
Abstract
Spontaneous intracerebral hemorrhage (SICH) remains a devastating form of stroke. Prior use of antiplatelets or warfarin before SICH is associated with poor outcomes, but the effects of direct oral anticoagulants (DOACs) remain unclear. This study aimed to clarify trends in prior antithrombotic use and to assess the associations between prior use of antithrombotics and in-hospital mortality using a multicenter prospective registry in Japan. In total, 1085 patients were analyzed. Prior antithrombotic medication included antiplatelets in 14.2%, oral anticoagulants in 8.1%, and both in 1.8%. Prior warfarin use was significantly associated with in-hospital mortality (odds ratio [OR] 5.50, 95% confidence interval [CI] 1.30–23.26, P < 0.05) compared to no prior antithrombotic use. No such association was evident between prior DOAC use and no prior antithrombotic use (OR 1.34, 95% CI 0.44–4.05, P = 0.606). Concomitant use of antiplatelets and warfarin further increased the in-hospital mortality rate (37.5%) compared to warfarin alone (17.2%), but no such association was found for antiplatelets plus DOACs (8.3%) compared to DOACs alone (11.9%). Prior use of warfarin remains an independent risk factor for in-hospital mortality after SICH in the era of DOACs. Further strategies are warranted to reduce SICH among patients receiving oral anticoagulants and to prevent serious outcomes.
Similar content being viewed by others


Introduction
Spontaneous intracerebral hemorrhage (SICH) is a devastating disorder of the central nervous system with high morbidity and mortality1,2. In contrast to the development of hyperacute treatments for ischemic stroke, scientifically proven treatments for acute-stage SICH are still lacking. Population-based epidemiological data have shown decreasing SICH incidence in high-income countries and increasing SICH incidence in low- to middle-income countries over the last four decades3. However, the Framingham Heart Study showed continued increases in ICH incidence, particularly among patients ≥ 75 years old4. The higher incidence of SICH among elderly patients is probably due to the higher prevalence of hypertension, amyloid angiopathy, and the use of antithrombotic (AT) medications2,4,5. Data from the Japanese Hisayama study demonstrated that the incidence of ICH declined significantly from the first cohort (1961–1974) to the second cohort (1974–1987), although no such trend was found in the third cohort (1988–2001), and the incidence of ICH among patients ≥ 80 years old increased constantly over time6. Japan is a super-aging country, and individuals using AT medications for the primary or secondary prevention of cardiovascular disease and ischemic stroke are increasing. Further, patients prescribed direct oral anticoagulants (DOACs) as an alternative to warfarin have been increasing since 2011, when these DOACs first became available7,8. These practical changes in AT medication use may influence bleeding complications such as SICH, but such data remain scarce in Japan. We therefore investigated current trends in prior AT use with SICH and its effects on in-hospital mortality in the DOAC era.
Methods
Study design
The Juntendo registry of spontaneous IntraCerebral Hemorrhage (J-ICH registry) is an observational, multicenter, prospective registry of patients with SICH. Patient enrollment ran from September 1, 2016, to December 31, 2019 at 5 stroke centers located in Tokyo or neighboring regions in Japan. We obtained informed consent from all participants and combined this data with a retrospective study of SICH for patients from whom consent could not be obtained due to disease severity and/or a lack of legal representatives, with an opt-out option. We enrolled patients with SICH who were ≥ 20 years old and with onset ≤ 7 days prior, excluding patients with bleeding due to arteriovenous malformations, brain tumors, blood disorders (e.g., coagulopathy, thrombocytopenia, leukemia), severe liver dysfunction, or collagen diseases. We collected clinical information from medical records such as age, sex, body mass index (BMI), vascular risk factors, prior AT medication, stroke severity (National Institutes of Health Stroke Scale, NIHSS), modified Rankin Scale (mRS) and mortality at discharge. We measured hematoma volume (HV) and collected information on intraventricular hemorrhage (IVH), hematoma growth (HG), use of reversal agent (vitamin K2, prothrombin complex concentrate [PCC], fresh frozen plasma [FFP], idarucizumab) and surgical treatment. HV was assessed using the ABC/2 method9, and HG was defined as a > 33% or > 6-ml increase relative to baseline hematoma volume within 72 h10. We investigated short-term outcomes such as in-hospital mortality and poor outcome (mRS 5-6) at discharge. We then analyzed associations between prior AT use and these outcomes.
Statistical analysis
Continuous variables were compared using either Student’s t-test or the Mann–Whitney U test, and analysis of variance (ANOVA) or the Kruskal–Wallis test were used for comparisons between three or more groups, as appropriate, after testing for the normality of distributions. Frequencies of categorical variables were compared using the χ2 test. Multivariate logistic regression analysis was performed to assess the risks of mortality and poor outcomes during hospitalization, adjusting for clinical variables identified by univariate analysis as showing significant or marginally significant (0.05 ≤ P < 0.10) differences between the presence or absence of each outcome. All analyses were performed using JMP version 14.2.0 software (SAS Institute Inc., Cary, NC, USA). Values of P < 0.05 were considered significant.
