatelet therapy was associated with a significantly lower risk of cerebral infarction [OR = 0.61, 95% CI (0.39–0.96), P = 0.033]. Restarting antiplatelet therapy after cerebral hemorrhage was not associated with a higher incidence rate of mortality [OR = 0.79, 95% CI (0.57, 1.08), P = 0.138], myocardial infarction [OR = 2.40, 95%CI (0.53,10.79), P = 0.253], hemiparesis [OR = 0.38, 95%CI (0.03,4.81), P = 0.451], neurological deficit [OR = 0.86,95%CI(0.32,2.33),P = 0.766].
Conclusion
Reinstitution of antiplatelet therapy after ICH was associated with a lower risk of thromboembolic complications.Resumption of antiplatelet therapy was not associated with a higher incidence of cerebral hemorrhage in Caucasians, but may be associated with a higher risk of cerebral hemorrhage recurrence in Asian populations.
Similar content being viewed by others


Background
Intracerebral hemorrhage refers to the nontraumatic rupture and bleeding of small arteries, which causes blood to accumulate in the brain. It is a type of stroke and can be classified as cerebral small vessel disease [1, 2]. It is one of the most common and serious complications in the current antithrombotic treatment process, and its occurrence is often accompanied by high mortality and disability rates. Since high risk factors for ICH (such as advanced age, hypertension, and smoking) are also risk factors for occlusive vascular disease [3], many ICH patients have ischemic stroke or coronary artery disease [4], which has a long-term onset under these conditions and is an important cause of death [5,6,7]. Antiplatelet therapy is the cornerstone of primary and secondary prevention of ischemic coronary artery disease and stroke; therefore, even after ICH, a considerable number of patients may still need to live antithrombosis treatment for prevention and treatment of occlusal vascular diseases. Among patients with cerebral hemorrhage, as many as 44% are indeed taking antithrombotic drugs [8, 9]. Under normal circumstances, if a patient develops new cerebral hemorrhage or enlarges the hematoma during antithrombotic treatment, the antithrombotic drugs will be stopped immediately. The discontinuation of these drugs is usually permanent. However, the risk of occlusive vascular events may be higher [9], and clinicians are often faced with the challenging decision of whether to restart antithrombotic therapy and, if so, when because of a perceived increased risk of recurrent intracerebral hemorrhage [10]. Nevertheless, we know that in the ten years after the incident, survivors still face a higher risk of death [7]. Therefore, most doctors are reluctant to start antiplatelet therapy in patients with a history of ICH. First, ICH can recur, and previous use of antiplatelet drugs is associated with early hematoma growth in the disease and a higher risk of death [11, 12]. Second, long-term treatment of antiplatelet drugs itself may also increase the incidence of hemorrhagic stroke [13]. To specifically analyze the benefits and safety of patients with ICH after restarting antiplatelet therapy, this article searched relevant studies for a systematic review, which aimed to provide a reference for clinical treatment plans.
Methods
Search strategy
We performed comprehensive searches in PubMed, The Cochrane Library, and Chinese National Knowledge Infrastructure from inception to March 2024. Keywords used to query the databases were selected from the MESH Medical Topics Database, Taking the pubmed database Database as an Example, we used the search terms (“intracranial hemorrhages” OR “brain hemorrhages” OR “cerebral hemorrhages”) AND (“antiplatelet” OR “antithrombotic” OR “anticoagulant” OR “aspirin” OR “clopidogrel” OR “ticlopidine” OR “cilostazol” OR “dipyridamole”) AND (“recurrent intracranial hemorrhage” OR “hematoma expansion” OR “venous thrombosis” OR “arterial thrombosis” OR “myocardial infarction” OR “ischemic stroke” OR “transient ischemic attack”). Articles published in both English and Chinese were included.
Inclusion and exclusion criteria
The inclusion criteria for our study were as follows: (1) Research design: randomized controlled trials or cohort studies; (2) Research objects: all adult ICH patients ≥ 18 years of age; (3) Intervention measures: restart antiplatelet treatment in the experimental group and not reinstate any antithrombotic drugs in the control group; (4) sample size ≥ 10 patients to avoid inclusion of case reports or small case series; (5) Outcome indicators: the experimental group and the control group reported recurrence or aggravation of cerebral hemorrhage(a detrimental event of ICH which results in progressive neurologic deteriorations and poor outcomes and defined as an increase in the hematoma volume or CT attenuation value), ischemic stroke, acute coronary syndrome, myocardial infarction and other cardiovascular events, mortality, hemiplegia, and modified Rankin’s scale (mRS) [14]: mRS score < 2 was divided into good functional outcome, while mRS score > 2 was divided into poor outcome. Quality of life (QOL) score, hemiplegia, neurological deficit.
The specific exclusion criteria were as follows: (1) review, case report, letter, commentary, and medical record reports; (2) studies for which the full text was not available or the data provided by the studies could not be converted in specific analysis; and (3) studies with antiplatelet treatment terminated or changed from antiplatelet treatment to other antithrombotic treatment in patients during follow-up.
