
Abstract
Background
No previous study has assessed the association between oxidative balance score (OBS) and dietary phytochemical index (DPI) with colorectal cancer (CRC) simultaneously. Therefore, this study investigated the association between OBS and DPI with the odds of CRC among the Iranian population.
Methods
This hospital-based age and sex-matched case–control study was conducted between September 2008 and January 2010 (142 controls and 71 cases were entered for analysis). New diagnosed CRC cases were selected from the Cancer Institute, Imam Khomeini Hospital of Tehran. Dietary intakes were determined by a semi-quantitative food frequency questionnaire (FFQ). Then, dietary indices were calculated by food items and nutrient intake. Logistic regression was utilized for assessing the tertiles of OBS and DPI.
Results
In multivariate analysis, OBS was associated with a 77% reduction in CRC odds in the last tertile than the first tertile (odds ratio (OR) = 0.23, confidence interval (CI): 0.07–0.72, Ptrend = 0.017). Also, we found a 64% reduction in CRC odds in the last tertile of DPI compared to the first tertile (OR = 0.36, CI: 0.15–0.86, Ptrend = 0.015).
Conclusions
A diet rich in phytochemicals and anti-oxidants, including fruits and vegetables (citrus fruits, colored berries, and dark-green leafy vegetables) and whole grains, may reduce the CRC odds.
Similar content being viewed by others

Background
Colorectal cancer (CRC) is the third most common cancer worldwide [1]. CRC is a multifactorial disease with modifiable (diet, smoking, and sedentary lifestyle) and non-modifiable (age, sex, family history, and race) determinants [2, 3]. Lifestyle and diet could positively or negatively affect CRC and play a significant role in its prevention [4]. High intakes of specific vitamins (including vitamins E, D, and C) and micronutrients (Ca, Mg, Zn, and Se) have been shown to protect against CRC. In contrast, alcohol consumption, high iron intake, and smoking exacerbate this condition [5].
It has been found that oxidative stress, an imbalance between pro-oxidant and anti-oxidant status, plays a key role in CRC pathogenesis [2, 6]. Oxidative stress induces macromolecular (protein, lipids, and deoxyribonucleic acid (DNA)) damage [7], which can subsequently provoke mutagenesis and carcinogenesis [8, 9]. Therefore, oxidative balance score (OBS) has been introduced to indicate the overall exposure balance of pro-oxidant and anti-oxidant [10]. A higher score of OBS indicates a higher exposure to anti-oxidants than pro-oxidants [5]. Previous studies have demonstrated an inverse association between OBS and CRC [11, 12]. To our knowledge, no study has been conducted on the relationship between this index and the risk of CRC in the Middle-Eastern population. Dietary intake of the Middle-Eastern population has its unique pattern: large portion sizes with high consumption of refined grains (bread and white rice) and a greater percentage of energy from carbohydrates [13].
Moreover, epidemiological studies have shown the protective effects of fruit and vegetable-rich diets against CRC, mainly attributed to their phytochemical content [14]. Phytochemicals are known as non-nutritive bioactive compounds (including phenolic compounds, isoprenoids, and organosulfur compounds) [15] with anti-cancer properties, which affect cancer initiation, promotion, and progression through anti-oxidant properties, anti-inflammatory activities, and regulation of cellular signaling pathways [16]. The phytochemical load of a diet is obtained by the dietary phytochemical index (DPI), calculated as the percentage of daily energy intake derived from phytochemical-rich foods [17]. A reverse association between DPI score and various diseases has been shown in previous studies, including obesity [18, 19], insulin resistance [15], stroke [20], knee osteoarthritis [21], and breast cancer [16, 22]. To our knowledge, studies have not yet simultaneously demonstrated the effect of OBS and DPI on CRC odds. Therefore, this study investigated the association between OBS and DPI with the odds of CRC among Iranian population.