The ethics review committee at Juntendo University School of Medicine and the relevant ethics committees at all participating sites approved this study. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research involving Human Subjects by the Ministry of Health, Labor, and Welfare of Japan.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study. We also combined retrospective data on SICH for patients from whom consent could not be obtained due to disease severity and/or a lack of legal representatives, with an opt-out option.
Result
Baseline characteristics and prior antithrombotic medication in SICH
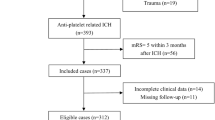
A total of 1102 cases of SICH were enrolled. After excluding cases lacking information on prior AT usage, 1085 patients were included for analysis (Fig. 1, Table 1). Among these 1085 enrolled patients, data were obtained retrospectively for only 24 patients (2.2%). Median age (interquartile range: IQR) was 71 years (60–80), and 598 patients (55.1%) were male. Hypertension was the highest vascular risk factor (69.5%), and atrial fibrillation (AF) was present in 8.6%. Previous ischemic stroke was observed in 9.8%, and coronary artery disease (angina pectoris or myocardial infarction) in 5.6%. Median time (IQR) from onset to arrival was 2 h (1–5), and median NIHSS score (IQR) on arrival was 10 (4–18). AT use before SICH was found in 262 patients (24.1%), comprising antiplatelet (AP) use in 154 (14.2%), oral anticoagulant (OAC) use in 88 (8.1%), and use of both AP and OAC (AP + OAC) in 20 (1.8%). The frequency of each prior AT use increased in an age-dependent manner and 35.5% of patients ≥ 75 years old had received some form of AT (Fig. 1). Among patients receiving AP before SICH, aspirin (58.6%) was the most frequent, and dual AP therapy (DAPT) was used in 26 (14.9%) (Supplemental Table 1). Among those receiving OACs, DOACs (65.7%) were used almost twice as often as warfarin (34.3%) (Fig. 2). Among patients receiving DOACs, dabigatran was the least used (4.2%), followed by edoxaban (28.2%), apixaban (29.6%), and rivaroxaban (38.0%), respectively (Fig. 2).

Flowchart of patient selection in the current study.

Prior use of antithrombotic (AT) medications in SICH. (A) Age-dependent prevalence of each AT medication. (B) Prior use of oral anti-coagulant (DOAC vs warfarin). (C) Prior use of DOAC subtypes. AP: antiplatelet; DOAC: direct oral anticoagulant; OAC: oral anticoagulant; SICH: spontaneous intracerebral hemorrhage.
Characteristics of hematoma and acute treatment
Median HV (IQR) was 13.5 ml (5–30), IVH was found in 393 (36.2%), and HG within 72 h was found in 45 (4.1%) (Table 1). The most prevalent hematoma location was the supratentorial deep (62.3%), followed by the lobes (23.5%), and cerebellum/brainstem (13.2%) (Table 1). When more details of hematoma location were categorized into age strata (< 55, 55–64, 65–74, or ≥ 75 years old), the putamen was the most frequent for patients < 55 years old, while the thalamus and lobar locations were the most frequent for those ≥ 75 years old (Supplemental Table 2). Hematoma evacuation was performed in 144 (13.2%), followed by endoscopy-guided aspiration in 97 (8.9%), and external ventricular drainage in 70 (6.5%). A reversal agent (prothrombin complex concentrate (PCC), fresh frozen plasma (FFP), idarucizumab) was used in 13 patients (12.0%) with prior OAC. Details of the reversal agents used are described in Supplemental Table 3.
Comparison of clinical and outcome features with or without prior AT use
We compared baseline characteristics, status of hematoma, and outcomes by each type of prior AT: no prior antithrombotic therapy (no ATT, n = 823); prior use of AP (n = 154); DOAC (n = 71); or warfarin (n = 37), respectively (Table 1). Patients with prior AT use were older and showed a higher prevalence of vascular risk factors and histories of ischemic stroke and coronary artery disease. Atrial fibrillation (AF) was significantly more frequent among patients with DOACs (81.7%) and warfarin (62.2%). Median HV tended to be greater in patients receiving AT, but the difference was not significant (P = 0.055). HG was highest in patients with warfarin (16.2%), followed by those with DOACs (11.3%), no ATT (3.3%), and AP (2.6%, P < 0.0001). Details of differences in hematoma location by each AT are also shown in Supplemental Table 2. The prevalence of lobar hemorrhage was highest with DOACs (32.4%), and the prevalence of cerebellar hemorrhage was highest with warfarin (13.5%). In-hospital mortality was highest in patients with warfarin (21.6%) followed by AP (13.6%), DOACs (11.3%), and no ATT (5.2%, P < 0.0001). A similar trend was observed in hospital deaths within 24 h (8.1% vs 5.8% vs 1.4% vs 1.5%, P < 0.001) and poor outcome (modified Rankin Scale (mRS) 5–6) at discharge (40.5% vs 31.8% vs 22.5% vs 14.7%, P < 0.0001), respectively. No significant differences were identified in clinical background, hematoma location, hematoma characteristics, and outcomes by each type of DOAC (Supplemental Table 4).