Study screening and data extraction
A single investigator (W.X.) had read the title and abstract produced by the initial search and shortlisted articles for further review. These articles were then independently reviewed by 2 investigators (C.T. and Z.J.) and selected based on the inclusion criteria and quality of data. Any disagreements were resolved by a third investigator (Q.Y.). The basic information of the extracted study included author, year, country, age, gender, intervention measures, treatment course, follow-up time limit, etc.
Study quality evaluation and statistical methods
The quality of studies were evaluated using the Cochrane Risk of Bias tool for randomized controlled trials (RCTs) and using the Newcastle‒Ottawa Scale (NOS) [15] for non-randomised studies, which was based on the selection of study groups, comparability of groups and ascertainment of outcome. We used Stata (version 15.0) to perform statistical analysis on the benefits and risks of antiplatelet resumption using the pooled odds ratio (OR) and 95% confidence interval (95% CI) as the effect parameter. The I2 statistic was used to evaluate heterogeneity (with I2 > 50% indicating significant heterogeneity) as was Cochran’s Q P value (with P value < 0.05 indicating significant heterogeneity). To account for heterogeneity, random-effects model was used throughout. Sensitivity analysis was performed to address the influence of each single study on the overall results by removing one study at a time and calculating the combined OR for the remaining studies. Begg’s test [16] and Egger’s test [17] were conducted to evaluate publication bias. All tests were 2-tailed, and P values < 0.05 were considered significant.
Results
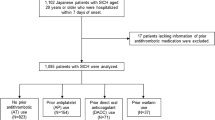
A total of 2360 titles and abstracts were screened, from which 35 studies met the inclusion criteria. The flow chart of study selection was shown in Fig. 1. There were 16 studies [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34] in Asia, 17 studies [35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51] in Europe or America, a study [52] in Australia.

Flow chart of study selection
The 35 studies were published between 1982 and 2024 and included 9758 patients. Among these patients, antiplatelet therapy was restarted in 2971 (30.45%) patients and not restarted in the remaining 6787 patients (69.55%). The mean age of patients, location of ICH, type of antiplatelet agents, timing of antiplatelet resumption, duration of follow-up, and NOS scores of the cohort study were all shown in Table 1. Quality assessment of included RCTs were shown in Fig. 2.

Quality assessment of included RCTs
Comparison of incidence rate of recurrence or aggravation of ICH
Thirty-five studies [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52] (9758 patients) reported the effect of antiplatelet therapy on the incidence of recurrence or aggravation of cerebral hemorrhage. The rate of recurrence or aggravation of cerebral hemorrhage in patients on antiplatelet therapy was 13.33% compared with 15.07% for patients not restarted on antiplatelet therapy (Fig. 2). The heterogeneity was detected (I2 = 46.6%, p = 0.002), We performed subgroup analyses by different races and ethnicities. Then there was no heterogeneity within subgroups. In the Asian population, restarting antiplatelet therapy was associated with higher incidence of recurrence or aggravation of cerebral hemorrhage [OR = 1.48, 95% CI (1.13–1.94), P = 0.004], and no significant heterogeneity (I2 = 13.0%, P = 0.305) was found between these articles; however, the opposite result appeared in the Caucasian population, restarting antiplatelet therapy was not associated with higher incidence of recurrence or aggravation of cerebral hemorrhage [OR = 0.85, 95% CI (0.67–1.06), P = 0.149], with no significant heterogeneity (I2 = 33.5%, P = 0.078), as shown in Fig. 3. A study [51] reported that restarting antiplatelet therapy in patients with non-lobar hemorrhage was associated with a lower incidence rate of cerebral hemorrhage [OR = 0.31, 95% CI (0.10–0.96), P = 0.047], and restarting antiplatelet therapy in patients with lobar hemorrhage was not associated with a higher incidence of cerebral hemorrhage [OR = 0.71, 95% CI (0.28–1.82), P = 0.480]. We did subgroup analyses according to different study designs. Due to the presence of heterogeneity (I2 = 53.1%, P = 0.001), random-effects model was chosen.Both RCTs and cohort studies showed that restarting antiplatelet therapy was not associated with a higher incidence rate of cerebral hemorrhage, as shown in Fig. 4. Subgroup analyses of different locations of the bleed showed that restarting antiplatelet therapy was not associated with a higher incidence rate of cerebral hemorrhage in either subarachnoid subgroup or subdural subgroup or intraparenchymal subgroup, as shown in Fig. 5. Subgroup analysis of different antiplatelet agents showed that aspirin was associated with a higher incidence rate of cerebral hemorrhage, but dipyridamole and ozagrel were not associated with a higher incidence rate of cerebral hemorrhage, as shown in Fig. 6.