Methods
Study population
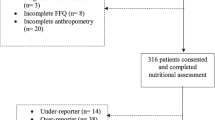
This hospital-based study was done at the Cancer Institute, Imam Khomeini Hospital of Tehran. Our study was conducted between September 2008 and January 2010. The sample size was calculated based on the previous study [23], considering the odds ratio (OR) = 0.45, α = 0.05, β = 0.2. The patients who had no previous diagnosis of cancer more than six months prior to the interview were included. The participants were between 40–75 years old and had no diagnosis of cancer elsewhere or a family history of adenomatous polyposis. Patients with acute and non-neoplastic diseases admitted to the same hospital were chosen as controls. Each case was matched for age (five-year classifications) and sex with two controls. At first, 267 patients were selected (178 controls and 89 cases). Fifty-four patients were removed from the study due to unwillingness, total energy intake (out of mean ± 3 standard deviations (SDs)), and incomplete food frequency questionnaire (FFQ) (Fig. 1). Finally, 142 controls and 71 cases were entered into the analysis. Some details of this study have been published previously [24].

Flow chart of the study
Dietary assessment
Dietary intakes were determined by a semi-quantitative FFQ. The validity of FFQ has been assessed among Iranian adults [25]. In this interview, a valid food album [26] for the convenience of participants was used. After calculating the gram of foods, the Nutritionist IV (version 7.0; N-Squared Computing, Salem, OR, USA) was utilized to calculate energy and intake of nutrients.
Dietary indices
Based on a method by Goodman et al. [27], the OBS was determined by collecting data from four classes: dietary pro-oxidants like saturated fatty acids (SFAs) [25, 25], polyunsaturated fatty acids (PUFAs), and iron; non-dietary pro-oxidants such as smoking and obesity; non-dietary anti-oxidant such as physical activity; and dietary anti-oxidants for example fiber, vitamin C, vitamin B9, vitamin E, selenium, zinc, and beta-carotene [6, 8, 28,29,30]. Every score of these 13 components was summed, and the range of total score was between 0–26 (Table 1).
According to a method developed by McCarty [17], the DPI was calculated by this formula: [DPI = (phytochemical-rich foods / total food intake) × 100]. Foods included fruits, vegetables, legumes, whole grains, soy products, nuts, olives, olive oil, spices, tea, and coffee. Natural fruit and vegetable juices were included in the fruit and vegetable groups, respectively, due to their phytochemical content.
Socio-demographic and anthropometric assessments
Some information like physical activity, socio-demographic specifications, history of having CRC in their families, smoking habits, and medication use were collected by questionnaires. Anthropometric indices such as weight and height were measured. The international physical activity questionnaires (IPAQ) were utilized to evaluate the physical activity level [31].
Statistical analysis
SPSS (version 23.0) was utilized for statistical analysis. The normality of data was determined by the Kolmogorov–Smirnov test. Mean (SD) or median (interquartile range (IQR)) was used for continuous variables, and the percentage was used for categorical variables. For categorical variables, the chi-square test was used; for continuous variables, independent samples T-test and Mann–Whitney were applied. Crude and adjusted models of logistic regression were utilized to assess the tertiles of OBS and DPI. The level of statistical significance was tested with a p-value < 0.05. Also, R software (version 3.0.2) was used for all figures' depictions.
Results
Table 2 shows the basic characteristic of the case and control groups. Based on this table, OBS, DPI, vegetables, fruits, SFA, PUFA, fiber, vitamin E, vitamin C, beta-carotene, history of CRC, taking aspirin, and acetaminophen were significantly different between the case and control groups.
Macronutrient and food intake across the tertiles of OBS and DPI are shown in Figs. 2, 3, 4 and 5. According to Fig. 2, participants in the last tertile of OBS had a higher significant intake of carbohydrates, SFA, monounsaturated fatty acids (MUFAs), and PUFA compared to the first tertile (P˂0.001 for all). But, according to Fig. 3, macronutrient intake was not significant between DPI tertiles. Compared to the first tertile, participants in the last tertile of OBS had higher significant consumption of refined grains (P˂0.001), vegetables (P˂0.001), processed meats (P = 0.008), dairy (P˂0.001), and vegetable oils (P = 0.01) (Fig. 4). Also, participants in the last tertile of DPI had higher consumption of whole (P˂0.001) and refined grains (P = 0.001), fruits (P˂0.001), vegetables (P˂0.001), fish, and poultry (P = 0.003), in comparison to the first tertile (Fig. 5).

