
Abstract
Background
Initial reports of 23Na magnetic resonance imaging (MRI) date back to the 1970s. However, methodological challenges of the technique hampered its widespread adoption for many years. Recent technical developments have overcome some of these limitations and have led to more optimal conditions for 23Na-MR imaging. In order to serve as a reliable tool for the assessment of clinical stroke or brain tumor patients, we investigated the repeatability and reproducibility of cerebral sodium (23Na) imaging in healthy subjects.
Methods
In this prospective, IRB approved study 12 consecutive healthy volunteers (8 female, age 31 ± 8.3) underwent three cerebral 23Na-MRI examinations at 3.0 T (TimTrio, Siemens Healthineers) distributed between two separate visits with an 8 day interval. For each scan a T1w MP-RAGE sequence for anatomical referencing and a 3D-density-adapted, radial GRE-sequence for 23Na-imaging were acquired using a dual-tuned (23Na/1H) head-coil. On 1 day, these scans were repeated consecutively; on the other day, the scans were performed once. 23Na-sequences were reconstructed according to the MP-RAGE sequence, allowing direct cross-referencing of ROIs. Circular ROIs were placed in predetermined anatomic regions: gray and white matter (GM, WM), head of the caudate nucleus (HCN), pons, and cerebellum. External 23Na-reference phantoms were used to calculate the tissue sodium content.
Results
Excellent correlation was found between repeated measurements on the same day (r2 = 0.94), as well as on a different day (r2 = 0.86). No significant differences were found based on laterality other than in the HCN (63.1 vs. 58.7 mmol/kg WW on the right (p = 0.01)). Pronounced inter-individual differences were identified in all anatomic regions. Moderate to good correlation (0.310 to 0.701) was found between the readers.
Conclusion
Our study has shown that intra-individual 23Na-concentrations in healthy subjects do not significantly differ after repeated scans on the same day and a pre-set time interval. This confirms the repeatability and reproducibility of cerebral 23Na-imaging. However, with manual ROI placement in predetermined anatomic landmarks, fluctuations in 23Na-concentrations can be observed.
Similar content being viewed by others

Background
Initial reports of 23Na magnetic resonance imaging (MRI) date back to the 1970s [1]. However, methodological challenges of the technique – low SNR due to low in-vivo sodium concentrations and low available field strengths – hampered its widespread adoption for many years. Recent technical developments such as clinical 3 Tesla MRI, improved coils, and faster gradients have overcome some of these limitations and have led to more optimal conditions for 23Na-MR imaging. Several recent publications have demonstrated the feasibility of 23Na-MRI for in-vivo imaging of physiological conditions in the kidney [2,3,4], cartilage and musculoskeletal system [5,6,7,8], heart [9,10,11], and prostate [12].
The use of 23Na-MRI for imaging of the brain was first described in 1983 by Hilal et al., who observed changes following an induced stroke in a cat model [13]. In 1987, Turski et al. utilized the technique in patients with a cerebral neoplasm [14]. Since then, several feasibility studies [15, 16] have utilized 23Na-MRI for the imaging of stroke [17,18,19], demyelinating diseases [20], and brain tumors. In the latter case, various brain tumors exhibit increased sodium concentrations relative to normal brain structures [21,22,23]. Theoretically, this observation is based on the presence of cell membrane depolarization prior to cell division. Since cell division is increased in neoplasia, intracellular sodium concentration (ISC) is thus increased and consequently the total 23Na-concentration rises [24]. Therefore, 23Na-MRI could be useful for predicting therapeutic tumor response in brain [22] or other organs [25].
In order to serve as a reliable tool for the assessment of clinical stroke or brain tumor patients, studies have to investigate the absolute levels and differences of sodium concentrations in healthy volunteers undergoing consecutive MRIs with a dual-tuned (23Na/1H) head-coil at different time points. Thus, the objective of this study was to verify the repeatability and reproducibility of cerebral 23Na-MR imaging in healthy subjects.