Risk of in-hospital mortality and poor outcome by prior antithrombotic use
We compared the risk of in-hospital mortality and poor outcome in patients with each prior use of AT compared to no ATT (Table 2). The risk of in-hospital mortality was significant for all types of AT compared to no ATT (odds ratio [OR] for AP 2.86, 95% confidence interval [CI] 1.64–4.98, OR for DOAC 2.30, 95% CI 1.04–5.11; OR for warfarin 5.00, 95% CI 2.16–11.6). After adjusting for covariate (Supplemental Table 5), including pre-stroke mRS, surgical treatment and use of reversal agents, only warfarin remained significantly associated with in-hospital mortality (adjusted OR [aOR] 5.50, 95% CI 1.30–23.26, P < 0.05) compared to no ATT. A similar trend was observed for hospital deaths within 24 h and poor outcomes at discharge, but the significance of these findings disappeared after adjusting for confounders.
Among the 25 patients with warfarin use and a prothrombin time international normalized ratio (PT-INR) ≥ 2, five patients (20.0%) received prothrombin complex concentrate (PCC), and 1 (4%) received fresh frozen plasma (FFP). No significant differences in HG or in-hospital mortality were seen between patients with and without treatment (33.3% vs 10.5% for HG, 16.7% vs 15.8% for in-hospital mortality, respectively). In patients with DOAC, only 4 patients (5.6%) received a reversal agent (one received idarucizumab, two received PCC, and one received FFP; Supplemental Table 3). Use of a reversal agent was not associated with any change in outcomes (data not shown).
Comparison of fatal cases within or after 24 h from hospitalization
To determine the impact on mortality of each AT medication after SICH, we compared clinical and hematological characteristics and hematoma location of patients who died within or more than 24 h from hospitalization (Table 3). Among patients who died within 24 h, all cases showed very severe neurological impairment (NIHSS score), and a large HV except in one case with prior DOAC use. Only one patient with prior DOAC use died in this group showed small HV (18 ml), but hematoma was located in brainstem.
Among patients who died more than 24 h after hospitalization, median age was higher in patients with any AT use than in no ATT. Grade of neurological severity and HV were still high, but milder than in cases who died within 24 h. The rate of HG was much higher in case with prior use of warfarin (60%) compared to use of DOACs (28.6%), no ATT (16.1%), and AP (8.3%).
Comparison of in-hospital mortality and poor outcome with combination of antiplatelet and oral anticoagulant
Finally, we compared the poor outcome (mRS5-6 at discharge) and in-hospital mortality with or without concomitant use of an antiplatelet among patients receiving an OAC (Fig. 3). Significant differences in rates of in-hospital mortality and poor outcome were evident among each group (P < 0.0001), and the AP + warfarin showed higher rates of in-hospital mortality and poor outcome than no ATT (37.5% vs 5.2%, and 62.5% vs 14.7%, respectively). The rate of in-hospital mortality and poor outcome was higher in AP + Warfarin than warfarin alone (37.5% vs 17.2% for in-hospital mortality, 62.5% vs 34.5 for poor outcome, respectively), but no such trend was observed between AP + DOAC and DOAC alone (8.3% vs 11.9% for in-hospital mortality, 25.0% vs 22.0% for poor outcome, respectively). When comparing several clinical background factors, hematoma location/characteristics, and treatment provided (OAC alone or OAC with concomitant use of AP) (Table 4), we did not find any significant differences in age, sex, rate of pre-stroke mRS ≥ 3, hematoma location/characteristics, or treatment provided in patients receiving DOACs. However, a tendency toward higher HV and a significantly higher rate of IVH were observed in patients receiving AP + warfarin compared to those on warfarin alone. Patients who received any surgery or a reversal agent were also more frequent among patients receiving AP + warfarin than among those on warfarin alone.

Association between prior antithrombotic medication and in-hospital mortality and functional outcome (mRS5-6) at discharge after SICH, dense bar: mRS6, light bar: mRS5.
Discussion
This multicenter registered study identified trends in AT use before SICH and revealed prior use of warfarin, but not of AP or DOACs, offered an independent risk factor for in-hospital mortality compared to no prior AT use. Further, patients with concomitant use of warfarin and antiplatelets showed a higher rate of in-hospital mortality and poor outcome than patients with no AT use or other combination AT use.