The contribution of macronutrient intake based on OBS tertile

The contribution of macronutrient intake based on DPI tertile

The consumption of food groups based on OBS tertile

The consumption of food groups based on DPI tertile
In multivariate analysis (Table 3), the OBS was associated with a 77% lower odds for CRC in the last tertile than the first tertile (Ptrend = 0.017). Furthermore, we detected a 64% significant reduction in the odds of CRC in the last tertile of DPI compared to the first tertile (Ptrend = 0.015).
Discussion
The present study showed that OBS and DPI were associated with a significant reduction in CRC odds.
In agreement with our findings, a cohort study with a 10-year follow-up among 80,063 Americans and the Iowa Women's Health Study involving 33,736 women aged 55 to 69 years revealed an inverse association between OBS and the risk of colon cancer [6, 32]. Furthermore, two observational studies conducted in the United States (US) reported a negative association between OBS and colorectal adenoma risk [11, 12]. These studies were conducted in the US, which cannot be generalized to other populations due to dietary and environmental differences. The present study is the first study conducted in the Middle East. Anti-oxidants are divergent in terms of their chemical structure and biological characteristics. Anti-oxidants can inhibit proliferation, induce apoptosis and regulate the nuclear factor kappa B (NF-κB) and mitogen-activated protein kinase (MAPK) pathways, which can lead to cell death in cancer cells [33].
Our results demonstrated that higher DPI scores were significantly associated with lower CRC odds. To our knowledge, no previous study has assessed the association between DPI score and CRC. Regarding chronic disease, meta-analyses have revealed that higher adherence to DPI is associated with a lower risk of overweight/obesity [34], hypertension, hypertriglyceridemia, and metabolic syndrome [35]. In our study, participants in the highest DPI had a higher intake of whole grains, fruits, vegetables, fish, and poultry and a lower intake of refined grains than the lowest tertile. It indicates that their diet has more phytochemical content and anti-oxidant properties to act against cancer. Phytochemicals have been shown to modulate these pathways by neutralizing oxidative stress, inhibiting the NF-kB pathway, suppressing MAPK/extracellular signal regulated-kinases (ERK), and increasing the activation of caspase 3 [36].
According to World Health Organization (WHO), one-third to half of the cancer deaths could be prevented by lifestyle modification, including diet, weight management, exercise, and avoiding tobacco and alcohol consumption [37]. Diet has a bidirectional effect on the development of CRC [38]. A high intake of fruits, vegetables, whole grains, and dairy products, along with a low intake of red and processed meats, was associated with reduced CRC risk [39]. Also, a review study has shown that following a healthy pattern, represented by a high intake of whole grains, vegetables, fruits, legumes, nuts, seafood, and dairy products, reduces the risk of CRC [40]. Furthermore, an inverse association has been found between adherence to plant-based diet index (PDI) and CRC [41]. Dietary factors that have been proposed for their anti-cancer properties involve phytochemicals (polyphenols, flavonoids, alkaloids, etc.) [42], anti-oxidants (beta-carotene), probiotics, omega-3, and vitamins [43]. It has been found that cell cycle, apoptosis, and signaling pathways are altered in various types of cancer.
The present study has several strengths. Several potential confounders were included in the analysis to reach an independent association. A valid and reliable FFQ was used for measuring dietary intakes. Also, there were several limitations in the study. First, the case–control study cannot show a causal relationship between the variables. Second, FFQ is based on memory and a subjective approach to evaluating diet, which may lead to measurement errors.