Methods
This study was performed without any financial or non-financial support from industry. The authors had complete control of the data submitted for publication. The local institutional review board (IRB) and ethics committee (Medical Ethics Committee II Mannheim, Germany; reference number: 2013 566 N – MA) approved this prospective baseline study which was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Healthy volunteers
After the procedure was fully explained, written informed consent was obtained from all participants prior to MR imaging. Twelve healthy volunteers (8 females, 4 males, mean age 31 ± 8.3 years) underwent three brain MRI examinations (V1–3,) spread between two separate visits with an interval of 8 days between. During one visit, two consecutive, repetitive scans (V1 and V2) were obtained. During a time gap of 5 min in between the two scans the subject was moved out of the gantry. The isocenter was identical to the prior examination using the scanner’s dedicated laser positioning device. At the second visit, only one examination was performed. The subject was positioned in a similar position according to anatomic landmarks and the isocenter was again set using the scanner’s dedicated laser positioning device. The group was subdivided randomly, whereby one half of the subjects received two MRI scans during the first visit and one MRI during the second visit. The other half of the subjects received one MRI on the first visit and two MRIs on the second visit. Besides the standard exclusion criteria for MRI (i.e. pacemaker), patients with a history of brain lesions or neurological symptoms were excluded. For both visits, the subjects were scheduled at the same time of the day (to exclude influences of circadian rhythm changes of sodium concentrations [26]) and were asked to abstain from the consumption of alcohol and coffee for eight hours prior to the exams.
Brain MRI
All MR examinations were performed on a 3.0 T MR-system (Siemens TimTrio; Siemens Healthineers, Erlangen, Germany). Individuals were positioned supine and head first in a dual-tuned (23Na/1H) radiofrequency (RF) coil (Rapid Biomedical, Germany). In addition to the survey sequences, the imaging protocol included the following sequence protocol: standard morphological, axial T2 weighted images; axial fluid attenuated inversion recovery (FLAIR) images; diffusion-weighted imaging (DWI) based on echo planar imaging; T1 weighted magnetization-prepared rapid acquisition gradient-echo (MP-RAGE) for anatomical referencing, and a three dimensional (3D)-density-adapted projection reconstruction 23Na-sequence [27]. No contrast media was administered. Sequence details are summarized in Table 1. Echo time was defined as the time period between the middle of the excitation pulse and the beginning of the readout. A cylindrical falcon tube with a 0.6% NaCl reference was placed within the field of view as a concentration reference.
Quantification of sodium concentration
23Na-MRI images were co-registered offline to the corresponding T1 weighted MP-RAGE image for each volunteer using the statistical parametric mapping toolbox (SPM8, The Wellcome Trust Centre for Neuroimaging, London) of MATLAB (R2010a, The MathWorks Inc., Natick, MA). Data sets of every patient were analyzed on an OsiriX DICOM viewer 3.8.1 (OsiriX Foundation, Geneva, Switzerland). A quantitative assessment of 23Na-concentration was performed by two radiologists (reader 1 and 2 with 6 and 2 years experience in 23Na-imaging, respectively) who independently, manually placed predetermined, identically-sized (0.508 cm2) circular region of interests (ROIs) on three consecutive slices according to the following specific anatomic landmarks: the bilateral central gray (centrum semiovale) and temporal white matter (GM/WM), the bilateral heads of the caudate nuclei, the pons at the level of the superior cerebellar pedunculi, and the bilateral cerebellum within the pedunculi cerebelli medius. These ROIs were placed on every examination. An example of a ROI placement is shown in Fig. 1. The ROIs were placed on the morphological 1H images (MP-RAGE) and afterwards copied onto the 23Na-images. Values for 23Na-concentration in millimoles per kilogram wet weight were calculated according to the following formula:

Left: Example of region-of-interest (ROI) placement in the head of the caudate nucleus on a 23Na-image; right: T1 MP-RAGE as an anatomical reference image
where [Na] is sodium concentration, tiss is tissue, ref. is reference phantom, SNa is signal intensity of sodium, f is fast, s is slow, TE is echo time, TR is repetition time, alfa/beta is 0.6/0.4 for brain tissue [28] and 0.0/1.0 for CSF.