Forest plot of the incidence of recurrence or aggravation of ICH after restarting antiplatelet treatment based on different races and ethnicities

Forest plot of the incidence of recurrence or aggravation of ICH after restarting antiplatelet treatment based on different study designs

Forest plot of the incidence of recurrence or aggravation of ICH after restarting antiplatelet treatment based on different locations of the bleed

Forest plot of the incidence of recurrence or aggravation of ICH after restarting antiplatelet treatment based on different antiplatelet drugs
Comparison of incidence rate of ischemic stroke
Thirteen studies [21, 22, 31, 33, 34, 37,38,39, 41, 43, 45, 46, 51] (3517 patients) reported the effect of antiplatelet therapy on the incidence rate of cerebral infarction. There was large statistical heterogeneity (I2 = 60.1%, P = 0.003). Heterogeneity did not decrease after subgroup division, and the random-effects model was used for analysis. The results showed that restarting antiplatelet treatment after ICH was associated with a lower incidence rate of cerebral infarction [OR = 0.61, 95% CI (0.39–0.96), P = 0.033], as shown in Fig. 7.

Forest plot of the incidence of ischemic stroke after restarting antiplatelet treatment after ICH
Comparison of incidence rate of mortality
Eleven studies [19, 21, 29, 34, 37,38,39, 42, 47, 49, 51] (2448 patients) reported the effect of antiplatelet therapy on mortality, and there was no heterogeneity among studies (I2 = 0%, P = 0.888). A random-effect model was used for analysis. The results showed that restarting antiplatelet treatment after ICH was not associated with a higher incidence rate of mortality [OR = 0.79, 95% CI (0.57, 1.08), P = 0.138], as shown in Fig. 8.

Forest plot of mortality of patients after restarting antiplatelet treatment after ICH
Other outcome indicators
The balance of ischemic cardiovascular events and recurrent ICH, among other bleeding complications, may affect functional outcomes and health-related quality of life measures after hospital discharge. In addition, the effect of recurrent ICH in patients taking antiplatelet therapy on these measures may not be accurately portrayed by the incidence of recurrent ICH alone. So we evaluated the effects of restarting antiplatelet therapy on QOL score, MRS score, neurological deficit, and hemiplegia. Restarting antiplatelet therapy after cerebral hemorrhage was not associated with a higher incidence rates of neurological deficits, cardiovascular events, or hemiparesis. Antiplatelet resumption after cerebral hemorrhage was not associated with lower rates of functional outcome MRS score, QOL score, as shown in Table 2. Due to the small number of included studies and low test power, sensitivity analysis and publication bias evaluation were not performed.
Sensitivity analysis
Because of significant heterogeneity when assessing the relationship between resumption of antiplatelet therapy and the incidence of recurrence or aggravation of cerebral hemorrhage, we conducted sensitivity analyses. Sensitivity analyses investigating the influence of a single study on the overall risk estimate by omitting one study at each turn yielded a narrow range of ORs from 0.98 (0.81–1.12) to 1.11 (0.92–1.33). In other words, no single study substantially contributed to the heterogeneity across studies.
Publication bias
Begg’s test and Egger’s test were performed on the incidence of recurrence or aggravation of cerebral hemorrhage after restarting antiplatelet treatment, and no evidence of publication bias was observed (Egger’s test: P = 0.55; Begg’s test: P = 0.98). Therefore, it was the same for ischemic stroke (Egger’s test: P = 0.83; Begg’s test: P = 0.86) and mortality (Egger’s test: P = 0.20; Begg’s test: P = 0.44).
Discussion
Our systematic review results showed that restarting antiplatelet therapy after ICH was associated with a lower risk of ischemic stroke, which was consistent with the research of Blackwell [13] and met clinical expectations. Among patients with ischemic stroke and a history of cardiovascular disease, restarting antiplatelet therapy was not associated with a higher rate of cardiovascular events (myocardial infarction, acute coronary syndrome), although cardiovascular events occurred in 5.71% and 3.27% after restarting or not restarting antiplatelet therapy, respectively. We included a small number of studies (only 3) [22, 47, 51], a total of 1174 patients, and the heterogeneity (I2 = 84.6%, P = 0.002) between studies. thus it’s still necessary to carefully read the research results. However, another RCT PICASSO [53], for the prevention of cardiovascular events in Asian patients with ischemic stroke at high risk of cerebral hemorrhage showed that compared with the use of antiplatelet drugs (cilostazol or aspirin) alone, the addition of probucol to antiplatelet therapy (cilostazol or aspirin) was associated with a lower risk of cardiovascular events. It may provide a new choice for Asian patients with ischemic stroke at a high risk of cerebral hemorrhage in the prevention of cardiovascular events.