Conclusions
In conclusion, following a diet rich in phytochemicals and anti-oxidants, including fruits and vegetables (citrus fruits, colored berries, and dark-green leafy vegetables), and whole grains, may reduce the CRC odds. Further prospective studies and randomized clinical trials are warranted to confirm the association between DPI and OBS with CRC. It is also suggested that future studies consider the effects of a diet rich in anti-oxidants on the endogenous oxidative stress pathway in CRC.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CRC:
-
Colorectal cancer
- DPI:
-
Dietary phytochemical index
- OBS:
-
Oxidative balance score
- FFQ:
-
Food frequency questionnaire
- DNA:
-
Deoxyribonucleic acid
- SFA:
-
Saturated fatty acids
- MUFA:
-
Monounsaturated fatty acids
- PUFA:
-
Polyunsaturated fatty acids
- IPAQ:
-
International physical activity questionnaires
- IQR:
-
Interquartile range
- NF-κB:
-
Nuclear factor kappa B
- MAPK:
-
Mitogen-activated protein kinase
- PDI:
-
Plant-based diet index
- ERK:
-
Extracellular signal regulated-kinases
- WHO:
-
World health organization
References
Favoriti P, Carbone G, Greco M, Pirozzi F, Pirozzi RE, Corcione F. Worldwide burden of colorectal cancer: a review. Updates Surg. 2016;68:7–11.
Rafiee P, Shivappa N, Hébert JR, Jaafari Nasab S, Bahrami A, Hekmatdoost A, Rashidkhani B, Sadeghi A, Houshyari M, Hejazi E. Dietary inflammatory index and odds of colorectal cancer and colorectal adenomatous polyps in a case-control study from Iran. Nutrients. 2019;11(6):1213.
Ali A, Manzoor MF, Ahmad N, Aadil RM, Qin H, Siddique R, et al. The burden of cancer, government strategic policies, and challenges in Pakistan: A comprehensive review. Front Nutr. 2022:1553:1–17.
Ganesan K, Jayachandran M, Xu B. Diet-derived phytochemicals targeting colon cancer stem cells and microbiota in colorectal cancer. Int J Mol Sci. 2020;21(11):3976.
Zhang W, Peng S-F, Chen L, Chen H-M, Cheng X-E, Tang Y-H. Association between the Oxidative Balance Score and Telomere Length from the National Health and Nutrition Examination Survey 1999–2002. Oxid Med Cell Longev. 2022;2022:1–11.
Dash C, Bostick RM, Goodman M, Flanders WD, Patel R, Shah R, Campbell PT, McCullough ML. Oxidative balance scores and risk of incident colorectal cancer in a US prospective cohort study. Am J Epidemiol. 2015;181(8):584–94.
Cho A, Kwon Y-J, Lim H-J, Lee HS, Kim S, Shim J-Y, Lee H-R, Lee Y-J. Oxidative balance score and serum γ-glutamyltransferase level among Korean adults: a nationwide population-based study. Eur J Nutr. 2018;57(3):1237–44.
Lakkur S, Goodman M, Bostick RM, Citronberg J, McClellan W, Flanders WD, Judd S, Stevens VL. Oxidative balance score and risk for incident prostate cancer in a prospective US cohort study. Ann Epidemiol. 2014;24(6):475-478. e474.
Manzoor MF, Arif Z, Kabir A, Mehmood I, Munir D, Razzaq A, Ali A, Goksen G, Coşier V, Ahmad N. Oxidative stress and metabolic diseases: Relevance and therapeutic strategies. Front Nutr. 2022;9:994309–994309.
Goodman M, Bostick RM, Dash C, Flanders WD, Mandel JS. Hypothesis: oxidative stress score as a combined measure of pro-oxidant and antioxidant exposures. Ann Epidemiol. 2007;17(5):394–9.
Kong SYJ, Bostick RM, Flanders WD, McClellan WM, Thyagarajan B, Gross MD, Judd S, Goodman M. Oxidative Balance Score, Colorectal Adenoma, and Markers of Oxidative Stress and InflammationOxidative Balance Score and Markers of Oxidative Stress. Cancer Epidemiol Biomark Prev. 2014;23(3):545–54.
Labadie J, Goodman M, Thyagarajan B, Gross M, Sun Y, Fedirko V, Bostick RM. Associations of oxidative balance-related exposures with incident, sporadic colorectal adenoma according to antioxidant enzyme genotypes. Ann Epidemiol. 2013;23(4):223–6.
Esmaillzadeh A, Azadbakht L. Major dietary patterns in relation to general obesity and central adiposity among Iranian women. J Nutr. 2008;138(2):358–63.
