
Abstract
Background
PE (preeclampsia) is a heterogeneous disorder with early onset PE (EOPE) and late onset PE (LOPE) subtypes. Associations between maternal miRNAs biosynthesis genes polymorphisms and risk of PE have been previously observed. However, the impact of polymorphisms in DGCR8 which is indispensable in miRNA maturing processing on the susceptibility to preeclampsia (PE) has not been elucidated yet. We, therefore, conducted a case-control study to evaluate the impact of polymorphisms in DGCR8 on the risk of EOPE and LOPE.
Methods
A total of 66 patients diagnosed with EOPE, 206 with LOPE and 330 healthy controls were recruited. Five SNPs in DGCR8 were genotyped including rs1558496, rs1640299, rs720012, rs720014, and rs9606241. Logistic regression was used to estimate the OR and the 95% CI for the associations.
Results
Increased risk of LOPE has been observed among patients with rs1640299 TG genotype (OR = 1.98 (95%CI: 1.38, 2.87), p = 2.32e-4) and rs720014 TC genotype (OR = 2.49 (95%CI: 1.72, 3.60), p = 1.40e-7). The DGCR8 rs1558496/ rs1640299/ rs720012/ rs720014/ rs9606241 haplotype T-G-A-C-A and T-G-A-C-G were associated with increased risk of LOPE (OR = 2.20 (95%CI: 1.49, 3.25), p = 5.90e-5, and 1.58 (95%CI: 1.06, 2.36), p = 0.024, respectively). And the haplotype T-T-G-T-A was associated with lower risk of LOPE (OR = 0.74 (95%CI: 0.58, 0.95), p = 0.018). These significant associations retained after false-positive discovery rate correction. However, none of the tested SNPs or haplotypes in DGCR8 gene is associated with risk of EOPE (p > 0.05).
Conclusions
Polymorphisms in DGCR8 might participate in the pathological process of preeclampsia. The rs1640299 T > G and rs720014 T > C polymorphisms are associated with late onset preeclampsia susceptibility.
Similar content being viewed by others


Introduction
PE (preeclampsia) complicates 2–5% of pregnancies and is a major cause of maternal, fetal, and neonatal morbidity and mortality [1]. Furthermore, PE could increase the risk of long-term cardiovascular diseases of both mothers and their offspring [2, 3]. Though efforts have been made, the exact etiology for PE is still unclear.
MicroRNAs (miRNAs) have been proposed to regulate the stability of mRNAs that encode proteins involved in maintaining various normal physiological processes [4]. The biosynthesis of miRNAs is a tightly regulated multistep process. Single nucleotide polymorphisms (SNPs) within those miRNAs biosynthesis genes can result in altered miRNAs expression and subsequently being associated with risks of some diseases [5,6,7]. A recent study conducted in Iran has also observed the association between SNPs within maternal miRNAs biosynthesis genes and risk of PE [8].
DiGeorge critical region 8 (DGCR8) is an RNA binding protein which interacts with Drosha to produce pre-microRNA in the nucleus and is indispensable in miRNA maturing processing [9]. DGCR8 also referred to as Pasha, could stabilize Drosha via protein- protein interaction, and take charge of recognizing ssRNA and dsRNA structures [10]. SNPs within the DGCR8 are associated with schizophrenia [11], primary open angle glaucoma [12] and various cancers [13,14,15]. However, the impact of polymorphisms in DGCR8 on the susceptibility to PE has not been elucidated.
Moreover, PE is a heterogeneous disorder with 2 distinct subtypes: in most PE cases, the clinical features first come into view at or after 34 weeks of gestation called late onset PE (LOPE), and about 10% of cases showed the symptoms before 34 weeks of gestation called early onset PE (EOPE) [16]. Heterogeneous phenotypes in PE were resulted from different pathophysiological mechanisms [17, 18]. Decreased spiral artery remodeling and poor placentation are involved in EOPE. On the other hand, LOPE seems to be the manifestation of a mismatch between the metabolic demands of the growing fetus and maternal supply [17, 18]. Recent studies also found that different genetic predisposition also existed between LOPE and EOPE [19, 20]. We, therefore, have genotyped 5 SNPs in DGCR8 including rs1558496, rs1640299, rs720012, rs720014, and rs9606241 in a case-control study to evaluate the impact of these genes polymorphisms on the risk of EOPE and LOPE.