Regarding the risk of restarting antiplatelet therapy after cerebral hemorrhage, some research data could be used as a reference for medical decision-making, but the results between the studies were not consistent [34, 41, 49, 54]. The latest American Heart Association (AHA) guidelines [55] vaguely recommended anticoagulant after non-lobar ICH or antiplatelet monotherapy after any ICH might be considered, particularly when there were strong indications for these agents (class IIb; level of evidence B). In terms of bleeding risk after restarting antiplatelet therapy after ICH, we had different results in different subgroups. The incidence of cerebral hemorrhage after restarting antiplatelet treatment (12.45%) is slightly lower than that without restarting antiplatelet treatment (17.09%) in the Caucasian population. This is unexpected because antiplatelet therapy generally seems to be associated with an increased risk of bleeding events. Although random effects cannot be ruled out, the underlying cause of this phenomenon may not be as counterintuitive as it first appears.On the one hand, arterial thrombosis can trigger haemorrhage [56]. On the other hand, more spontaneous intracerebral haemorrhages than expected might be due to haemorrhagic transformation of ischaemic stroke.The RCT RESTART by Salman [51] also found that restarting antiplatelet therapy after cerebral hemorrhage significantly reduced the incidence of cerebral hemorrhage.Therefore, in the Caucasian population, the modest increase in the risk of recurrent ICH with antiplatelet therapy cannot exceed the established benefits of antiplatelet therapy for secondary prevention [13]. In contrast, in the Asian population, the results of our systematic review showed that the risk of recurrence or aggravation of cerebral hemorrhage was significantly increased after restarting antiplatelet therapy. Several studies [57,58,59] have shown that certain ethnicities were associated with a greater risk of hemorrhagic strokes. In addition, in a systematic review by van Asch [60], the incidence rate of ICH was 51.8 per 100,000 person-years in Asians, which was significantly higher than the incidence rate in Caucasians of 24.2 per 100,000 person-years. Moreover, compared with Caucasians, Asian populations have a higher ICH incidence rate associated with hypertension and a lower ICH incidence rate associated with cerebral amyloid angiopathy [61, 62]. In the presence of cerebral microbleeds, Asians are at greater risk of ICH. Due to the special epidemiological characteristics, etiology and pathophysiology of ICH among Asian populations, we must strictly and carefully extrapolate the research results to Asian populations.
Among the studies included in our systematic review, Salman’s study [51] reported on cerebral lobar hemorrhage and non-lobar hemorrhage: interestingly, in the lobar hemorrhage subgroup, starting antiplatelet therapy did not seem to be associated with a higher rate of recurrent ICH [OR = 0.71, 95% CI (0.28–1.82), P = 0.480]. Although Salman’s study found that restoration of antithrombotic drugs in patients with lobar hemorrhage would not lead to a significant increase in recurrent ICH, several confounding factors were not considered, such as the number of cortical microbleeds at baseline, the degree of white matter disease/hypertension, and a prior history of cerebral hemorrhage. Another study [63] by Salman concluded that there was no significant difference in the recurrence rate of cerebral hemorrhage after strict lobar microhemorrhage and hemorrhage in other locations. However, it is worth noting that only 7/122 (15%) and 23/132 (29%) patients had severe cortical microbleeds in the restarted antiplatelet therapy experimental group and the non-restarted antiplatelet therapy control group, respectively. Patients with multiple cortical microbleeds were considered to be at higher risk of recurrent cerebral hemorrhage and were underrepresented in this study. This was contradictory to Biffi’s observational study [64] regarding the risk of recurrent ICH in patients with lobar hemorrhage after resuming aspirin. Both randomized controlled trial [65] and pooled analyse [66] of population-based study found that patients with a history of lobar hemorrhage had a higher risk of cerebral hemorrhage than those with non-lobar hemorrhage; meanwhile, patients with lobar ICH without comorbid atrial fibrillation had a risk of recurrent ICH greater than the risk of ischemic stroke. The difference in bleeding location (lobar ICHs and non-lobar ICHs) was fundamentally the reason for the difference in the two different pathophysiological mechanisms. Most lobar hemorrhages in elderly patients may be secondary to amyloid deposits in the distal middle and small arteries near the cortex. Therefore, patients with moderate to severe cerebral amyloid angiopathy must be cautiously initiated antiplatelet therapy. Further studies are needed in this patient population.
In the non-lobar hemorrhage subgroup, the resumption of antiplatelet therapy was associated with a lower recurrence of ICH. It is generally believed that non-lobar or subcortical cerebral hemorrhage is caused by Charcot-Bouchard affecting the penetrating arterioles secondary to chronic hypertension. The result of a RCT by Banerjee [65] showed that patients with a history of non-lobar hemorrhage have a lower risk of cerebral hemorrhage than those with lobar hemorrhage. Snyder [67] found that the resumption of antiplatelet therapy after non-lobar hemorrhage did not increase ICH recurrence. After the absorption of hematoma and improvement of secondary tissue damage, patients with hypertension-related non-lobar hemorrhage with no obvious cerebral micro-hemorrhage and strong indications for antiplatelet therapy may safely restart antiplatelet therapy. However, the determination of the optimal timing of resumption and the selection of appropriate types of antiplatelet drugs remain unsolved. The selection of high-risk patients, determination of the optimal timing of resuming treatment, and choice of appropriate antiplatelet agent are issues that remain unresolved in relation to ICH. Nevertheless, the administration of antiplatelet therapy might be as early as possible to prevent new ischemic lesions and subsequent vascular events [68]. A large amount of research is essential to determine the balance time point in the middle.