Johnson IT. Phytochemicals and cancer. Proceedings of the Nutrition Society. 2007;66(2):207–15.
Bahadoran Z, Mirmiran P, Tohidi M, Azizi F. Dietary phytochemical index and the risk of insulin resistance and β-cell dysfunction: a prospective approach in Tehran lipid and glucose study. Int J Food Sci Nutr. 2015;66(8):950–5.
Bahadoran Z, Karimi Z, Houshiar-Rad A, Mirzayi H-R, Rashidkhani B. Dietary phytochemical index and the risk of breast cancer: a case control study in a population of Iranian women. Asian Pac J Cancer Prev. 2013;14(5):2747–51.
McCarty MF. Proposal for a dietary “phytochemical index.” Med Hypotheses. 2004;63(5):813–7.
Asgari E, Jayedi A, Firouzabadi FD, Noruzi Z, Farazi M, Djafarian K, Shab-Bidar S. Association of the dietary phytochemical index with general and central obesity in a sample of Iranian adults. JFF. 2021;83:104546.
Eslami O, Khoshgoo M, Shidfar F. Dietary phytochemical index and overweight/obesity in children: a cross-sectional study. BMC Res Notes. 2020;13(1):1–5.
Rigi S, Mousavi SM, Shakeri F, Keshteli AH, Benisi-Kohansal S, Saadatnia M, Esmaillzadeh A. Dietary phytochemical index in relation to risk of stroke: a case-control study. Nutr Neurosci.. 2022;25(11):2239–46.
Amirkhizi F, Ghoreishy SM, Hamedi-Shahraki S, Asghari S. Higher dietary phytochemical index is associated with lower odds of knee osteoarthritis. Sci Rep. 2022;12(1):1–8.
Ghoreishy SM, Aminianfar A, Benisi-Kohansal S, Azadbakht L, Esmaillzadeh A. Association between dietary phytochemical index and breast cancer: a case–control study. Breast Cancer. 2021;28(6):1283–91.
Terry P, Giovannucci E, Michels KB, Bergkvist L, Hansen H, Holmberg L, Wolk A. Fruit, vegetables, dietary fiber, and risk of colorectal cancer. J Natl Cancer Inst. 2001;93(7):525–33.
Kahrizsangi MA, Ebrahimi Z, Shateri Z, Mansouri F, Zangene A, Rajabzadeh-Dehkordi M, Nouri M, Rashidkhani B. Carbohydrate quality indices and colorectal cancer risk: a case-control study. BMC Cancer. 2023;23(1):347.
Mirmiran P, Esfahani FH, Mehrabi Y, Hedayati M, Azizi F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 2010;13(5):654–62.
Ghaffarpour M, Houshiar-Rad A, Kianfar H. The manual for household measures, cooking yields factors and edible portion of foods. Tehran: Nashre Olume Keshavarzy. 1999;7(213):42–58.
Goodman M, Bostick RM, Dash C, Terry P, Flanders WD, Mandel J. A summary measure of pro-and anti-oxidant exposures and risk of incident, sporadic, colorectal adenomas. Cancer Causes Control. 2008;19(10):1051–64.
Slattery ML, John EM, Torres-Mejia G, Lundgreen A, Lewinger JP, Stern MC, Hines L, Baumgartner KB, Giuliano AR, Wolff RK. Angiogenesis genes, dietary oxidative balance and breast cancer risk and progression: the Breast Cancer Health Disparities Study. Int J Cancer. 2014;134(3):629–44.
Slattery ML, Lundgreen A, Torres-Mejia G, Wolff RK, Hines L, Baumgartner K, John EM. Diet and lifestyle factors modify immune/inflammation response genes to alter breast cancer risk and prognosis: the Breast Cancer Health Disparities Study. Mutat Res/Fund Mol Mech Mutagenesis. 2014;770:19–28.
Nouri M, Soltani M, Rajabzadeh-Dehkordi M, Rafieipour N, Askarpour M, Najafi M, Faghih S. Dietary Antioxidant Capacity Indices are Negatively Correlated to LDL-Oxidation in Adults. Int J Clin Pract. 2023;2023:5446163.
