
Abstract
Background
Kidney transplant recipients (KTRs) are at an elevated risk of progressing to severe infections upon contracting COVID-19. We conducted a study on risk factors and multi-pathogen infections in KTRs with SARS-CoV-2 Omicron variant.
Methods
KTRs were subjected to a thorough etiological evaluation. Whenever feasible, they were also provided with bronchoscopy and bronchoalveolar lavage to enable metagenomic next-generation sequencing (mNGS), ideally within a 48-hour window post-admission. We performed a retrospective analysis for pathogens and risk factors of KTRs with the COVID-19 virus variant Omicron.
Results
We included thirty patients in our study, with sixteen exhibiting single infection of COVID-19 and fourteen experiencing co-infections, predominantly with Pneumocystis jirovecii. Notably, patients with severe cases demonstrated significantly elevated levels of C-reactive protein (CRP) and interleukin-6 compared to those with moderate cases (P < 0.05). Furthermore, individuals whose conditions progressed had markedly higher baseline serum creatinine levels than those without such progression (P < 0.05). The presence of heart failure, acute exacerbation of renal dysfunction, and a history of opportunistic infections were significantly associated with a higher likelihood of deterioration and hospital admission due to the SARS-CoV-2 Omicron variant, as compared to the control group (P < 0.05). In subsequent follow-up analysis, the all-cause rehospitalization rate was observed to be 21.4%, with Pneumocystis jirovecii infection accounting for half of these cases.
Conclusion
Among KTRs, a significant coinfection rate of 47% was observed, with Pneumocystis jirovecii emerging as the predominant pathogen in these cases. The development of heart failure, acute exacerbation of chronic renal dysfunction, and a prior history of opportunistic infections have been identified as potential risk factors that may contribute to clinical deterioration in KTRs. Additionally, Pneumocystis jirovecii infection has been established as a critical factor influencing the rate of all-cause rehospitalization within this patient population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a highly transmissible and pathogenic coronavirus that emerged in late 2019 and has caused a pandemic of acute respiratory disease-coronavirus disease 2019(COVID-19), and over 767 million confirmed cases have been reported to the World Health Organization (WHO), including approximately 6.94 million deaths. Although most infections in the general population are mild and have a good prognosis, kidney transplant recipients have poorer prognosis. The immunosuppressed state makes them highly susceptible to severe COVID-19 infections and increases their mortality rates [1]. Furthermore, kidney transplant recipients are also prone to opportunistic infections, such as Pneumocystis jirovecii and cytomegalovirus, which can be difficult to distinguish from COVID-19 pneumonia. In December 2022, the SARS-CoV-2 Omicron variant pandemic significantly impacted the Chinese population, with kidney transplant patients being particularly vulnerable. To address this, we undertook a study specifically examining the risk factors and multi-pathogen infections associated with Omicron variant pneumonia in KTRs. This research diverges from previous studies that focused on multiple subtypes of COVID-19. Notably, our study predominantly utilized Bronchoalveolar Lavage Fluid (BALF) for mNGS, marking the first comprehensive investigation of coinfection pathogens in KTRs with the Omicron variant using this approach.
Methods
Study design
A retrospective analysis was conducted on kidney transplant recipients with omicron variant. The research protocol was approved by the Ethics Committee of the Peking University Third Hospital [Ethical Approval Number: 2021(214-01)], and informed consent was obtained from all participants.
Study subjects
Patients with postkidney transplantation and subsequent COVID-19 infection admitted to the Infectious Diseases Department of Peking University Third Hospital between January 1st and August 31st 2022 were enrolled in this cohort study. The inclusion criteria were (1) aged ≥ 18 years; (2) post kidney transplantation; (3) met the diagnostic criteria of New Coronavirus Infection Diagnosis and Treatment Plan (China Trial Version 10) [2]. (4) The SARS-CoV-2 strain is identified as Omicron variant by Sanger sequence or BALF-mNGS. (5) Ethnicity: Asian Chinese Han population.
The exclusion criteria were as follows: patients with other diseases that cause immunosuppression, including malignancy patients undergoing chemotherapy, transplantation of organs other than kidneys, hematopoietic stem cell transplantation, and HIV infections, or other autoimmune diseases. We meticulously reviewed the medical records of KTRs to obtain detailed information, particularly regarding their prior history of opportunistic infections. Additionally, we conducted a thorough inquiry into the patients’ previous treatments and any documented opportunistic infections.
