
Abstract
Background
The Geriatric Depression Scale (GDS) has shown good validity and reliability, but few studies have examined the GDS among very old adults or the Swedish translation.
Objectives
Evaluate the validity and reliability of the Swedish version of GDS-15 among very old adults.
Methods
In the Umeå85 + /GErontological Regional DAtabase (GERDA) study, 387 participants were assessed with both the GDS-15 and the Montgomery-Åsberg Depression Rating Scale (MADRS). The mean age was 91 years. Concurrent validity between the scales was calculated using Spearman's correlation. We used the Diagnostic and Statistical Manual of Mental Disorders (DSM) V symptom criteria for depression based on MADRS item scores to define depression. We calculated the Area Under the Curve (AUC) and found an optimal cut-off.
A convenience sample with 60 individuals was used to calculate test–retest reliability with Cohen’s kappa and Intraclass Correlation Coefficient (ICC).
Results
Spearman's correlation coefficients between total scores for GDS-15 and MADRS were 0.60. Cronbach's alpha for the whole scale was 0.73. The AUC was 0.90 for distinguishing major depression, and the recommended cut-off of ≥ 5 showed a sensitivity of 95.2% and specificity of 65.8%. The test–retest showed that Cohen’s kappa was substantial (0.71) and the ICC was excellent (0.95).
Conclusions
The Swedish version of the GDS-15 showed good validity and reliability among very old adults. The generally recommended cut-off of ≥ 5 seems reasonable to use with the Swedish version and among very old adults.
Similar content being viewed by others


Introduction
Globally, the percentage of older adults is increasing. The United Nations (UN) estimates that by 2060, the number of older people will double from approximately 9% to approximately 18% [1]. In a systematic review article, Luppa and coworkers found that the pooled prevalence of depressive disorders according to assessment scales among those aged 75 or older was 17.1% (95% confidence interval 9.7–26.1%). Moreover, the rates of depression increase substantially among people in the age group 85–89 by 20–25% and 90 years and older by 30–50% [2]. Similar results were found in a Swedish study among very old adults, where the prevalence of depression in 85-year-olds was 16.8% and increased among 90-year-olds and 95-year-olds and older to 34.1% and 32.3%, respectively. In addition to the high prevalence, undertreatment of depression was found where 33% had no antidepressant treatment and 59% were still depressed despite antidepressant treatment [3].
The Geriatric Depression Scale-15 item version (GDS-15) was created in English in 1986 from the GDS-30 item version [4]. It has been translated into more than 30 languages and is one of the most commonly used depression screening tools administered worldwide in geriatric populations. The questionnaire was designed to be answered with a simple "yes" or "no" answer, facilitating ease of use for older individuals, including those with impaired cognition. Each item gives one point where the scoring answer is “yes” for some questions and “no” for others. A systematic review and meta-analysis on the recommended GDS-15 cut-off score of ≥ 5 found a pooled sensitivity of 0.89 and specificity of 0.77. The samples included in the studies had an average age ranging from 66 to 87, and the majority of them excluded individuals with impaired cognition [5]. Conradsson et al. found that among very old people with Mini-Mental State Examination (MMSE) scores ≥ 10, the GDS-15 was useful for assessing depressive symptoms [6]. A meta-analysis found evidence that the scale's factor structure varies depending on linguistic and cultural factors, and the number of factors ranged from two to nine. [7].
The Swedish version of the GDS-15, translated in 1995, has only undergone partial validation, and there is still a need for comprehensive validation of the entire scale. In one study of the original 30-item version of the GDS that involved stroke patients, the GDS was compared with six other depression rating scales; however, the remaining scales are not commonly used in clinical practice in Sweden today. It showed Pearson correlation coefficients ranging from 0.37 to 0.88 for concurrent validity when comparing GDS to the other scales and 0.75 compared to a clinical measurement of depression severity [8]. A rare study of the Swedish version of the GDS-15 in older adults (aged 75.7 ± 6.1) found a high sensitivity of 94% and specificity of 88% for the cut-off value of ≥ 6 [9] to detect a major depressive episode in 17 of 113 volunteers, but minor depression was not investigated. Further, the test–retest reliability has not been tested in the Swedish version of the GDS-15.