Biernat E, Stupnicki R, Lebiedziński B, Janczewska L. Assessment of physical activity by applying IPAQ questionnaire. Phys Educ Sport. 2008;52(2):83–9.
Mao Z, Prizment AE, Lazovich D, Gibbs DC, Bostick RM. Dietary and Lifestyle Oxidative Balance Scores and Incident Colorectal Cancer Risk among Older Women; the Iowa Women’s Health Study. Nutr Cancer. 2021;73(11–12):2323–35.
Gothai S, Muniandy K, Gnanaraj C, Ibrahim IAA, Shahzad N, Al-Ghamdi SS, Ayoub N, Veeraraghavan VP, Kumar SS, Esa NM. Pharmacological insights into antioxidants against colorectal cancer: A detailed review of the possible mechanisms. Biomed Pharmacother. 2018;107:1514–22.
Wei C, Liu L, Liu R, Dai W, Cui W, Li D. Association between the Phytochemical Index and Overweight/Obesity: A Meta-Analysis. Nutrients. 2022;14(7):1429.
Mehranfar S, Jalilpiran Y, Ejtahed H-S, Seif E, Shahrestanaki E, Mahdavi-Gorabi A, Esmaeili-Abdar M, Larijani B, Qorbani M: Association of dietary phytochemical index with cardiometabolic risk factors. Int J Vitam Nutr Res 2022.
Ayaz M, Nawaz A, Ahmad S, Mosa OF, EisaHamdoon AA, Khalifa MA, Sadiq A, Ullah F, Wadood A, Kabra A. Underlying anticancer mechanisms and synergistic combinations of phytochemicals with cancer chemotherapeutics: potential benefits and risks. J Food Qual. 2022;2022:1–5.
Marbini MH, Amiri F, Hezaveh ZS. Dietary glycemic index, glycemic load, insulin index, insulin load and risk of diabetes-related cancers: A systematic review of cohort studies. Clinical Nutrition ESPEN. 2021;42:22–31.
Chen H, Liu RH. Potential mechanisms of action of dietary phytochemicals for cancer prevention by targeting cellular signaling transduction pathways. J Agric Food Chem. 2018;66(13):3260–76.
Schwingshackl L, Knüppel S, Michels N, Schwedhelm C, Hoffmann G, Iqbal K, De Henauw S, Boeing H, Devleesschauwer B. Intake of 12 food groups and disability-adjusted life years from coronary heart disease, stroke, type 2 diabetes, and colorectal cancer in 16 European countries. Eur J Epidemiol. 2019;34(8):765–75.
Tabung FK, Brown LS, Fung TT. Dietary patterns and colorectal cancer risk: a review of 17 years of evidence (2000–2016). Curr Colorectal Cancer Rep. 2017;13(6):440–54.
Wu B, Zhou R-L, Ou Q-J, Chen Y-M, Fang Y-J, Zhang C-X. Association of plant-based dietary patterns with the risk of colorectal cancer: a large-scale case–control study. Food Funct. 2022;13(20):10790–801.
Zheng Z, Zhang L, Hou X. Potential roles and molecular mechanisms of phytochemicals against cancer. Food Funct. 2022;13(18):9208–25.
Andreescu N, Puiu M, Niculescu M. Effects of dietary nutrients on epigenetic changes in cancer. Cancer Epigenetics Precision Med. 2018;1856:121–139.
Acknowledgements
We sincerely thank all field investigators, staff, and participants of the present study.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
S.B, F.D, A.A, Z.S, M.A.K, and E.T; Contributed to writing the first draft. M.N and B.R; Contributed to all data and statistical analysis, and interpretation of data. M.N and B.R.; Contributed to the research concept, supervised the work, and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki and was approved by the Medical Research and Ethics Committee of Shiraz University of Medical Science (IR.SUMS.SCHEANUT.REC.1401.011). All participants read and signed the informed consent form.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bentyaghoob, S., Dehghani, F., Alimohammadi, A. et al. Oxidative balance score and dietary phytochemical index can reduce the risk of colorectal cancer in Iranian population. BMC Gastroenterol 23, 183 (2023). https://doi.org/10.1186/s12876-023-02826-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-023-02826-z