Methods
Study design
A case-control study that included 66 EOPE, 206 LOPE and 330 controls was conducted between Mar 2016 and Dec2017 at two hospitals in Hunan province of China (the Liuyang Municipal Hospital of Maternal and Child Health (LYMHMCH), and the Third Xiangya Hospital of Central South University (TXYHCSU)). The inclusion criteria for participants have been depicted in our previous study [21]. In brief, cases were clinical diagnosed PE patients combined with absence of diabetes mellitus, renal disease, or chronic cardiovascular diseases. All the controls were confirmed with normal blood pressure during pregnancy and with no history of aforementioned chronic diseases.
Clinical definitions
The diagnostic criteria for PE was de novo hypertension (≥140/90 mmHg) after 20 weeks of gestation accompanied with proteinuria (≥ 1+ on dipstick), or without proteinuria but showed one or more of the following symptoms: thrombocytopenia, impaired liver function, de novo renal insufficiency, pulmonary edema, cerebral or visual disturbance. PE was further classified as EOPE (diagnosed before 34 weeks of gestation), or LOPE (diagnosed at or after 34 weeks of gestation).
Information collection and genotyping
The study protocol was approved by Ethical Review Committee of the Central South University and IRB (institutional review boards) from LYMHMCH. Written informed consent was obtained from all participants. A self-administered questionnaire was used to collect demographic, reproductive and medical history within two days before or after delivery. Meanwhile, 5 ml of venous blood sample from each participant was collected and processed for genomic DNA extraction with the TIANamp blood DNA kit (DP318–03, TIANGEN, Beijing) within 24 h. Information on maternal complications was abstracted from the medical records. Five candidate SNPs in DGCR8 were selected and genotyped with the SEQUENOM MassARRAY iPLEX platform, including rs1558496, rs1640299, rs720012, rs720014, and rs9606241. Information on location and potential functions of selected SNPs were listed in Additional file 1: Table S1.
Statistical analysis
χ2 test was conducted for comparison on maternal characteristics between EOPE, LOPE and control groups. The χ2 partition method (α’ = α/ (3*(3–1)/2) + 1) =0.0125) was used for further comparison between each of the two groups. Hardy-Weinberg equilibrium was detected in control group. The risk of LOPE and EOPE associated with genotypes or haplotype frequencies was calculated as the odds ratio (OR) with 95% confidence interval (95%CI) by unconditional logistic regression model. The false-positive discovery rate (FDR) correction was adopted to adjust multiple comparison tests. Two-tailed p values < 0.05 were considered statistically significant. Statistical analyses were performed with SAS software, version 9.2 (SAS Institute, Inc., Cary, NC). The impact of these selected SNPs on the expression of the proteins was further evaluated through Ensembl’s Variant Effect Predictor (VEP) tool (http://grch37.ensembl.org/info/docs/tools/vep/index.html).
Results
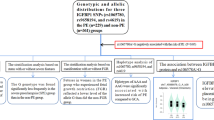
General information on enrolled cases and controls were all listed in Table 1. Both EOPE and LOPE cases were older than controls. Compared to LOPE cases and controls, the EOPE cases were more likely to be nulliparous and exposure to active and/or passive smoking during pregnancy. And LOPE cases had higher risk of GDM than EOPE and controls. No significant differences in the distribution of maternal education, or fetal gender were found between EOPE, LOPE and controls.
The genotyping completion rates were 100% for all SNPs. All of the selected genes have showed polymorphisms and observed with HWE in the control group. Results from VEP showed that all of the 5 selected SNPs had a predicted ‘modifier’ impact (Additional file 1: Table S1).Table 2 showed the odds ratios for 5 selected SNPs and PE subtypes. After the FDR correction, increased risk of LOPE has been still observed among patients with rs1640299 TG genotype (OR = 1.98 (95%CI: 1.38, 2.87), p = 2.32e-4) and rs720014 TC genotype (OR = 2.49 (95%CI: 1.72, 3.60), p = 1.40e-7). However, none of the tested SNPs was associated with risk of EOPE (p > 0.05). Compared with controls, though the frequencies of rs720012 AA genotype were higher in LOPE group, this association became insignificant after FDR correction (p = 0.067).
The associations between possible haplotypes and risk of EOPE and LOPE were estimated and listed in Table 3. The DGCR8 rs1558496/ rs1640299/ rs720012/ rs720014/ rs9606241 haplotype T-G-A-C-A and T-G-A-C-G were significantly associated with increased risk of LOPE (OR = 2.20 (95%CI: 1.49, 3.25) and 1.58 (95%CI: 1.06, 2.36), respectively). However, the haplotype T-T-G-T-A was associated with lower risk of LOPE (OR = 0.74 (95%CI: 0.58, 0.95)). Those associations retained after FDR correction (p < 0.05).