Before DOACs became available, three Japanese retrospective studies of SICH showed prior AP use in 17.9–20.2%, OAC (warfarin) use in 2.6–6.7%, and AP + OAC use in 1.5–2.8%11,12,13. A larger nationwide population-based cohort study in Taiwan14 showed lower prior AP use (12.0%), and OAC use (1.9%) than in Japanese studies. Meanwhile, investigations from Western countries (Italy, The Netherlands, Germany, and the United States) in the same periods15,16,17,18 showed much higher prevalence for prior use of both AP (25.1–25.6%) and OAC (8.8–25.8%) than East Asia. This may be due to the higher frequency of cardiovascular disease or AF in Western countries than in East Asia19,20,21.
Since DOACs became available, the prevalence of AT use has been changing. Similar to our data, three studies from Japan and Korea have shown much higher use of prior OACs (10.4–13.2%) after DOACs became available22,23,24, while a larger-scale investigation from August 2015 to July 2019 in China still showed a low prevalence of OAC use (1.9%)25. Trends in prior use of both AP (24.3–28.2%) and OAC (14.1–21.9%) seemed comparable to data from the United States and Europe between before and after DOACs became available26,27,28.
The incidence of ICH with prior OAC use (OAC-ICH) increased from 0.8 per 100,000 in 1988 to 4.4 per 100,000 in 1999, before DOACs became available in the United States18. However, two recent studies from Denmark and the Netherlands showed that the incidence of OAC-ICH was decreasing from before and after DOACs became available (33 or 10.5 per 100,000 person-years to 24 or 7.7 per 100,000 person-years, respectively)29,30. These findings may reflect DOACs having about a 50% lower risk of intracranial bleeding compared to warfarin in patients with AF31. A key question is whether similar trends will be observed in East Asians, which have about double the incidence of SICH compared to other ethnicities2, but no such longitudinal studies have yet been undertaken.
The rate of prior OAC use comprised about two-thirds DOACs in our study. Several previous studies have shown higher rates of warfarin than DOACs among prior users of OACs in SICH24,26,27,28,29, but a more recent report demonstrated a similar or higher rate of DOAC use compared to warfarin use32. Because real-world Japanese data indicated that the use of OACs was increasing and DOACs were rapidly replacing warfarin in patients with non-valvular atrial fibrillation7, these situations might result in an increment in the rate of prior DOAC users in Japanese SICH. Indeed, a prospective Japanese multi-stroke center cohort (the PASTA registry) that enrolled acute stroke patients receiving prior OAC from April 2016 to September 2019 showed a similar rate of prior OAC use in SICH (DOACs 73% vs warfarin 27%)33.
Although prior AP or warfarin use was associated with mortality and poor outcome in patients with SICH34,35, the impact of prior DOAC use on in-hospital mortality remains inconclusive36,37. A nationwide, cross-sectional Japanese analysis showed that prior use of DOAC (DOAC-ICH) was associated with significantly lower in-hospital mortality than prior use of warfarin (vitamin k antagonist (VKA)-ICH)) in SICH38. The rate of in-hospital mortality for DOAC-ICH was significantly lower than that for VKA-ICH at both 1 day and discharge (2.6% vs 6.5% at 1 day, and 17.6% vs 25.3% at discharge, respectively). Similar trends between DOAC-ICH and VKA-ICH were found in our results (1.4% vs 8.1% at 1 day and 11.3% vs 21.6% at discharge). Recent reports from Japan and Korea have also shown a lower rate of mortality in DOAC-ICH than in VKA-ICH24,39. These data may imply the greater safety of DOACs compared to warfarin for thromboembolic prevention in patients with a high risk of ICH. Compared to those studies from East Asia, higher rates of in-hospital mortality from SICH were reported both in DOAC-ICH (26.5–63.1%) and in VKA-ICH (32.6–62.7%) from the United States and European countries26,27,40,41. The reasons of different rates of in-hospital mortality are not known between different regions, but treatment strategies including surgery or early referral to stroke unit might influence the case fatality2. Although one meta-analysis showed that VKA-ICH was significantly associated with higher in-hospital mortality as well as larger hematoma volume, and enlargement of hematoma compared to cases of SICH with no anticoagulant35, no such relationship was noted between prior use of DOAC and no prior use of OAC due to an insufficient number of studies. Several meta-analyses have compared outcomes between VKA-ICH and DOAC-ICH, yielding inconclusive result42,43,44, but data assessments of outcomes among patients with prior AT use compared to control (no prior AT) have remained scarce. Only one single center analysis from Amsterdam reported the risk of mortality and poor outcome with prior use of VKA compared to no prior AT medication27. Our data showed that the mortality rate within 24 h from hospitalization was lower in no ATT and DOAC-ICH (1.5% and 1.4%) than in AP or VKA-ICH (5.8% and 8.1%). This might have affected the lower total mortality rate in DOAC-ICH. Much larger HV and greater neurological severity might be associate with hyperacute fatality among this group, but HV was small (18 ml) in a case with DOAC-ICH in this study. In patients who died after more than 24 h, HG might play an important role for mortality in addition to baseline HV and neurological severity, especially in cases with VKA-ICH. In this regard, a larger study comparing hematological characteristics between DOAC-ICH and VKA-ICH is warranted.