There is a lack of studies among very old adults; one exception is Zhang et al. [10]. While there have been studies investigating the test–retest reliability of the GDS-15 [11, 12] to the best of the authors' knowledge, there is a lack of research utilizing these results to calculate the least significant change.
Aim
This study aims to evaluate the validity and reliability of the Swedish version of the GDS-15 among very old adults ≥ 85 years. This study also examines whether there are differences in the scale depending on subgroups divided by sex, age group, and MMSE scores.
Material and methods
Data source
The sample used in this study was taken from the Umeå85 + /GErontological Regional DAtabase (GERDA) study. This study invited to participate, every second 85-year-old, randomly selected by their odd or even position in the population registry, every 90-year-old, and every 95-year-old or older. Participants were recruited from Umeå, an urban municipality in northern Sweden, and five rural municipalities in the county of Västerbotten. The study started recruiting during 2000–2002 and then every five years until 2017. After five years, previous participants were invited to participate again. In addition, new participants were recruited from the same area. The participants were included irrespective of ongoing treatment with antidepressants.
A convenience sample was collected in 2022 to be used for the test–retest reliability. Individuals from senior citizen organizations, stroke inpatients and outpatients as well as individuals in nursing homes who were above the age of 70 years and lived in the urban municipality of Luleå in the county of Norrbotten were invited to participate.
Participants
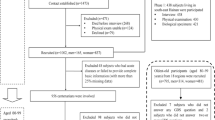
Most participants in the Umeå85 + /GERDA study performed the GDS. Between 2000 and 2002, those with high GDS scores received a new visit within a few days by a physician specialist in geriatric medicine for a depression assessment, which included the Montgomery-Åsberg Depression Rating Scale (MADRS). However, other interviewers who were specifically trained for the task, such as medical students, nurses, or physiotherapists, could have performed the initial GDS assessments, and any ambiguities were settled by senior researchers. Although the scales were conducted on different days, possibly by different interviewers, and the participants were selected based on previous results, it was decided that all 104 participants from 2000–2002 would be included in the present study. This decision considered that the scales were performed within a few days of each other. In 2005, it was decided that the MADRS would be administered by all interviewers who were physicians or medical students who had completed their psychiatric clinical practice and were trained to use the scale. This meant that the MADRS and GDS assessments were performed at the same time by the same interviewer. Between 2000 and 2017, 418 assessments were conducted using the GDS and MADRS. Conradsson et al. [6] showed that GDS-15 scores in individuals who scored 10 or more on the MMSE were valid. Therefore, we removed those with an MMSE score below ten (18 assessments) and those with more than one unanswered GDS item (13 assessments). The remaining 387 assessments constituted the final sample and included 334 individual participants, of whom 46 participated more than once. The assessments were counted as individuals since the time between participation was five years or more.
All participants in the convenience sample were recruited in 2022 and assessed twice by the same author (JN), an experienced geriatrician.
Assessments
The Montgomery-Åsberg Depression Rating Scale (MADRS) was designed in 1978 to be particularly sensitive to changes in depression during treatment [13]. The MADRS includes 10 items, and the version used in this study scored from 0 to 60 points, with higher scores indicating more depressive mood. Kyle et al. used a cut-off score ≤ 12 on the MADRS as "marked recovery" from depression when comparing two antidepressants in elderly depressed patients [14]. However, no consensus has emerged for a specific cut-off score for depression or remission, with scores varying from 4–12 [15]. The scale has shown good reliability and validity, with a sensitivity of 0.80 and specificity of 0.82 among individuals with a mean age of 81 and MMSE scores ≥ 20 points [16]. It is used in Swedish healthcare today to diagnose and detect persons with probable depression due to its close association with DSM-V depression criteria and to follow up on antidepressant treatment.