Over the course of our research period, we admitted a total of 580 patients. Among these, 475 were identified with COVID-19. Within this group, we identified 33 KTRs. Of these KTRs, 30 were confirmed to have the Omicron variant, while the remaining 3 had COVID-19 cases that not be definitively classified. Ultimately, it was these 30 KTRs with the Omicron variant who were included in the final analysis (Fig. 1).

Flowchart of patient selection proces in the study
Data collection
Data were collected on the demographic characteristics of all patients, including age and sex, medical history, physical examination, laboratory tests, chest CT scans, treatment plans, and clinical outcomes.
Specimen collection and pathological testing
Upon admission, within a 48-hour window, we systematically collected a range of diagnostic samples. This included blood cultures, sputum cultures, and smear microscopy with specific attention to acid-fast staining. We performed sputum multipathogen PCR testing to identify a spectrum of bacterial and viral pathogens, including Streptococcus pneumoniae, Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa, Haemophilus influenzae, Acinetobacter baumannii, Burkholderia cepacia, as well as influenza virus, respiratory syncytial virus, parainfluenza virus, adenovirus, Mycoplasma, Chlamydia, and Legionella pneumophila.
Furthermore, whole blood multipathogen PCR testing was predominantly employed for the quantitative detection of human cytomegalovirus and Epstein-Barr virus. In addition to PCR-based methods, we also conducted blood tests for 1,3-β-D-glucan (G-test) and galactomannan antigen (GM test) to enhance the diagnostic accuracy for fungal infections. If permitted by the patients’ consent and their medical condition, bronchoscopy and bronchoalveolar lavage were conducted within a 48-hour window following hospital admission.BALF was submitted for mNGS. If lung inflammation was diffusely distributed with a uniform morphology (such as widespread ground-glass opacity), bronchoalveolar lavage was typically performed in the right middle lobe or lingular segment of the left upper lobe. If lung inflammation was present in multiple lobes with varied morphologies (including ground-glass opacities, consolidation, and nodules), multiple-point lavages were conducted across different lung lobes (with a total lavage volume not exceeding 200 ml). BALF samples collected from different lobes were mixed and promptly sent for NGS analysis. The patients who did not get BALF- mNGS would get SARS-CoV-2 Sanger sequencing for the strain confirmation.
Patients are categorized into mild, moderate, severe, and critical types of COVID-19 based on the classification criteria outlined in the New Coronavirus Infection Diagnosis and Treatment Plan (China Trial Version 10) [2].
Statistical analysis
Statistical analysis was conducted using SPSS software version 20.0. Categorical data are expressed as frequencies and percentages. Normally distributed continuous data are represented as the mean ± standard deviation, while nonnormally distributed data are expressed as medians with interquartile ranges. T tests were applied to normally distributed data, whereas nonparametric tests or chi-square tests were used for nonnormally distributed data. A P value of less than 0.05 indicated a statistically significant difference.
Results
Clinical characteristics of KTRs in our study
Thirty patients were included in the study. The median age was 49.5 years (IQR: 43.5–56.3 years). Twenty-five were male, and five were female. The median duration since kidney transplant was 84.5 months (IQR: 31.8-120.0months). None of the 30 patients had a history of receiving the COVID-19 vaccine. The condition of 5 patients (13.3%) was progressive during their hospital stay (Table 1). On average, the patients experienced 12.0 days (IQR: 8.5–20.0 days) of illness before admission. Twenty-one patients (70%) were diagnosed with a moderate form of COVID-19, and 9 patients (30%) were diagnosed with the severe form (Table 1).
Microbiological findings
Out of the 30 patients in our study, BALF was subjected to mNGS in 27 cases. The remaining 3 patients did not undergo bronchoscopy. Despite this, routine microbiological assessments failed to yield any positive indications of coinfection. Our analysis showed that 16 patients experienced a singular infection with the COVID-19 virus, whereas 14 patients had coinfections involving the COVID-19 virus and other pathogens, as illustrated in Fig. 2.

a Pathogens coinfected in kidney transplant patients with novel coronavirus infection. b Specific distribution of coinfections in kidney transplant patients with novel coronavirus infection
-
Nine had concurrent infections with Pneumocystis jirovecii.
-
Five had bacterial coinfections: Klebsiella pneumoniae (N = 3), Staphylococcus aureus(N = 1), Proteus mirabilis (N = 1).
-
Five had cytomegalovirus infection.
-
Five had aspergillosis infections.