With:
T2ref/f = 7.15 msec, T2ref/s = 33.7 msec
Brain: T2tiss/f = 4 msec, T2tiss/s = 29 msec and T1tiss/s = 29 msec
CSF: T2tiss/s = 55 msec and T1tiss = 58.1 msec
Statistical analysis
JMP 10.0 (SAS Institute Inc., Cary, North Carolina, USA) was used for statistical analysis. Descriptive statistics (median, mean, 95% confidence interval and standard deviation (SD)) were used for all data. For the analysis of repeatability and reproducibility of cerebral 23Na-concentrations, repeatability was defined as repeated exams on the same day (V1 and V2) with the same experimental setup, whereas reproducibility was defined as a repeated exam (V3) with a pre-set time interval of 8 days. Repeatability and reproducibility analyses were performed using a Pearson’s momentum correlation. Intra-individual 23Na-concentrations in specific ROIs were tested with repeated measures ANOVA using a Dunnett’s test. Chi-squared tests were performed for subgroup analysis in terms of the left versus the right hemisphere. P values less than 0.05 were considered statistically significant. A normal distribution was confirmed using a Kolmogorov-Smirnov test (0.019 < p < 0.622). Due to the data scale, Spearman’s rho tests were chosen to determine the inter-reader correlation.
Results
Quantification of 23Na-concentration
The overall mean 23Na-concentration (in millimoles per kilogram wet weight) for both readers and sides was 51.5 ± 4.5 mmol/kg WW and 40.9 ± 3.8 mmol/kg WW for the respective gray and white matter, 60.9 ± 8.1 mmol/kg WW for the head of the caudate nucleus, 39.8 ± 5.3 mmol/kg WW for the pons, and 40.1 ± 4.9 mmol/kg WW for the cerebellum. Subgroup analysis comparing the left and right hemisphere did not reveal statistically significant differences other than in the head of the caudate nucleus. 23Na-concentrations of the head of the caudate nucleus were 63.1 ± 8.4 mmol/kg WW on the left compared to 58.7 ± 7.3 mmol/kg WW on the right (p = 0.01) (Fig. 2).

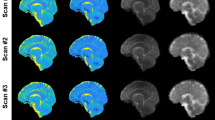
Top: First examination (V1) on the first examination day with 23Na-image, T1 MP-RAGE and DWI (from left to right); bottom: Second examination (V2) on the first examination day
Inter-individual 23Na-fluctuations
Pronounced inter-individual differences were identified in all anatomic regions. The max/min 23Na concentration values and maximum percentage differences were: Gray matter = 65.4/42.4 mmol/kg WW (35.1%), white matter 52.9/34.5 mmol/kg WW (34.7%), caudate head = 81.5/49.5 mmol/kg WW (39.3%), pons = 58.4/33.2 mmol/kg WW (43.0%), and cerebellum 52.3/33.0 mmol/kg WW (36.9%).
Repeatability analysis: intra-individual 23Na-concentrations
Excellent correlation (r2 = 0.94) was found between repeated measurements on the same day (V1 and V2). An example of two consecutive images is shown in Fig. 3. Overall, the mean 23Na-concentration measured at V1 and V2 were not significantly different (V1: 52.7 ± 20.7 mmol/kg WW vs V2: 53.2 ± 20.8 mmol/kg WW; p > 0.05). Similarly, there was no significant difference across all anatomic regions between measurements at V1 and V2 (compare Table 2; p > 0.05). The order of the MRI examinations (two examinations at the first or the second appointment) had no significant influence on the 23Na-concentration (0.206 < p < 0.886).