Discussion
In our study, we have evaluated five SNPs (rs1558496, rs1640299, rs720012, rs720014 and rs9606241) of the DGCR8 gene with the risk of EOPE and LOPE in Han-Chinese population. The results showed that rs1640299 genotype TG and rs720014 genotype TC were associated with increased risk of LOPE. DGCR8 haplotypes are also significantly associated with risk of LOPE. However, none of the tested SNPs or haplotypes in DGCR8 gene is associated with risk of EOPE.
Generation of pre-miRNAs from the longer pri-miRNAs by the microprocessor is the first step of miRNAs maturation [9]. As a key component of microprocessor, DGCR8 takes charge of stabilizing Drosha via protein- protein interaction, recognizing the pri-miRNA at the ssRNA-dsRNA junction and directing Drosha to a specific cleavage site [10]. It is indispensable for miRNAs biogenesis. Emerging evidence has supported that the genetic variations within DGCR8 were associated with various diseases [11,12,13,14,15]. The polymorphism in rs1640299 was reported to be associated with risk of laryngeal cancer [13] and bladder cancer [14], and could increase the effect of black carbon pollutant exposures on blood pressure (BP) [22]. In our study, we also found that compared with wild genotype, the risk of LOPE among rs1640299 TG genotype carriers was increased by almost 2 fold (OR = 1.98 (95%CI: 1.38, 2.87)). Moreover, patients with rs720014 TC genotype had a 2.49 fold increased risk of LOPE (OR = 2.49 (95%CI: 1.72, 3.60)). Previous studies conducted in Caucasians also found that ovarian cancer survival [23] and radiotherapy induced pneumonitis in patients with non-small cell lung cancer [24] were significantly associated with polymorphism in rs720014, but not associated with rs720012 polymorphism which is in consist with our findings. The polymorphisms in rs1640299 and rs720014 were both located at the 3′UTR of DGCR8 which is not translated directly into the protein. However, based on the bioinformatic prediction (http://snpinfo.niehs.nih.gov/index.html), rs1640299 is located at the binding sites of miR-1256 and miR-583 in the 3′UTR of DGCR, and rs720014 is located at the binding sites of miR-106, miR-17, miR-20, miR-518, miR-770 and miR-93. Mutations on those two 3′UTR sites might lead to impairment of those miRNAs binding and thereby modify the process of miRNAs maturation and consequently may play a pivotal role in PE. Additionally, impairment of miRNAs binding could also affect mRNA stability and lead to upgraded DGCR8 expression which has been previously observed in Iranian PE patients [25]. However, the specific molecular mechanisms of those two SNPs need further experimental validation.
The impact of polymorphisms in rs9606248 and rs1558496 on susceptibility to diseases has been previously tested in breast cancer [26] and colon cancer [27]. And no significant association has been observed. Our results also suggest no significant association existing between those two SNPs and EOPE/ LOPE.
Growing evidence proved that LOPE and EOPE are two distinct phenotypes of PE, which were resulted from different pathophysiological mechanisms [17, 18]. Decreased spiral artery remodeling and poor placentation are involved in EOPE. On the other hand, LOPE seems to be the manifestation of a mismatch between the metabolic demands of the growing fetus and maternal supply [17, 18]. Recently, studies conducted in Australia and Brazilian found that maternal polymorphisms in HIF1α [19] and ACVR2A [20] genes were associated with risk of EOPE, but not with LOPE. Those findings implied that different genetic predisposition existed between LOPE and EOPE. Our study added evidence to this hypothesis: DGCR8 polymorphisms are only associated with LOPE susceptibility. The DGCR8 gene plays a central role in angiogenesis and cardiovascular function [28, 29]: deletion of DGCR8 in cardiomyocytes could lead to the increase of angiogenesis genes and left ventricular malfunction. The angiogenic/anti-angiogenic imbalance is milder in LOPE rather than in EOPE [30]. We speculated that the polymorphisms in rs1640299 and rs720014 may only cause mild angiogenic/anti-angiogenic imbalance which result different genetic predisposition observed in our study.
Strengths and limitations should be considered when interpreting the study findings. Diagnosis of EOPE/ LOPE was based on medical records not self-report, which minimized potential disease misclassification. However, the limitation should not be ignored as well. Our case control study only explores the association between SNPs in DGCR8 and EOPE/ LOPE development, not the causal relationship. And the functional study of those SNPs to the development of LOPE has not been conducted in present study. Moreover, our study was conducted among Chinese with relative small sample size. The replication of our finding in an independent population is needed.