Use of a reversal agent may improve outcomes for patients with VKA-ICH 45, but only 24% of patients with VKA-ICH and PT-INR ≥ 2 used a reversal agent such as PCC or FFP in this study. We could not find significant differences in hematoma growth or in-hospital mortality between groups with and without use of a reversal agent (data not shown), but the lower total use of reversal agents among patients receiving warfarin might have affected the study outcomes. In DOAC-ICH, only four patients (5.6%) received a reversal agent (two with PCC, one with FFP, and one with idarucizumab, respectively). The reversal agent for factor Xa inhibitors (andexanet alfa) had not been available during the study periods in Japan. A recent meta-analysis showed the mortality rate of DOAC-related bleeding was higher in patients with intracranial bleeding than in those with extracranial bleeding, and effective hemostasis was significantly associated with lower risk of death46. The efficacy and safety of specific reversal agents to DOAC (idarucizumab and andexanet alfa) compared to a non-specific traditional reversal agent (FFP or PCC) remains inconclusive in DOAC-ICH47. Thus, further studies are warranted to determine the net clinical benefits of reversal agents and to clarify which reversal agents are most beneficial for DOAC-ICH.
Our results also showed that concomitant use of AP and warfarin was associated with much higher in-hospital mortality than warfarin alone after SICH, while no such association was observed among patients on DOACs. Dual antithrombotic therapy (DAT) with warfarin (warfarin plus single antiplatelet) has been shown to increase the risk of intracranial bleeding to three times that with warfarin alone in elderly AF patients48. One meta-analysis that compared safety and efficacy of either DAT with DOAC or with warfarin in patients with AF undergoing percutaneous coronary intervention (PCI) showed that the risk of major bleeding was significantly lower in DAT with DOAC than with warfarin (risk ratio 0.59, 95% CI 0.49–0.71), and without any increase in cardiovascular events49. Thus, DAT with DOACs could be beneficial to reduce the risk of SICH compared to DAT with warfarin. A nationwide study from the United States with a large number of cases showed that in-hospital mortality was significantly higher with prior use of both warfarin (aOR 1.62, 97.5% CI, 1.53–1.71) and DOAC (aOR 1.21, 97.5% CI 1.11–1.32) compared to no prior use of OAC in SICH, and DOAC-ICH showed a lower risk of in-hospital mortality than VKA-ICH (aOR 0.75, 97.5% CI 0.69–0.81)26. Concomitant use of an antiplatelet significantly increased the risk of in-hospital mortality in VKA-ICH compared to warfarin alone, but the same trend was not found among patients with DOAC-ICH26. A recent sub-analysis of the PASTA registry also demonstrated that prior use of the combination of warfarin and antiplatelet was significantly associated with in-hospital mortality compared to DOAC monotherapy (OR 20.57, 95% CI 1.75-241.75) in patients with SICH39. Because of the limited number of enrolled patients and lower statistical power, we could not confirm an independent association between DAT with warfarin and in-hospital morality compared to no prior AT use in this study. However, in-hospital mortality was about 7 times higher in VKA-ICH with antiplatelet compared to no prior AT use (37.5% vs 5.2%). The larger HV and higher rate of intraventricular hemorrhage in AP + Warfarin probably increased the risk of in-hospital mortality compared to warfarin alone, but no such effect was not found in groups with DOAC-ICH. We did not collect the time of last DOAC intake before ICH in this study. The association between blood concentration of DOAC and outcome remained unclear for DOAC-ICH. Cerebellar hemorrhage may also increase the risk of in-hospital mortality by compressing the brainstem or increasing the risk of hydrocephalus. The prevalence of cerebellar hemorrhage was highest in AP + warfarin (25.0%), but none of those patients had died by discharge in this study.
DAT with warfarin represents a significant risk for SICH and following high in-hospital mortality, as demonstrated by the current and previous studies. Thus, when physicians use ATs, monotherapy with DOAC should be considered favorably. If patients need to be treated by DAT, warfarin should not be the first choice. Usage of non-pharmacological devices such as left atrial appendage closure will also be beneficial in patients with AF who have to use DAT with warfarin to reduce the risk of SICH50.