In addition, several limitations exist in our meta-analysis. First, we included only Chinese and English studies, and language restrictions may cause bias and affect the applicability of our research results. Second, only a relatively small number of RCTs were included in our systematic review. Third, to obtain as much data as possible, we included not only studies of spontaneous ICH but also subdural hemorrhage and subarachnoid hemorrhage. Hence, there was variability in the selection criteria of individual studies. Fourth, the effect of antiplatelet therapy may depend on the type of drug used. Previous study [69] showed that low-dose aspirin treatment after hemorrhagic stroke was associated with improved survival, but clopidogrel did not have these beneficial effects. Cilostazol had a lower bleeding tendency [53]. Different antiplatelet drugs have different effects. Since most of the studies we included did not separately count the patient’s condition after the application of antiplatelet drugs with different mechanisms of action and the time to restart antiplatelet therapy, our study failed to analyze the difference in the efficacy of various antiplatelet agents. Fifth, for some of the outcome indicators, such as neurological deficit, hemiplegia, incidence of cardiovascular events, MRS score, and QOL score, both the number of included studies and patients were small and insufficient, so the conclusion from this part of the analysis is difficult to be convincing. Finally, although our study found a large difference in the incidence of ICH between Asians and Caucasians after restarting antiplatelet therapy, we failed to determine what causes the difference (epidemiology, etiology or pathophysiological variations).
Conclusion
In summary, reinstitution of antiplatelet therapy after ICH was associated with a lower risk of thromboembolic complications.Resumption of antiplatelet therapy was not associated with a higher incidence of cerebral hemorrhage in Caucasians, but may be associated with a higher risk of cerebral hemorrhage recurrence in Asian populations.
Data availability
Datasets are available through the corresponding author upon reasonable request.
Abbreviations
- ICH:
-
Intracranial hemorrhage
- mRS:
-
Modified Rankin’s scale
- QOL:
-
Quality of life
- NOS:
-
Newcastle‒Ottawa Scale
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- RCT:
-
Randomized controlled trial
- NR:
-
Not reported
References
Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges[J]. Lancet Neurol. 2010;9(7):689–701. https://doi.org/10.1016/S1474-4422(10)70104-6.
Cuadrado-Godia E, Dwivedi P, Sharma S et al. Cerebral small vessel disease: a review focusing on pathophysiology, biomarkers, and machine learning Strategies[J]. J Stroke. 2018;20(3):302–20. https://doi.org/10.5853/jos.2017.02922.
O’Donnell MJ, Xavier D, Liu L et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study[J]. Lancet. 2010;376(9735):112–23. https://doi.org/10.1016/S0140-6736(10)60834-3.
Poon MT, Fonville AF, Al-Shahi Salman R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis[J]. J Neurol Neurosurg Psychiatry 2014,85(6):660–7. https://doi.org/10.1136/jnnp-2013-306476
Béjot Y, Cordonnier C, Durier J et al. Intracerebral haemorrhage profiles are changing: results from the Dijon population-based study[J]. Brain. 2013;136(Pt2):658–64. https://doi.org/10.1093/brain/aws349.
Vermeer SE, Algra A, Franke CL, et al. Long-term prognosis after recovery from primary intracerebral hemorrhage[J]. Neurology. 2002;59(2):205–9. https://doi.org/10.1212/wnl.59.2.205.
Hansen BM, Nilsson OG, Anderson H et al. Long term (13 years) prognosis after primary intracerebral haemorrhage: a prospective population based study of long term mortality, prognostic factors and causes of death[J]. J Neurol Neurosurg Psychiatry. 2013;84(10):1150–5. https://doi.org/10.1136/jnnp-2013-305200.
Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients[J]. Br Med J 2002,324(7329):71–86. https://doi.org/10.1136/bmj.324.7329.71
Pasquini M, Charidimou A, van Asch CJ et al. Variation in restarting antithrombotic drugs at hospital discharge after intracerebral haemorrhage[J]. Stroke 2014,45(9):2643–8. https://doi.org/10.1161/STROKEAHA.114.006202
Monden K, Sadamori H, Hioki M, et al. Safety and feasibility of liver resection with continued antiplatelet therapy using aspirin[J]. J Hepato-Biliary-Pancreat Sci. 2017;24(7):375–81. https://doi.org/10.1002/jhbp.461.
Roquer J, Vivanco-Hidalgo RM, Capellades J et al. Ultraearly hematoma growth in antithrombotic pretreated patients with intracerebral hemorrhage[J]. Eur J Neurol 2018,25(1):83–9. https://doi.org/10.1111/ene.13458
Toyoda K, Yasaka M, Nagata K et al. Antithrombotic therapy influences location, enlargement, and mortality from intracerebral hemorrhage. The bleeding with antithrombotic therapy (BAT) retrospective Study[J]. Cerebrovasc Dis,2009,27(2):151–9. https://doi.org/10.1159/000177924
Antithrombotic Trialists’ (ATT), Collaboration, Baigent C, Blackwell L et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials[J]. Lancet 2009,373(9678):1849–60. https://doi.org/10.1016/S0140-6736(09)60503-1
Bamford JM, Sandercock PA, Warlow CP, et al. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1989;20(6):828. https://doi.org/10.1161/01.str.20.6.828.
Wells G. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses[C]// Symposium on Systematic Reviews: Beyond the Basics. 2014.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias[J]. Biometrics. 1994;50(4):1088–101. https://doi.org/10.2307/2533446.