Cognition was assessed using the frequently used Mini-Mental State Examination (MMSE), which gives a rough estimate of various cognitive functions. The result is stated in points, with 30 as the maximum score. It is often used to express the degree of cognitive impairment, where 18–23 indicates mild impairment and ≤ 17 indicates severe impairment [17].
Cognitive assessment in the convenience sample was made with the Six Item Screener, which is suitable for telephone assessment. The Six Item Screener was chosen since some interviews were conducted over the telephone due to the COVID-19 pandemic. The Six Item Screener is a brief cognitive screening tool for identifying subjects with cognitive impairment. Each item can score one or zero points, and scores below four indicate cognitive impairment, with a sensitivity of 88.7% and specificity of 88.0% [18].
Activities of daily living (ADL) were assessed using the Barthel Index, where 20 points correspond to total independence and 0 points correspond to total dependence [19]. Participants living in nursing homes, including residential homes, nursing homes, and group dwellings for people with dementia disorders, were included.
Statistics
Concurrent validity
Concurrent validity between the GDS and the MADRS was measured using correlation calculations. Spearman's correlation was chosen as the analysis method after a graphical examination, which showed that the data were not normally distributed. A correlation was also examined between the individual items of the GDS and the MADRS.
Cut-off (ROC analysis)
A scatter plot was used to visualize GDS-15 and MADRS scores. As part of our evaluation of the cut-off on GDS, we first needed to determine whether participants were depressed. For this purpose, we compared the MADRS with the DSM-V criteria for depression. The DSM-V requires five or more symptoms where at least one of the symptoms should be either a depressed mood or loss of interest. The symptoms of depressed mood and loss of interest are assessed in MADRS items 1, 2 (depressed mood), and 8 (loss of interest or pleasure). It was decided that participants with two points or more on four MADRS items, including either depressed mood or loss of interest, were considered to have major depression. However, items 6, "concentration difficulties", and 7, "lassitude", were counted as one symptom since they together were considered to assess the DSM-V criterion "diminished ability to think or concentrate, or indecisiveness". We chose four symptoms instead of five, considering that the DSM-V symptom "fatigue or loss of energy nearly every day" is not included in any MADRS item but can be assumed to be highly prevalent in the geriatric population. Participants who scored 2 points or more on one of the MADRS items 1, 2, and 8 but did not meet the criteria of the four symptoms described above were considered to have minor depression.
We used Fisher's r-to-z transformation test, a two-tailed test for independent samples, to compare the correlation coefficients across age groups, sex, and cognition subgroups.
T-tests and Chi-2 tests were conducted to detect significant differences in GDS, MADRS, MMSE, age, and sex between the groups enrolled in the study before or after 2005 since assessments with MADRS between 2000–2002 were made on indication GDS ≥ 5.
We used the Area Under the Curve (AUC) of the Receiver Operating Characteristics (ROC) curve to measure the performance of the GDS. The ROC curve was also used to assess the cut-off value with the highest specificity and sensitivity. AUC and ROC curves for the independent subgroups (sex, age group, and MMSE) were compared to identify significant differences in scale function.
Construct validity (factor analysis)
Factor structure was computed through exploratory factor analysis using principal component analysis. The number of factors was determined using Kaiser's eigenvalue-greater-than-one rule and Cattell's scree plot. Factor loadings were redistributed with direct oblimin rotation to determine which items measure which factors.
Internal reliability
Internal reliability, or consistency, demonstrates whether items of a scale measure the same construct and was analyzed by calculating Cronbach's alpha. Item-total correlation evaluates how an item correlates with the scale's total score. A correlation less than 0.2 indicates that the item might measure something other than the scale as a whole [20]. The scale was also tested to see if alpha increased when an item was removed, which is used to validate the items.