As shown in Fig. 2; Table 1, among the KTRs, 53% experienced a single COVID-19 infection. The rate of co-infection was 47%. The most prevalent co-infection was Pneumocystis jirovecii followed by cytomegalovirus , bacterial infections, and aspergillosis.
Treatment and prognosis
In our cohort of 30 patients, 21 (70%) were diagnosed with a moderate form of COVID-19, while 9 (30%) presented with severe cases, as classified by the New Coronavirus Infection Diagnosis and Treatment Plan (China Trial Version 10). Post-hospital admission, we observed a loss of transplanted kidney function in 3 patients. Additionally, 3 patients with critical conditions required mechanical ventilation. Notably, BALF analysis in one of the critical patients indicated a concurrent infection with Pneumocystis jirovecii and Aspergillus. Another critical patient was found to have a concurrent infection with Klebsiella pneumoniae.
All patients were treated with antiviral therapy (/Nirmatrelvir/Ritonavir or Molnupiravir) and corticosteroids postadmission (Table 1).
-
Nine patients (30%) received tocilizumab, and two patients (6.7%) were administered baricitinib.
-
Nine patients with concurrent Pneumocystis jirovecii infection were treated with high doses of sulfonamide.
-
Five patients with cytomegalovirus coinfections were given ganciclovir.
-
Five patients underwent antifungal treatment with voriconazole, targeting Aspergillus infection.
Subgroup analysis based on clinical typing of COVID-19 at admission
The 30 patients were divided into two groups based on the clinical type of COVID-19 infection: the moderate type group (N = 21) and the severe type group (N = 9). A nonparametric test was used to compare the two groups (Tables 2 and 3).
Biomarkers
Patients in the severe group had significantly higher levels of CRPand interleukin-6 (IL-6) than those in the moderate group. This difference was statistically significant (P < 0.05). No significant differences were observed in other clinical indicators between the two groups (Table 4).
These findings suggest that biomarkers such as CRP and IL-6 can indicate the severity of COVID-19 in KTRs.
Subgroup analysis based on the presence of coinfections beyond the novel coronavirus
The 30 cases were divided into two groups based on the presence of coinfection: single COVID-19 virus variant Omicron infection (N = 16) and coinfections (N = 14). Nonparametric statistical analysis revealed no significant differences between the two groups. An assessment of the history of opportunistic infections and antiviral treatments administered prior to hospitalization using the chi-square test also showed no significant differences (P > 0.05) (Tables 2 and 3).
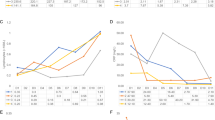
Subgroup analysis of predictive factors for deterioration post-admission
In our study, we defined the “progressive group” as those patients whose COVID-19 classification worsened from the baseline type to a more severe category following hospitalization. This progression could range from mild to moderate, severe, critical, or even fatal, as depicted in Figs. 3 . Conversely, patients whose COVID-19 classification remained the same or improved post-hospitalization were categorized as the “stable group”, as shown in Fig. 3.

The description of progressing group: COVID-19 classification progress from admitted to hospital to hospitalization

Follow-up of kidney transplant patients with COVID-19 conditions after discharge
The cohort was divided into two groups: the stable group, comprising 25 patients, and the progressive group, with 5 patients. This categorization was based on the observed conditions during hospitalization, such as a shift from moderate to severe or critically severe stages. Our analysis revealed significantly higher baseline creatinine levels in the progressive group compared to the stable group (P < 0.05). No significant differences were observed in other clinical indicators between these two groups.
We conducted statistical analyses using chi-square tests to assess potential predictive factors for post-admission deterioration in KTRs. These factors included a history of opportunistic infections, presence of coinfections, concurrent heart failure, acute exacerbation of renal dysfunction, and the clinical type of COVID-19 pneumonia upon admission. The results underscored that heart failure, acute exacerbation of renal dysfunction, and a history of opportunistic infections were significant risk factors for deterioration post-hospitalization in KTRs, as detailed in Tables 2 and 3.
Follow-up analysis
As shown in Fig. 3, over a follow-up period of 4.5(2.0–7.0) months, the all-cause rehospitalization rate was 21.4% (6/28). Rehospitalization reasons were heart failure (N = 1), transplant kidney dysfunction (N = 1), gastrointestinal bleeding (N = 1), and pulmonary opportunistic infections (Pneumocystis jirovecii N = 3). No cytomegalovirus or Aspergillus infections were observed (Fig. 3).