Egger M, Smith GD, Schneider M, et al. Bias in meta-analysis detected by a simple[J]. BMJ Clin Res. 1997;315(7109):629–34. https://doi.org/10.1136/bmj.315.7109.629.
Suzuki S, Sano K, Handa H, et al. Clinical study of OKY-046, a thromboxane synthetase inhibitor, in prevention of cerebral vasospasms and delayed cerebral ischaemic symptoms after subarachnoid haemorrhage due to aneurysmal rupture: a randomized double-blind study[J]. Neurol Res. 1989;11(2):79–88. https://doi.org/10.1080/01616412.1989.11739867.
Tokiyoshi K, Ohnishi T, Nii Y. Efficacy and toxicity of thromboxane synthetase inhibitor for cerebral vasospasm after subarachnoid hemorrhage[J]. Surg Neurol. 1991;36(2):112–8. https://doi.org/10.1016/0090-3019(91)90228-2.
Torihashi K, Sadamasa N, Yoshida K, et al. Independent predictors for recurrence of chronic subdural hematoma: a review of 343 consecutive surgical cases. Neurosurgery. 2008;63(6):1125–9. https://doi.org/10.1227/01.NEU.0000335782.60059.17.
Jia WH, Zhou LC. Ban Nao Chu Xue Shi De que xue xing Cu Zhong Huan Zhe Shi Yong kang xue xiao ban Yao Wu Er Ji Yu Fang De Diao cha[J]. Chin J Neurol. 2010;43(12):828–31. https://doi.org/10.3760/cma.j.issn.1006-7876.2010.12.004. (in Chinese).
Chong BH, Chan KH, Pong V, et al. Use of aspirin in Chinese after recovery from primary intracranial haemorrhage[J]. Thromb Haemost. 2012;107(2):241–7. https://doi.org/10.1160/TH11-06-0439.
Chon KH, Lee JM, Koh EJ, et al. Independent predictors for recurrence of chronic subdural hematoma[J]. Acta Neurochir. 2012;154(9):1541–8. https://doi.org/10.1007/s00701-012-1399-9.
Okamura A, Kawamoto Y, Sakoda E, et al. Evaluation of recurrence factors and Gorei-san administration for chronic subdural hematoma after percutaneous subdural tapping.[J]. Hiroshima J Med Sci. 2013;62(4):77–82. PMID: 24597210.
Okano A, Oya S, Fujisawa N, et al. Analysis of risk factors for chronic subdural haematoma recurrence after burr hole surgery: optimal management of patients on antiplatelet therapy[J]. Br J Neurosurg. 2014;28(2):204–8. https://doi.org/10.3109/02688697.2013.829563.
Teo KC, Mahboobani NR, Lee R, et al. Warfarin associated intracerebral hemorrhage in Hong Kong Chinese.[J]. Neurol Res. 2014;36(2):143–9. https://doi.org/10.1179/1743132813Y.0000000275.
Tugcu B, Tanriverdi O, Baydin S, et al. Can recurrence of chronic subdural hematoma be predicted? A retrospective analysis of 292 Cases[J]. J Neurol Surg Part A: Cent Eur Neurosurg. 2014;75(1):37–41. https://doi.org/10.1055/s-0032-1330961.
Wada M, Yamakami I, Higuchi Y, et al. Influence of antiplatelet therapy on postoperative recurrence of chronic subdural hematoma: a multicenter retrospective study in 719 patients[J]. Clin Neurol Neurosurg. 2014;120:49–54. https://doi.org/10.1016/j.clineuro.2014.02.007.
Mizutani K, Miwa T, Tamura R, et al. The perioperative management of antiplatelet agents for chronic subdural hematoma.[J]. Clin Neurol Neurosurg. 2014;117:100–1. https://doi.org/10.1016/j.clineuro.2013.11.035
Chen T, Xu G, Tan D, et al. Effects of platelet infusion, anticoagulant and other risk factors on the rehaemorrhagia after surgery of hypertensive cerebral hemorrhage[J]. Volume 19. European Review for Medical & Pharmacological Sciences; 2015. pp. 795–9. 5PMID: 25807432.
Amano T, Takahara K, Maehara N, et al. Optimal perioperative management of antithrombotic agents in patients with chronic subdural hematoma[J]. Clin Neurol Neurosurg. 2016;151:43–50. https://doi.org/10.1016/j.clineuro.2016.10.002.
Kuwabara M, Takashi S, Kiyoshi Y, et al. The Effect of Irrigation Solutions on recurrence of chronic subdural hematoma: a consecutive cohort study of 234 Patients[J]. Neurol Med Chir. 2017;57(5):210–6. https://doi.org/10.2176/nmc.oa.2016-0228.
Liang GL, Wang XL, Ou B. Nao Chu Xue Huan Zhe Fu Yong kang xue xiao ban Yao Wu Yu Nao Cu Zhong Fu Fa de guan xi he an quan xing Yan jiu[J]. Mod Diagnosis Treat, 2017(12):2222–4.https://doi.org/10.3969/j.issn.1001-8174.2017.12.041(in Chinese).