Conclusion
Our studies confirmed that polymorphisms in DGCR8 might participate in the pathological process of preeclampsia. The rs1640299 T > G and rs720014 T > C polymorphisms are associated with late onset preeclampsia susceptibility. However, the polymorphisms in DGCR8 are not associated with risk of early onset preeclampsia. The mechanism on how those SNP modifies the susceptibility to pregnancy induced hypertension needs further research.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- DGCR8:
-
DiGeorge critical region 8
- EOPE:
-
Early onset preeclampsia
- FDR:
-
False-positive discovery rate
- GDM:
-
Gestational diabetes mellitus
- LOPE:
-
Late onset preeclampsia
- miRNA:
-
microRNA
- PE:
-
Preeclampsia
- SNPs:
-
Single nucleotide polymorphisms
- VEP:
-
Variant Effect Predictor
References
American College of Obstetricians and Gynecologists. Hypertension in pregnancy: executive summary. Obstet Gynecol. 2013;122:1122–31.
Irgens HU, Reisaeter L, Irgens LM, Lie RT. Long term mortality of mothers and fathers after pre-eclampsia: population based cohort study. Bmj. 2001;323:1213–7.
Backes CH, Markham K, Moorehead P, Cordero L, Nankervis CA, Giannone PJ. Maternal preeclampsia and neonatal outcomes. J Pregnancy. 2011;2011 214365.
Winter J, Jung S, Keller S, Gregory RI, Diederichs S. Many roads to maturity: microRNA biogenesis pathways and their regulation. Nat Cell Biol. 2009;11(3):228–34.
Song FJ, Chen KX. Single-nucleotide polymorphisms among microRNA: big effects on cancer. Chin J Cancer. 2011;30(6):381–91.
Beveridge NJ, Gardiner E, Carroll AP, Tooney PA, Cairns MJ. Schizophrenia is associated with an increase in cortical microRNA biogenesis. Mol Psychiatry. 2010;15(12):1176–89.
Zhang M, Ma H, Wang S, Shen H. Evaluation of genetic variants in microRNA biosynthesis genes and risk of breast cancer in Chinese women. Int J Cancer. 2013;133(9):2216–24.
Rezaei M, Eskandari F, Mohammadpour-Gharehbagh A, et al. The Drosha rs10719 T>C polymorphism is associated with preeclampsia susceptibility. Clin Exp Hypertens. 2018;40(5):440–5.
Lee Y, Jeon K, Lee JT, Kim S, Kim VN. MicroRNA maturation: stepwise processing and subcellular localization. EMBO J. 2002;21:4663–70.
Landthaler M, Yalcin A, Tuschl T. The human DiGeorge syndrome critical region gene 8 and its D. melanogaster homolog are required for miRNA biogenesis. Curr Biol. 2004;14:2162–7.
Zhou Y, Wang J, Lu X, et al. Evaluation of six SNPs of MicroRNA machinery genes and risk of schizophrenia. J Mol Neurosci. 2013;49(3):594–9.
Molasy M, Walczak A, Przybyłowska-Sygut K, et al. The analysis of single nucleotide polymorphisms of the DGCR8 and XPO5 genes, and their association with the incidence of primary open angle glaucoma. Klin Ocz 2016;118(2):122–132. (PMID:29912490) (DOI: https://doi.org/10.5114/ko.2016.71686).
Bruzgielewicz A, Osuch-Wójcikiewicz E, Walczak A, et al. Evaluation of polymorphisms in microRNA biosynthesis genes and risk of laryngeal cancer in the polish population. Pol J Pathol. 2016;67(3):283–90.
Ke HL, Chen M, Ye Y, et al. Genetic variations in micro-RNA biogenesis genes and clinical outcomes in non-muscle-invasive bladder cancer. Carcinogenesis. 2013;34:1006–11.
Wen J, Lv Z, Ding H, Fang X, Sun M. Association of miRNA biosynthesis genes DROSHA and DGCR8 polymorphisms with cancer susceptibility: a systematic review and meta-analysis. Biosci Rep. 2018;38:3). pii: BSR20180072.
Hutcheon JA, Lisonkova S, Joseph KS. Epidemiology of preeclampsia and the other hypertensive disorders of pregnancy. Best Pract Res Clin Obstet Gynaecol. 2011;25:391–403.
Valensise H, Vasapollo B, Gagliardi G, Novelli GP. Early and late preeclampsia: two different maternal hemodynamic states in the latent phase of the disease. Hypertension. 2008;52:873–80.