Several limitations should be considered. First, this was a prospective study with some retrospective data using a multi-center registry, but not all patients were enrolled. These issues may have introduced selection biases. Second, the number of patients with prior use of OACs, particularly warfarin, was very small. However, a post hoc power calculation found relatively sufficient statistical power (81%) for in-hospital mortality among patients with prior use of warfarin compared to no prior AT use. Third, information on the timing of last intake of DOAC and administration of each reversal agent was unavailable, and might have influenced hematoma characteristics and outcomes. Fourth, patients receiving OACs were older, more frequently had comorbidities, and showed higher HV. These background and clinical conditions might have affected treatment decisions or the selection of aggressive treatments and subsequent care, which would have related to final outcomes. Fifth, compared to those receiving antiplatelets and DOACs, patients on warfarin might have experienced more severe comorbidities such as cardiac valvular disease, cardiac valve replacement, and several coexisting heart diseases requiring AP and warfarin. These issues were not investigated in this study and might have contributed to the prognosis in this study.
Conclusion
Among patients with Japanese SICH, a different trend was seen in prior AT use compared to before DOACs became available. In patients with prior use of OACs, DOACs were used at almost double the rate of warfarin. Prior warfarin use, but not prior use of AP or DOACs, was a significant risk for in-hospital mortality compared to no prior AT use. DAT with warfarin may further increase the risk of in-hospital mortality after SICH.
Data availability
The datasets used and/or analyzed in the current study are available from the corresponding author on reasonable request.
Abbreviations
- AF:
-
Atrial fibrillation
- aOR:
-
Adjusted odds ratio
- AP:
-
Antiplatelet
- AT:
-
Antithrombotic
- ATT:
-
Antithrombotic therapy
- BMI:
-
Body mass index
- DAT:
-
Dual antithrombotic therapy
- DOAC:
-
Direct oral anticoagulant
- FFP:
-
Fresh frozen plasma
- HG:
-
Hematoma growth
- HV:
-
Hematoma volume
- ICH:
-
Intracerebral hemorrhage
- IVH:
-
Intraventricular hemorrhage
- MI:
-
Myocardial infarction
- mRS:
-
Modified Rankin Scale
- NIHSS:
-
National Institutes of Health Stroke Scale
- OAC:
-
Oral anticoagulant
- PCC:
-
Prothrombin complex concentrate
- PT-INR:
-
Prothrombin time international normalized ratio
- SICH:
-
Spontaneous intracerebral hemorrhage
- VKA:
-
Vitamin K antagonist
References
Sacco, S., Marini, C., Toni, D., Olivieri, L. & Carolei, A. Incidence and 10-year survival of intracerebral hemorrhage in a population-based registry. Stroke 40, 394–399 (2009).
van Asch, C. J. et al. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: A systematic review and meta-analysis. Lancet Neurol. 9, 167–176 (2010).
Feigin, V. L., Lawes, C. M., Bennett, D. A., Barker-Collo, S. L. & Parag, V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: A systematic review. Lancet Neurol. 8, 355–369 (2009).
Lioutas, V. A. et al. Assessment of incidence and risk factors of intracerebral hemorrhage among participants in the Framingham Heart Study between 1948 and 2016. JAMA Neurol. 77, 1252–1260 (2020).
Lovelock, C. E., Molyneux, A. J. & Rothwell, P. M. Change in incidence and aetiology of intracerebral haemorrhage in Oxfordshire, UK, between 1981 and 2006: A population-based study. Lancet Neurol. 6, 487–493 (2007).
Gotoh, S. et al. Trends in the incidence and survival of intracerebral hemorrhage by its location in a Japanese community. Circ. J. 78, 403–409 (2014).
Akao, M. et al. 10-year trends of antithrombotic therapy status and outcomes in japanese atrial fibrillation patients—The Fushimi AF Registry. Circ. J. 86, 726–736 (2022).
Miyazaki, S. et al. Trends of anticoagulant use and outcomes of patients with non-valvular atrial fibrillation: Findings from the RAFFINE registry. J. Cardiol. 80, 41–48 (2022).
Kothari, R. U. et al. The ABCs of measuring intracerebral hemorrhage volumes. Stroke. 27, 1304–1305 (1996).
Demchuk, A. M. et al. Prediction of haematoma growth and outcome in patients with intracerebral haemorrhage using the CT-angiography spot sign (PREDICT): A prospective observational study. Lancet Neurol. 11, 307–314 (2012).
Toyoda, K. et al. Antithrombotic therapy and predilection for cerebellar hemorrhage. Cerebrovasc. Dis. 23, 109–116 (2007).
Toyoda, K. et al. Antithrombotic therapy influences location, enlargement, and mortality from intracerebral hemorrhage. The Bleeding with Antithrombotic Therapy (BAT) Retrospective Study. Cerebrovasc. Dis. 27, 151–159 (2009).