Test–retest
Test–retest reliability was analyzed with correlation, Cohen’s weighted kappa, and Intraclass Correlation Coefficients (ICC). Cohen’s Kappa was deemed according to the following criteria: moderate (0.40–0.59), substantial (0.60–0.79), and outstanding (> 0.80) [21]. Absolute reliability or ICC was deemed according to the following criteria: poor (< 0.5), moderate (0.5–0.75), good (0.75–0.9), and excellent (> 0.9) [22]. The within-subject standard deviation or within-people mean square residual was calculated using ANOVA (the F-test in SPSS’s Scales module was used). The least significant change between the two tests was calculated using within-subject standard deviation multiplied by the \(\sqrt{2}\) and 1.96, the latter to obtain the 95% confidence interval [23, 24, 25]. The least significant change is the minimum score needed to exceed a measurement error for a scale.
All analyses were performed using SPSS. IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp. A two-tailed probability value of ≤ 0.05 was considered significant.
Results
Sample
Table 1 shows that the main sample consisted of 387 individuals with a mean age of 91.0 (± 5.0) years, 65.1% were women, 36.2% were living in nursing homes and 82.4% were living alone. The average number of years in school was 6.7 ± 2.2 and they had an MMSE score of 22.5 (± 5.2). The mean GDS score was 4.0 (± 3.0), 158 individuals (40.8% of the total) had a GDS score ≥ 5 points and the mean MADRS score was 5.0 (± 5.0). The convenience sample consisted of 60 individuals with a mean age of 80.7 (± 5.4) years, 40% were women, 20% were living in nursing homes and 46.7% were living alone. The average number of years in school was 10.5 ± 3.5 and the average Six Item Screener was 4.4 (± 1.6). The mean GDS was 3.2 (± 3.4) for the first assessment and 3.3 (± 3.4) for the second assessment. On the first assessment, there were 13 individuals (21.7%) who had a GDS score ≥ 5 points and on the second assessment 14 (23.3%).
We considered the main sample of 387 assessments to be different individuals since they had been conducted at least five years apart. There were 46 participants in the main sample with two different assessments five years apart and removal of one of these yielded similar results for the validity calculations (data not shown). The change in Geriatric Depression Scale for these 46 participants is displayed in additional Fig. 1.

Scatter plot visualizing the main sample participants (N = 387) based on their GDS-15 and MADRS assessments. LEGEND: GDS = Geriatric Depression Scale. MADRS = Montgomery-Åsberg Depression Rating Scale. DSM = Diagnostic and Statistical. Manual of Mental Disorders. Solid line = regression (R2 linear = 0.411). Horizontal line = recommended GDS cut-off ≥ 5 for any depression. Vertical dotted line = suggested MADRS cut-off ≥ 13 points for any depression, commonly used in Sweden
Concurrent validity
Spearman's correlation between the total GDS and MADRS scores showed a correlation coefficient of 0.60, with the results presented in Table 2. Every item in the GDS showed a significant correlation with the total score on the MADRS; the coefficients ranged from 0.11–0.40, except for GDS item 9 ("Do you prefer to stay at home, rather than going out and doing new things?"). In addition, item 9 did not significantly correlate with any of the individual items within the MADRS.
According to the DSM-V, a diagnosis of depression requires the presence of either a depressed mood or a loss of interest. These symptoms are met by MADRS items 1, 2, and 8. Correlation analysis of these items with the total GDS score gave results of 0.52, 0.51, and 0.29, respectively. GDS items that strongly related to these MADRS items were 5 ("Are you in good spirits most of the time?") and 7 ("Do you feel happy most of the time? "), with coefficients ranging from 0.10–0.40.
Based on sex, age group (85, 90, and ≥ 95 years), and MMSE score (10–17, 18–23, and 24–30 points), no significant differences in correlation between GDS and MADRS were shown in any of the groups (data not shown).
Cut-off (ROC analysis)
Figure 1 shows a scatter plot visualizing the main sample participants based on their GDS-15 and MADRS assessments. Major depression, based on the criteria in this study, was distinguished in the area under the curve at a level of 0.90 (see Fig. 2). The recommended cut-off value of ≥ 5 resulted in a sensitivity of 95.2% and a specificity of 65.8%. The positive predictive value (PPV) was 25.3%, and the negative predictive value (NPV) was 99.1%. The sensitivity was 90.5% for the cut-off value ≥ 6, and the specificity was 77.1%. When distinguishing any depression (major and minor) from no depression, a cut-off ≥ 5 showed a sensitivity of 75.0%, specificity of 68.1%, PPV of 38.0%, and NPV of 91.3%. Cut-off ≥ 6 had a sensitivity of 63.8% and a specificity of 78.5%.