Total 23Na-concentrations with standard deviations (SD) according to laterality (GM = gray matter; WM = white matter; HCN = head of the caudate nucleus); * indicates significant difference with p = 0.01
Reproducibility analysis: intra-individual 23Na-concentrations
Excellent correlation (r2 = 0.86) was found between V1 and V3 measurements. Overall, mean 23Na-concentrations measured at V1 and V3 were not significantly different (V1: 52.7 ± 20.7 mmol/kg WW vs V2: 53.1 ± 21.6 mmol/kg WW; p > 0.05). Similarly, there were no significant differences across the anatomic regions between measurements of V1 and V3 (compare Table 2; p > 0.05). When comparing the maximum and the minimum values for the 23Na-concentration, the mean percentage of intra-individual differences ranged from 6.5% (GM) and 10% (Pons).
Inter-reader agreement
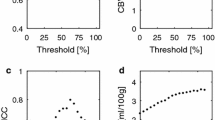
Moderate to good correlation (0.310 to 0.701) was found between the two readers. Overall, the mean 23Na-concentration as measured for the different anatomic regions by reader 2 was greater than that measured by reader 1 (see Fig. 4). The largest discrepancies were seen in the gray matter and in the head of the caudate (47.4 vs. 55.5 mmol/kg WW and 56.0 vs. 65.8 mmol/kg WW, respectively; p > 0.05).

Bland-Altman plot, plotting the ratio of the two readers versus the average of both readers. The lines and given numbers on the right side represent the mean of the ratio and the +/− 1.96 standard deviation (SD) of the ratio
Discussion
The potential of 23Na-MRI for brain imaging in oncological and non-oncological applications remains to be ultimately determined [29]. To further implement 23Na-MRI in clinical neuroimaging, particularly in the setting of oncological follow-up, certain fundamental requirements are to be fulfilled. One of these is the intra-individual reliability and reproducibility of brain 23Na-concentrations on consecutive MR examinations. Little published data are available regarding the 23Na-concentrations of healthy gray and white matter, but the values of the current study are in the range described in the literature [20, 21, 30]. This study showed no significant asymmetries in the 23Na-concentrations of several predefined areas of the human brain, other than between the left and right caudate head. These differences could be attributed to partial volume effects of the immediately adjacent cerebrospinal fluid (CSF). The relatively narrow head of the caudate nucleus impeded the manual ROI placement, which could explain these differences. One way to potentially solve this problem is by normalization of the data to a reference brain data set, as done in psychiatry studies for hippocampus volume measurements and the use of semi-automatic segmentation tools. Statistically significant intra-individual differences were neither seen between two consecutive MR exams nor between MR exams separated temporally by 8 days. This supports the repeatability and reproducibility of cerebral 23Na-MRI. However, per-patient differences in sodium concentration were as high as 10%, depending on the anatomic region. This potential bias should be considered in any further longitudinal or follow up study. Nevertheless, future studies may benefit from an intra-individual longitudinal approach, since inter-individual differences at a single time point can reach over 30%. Another important consideration for the clinical implementation of brain 23Na-MRI would be the development of a simple evaluation method for 23Na-MRI imaging with sufficient inter-reader reliability. The inter-reader reliability in this study was moderate but not perfect; however, this may be explained in part by the differences in clinical 23Na-MRI experience between the readers (6 vs. 2 years). As previously mentioned, a semi-automatic segmentation tool could facilitate this assessment and decrease inter-reader variability. In general, several future avenues may benefit from a broader clinical implementation of 23Na-MRI. Accuracy and quantification of 23Na concentrations between different research facilities, hospitals, and techniques (e.g. UTE, radial or cones scheme [31]) should be confirmed. Double-tuned coils seem to be the ideal instrument for 23Na-imaging enabling the appropriate fusion of 1H- and 23Na-images. Although the reliability of the current technique appears to be sufficient, this potential (small) for bias should be taken into account within further studies. While intra-individual comparison seems acceptable for assessment of 23Na concentration, biases may arise due to natural inter-individual differences, and further follow-up studies are necessary. Finally, future semi-automatic segmentation tools as proposed could help to partially overcome biases due to inter-reader interpretative differences.