Yamashita, S., Kimura, K., Iguchi, Y. & Shibazaki, K. Prior oral antithrombotic therapy is associated with early death in patients with supratentorial intracerebral hemorrhage. Intern. Med. 50, 413–419 (2011).
Liu, Z. H. et al. Previous antithrombotic therapy, particularly anticoagulant, is associated with unfavorable outcomes in patients with primary spontaneous intracerebral hemorrhage receiving craniotomy: A Nationwide Population-Based Cohort Study. World Neurosurg. 128, e59–e73 (2019).
Pezzini, A. et al. Antithrombotic medications and the etiology of intracerebral hemorrhage: MUCH-Italy. Neurology. 82, 529–535 (2014).
Schols, A. M. et al. Incidence of oral anticoagulant-associated intracerebral hemorrhage in the Netherlands. Stroke. 45, 268–270 (2014).
Stein, M. et al. In-hospital mortality after pre-treatment with antiplatelet agents or oral anticoagulants and hematoma evacuation of intracerebral hematomas. J. Clin. Neurosci. 26, 42–45 (2016).
Flaherty, M. L. et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology. 68, 116–121 (2007).
Bhatt, D. L. et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 295, 180–189 (2006).
Go, A. S. et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 285, 2370–2375 (2001).
Inoue, H. et al. Prevalence of atrial fibrillation in the general population of Japan: An analysis based on periodic health examination. Int. J. Cardiol. 137, 102–107 (2009).
Suda, S. et al. Characteristics of acute spontaneous intracerebral hemorrhage in patients receiving oral anticoagulants. J. Stroke Cerebrovasc. Dis. 28, 1007–1014 (2019).
Hagii, J. et al. Characteristics of intracerebral hemorrhage during rivaroxaban treatment: Comparison with those during warfarin. Stroke. 45, 2805–2807 (2014).
Woo, H. G. et al. Intracerebral hemorrhage associated with warfarin versus non-vitamin K antagonist oral anticoagulants in Asian patients. J. Clin. Neurosci. 61, 160–165 (2019).
Liu, D. et al. Prior antithrombotic therapy is associated with increased risk of death in patients with intracerebral hemorrhage: Findings from the Chinese Stroke Center Alliance (CSCA) Study. Aging Dis. 12, 1263–1271 (2021).
Inohara, T. et al. Association of intracerebral hemorrhage among patients taking non-vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital mortality. JAMA. 319, 463–473 (2018).
Baharoglu, M. I., Coutinho, J. M., Marquering, H. A., Majoie, C. B. & Roos, Y. B. Clinical outcome in patients with intracerebral hemorrhage stratified by type of antithrombotic therapy. Front. Neurol. 12, 684476 (2021).
Roquer, J. et al. Interaction of atrial fibrillation and antithrombotics on outcome in intracerebral hemorrhage. Neurology. 93, e1820–e1829 (2019).
Hald, S. M. et al. Trends in incidence of intracerebral hemorrhage and association with antithrombotic drug use in Denmark, 2005–2018. JAMA Netw Open. 4, e218380 (2021).
Peeters, M. T., Vroman, F., Schreuder, T. A., van Oostenbrugge, R. J. & Staals, J. Decrease in incidence of oral anticoagulant-related intracerebral hemorrhage over the past decade in the Netherlands. Eur Stroke J. 7, 20–27 (2022).
López-López, J. A. et al. Oral anticoagulants for prevention of stroke in atrial fibrillation: Systematic review, network meta-analysis, and cost effectiveness analysis. BMJ. 359, j5058 (2017).
Pedersen, T. G. B. et al. Trends in the incidence and mortality of intracerebral hemorrhage, and the associated risk factors, in Denmark from 2004 to 2017. Eur. J. Neurol. 29, 168–177 (2022).
Suda, S. et al. Characteristics of ischemic versus hemorrhagic stroke in patients receiving oral anticoagulants: Results of the PASTA Study. Intern. Med. 61, 801–810 (2022).
Goeldlin, M. B. et al. Intracerebral haemorrhage volume, haematoma expansion and 3-month outcomes in patients on antiplatelets. A systematic review and meta-analysis. Eur. Stroke J. 6, 333–342 (2021).
Seiffge, D. J. et al. Meta-analysis of haematoma volume, haematoma expansion and mortality in intracerebral haemorrhage associated with oral anticoagulant use. J. Neurol. 266, 3126–3135 (2019).
Tsivgoulis, G. et al. Neuroimaging and clinical outcomes of oral anticoagulant-associated intracerebral hemorrhage. Ann. Neurol. 84, 694–704 (2018).