Receiver Operating Characteristic (ROC) curve for the main sample (N = 387)
The sensitivity, specificity, PPV, and NPV for the individual subgroups (sex, age group, and MMSE scores) are shown in Table 3. The comparison of AUC for the subgroups showed no significant difference (data not shown).
Construct validity (factor analysis)
The Principal Component Analysis resulted in a Kaiser's eigenvalue over 1 for four factors, with a cumulative variance of 46.8%. Based on Cattell's scree plot, only one factor was validated as significant with a clear "elbow" in the graph. This factor alone accounted for as much as 23.5% of the variance, unlike the other three factors, which only explained between 7.1 and 8.7% separately (data not shown).
Internal reliability
Internal reliability was evaluated with Cronbach's alpha for the main sample; the results are shown in Table 4. Cronbach's alpha for the total scale was 0.73 and corrected item-to-total correlations ranged from 0.07 – 0.49. Items 6, 9, and 10 correlated below 0.2, and removing these items yielded a higher alpha for the total scale. Removal of item 9 caused the highest increase in alpha to 0.74.
Test–retest
Table 4 shows that Cohen’s weighted kappa was 0.71 for the convenience sample, and item kappa varied between 1.0–0.47. The ICC was 0.95 for the whole sample, and the item ICC ranged between 1.0 and 0.64. The item with the lowest kappa and ICC was item 9. The within-people residual mean square was 1.08, and the least significant change was calculated to be 2.99 with a 95% confidence interval.
Discussion
The study has demonstrated good validity and internal reliability of the Swedish version of the GDS-15 among very old adults regardless of sex, age group, or MMSE scores ≥ 10. The scale showed high values for sensitivity and specificity, 95.2% and 65.9%, respectively, when compared to a depression assessment based on MADRS used according to DSM-V. We believe the results were comparable with other studies in this field and find that the Swedish version of GDS-15 is suitable as a screening tool for depression among very old people.
Concurrent validity
Concurrent validity was examined using the Montgomery-Åsberg Depression Rating Scale (MADRS), which has previously demonstrated good validity in measuring depression among individuals with a mean age of 81 and Mini-Mental State Examination (MMSE) scores ≥ 20 points [14]. Spearman's correlation between the two scales showed an acceptable correlation, indicating that the Swedish version of the GDS is also a valid screening tool for depression among the very old.
In the correlation analysis between the total GDS score and MADRS items 1, 2 (depressed mood), and 8 (loss of interest), it appears that the overall GDS scale captures a form of depression characterized by a greater emphasis on "sadness" rather than a focus on "loss of interest". It is also possible that very old adults give up their interests for reasons other than depression and, therefore, they less frequently experience this particular depressive pattern.
Cut-off (ROC curve)
We created a new variable for major and minor depression by utilizing the MADRS to meet the criteria outlined in the DSM-V. We believe this yielded a superior result compared to using a cut-off score for MADRS, since there is no consensus on which cut-off to use for MADRS and, further, DSM-V is often used for diagnosing depression. Additionally, assessments were performed by a physician or trained medical student rather than the participants themselves, and almost all DSM criteria are found in the MADRS.
As shown in Fig. 1, the GDS cut-off ≥ 5 misses very few individuals with major depression but presents some difficulty for those with minor depression. The scatter plot is comparable to a Canadian study comparing GDS with MADRS [26] in a younger sample with a mean age of 75 ± 6.5 years. It can be argued that a lower cut-off would be better for screening since it increases sensitivity and thus further reduces the risk of missing individuals with depression, which was supported by de Craen et al. [27], who argued that a cut-off of ≥ 4 or ≥ 3 would be better when screening for depression. Nevertheless, the sensitivity for the generally recommended cut-off ≥ 5 is so high that a lower cut-off would not increase sensitivity sufficiently compared to the decrease in specificity that this entails. Thus, we argue that the generally recommended cut-off ≥ 5 is also reasonable for the Swedish translation of the GDS-15 when used to screen for both major and minor depression.