Teo KC, Lau GK, Mak R, et al. Antiplatelet Resumption after Antiplatelet-Related Intracerebral Hemorrhage: a Retrospective Hospital-based Study[J]. World Neurosurg. 2017;106:85–91. https://doi.org/10.1016/j.wneu.2017.06.015.
Mendelow AD, Stockdill G, Steers AJW, et al. Double-blind trial of aspirin in patients receiving tranexamic acid for subarachnoid haemorrhage[J]. Acta Neurochir. 1982;62(3–4):195–202. https://doi.org/10.1007/BF01403624.
Shaw MDM, Foy PM, Conway M, et al. Dipyridamole and postoperative ischemic deficits in aneurysmal subarachnoid hemorrhage.[J]. J Neurosurg. 1985;63(5):699–703. https://doi.org/10.3171/jns.1985.63.5.0699.
Juvela S. Aspirin and delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage[J]. J Neurosurg. 1995;82(6):945–52. https://doi.org/10.3171/jns.1995.82.6.0945.
Hop JW, Rinkel GJE, Algra A, et al. Randomized pilot trial of postoperative aspirin in subarachnoid hemorrhage[J]. Neurology. 2000;54(4):872–8. https://doi.org/10.1212/wnl.54.4.872.
Walter M, van den Bergh. Randomized Controlled Trial of Acetylsalicylic Acid in Aneurysmal Subarachnoid Hemorrhage: the MASH Study[J]. Stroke,2006,37(9):2326–30. https://doi.org/10.1161/01.STR.0000236841.16055.0f
Lindvall P, Koskinen L. Anticoagulants and antiplatelet agents and the risk of development and recurrence of chronic subdural haematomas[J]. J Clin Neurosci. 2009;16(10):1287–90. https://doi.org/10.1016/j.jocn.2009.01.001.
Flynn R, Macdonald TM, Murray GD, et al. Prescribing antiplatelet medicine and subsequent events after intracerebral hemorrhage[J]. Stroke. 2010;41(11):2606–11. https://doi.org/10.1161/STROKEAHA.110.589143.
Aspegren OP, Åstrand R, Lundgren M, et al. Anticoagulation therapy a risk factor for the development of chronic subdural hematoma[J]. Clin Neurol Neurosurg. 2013;115(7):981–4. https://doi.org/10.1016/j.clineuro.2012.10.008.
Baraniskin A, Steffens C, Harders A et al. Impact of pre-hospital antithrombotic medication on the outcome of chronic and acute subdural hematoma.[J]. J Neurol Surg A Central Eur Neurosurg. 2014;75(1):31–6. https://doi.org/10.1055/s-0032-1325629.
Leroy HA, Rabih Aboukaïs, Reyns N, et al. Predictors of functional outcomes and recurrence of chronic subdural hematomas[J]. J Clin Neurosci. 2015;22(12):1895–900. https://doi.org/10.1016/j.jocn.2015.03.064.
Nielsen PB, Larsen TB, Flemming S et al. Restarting anticoagulant treatment after intracranial hemorrhage in patients with atrial fibrillation and the impact on recurrent stroke, mortality, and bleeding: a Nationwide Cohort Study[J]. Circulation. 2015;132(6):517–25. https://doi.org/10.1161/Circulationaha.115.015735
Guha DCS, Macdonald RL. Timing of the resumption of antithrombotic agents following surgical evacuation of chronic subdural hematomas: a retrospective cohort study.[J]. J Neurosurg 2016,124(3):750–9 https://doi.org/10.3171/2015.2.JNS141889.
Kamenova M, Nevzati E, Lutz K, et al. Burr-Hole drainage for chronic subdural hematoma under low-dose acetylsalicylic acid: a comparative risk analysis study[J]. World Neurosurg. 2017;100:594–600. https://doi.org/10.1016/j.wneu.2017.01.065.
Brennan PM, Kolias AG, Joannides AJ et al. The management and outcome for patients with chronic subdural hematoma: a prospective, multicenter, observational cohort study in the United Kingdom[J]. J Neurosurg. 2017:1–8. https://doi.org/10.3171/2016.8.JNS16134.
Chen CJ, Ding D, Buell TJ, et al. Restarting antiplatelet therapy after spontaneous intracerebral hemorrhage: functional outcomes[J]. Neurology. 2018;91(1):e26–36. https://doi.org/10.1212/WNL.0000000000005742.
Abboud T, Dhrsen L, Gibbert C, et al. Influence of antithrombotic agents on recurrence rate and clinical outcome in patients operated for chronic subdural hematoma[J]. Neurocirugía (English Edition). 2018;29(2):86–92. https://doi.org/10.1016/j.neucir.2017.09.006.
Salman AS, Dennis MS, Sandercock P et al. Effects of antiplatelet therapy after stroke due to intracerebral haemorrhage (RESTART): a randomised, open-label trial[J]. Lancet 2019,393(10191):2613–23. https://doi.org/10.1016/S0140-6736(19)30840-2
Rust T, Kiemer N, Erasmus A. Chronic subdural haematomas and anticoagulation or anti-thrombotic therapy[J]. J Clin Neurosci. 2006;13(8):823–7. https://doi.org/10.1016/j.jocn.2004.12.013.