Limitations
Our study had a number of limitations. Since it was initiated as a baseline study, the study group was relatively small and young without any known medical conditions. To evaluate the true clinical value of this technique, further evaluations in longitudinal studies will be necessary both in healthy volunteers as well as in patients.
Conclusion
Our study has shown that intra-individual 23Na-concentrations in healthy subjects do not significantly differ after repeated scans on the same day and a pre-set time interval. This confirms the repeatability and reproducibility of cerebral 23Na-imaging and serves as a baseline for future studies. However, with manual placement of ROIs in predetermined anatomic landmarks, fluctuations in 23Na-concentrations can be observed. This must be taken into account if 23Na-imaging is to be considered as a potential tool for therapeutic monitoring.
Abbreviations
- DWI:
-
Diffusion-weighted imaging
- FLAIR:
-
Fluid attenuated inversion recovery
- GM, WM:
-
Gray and white matter
- HCN:
-
Head of the caudate nucleus
- IRB:
-
Institutional review board
- ISC:
-
Intracellular sodium concentration
- MP-RAGE:
-
Magnetization-prepared rapid acquisition gradient-echo
- MRI:
-
Magnetic resonance imaging
- RF:
-
Radiofrequency
- SD:
-
Standard deviation
References
Berendsen HJ, Edzes HT. The observation and general interpretation of sodium magnetic resonance in biological material. Ann N Y Acad Sci. 1973;204:459–85.
Haneder S, et al. Quantitative and qualitative 23Na MR imaging of the human kidneys at 3 T: before and after a water load. Radiology. 2011;260(3):857–65.
Maril N, et al. Sodium MRI of the human kidney at 3 tesla. Magn Reson Med. 2006;56(6):1229–34.
Haneder S, et al. Quantitative in vivo 23Na MR imaging of the healthy human kidney: determination of physiological ranges at 3.0T with comparison to DWI and BOLD. MAGMA. 2013;26(6):501–9.
Trattnig S, et al. Advanced MR methods at ultra-high field (7 tesla) for clinical musculoskeletal applications. Eur Radiol. 2012;22(11):2338–46.
Noebauer-Huhmann IM, et al. Sodium imaging of the lumbar intervertebral disk at 7 T: correlation with T2 mapping and modified Pfirrmann score at 3 T--preliminary results. Radiology. 2012;265:555–64.
Borthakur A, et al. Quantifying sodium in the human wrist in vivo by using MR imaging. Radiology. 2002;224(2):598–602.
Constantinides CD, et al. Human skeletal muscle: sodium MR imaging and quantification-potential applications in exercise and disease. Radiology. 2000;216(2):559–68.
Jerecic R, et al. ECG-gated 23Na-MRI of the human heart using a 3D-radial projection technique with ultra-short echo times. MAGMA. 2004;16(6):297–302.
Konstandin S, Schad LR. Two-dimensional radial sodium heart MRI using variable-rate selective excitation and retrospective electrocardiogram gating with golden angle increments. Magn Reson Med. 2012;70:791–9.
Greiser A, Haase A, von Kienlin M. Improved cardiac sodium MR imaging by density-weighted phase-encoding. J Magn Reson Imaging. 2005;21(1):78–81.
Hausmann D, et al. Apparent diffusion coefficient and sodium concentration measurements in human prostate tissue via Hydrogen-1 and Sodium-23 magnetic resonance imaging in a clinical setting at 3 T. Investig Radiol. 2012.
Hilal SK, et al. In vivo NMR imaging of tissue sodium in the intact cat before and after acute cerebral stroke. AJNR Am J Neuroradiol. 1983;4(3):245–9.
Turski PA, et al. Experimental and human brain neoplasms: detection with in vivo sodium MR imaging. Radiology. 1987;163(1):245–9.