Construct validity (factor analysis)
The four-factor model proposed by Kaiser's eigenvalue resulted in factors that were too similar, making them unsuitable for use as distinct factors. Therefore, we propose a one-factor model, as derived from Cattel's Scree plot, which clearly speaks for a one-factor model, and we named that factor "depression". This is comparable with a Chinese study that found a two-factor model according to Kaiser's Eigenvalue. However, factor number two was challenging to interpret and not considered meaningful, and Cattel's Scree plot showed a one-factor model [28].
Internal reliability
The Cronbach's α of 0.73 is comparable to one Swedish GDS-15 study with a Cronbach's α ranging from 0.636 to 0.775, depending on MMSE scores [6]. Other studies have found alpha scores ranging from 0.55 for the Dutch translation [29] to 0.90 for the Iranian translation [30]. The item-total correlation below 0.2 for items 6, 9, and 10 and the increase in alpha when removed may indicate that the items measure something different from the scale as a whole.
GDS item 9 ("Do you prefer to stay at home rather than going out and doing new things?") has, in previous studies, shown low results for item 9 in various analyses [31, 32], indicating that this item measures something other than depression or that it is just not relevant among very old adults. Item 10 ("Do you feel you have more problems with your memory than most?") also showed poor results. An item response theory (IRT) analysis of the Swedish GDS-15 identified item 10 with the highest difficulty, indicating that the item marks an exceptionally high degree of depression [31]. This could explain the low results in this study, as very high GDS scores were rare.
Test–retest
The results show that Cohen’s weighted kappa was substantial, and the ICC was excellent for the GDS-15. Little is known about how sensitive the GDS-15 is to change. The least significant change between two measurements in this study was 2.99 tested with a mean of two days apart, i.e., there must be at least three points between two tests to exceed measurement error on an individual level. However, the clinically relevant change between the two measurements might be larger. On average, two days between testing in this study seems suitable to detect measurement errors and not change in mood.
Strengths and weaknesses
Few studies on GDS have been performed among very old adults. However, we know that depression becomes more common with age, and this age group will benefit significantly from having a well-functioning screening scale for depression. Therefore, a strength of this study is the high age of our study sample compared to previous studies [26, 32].
The large number of assessments included in the study is another strength.
A weakness of this study is that we compared GDS to a different assessment scale instead of a physician-established diagnosis of depression. However, MADRS was performed by trained professionals and compared to DSM-V criteria for a depression assessment, which is often the case in clinical settings. Additionally, the MADRS needs to be better studied among very old adults.
Conclusion
The Swedish version of the GDS-15 showed good validity and internal reliability for screening for depression in very old adults, ≥ 85 years, with no difference regarding sex, age groups, or MMSE scores ≥ 10. The generally recommended cut-off value of ≥ 5 seems reasonable for use with the Swedish translation.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due to General Data Protection Regulation (GDPR) and ethical approval used in this study but are available from the corresponding author on reasonable request.
References
United Nations. World Population Prospects - Population Division 2022 [cited 2022–05–30]. Available from: https://population.un.org/wpp/default.aspx?aspxerrorpath=/wpp/Graphs/Probabilistic/PopPerc/65plus/900.
Luppa M, Sikorski C, Luck T, Ehreke L, Konnopka A, Wiese B, et al. Age- and gender-specific prevalence of depression in latest-life–systematic review and meta-analysis. J Affect Disord. 2012;136(3):212–21.
Bergdahl E, Gustavsson JM, Kallin K, von Heideken WP, Lundman B, Bucht G, et al. Depression among the oldest old: the Umeå 85+ study. International psychogeriatrics / IPA. 2005;17(4):557–75.