Kim BJ, Lee EJ, Kwon SU, et al. Prevention of cardiovascular events in Asian patients with ischaemic stroke at high risk of cerebral haemorrhage (PICASSO): a multicentre, randomised controlled trial. Lancet Neurol. 2018;17(6):509–18. https://doi.org/10.1016/S1474-4422(18)30128-5.
Ottosen TP, Grijota M, Hansen ML, et al. Use of antithrombotic therapy and long-term clinical outcome among patients surviving intracerebral hemorrhage. Stroke. 2016;47(7):1837–43. https://doi.org/10.1161/STROKEAHA.116.012945.
Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(7):2160–236. https://doi.org/10.1161/STR.0000000000000024.
Garcia-Yebenes I, Sobrado M, Zarruk JG, et al. A mouse model of hemorrhagic transformation by delayed tissue plasminogen activator administration after in situ thromboembolic stroke. Stroke. 2011;42(1):196–203. https://doi.org/10.1161/STROKEAHA.110.600452.
Rodriguez-Torres A, Murphy M, Kourkoulis C, et al. Hypertension and intracerebral hemorrhage recurrenceamong white, black, and hispanic individuals. Neurology. 2018;91(1):e37–44. https://doi.org/10.1212/WNL.0000000000005729.
Venketasubramanian N, Yoon BW, Pandian J, et al. Stroke epidemiology in South, East, and South-East Asia: a review. J Stroke. 2017;19(3):286–94. https://doi.org/10.5853/jos.2017.00234.
Li YG, Lip GYH. Anticoagulation resumption after intracerebral hemorrhage. Curr Atheroscler Rep. 2018;20(7):32. https://doi.org/10.1007/s11883-018-0733-y.
van Asch CJ, Luitse MJ, Rinkel GJ, et al. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9(2):167–76. https://doi.org/10.1016/S1474-4422(09)70340-0.
Tsai CF, Anderson N, Thomas B, et al. Comparing risk factor profiles between intracerebral hemorrhage and ischemic stroke in Chinese and white populations: systematic review and meta-analysis. PLoS ONE. 2016;11(3):e0151743. https://doi.org/10.1371/journal.pone.0151743.
Chen YW, Lee MJ, Smith EE. Cerebral amyloid angiopathy in East and West. Int J Stroke. 2010;5(5):403–11. https://doi.org/10.1111/j.1747-4949.2010.00466.x.
Al-Shahi Salman R, Minks DP, Mitra D, et al. Effects of antiplatelet therapy on stroke risk by brain imaging features of intracerebral haemorrhage and cerebral small vessel diseases: subgroup analyses of the RESTART randomised, open-label trial. Lancet Neurol. 2019;18(7):643–52. https://doi.org/10.1016/S1474-4422(19)30184-X.
Biffi A, Halpin A, Towfighi A, et al. Aspirin and recurrent intracerebral hemorrhage in cerebral amyloid angiopathy. Neurology. 2010;75(8):693–8. https://doi.org/10.1212/WNL.0b013e3181eee40f.
Banerjee G, Wilson D, Ambler G, et al. Longer term stroke risk in intracerebral haemorrhage survivors[J]. J Neurol Neurosurg Psychiatry. 2020;91(8):840–5. https://doi.org/10.1136/jnnp-2020-323079.
Li L, Poon MTC, Samarasekera NE, et al. Risks of recurrent stroke and all serious vascular events after spontaneous intracerebral haemorrhage: pooled analyses of two population-based studies. Lancet Neurol. 2021;20(6):437–47. https://doi.org/10.1016/S1474-4422(21)00075-2.
Snyder MH, Ironside N, Kumar JS et al. Antiplatelet therapy and delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. J Neurosurg 2021 Nov 5:1–13. https://doi.org/10.3171/2021.7.JNS211239
Kang DW, Han MK, Kim HJ, et al. New ischemic lesions coexisting with acute intracerebral hemorrhage. Neurology. 2012;79(9):848–55. https://doi.org/10.1212/WNL.0b013e3182648a79.
González-Pérez A, Gaist D, de Abajo FJ, et al. Low-dose aspirin after an episode of Haemorrhagic Stroke is Associated with Improved Survival. Thromb Haemost. 2017;117(12):2396–405. https://doi.org/10.1160/TH17-05-0342.
Funding
None.
Author information
Authors and Affiliations
Contributions
W.X and C.T contributed equally to the study and were co-first authors. W.X and Q.Y contributed to the design, W.X and C.T statistical analysis, participated in most of the study steps. C.T and Q.Y prepared the manuscript. Z.J assisted in designing the study. All authors have read and approved the content of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not declared.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, X., Chen, T., Zhou, J. et al. Racial and ethnic differences in restarting antiplatelet therapy in patients with primary intracranial hemorrhage: a systematic review and meta-analysis. BMC Neurol 24, 280 (2024). https://doi.org/10.1186/s12883-024-03790-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-024-03790-1