Discussion
Kidney transplant recipients are prone to opportunistic infections, such as Pneumocystis jirovecii and cytomegalovirus infections, due to prolonged immunosuppression and susceptibility to a variety of pathogens. KTRs have a poorer prognosis than the general population with regard to COVID-19 infections. Early data revealed that the mortality rate of KTRs infected with COVID-19 ranges from 20 to 32% [1, 3,4,5], according to data from WHO, the infection fatality ratio for COVID-19 in the general population is estimated to converge at approximately 0.5 to 1% [6].
In multiple early reviews concerning postkidney transplant COVID-19 infections, the occurrence of severe complications such as respiratory distress, acute kidney injury, and acute myocardial infarction, as well as the rate of severe cases and mortality, were significantly higher than in the general population [7, 8]. The previous studies were based on multiple variants of COVID-19 (including alpha, beta, delta, etc.) Our study is solely focused on the variant Omicron, which was a pandemic in China in 2023 and gave us a real prognosis for the COVID-19 virus variant Omicron in KTRs.
In our analysis, both heart and kidney dysfunction, as well as a history of opportunistic infections, significantly influenced the exacerbation of COVID-19 posthospitalization. Patients with deteriorating heart and kidney function should be particularly risk factors for disease progression. The severity categorization of COVID-19 in kidney transplant patients and concurrent infections does not contribute as risk factors for posthospitalization exacerbation.
KTRs experience rapid disease progression after COVID-19 infection. A multicenter study in Italy in 2020 found that approximately 75% of patients experienced acute exacerbation within one week, 39% needed mechanical ventilation, and 21% needed renal replacement therapy [9]. The outcomes varied greatly for the different research times, viral strains and countries. In our study, all patients were infected with the Omicron strain of SARS-CoV-2 in 2023. The included data cover hospitalizations from January 1st to August 31st, 2023, with access to advanced life support conditions such as ICU admission, mechanical ventilation, and ECMO, accurately reflecting the outcomes of moderate and severe cases postkidney transplant with Omicron variant infections. In our study, the mortality rate was 6.7%, which is lower compared with earlier data on mortality rates in postkidney transplant COVID-19 patients.
Furthermore, our study revealed that KTRs had a high rate of coinfection with coronavirus and other pathogens, reaching up to 46.6%. Pathogens were Pneumocystis jirovecii (N = 9, 56.3%), bacteria (N = 5, 16.7%), cytomegalovirus (N = 5, 16.7%), and aspergillosis (N = 5, 16.7%). A multipathogeninfection was identified (N = 7, 23.3%). Both our clinical experience and the literature suggest that the general population rarely experiences coinfections in the early stages of COVID-19, with coexisting bacterial infections seen in approximately 3–8% of the general COVID-19-positive population. Among those with severe forms, approximately 12% experience bacterial infections, and the prevalence of mixed bacterial and fungal infections is 8%. Langford et al. assessed bacterial coinfections during and after a COVID-19 diagnosis, identifying a primary coinfection prevalence of 3.5% (95% CI 0.4–6.7%) and a secondary (hospital-acquired) coinfection prevalence of 14.3% [10, 11]. The high coinfection rate in our study among kidney transplant patients post-COVID-19 can be attributed to the aggressive and timely implementation of bronchoscopies and bronchoalveolar lavage mNGS. Traditional pathogen testing methods, including microscopic examinations, cultures, serological antigen-antibody tests, and PCR, show significantly lower positive rates than mNGS, especially when determining coinfections with viruses and fungi. This aligns with the findings of Zhang’s research [12]. Traditional microbiological testing methods are technically mature and highly reliable with vast clinical applications. mNGS technology theoretically offers nonpresumptive, one-time testing for unknown pathogens with a broader detection scope. They recommend considering mNGS to identify pathogens, especially for immunosuppressed hosts suspected of having lower respiratory infections, suggesting causes other than common community-acquired pneumonia (CAP) pathogens [13, 14].
Currently, anti-coronavirus drugs (such as Nirmatrelvir/Ritonavir and Molnupiravir) are indicated for high-risk groups infected with coronavirus within 5 days of onset, which can reduce the rate of severe cases. Radcliffe C and others reported that Molnupiravir can reduce the severity and mortality rate in postkidney transplant patients infected with coronavirus [15]. In our study, the rates of disease exacerbation in the nonantiviral and antiviral drug groups were 22.2% and 14.3%, respectively. The rate of disease exacerbation in the antiviral drug group was lower than that in the nonantiviral group, but without statistic difference. (P > 0.05). Ritonavir has a strong drug-drug interaction with CYP3A-dependent drugs. Immunosuppressive drugs such as calcineurin inhibitors (e.g., tacrolimus and cyclosporine) and mammalian target of rapamycin (mTOR) inhibitors rely heavily on CYP3A metabolism, which are important drugs in KTRs. KTRs are particularly vulnerable to COVID-19 morbidity and mortality due to immunosuppression, comorbidities [16, 17].