Sheikh J, Yesavage J. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;5:165–72.
Pocklington C, Gilbody S, Manea L, McMillan D. The diagnostic accuracy of brief versions of the Geriatric Depression Scale: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2016;31(8):837–57.
Conradsson M, Rosendahl E, Littbrand H, Gustafson Y, Olofsson B, Lövheim H. Usefulness of the Geriatric Depression Scale 15-item version among very old people with and without cognitive impairment. Aging Ment Health. 2013;17(5):638–45.
Kim G, DeCoster J, Huang CH, Bryant AN. A meta-analysis of the factor structure of the Geriatric Depression Scale (GDS): the effects of language. Int Psychogeriatr. 2013;25(1):71–81.
Agrell B, Dehlin O. Comparison of six depression rating scales in geriatric stroke patients. Stroke. 1989;20(9):1190–4.
Pellas J, Damberg M. Accuracy in detecting major depressive episodes in older adults using the Swedish versions of the GDS-15 and PHQ-9. Ups J Med Sci. 2021;126(1):e7848–5.
Zhang C, Zhang H, Zhao M, Chen C, Li Z, Liu D, et al. Psychometric properties and modification of the 15-item geriatric depression scale among Chinese oldest-old and centenarians: a mixed-methods study. BMC Geriatr. 2022;22(1):144.
Kieffer KM, Reese RJ. A Reliability Generalization Study of the Geriatric Depression Scale. Educ Psychol Measur. 2002;62(6):969–94.
Pedraza O, Dotson VM, Willis FB, Graff-Radford NR, Lucas JA. Internal Consistency and Test-Retest Stability of the Geriatric Depression Scale-Short Form in African American Older Adults. J Psychopathol Behav Assess. 2009;31(4):412–6.
Montgomery SA, Åsberg M. A New Depression Scale Designed to be Sensitive to Change. Br J Psychiatry. 1979;134(4):382–9.
Kyle CJ, Petersen HE, Overø KF. Comparison of the tolerability and efficacy of citalopram and amitriptyline in elderly depressed patients treated in general practice. Depress Anxiety. 1998;8(4):147–53.
Zimmerman M, Chelminski I, Posternak M. A review of studies of the Montgomery-Asberg Depression Rating Scale in controls: implications for the definition of remission in treatment studies of depression. Int Clin Psychopharmacol. 2004;19(1):1–7.
Engedal K, Kvaal K, Korsnes M, Barca ML, Borza T, Selbaek G, et al. The validity of the Montgomery-Aasberg depression rating scale as a screening tool for depression in later life. J Affect Disord. 2012;141(2–3):227–32.
Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922–35.
Callahan CM, Unverzagt FW, Hui SL, Perkins AJ, Hendrie HC. Six-Item Screener to Identify Cognitive Impairment among Potential Subjects for Clinical Research. Med Care. 2002;40(9):771–81.
Collin C, Wade DT, Davies S, Horne V. The Barthel ADL Index: a reliability study. Int Disabil Stud. 1988;10(2):61–3.
Streiner D, Norman GR, Cairney J. Health measurement scales : a practical guide to their development and use. 5th ed. New York: Oxford University Press. 2015.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–74.
Koo TK, Li MY. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med. 2016;15(2):155–63.
Conradsson M, Lundin-Olsson L, Lindelöf N, Littbrand H, Malmqvist L, Gustafson Y, et al. Berg Balance Scale: Intrarater Test-Retest Reliability Among Older People Dependent in Activities of Daily Living and Living in Residential Care Facilities. Phys Ther. 2007;87(9):1155–63.
Lövheim H, Lundman B, Nygren B. Absolute reliability of the Resilience Scale. J Nurs Meas. 2012;20(3):258–60.
Bland JM, Altman DG. Measurement error Bmj. 1996;313(7059):744.