Tsivgoulis, G. et al. Direct oral anticoagulant- vs vitamin K antagonist-related nontraumatic intracerebral hemorrhage. Neurology. 89, 1142–1151 (2017).
Kurogi, R. et al. Comparing intracerebral hemorrhages associated with direct oral anticoagulants or warfarin. Neurology. 90, e1143–e1149 (2018).
Nomura, K. et al. Vitamin K antagonists but not non-vitamin K antagonists in addition on antiplatelet therapy should be associated with increase of hematoma volume and mortality in patients with intracerebral hemorrhage: A sub-analysis of PASTA registry study. J. Neurol. Sci. 448, 120643 (2023).
Apostolaki-Hansson, T., Ullberg, T., Norrving, B. & Petersson, J. Prognosis for intracerebral hemorrhage during ongoing oral anticoagulant treatment. Acta Neurol. Scand. 139, 415–421 (2019).
Gerner, S. T. et al. Characteristics in non-vitamin K antagonist oral anticoagulant-related intracerebral hemorrhage. Stroke. 50, 1392–1402 (2019).
Boulouis, G. et al. Outcome of intracerebral haemorrhage related to non-vitamin K antagonists oral anticoagulants versus vitamin K antagonists: A comprehensive systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry. 89, 263–270 (2018).
Wilson, D. et al. Outcome of intracerebral hemorrhage associated with different oral anticoagulants. Neurology. 88, 1693–1700 (2017).
Lioutas, V. A. et al. Clinical outcomes and neuroimaging profiles in nondisabled patients with anticoagulant-related intracerebral hemorrhage. Stroke. 49, 2309–2316 (2018).
Steiner, T. et al. Fresh frozen plasma versus prothrombin complex concentrate in patients with intracranial haemorrhage related to vitamin K antagonists (INCH): A randomised trial. Lancet Neurol. 15, 566–573 (2016).
Gómez-Outes, A. et al. Meta-analysis of reversal agents for severe bleeding associated with direct oral anticoagulants. J. Am. Coll. Cardiol. 77, 2987–3001 (2021).
Chaudhary, R. et al. Evaluation of direct oral anticoagulant reversal agents in intracranial hemorrhage: A systematic review and meta-analysis. JAMA Netw Open. 5, e2240145 (2022).
Shireman, T. I., Howard, P. A., Kresowik, T. F. & Ellerbeck, E. F. Combined anticoagulant-antiplatelet use and major bleeding events in elderly atrial fibrillation patients. Stroke. 35, 2362–2367 (2004).
Brunetti, N. D. et al. Meta-analysis study on direct oral anticoagulants vs warfarin therapy in atrial fibrillation and PCI: Dual or triple approach?. Int. J. Cardiol. Heart Vasc. 29, 100569 (2020).
Reddy, V. Y. et al. 5-year outcomes after left atrial appendage closure: From the PREVAIL and PROTECT AF trials. J. Am. Coll. Cardiol. 70, 2964–2975 (2017).
Funding
This work was partly supported by research Grants from Juntendo University and Jichi Medical University.
Author information
Authors and Affiliations
Consortia
Contributions
R.T. contributed to conception and design of the work. H.U., J.T., R.S., K.Y., S.T., M.Y., Y.U., T.Y., M.H., Y.Y., C.M., and R.T. contributed to data acquisition. H.U., K.Y., M.M., and R.T. contributed to data analysis and writing of the original draft. M.M., A.K., T.U., N.H., and H.A. contributed to review of the manuscript. All authors reviewed and approved the manuscript for submission and had final responsibility for the decision to submit for publication.
Corresponding author
Ethics declarations
Competing interests
Y.U. reports research funds from Bristol-Myers Squibb., T.Y. reports honoraria from Daiichi Sankyo, T.U. reports honoraria from Daiichi Sankyo, Boehringer Ingelheim, Otsuka Pharmaceutical, Bayer Pharmaceutical, Bristol-Myers Squibb, and Pfizer Japan Inc., N.H. reports honoraria from Boehringer Ingelheim, Bristol-Myers Squibb, Otsuka Pharmaceutical, and Daiichi Sankyo, H.A. reports research funds from Otsuka Pharmaceutical, and R.T. reports honoraria from Boehringer-Ingelheim, Bayer, Pfizer, Bristol-Myers Squibb, Daiichi Sankyo, Sanofi, Otsuka Pharmaceutical, and CSL Behring. H.U., J.T., R.S., K.Y., S.T., M.Y., M.H., Y.Y., C.M., M.M., and A.K. report no competing interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ueno, H., Tokugawa, J., Saito, R. et al. Trends in prior antithrombotic medication and risk of in-hospital mortality after spontaneous intracerebral hemorrhage: the J-ICH registry. Sci Rep 14, 12009 (2024). https://doi.org/10.1038/s41598-024-62717-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-62717-5
- Springer Nature Limited