In the American Society of Transplantation’s statement on oral antiviral therapy for COVID-19 in organ transplant recipients,Nirmatrelvir/Ritonavir poses significant challenges for use in many transplant patients. This is due to notable drug interactions and the complexities associated with therapeutic drug monitoring, particularly for outpatients actively infected with COVID-19. Molnupiravir, on the other hand, has shown relatively low efficacy and has not yet been evaluated in the context of transplant recipients [18].
Our analysis observed a lower rate of disease exacerbation among patients treated with antiviral drugs compared to those in the non-antiviral group (22.2% vs. 14.3%); however, this difference was not statistically significant. The small sample size in our research introduces a limitation that cannot be overlooked. As a result, it is imperative that further evaluations be conducted to ascertain the efficacy and safety of Oral Antiviral Therapy for COVID-19, particularly within the cohort of transplant recipients. During the follow-up study, the all-cause rehospitalization rate was 21.4%, with half of the cases being opportunistic lung infections (Pneumocystis jirovecii pneumonia). Risk factors for Pneumocystis jirovecii infection include the use of immunosuppressive agents, cancer, solid organ and stem cell transplantation, autoimmune diseases, inflammatory diseases, and congenital immune deficiencies. In recent years, the SARS-CoV-2 pandemic has become a concern. SARS-CoV-2 can impair the host’s immune system, increasing the risk of bacterial and fungal coinfections, including Pneumocystis jirovecii [19]. Therefore, SARS-CoV-2 infection has also become a risk factor for Pneumocystis jirovecii infection. Therefore, in patients with COVID-19 postkidney transplantation, there should be increased emphasis on the preventive treatment of Pneumocystis jirovecii pneumonia.
There are some limitations in our study: firstly, the KTR patients admitted to hospital were included, but not mild outpatient patients, which means that patients who need hospitalization might lead to selection of severe infection probably secondary to an opportunistic infections. This study does not reflect the generel population of KTR infected with COVID19. Secondly, the sample size is small and it is a single centre study, we hope to increase the sample size and research centers in the future.
In summary, our study indicates that KTRs are at a heightened risk for coinfections with the SARS-CoV-2 Omicron variant. We emphasize the importance of proactive bronchoscopy and bronchoalveolar lavage for precise pathogen identification, which is crucial for accurate diagnosis and can significantly contribute to reducing mortality rates among this vulnerable population. Furthermore, our findings suggest that acute exacerbations of cardiac and renal dysfunction, along with a history of opportunistic infections, are potential risk factors that may predict the deterioration of COVID-19 conditions post-hospital admission. These insights underscore the need for vigilant monitoring and tailored treatment strategies for KTRs to improve clinical outcomes during the ongoing pandemic.”
Data availability
No, I don’t have any research data outside the submitted manuscript file. The datasets generated during and analyzed during the current study are available from Dr. Lu.
References
Paolo Cravedi, Suraj S, Mothi Y, Azzi, et al. COVID-19 and kidney transplantation: results from the TANGO International Transplant Consortium. Am J Transpl. 2020;20(11):3140–8. https://doi.org/10.1111/ajt.16185.
New Coronavirus Infection Diagnosis and Treatment Plan. (China Trial Version 10). https://www.gov.cn/zhengce/zhengceku/2023-01/06/content_5735343.htm[accessed 5 January 2023].
Akalin E, Azzi Y, Bartash R, et al. Covid-19 and kidney transplantation. N Engl J Med. 2020;382(25):2475–7. https://doi.org/10.1056/NEJMc2011117.
Elias M, Pievani D, Randoux C, et al. COVID-19 infection in kidney transplant recipients: disease incidence and clinical outcomes. J Am Soc Nephrol. 2020;31(10):2413–23. https://doi.org/10.1681/ASN.2020050639.
Devprakash Choudhary D, Kenwar A, Sharma, et al. Risk factors for mortality in kidney transplant recipients with COVID-19: a singlecenter experience and case–control study. BMC Nephrol. 2022;23(1):241. https://doi.org/10.1186/s12882-022-02821-8.