Herrmann N, Mittmann N, Silver IL, Shulman KI, Busto UA, Shear NH, et al. A validation study of The Geriatric Depression Scale short form. Int J Geriatr Psychiatry. 1996;11(5):457–60.
de Craen AJ, Heeren TJ, Gussekloo J. Accuracy of the 15-item geriatric depression scale (GDS-15) in a community sample of the oldest old. Int J Geriatr Psychiatry. 2003;18(1):63–6.
Chiu HF, Lee HC, Wing YK, Kwong PK, Leung CM, Chung DW. Reliability, validity and structure of the Chinese Geriatric Depression Scale in a Hong Kong context: a preliminary report. Singapore Med J. 1994;35(5):477–80.
van de Rest O, van der Zwaluw N, Beekman AT, de Groot LC, Geleijnse JM. The reliability of three depression rating scales in a general population of Dutch older persons. Int J Geriatr Psychiatry. 2010;25(10):998–1005.
Malakouti SK, Fatollahi P, Mirabzadeh A, Salavati M, Zandi T. Reliability, validity and factor structure of the GDS-15 in Iranian elderly. Int J Geriatr Psychiatry. 2006;21(6):588–93.
Johansson S, Lövheim H, Olofsson B, Gustafson Y, Niklasson J. A clinically feasible short version of the 15-item geriatric depression scale extracted using item response theory in a sample of adults aged 85 years and older. Aging Ment Health. 2022;26(2):431–7.
Wongpakaran N, Wongpakaran T, Kuntawong P. Evaluating hierarchical items of the geriatric depression scale through factor analysis and item response theory. Heliyon. 2019;5(8):e02300.
Acknowledgements
The authors wish to acknowledge everyone who contributed to data collection and those who participated for their time and commitment.
Funding
Open access funding provided by Umea University. The study was funded by The Swedish Research Council (grant no. K2014– 99X-22610–01–6); a regional agreement between Umeå University and Västerbotten County Council on cooperation in the fields of medicine, odontology and health; Norrbotten County Council; the Research Foundation of the Faculty of Medicine and Odontology at Umeå University; the Swedish Dementia Association; Strategic Research Area Health Care Science (SFO-V), the European Union and the Regional Development Fund: the Interreg IIIA Mitt-Scandia and the Bothnia-Atlantica Program. The funders had no role in the study design, data collection, analysis, preparation of the manuscript or decision to publish. Open-access funding was provided by Umea University. Funders had no role in trial design, data collection, analysis, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the conception and design and/or acquisition of data and/or analysis and interpretation of data; participated in drafting the article or revising it critically for important intellectual content; and gave final approval of the version to be submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The potential participants for the Umeå85 + /GERDA project were first sent a letter with information about the study and later telephoned to receive their informed consent for participation. If there were any concerns regarding individuals' ability to provide informed consent, consent was discussed with their next of kin. The interviews were conducted by specially trained physicians or medical students and between 2000 and 2002, also by physiotherapists or nurses in the participants' homes. Participants were allowed to intermit or terminate the interview at any time. For both samples, if the screening instruments showed signs of depressive disorder, they were either encouraged to contact their physician or a referral was sent. Ethical approval was obtained from the Regional Ethical Review Board in Umeå, Sweden (99–326, 05–063 M, 09–178 M, 2015–296-31 M, 2016–501-32 M, 2020–01428, and 2021–00023).
For the convenience sample, the majority were asked directly for their consent to participate, at senior citizen gatherings, or at consultation meetings with the geriatrician who then assessed them. For nursing home residents, the nurse in charge of the nursing home selected suitable residents and asked for their permission to be visited by the assessor. Then, the assessor visited them and asked for their consent to participate. If previously unknown symptoms of depression were found, the participant was referred to their physician, or if suitable, treatment was offered directly by the geriatrician. Ethical approval for the convenience sample was obtained from the Swedish Ethical Review Authority (2021–05968-01).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
Cite this article
Snellman, S., Hörnsten, C., Olofsson, B. et al. Validity and test–retest reliability of the Swedish version of the Geriatric Depression Scale among very old adults. BMC Geriatr 24, 261 (2024). https://doi.org/10.1186/s12877-024-04869-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-024-04869-7