Von Dadelszen P, Magee LA, Roberts JM. Subclassification of preeclampsia. Hypertens Pregnancy. 2003;22:143–8.
Andraweera PH, Dekker GA, Thompson SD, Dissanayake VH, Jayasekara RW, Roberts CT. Hypoxia-inducible factor-1α gene polymorphisms in early and late onset preeclampsia in Sinhalese women. Placenta. 2014;35(7):491–5.
Ferreira LC, Gomes CE, Araújo AC, Bezerra PF, Duggal P, Jeronimo SM. Association between ACVR2A and early-onset preeclampsia: replication study in a northeastern Brazilian population. Placenta. 2015;36(2):186–90.
Li X, Tan H, Chen M, Zhou S. Transforming growth factor beta 1 related gene polymorphisms in gestational hypertension and preeclampsia: a case-control candidate gene association study. Pregnancy Hypertens. 2018;12:155–60.
Wilker EH, Baccarelli A, Suh H, Vokonas P, Wright RO, Schwartz J. Black carbon exposures, blood pressure, and interactions with single nucleotide polymorphisms in MicroRNA processing genes. Environ Health Perspect. 2010;118(7):943–8.
Liang D, Meyer L, Chang DW, et al. Genetic variants in MicroRNA biosynthesis pathways and binding sites modify ovarian cancer risk, survival, and treatment response. Cancer Res. 2010;70(23):9765–76.
Li R, Pu X, Chang JY, et al. MiRNA-related genetic variations associated with radiotherapy-induced toxicities in patients with locally advanced non-small cell lung Cancer. PLoS One. 2016;11(3):e0150467.
Dargahi R, Shahbazzadegan S, Naghizadeh-Baghi A, Sefati-Kooyakhi S. Expression levels of Drosha and dicer enzymes and DGCR8 protein in pre-eclamptic patients. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2018;20(12):40–9. https://doi.org/10.22038/IJOGI.2017.10429.
Yao S, Graham K, Shen J, et al. Genetic variants in microRNAs and breast cancer risk in African American and European American women. Breast Cancer Res Treat. 2013;141(3):447–59.
Mullany LE, Herrick JS, Wolff RK, Buas MF, Slattery ML. Impact of polymorphisms in microRNA biogenesis genes on colon cancer risk and microRNA expression levels: a population-based, case-control study. BMC Med Genet. 2016;9(1):21.
Chen X, Wang L, Huang R, et al. Dgcr8 deletion in the primitive heart uncovered novel microRNA regulating the balance of cardiac-vascular gene program. Protein Cell. 2019;10(5):327–46.
Rao PK, Toyama Y, Chiang HR, et al. Loss of cardiac microRNA-mediated regulation leads to dilated cardiomyopathy and heart failure. Circ Res. 2009;105(6):585–94.
Schaarschmidt W, Rana S, Stepan H. The course of angiogenic factors in early- vs. late-onset preeclampsia and HELLP syndrome. J Perinat Med. 2013;41(5):511–6.
Acknowledgements
We thank the health workers in the Liuyang Municipal Hospital of Maternal and Child Health, and the Third Xiangya Hospital of Central South University for their assisting in the fieldwork.
Funding
The study was supported by National Natural Science Foundation of China (Grant # 81872685), Natural Science Foundation of Hunan Province (Grant # 2017JJ3215), and Open Project of Key Laboratory of Environmental Pollution Monitoring and Disease Control, Guizhou Medical University (Grant #GMU-2017-HJZ-05). None of the funding that we had received plays role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
YZ and JL designed the research; XH and ZL conducted the literature review, statistical analysis, and drafted the manuscript; DW did the data interpretation and experimental work including Genomic DNA extraction and genotyping; XH participated in the data clean and statistical analysis; ZL supervised the field activities and data interpretation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was reviewed by the Ethical and Confidentiality Committee of Central-South University (Reference XYGW-2016-01, approved on 3rd Mar 2016) and institution review boards (IRB) from the Liuyang Municipal Hospital of Maternal and Child Health. Written consent has been signed by all participants. All personal information has been recoded with initials or numbers which guaranteed no information of the participants can be identified in data analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicting interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. SNPs evaluated in this study and their minor allele frequencies (MAF) in the Han-Chinese population. (DOCX 17 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Huang, X., Li, Z., Lei, J. et al. Genetic polymorphism in DGCR8 is associated with late onset of preeclampsia. BMC Med Genet 20, 151 (2019). https://doi.org/10.1186/s12881-019-0887-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12881-019-0887-7