World Health Organization. Estimating mortality from COVID-19. https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci-Brief-Mortality-2020.1.
KremerD PTT, Verhaar MC, et al. A systematic review and meta-analysis of COVID-19 in kidney transplant recipients: lessons to be learned. Am J Transpl. 2021;21(12):936–3945. https://doi.org/10.1111/ajt.16742.
Mahalingasivam V, Craik A, Tomlinson LA, et al. A systematic review of COVID-19 and kidney transplantation. Kidney Int Rep. 2021;6(1):24–45. https://doi.org/10.1016/j.ekir.2020.10.023.
Alberici F, Delbarba E, Manenti C, et al. A single center observational study of the clinical characteristics and short-term outcome of 20 kidney transplant patients admitted for SARS-CoV-2 pneumonia. Kidney Int. 2020;97(6):1083–8. https://doi.org/10.1016/j.kint.
Bradley J, Langford M, Therefore S, Raybardhan, et al. Antibiotic prescribing in patients with COVID-19: rapid review and meta-analysis. Clin Microbiol Infect. 2021;27(4):520–31. https://doi.org/10.1016/j.cmi.2020.12.018.
Maria Calderon G, Gysin A, Gujjar, et al. Bacterial coinfection and antibiotic stewardship in patients with COVID-19: a systematic review and meta-analysis. BMC Infect Dis. 2023;23(1):14. https://doi.org/10.1186/s12879-022-07942-x.
Zhang JW, Yan HX, WU J, et al. Long Term Management Topic of Renal Transplant Recipients Pathogeny research of pulmonary infection after renal transplantation based onmetagenomics nextgeneration sequencing. Chin J Organ Transpl. 2021;42(5):260–4. https://doi.org/10.3760/cma.j.cn421203-20210224-00069.
Editorial Board of Chinese Journal of Infectious Diseases. Clinical practice expert consensus for the application of metagenomic next generation sequencing. Chin J Infect Dis. 2020;38(11):681–9. https://doi.org/10.3760/cma.j.cn311365-20200731-00732.
Chinese Thoracic Society. Consensus of clinical pathways of metagenomic next-generation sequencing test in diagnosis of lower respiratory tract infections in China. Chin J Tuberc Respir Dis. 2023;46(4):322–35. https://doi.org/10.3760/cma.j.cn112147-20220701-00553.
Radcliffe C, Palacios CF, Azar MM, et al. Real-world experience with available, outpatient COVID-19 therapies in solid organ transplant recipients during the Omicron surge. Am J Transpl. 2022;22(10):2458–63. https://doi.org/10.1111/ajt.17098.
Tang Y, Li Y, Song T. Optimizing the use of nirmatrelvir/ritonavir in solid organ transplant recipients with COVID-19: a review of immunosuppressant adjustment strategies. Front Immunol. 2023;14:1150341.
Nair V, Jandovitz N, Hirsch JS, Nair G, Abate M, Bhaskaran M, et al. COVID-19 in kidney transplant recipients. Am J Transpl. 2020;20:1819–25. https://doi.org/10.1111/ajt.15967].
Kumar D, Humar A, Ison MG, Kaul D, Blumberg E. Theodoropoulos N. AST Statement on oral antiviral therapy for COVID-19 for Organ Transplant recipients. [accessed on 21 May 2022].
Xue T, Kong X. Liang Ma. Trends in the Epidemiology of Pneumocystis Pneumonia in Immunocompromised Patients without HIV Infection. J Fungi (Basel). 2023,31;9(8):812. https://doi.org/10.3390/jof908081.
Acknowledgements
Not applicable.
Funding
The study was not supported by any funding.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Jing Chen, Yuanbo Su, and Ming Lu. The first draft of the manuscript was written by [Jing Chen], and all authors commented on previous versions of the manuscript. All the authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We received approval from the Ethics Committee of the Peking University Third Hospital [Ethical Approval Number: 2021(214-01)]. We confirm that their study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. We confirm that all subjects provided informed consent to participate in the study. We confirm that participants provided consent for publication if any identifying information was included in the manuscript.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, J., Su, Y. & Lu, M. Risk factors and multi-pathogen infections in kidney transplant recipients with omicron variant pneumonia: a retrospective analysis. BMC Infect Dis 24, 559 (2024). https://doi.org/10.1186/s12879-024-09444-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09444-4