Clayton DB, Lenkinski RE. MR imaging of sodium in the human brain with a fast three-dimensional gradient-recalled-echo sequence at 4 T. Acad Radiol. 2003;10(4):358–65.
Kohler S, et al. Fast three-dimensional sodium imaging of human brain. Magma. 2001;13(2):63–9.
Maudsley AA, Hilal SK. Biological aspects of sodium-23 imaging. Br Med Bull. 1984;40(2):165–6.
Thulborn KR, et al. Sodium MR imaging of acute and subacute stroke for assessment of tissue viability. Neuroimaging Clin N Am. 2005;15(3):639–53 xi-xii.
Thulborn KR, et al. Comprehensive MR imaging protocol for stroke management: tissue sodium concentration as a measure of tissue viability in nonhuman primate studies and in clinical studies. Radiology. 1999;213(1):156–66.
Zaaraoui W, et al. Distribution of brain sodium accumulation correlates with disability in multiple sclerosis: a cross-sectional 23Na MR imaging study. Radiology. 2012;264(3):859–67.
Ouwerkerk R, et al. Tissue sodium concentration in human brain tumors as measured with 23Na MR imaging. Radiology. 2003;227(2):529–37.
Thulborn KR, et al. Quantitative sodium MR imaging and sodium bioscales for the management of brain tumors. Neuroimaging Clin N Am. 2009;19(4):615–24.
Nagel AM, et al. The potential of relaxation-weighted sodium magnetic resonance imaging as demonstrated on brain tumors. Investig Radiol. 2011;46(9):539–47.
Laymon CM, et al. Combined imaging biomarkers for therapy evaluation in glioblastoma multiforme: correlating sodium MRI and F-18 FLT PET on a voxel-wise basis. Magn Reson Imaging. 2012;30(9):1268–78.
Danisch, M., et al., [Bilateral Na MR imaging of the breast and quantification of sodium concentration.]. Z Med Phys. 2013;24:65–72.
Harrington MG, et al. Cerebrospinal fluid sodium rhythms. Cerebrospinal Fluid Res. 2010;7:3.
Nagel AM, et al. Sodium MRI using a density-adapted 3D radial acquisition technique. Magn Reson Med. 2009;62(6):1565–73.
Hubbard PS. Nonexponential nuclear magnetic relaxation by quadrupole interactions. J Chem Phys. 1970;53(3):985–7.
Madelin G, et al. Sodium MRI: methods and applications. Prog Nucl Magn Reson Spectrosc. 2014;79C:14–47.
Madelin G, Regatte RR. Biomedical applications of sodium MRI in vivo. J Magn Reson Imaging. 2013;38(3):511–29.
Konstandin S, Nagel AM. Measurement techniques for magnetic resonance imaging of fast relaxing nuclei. MAGMA. 2014;27(1):5–19.
Acknowledgements
Not applicable.
Funding
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
All authors have read and approved the manuscript. MM: Project development, Data Collection, Data analysis, Manuscript writing. SH: Project development, Data Collection, Data analysis, Manuscript writing. SK: Data analysis, Manuscript editing. JB: Data Collection, Manuscript editing. JM: Manuscript editing. LS: Manuscript editing. HK: Project development, Manuscript editing. SS: Project development, Manuscript editing. CK: Project development, Data Collection, Data analysis, Manuscript writing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The local institutional review board (IRB) and ethics committee (Medical Ethics Committee II Mannheim, Germany; reference number: 2013 566 N – MA) approved this prospective baseline study which was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
After the procedure was fully explained, written informed consent was obtained from all participants prior to MR imaging.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Meyer, M.M., Haneder, S., Konstandin, S. et al. Repeatability and reproducibility of cerebral 23Na imaging in healthy subjects. BMC Med Imaging 19, 26 (2019). https://doi.org/10.1186/s12880-019-0324-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-019-0324-6