
Abstract
Background
Few studies assess the link between plant-based diets and colorectal cancer (CRC) incidence. To our knowledge, no study has examined the association between pro-vegetarian dietary pattern (PDP) and CRC globally or among Iranians. Therefore, the objective of our matched case-control study was to evaluate the association between PDP and CRC in the Iranian population.
Methods
The present research was a hospital-based case (n = 71)-control (n = 142) study conducted in the same hospitals in Tehran, Iran. This study used a reliable and valid semi-quantitative food frequency questionnaire to evaluate the participants’ dietary intake. According to the residual method, the selected plant and animal foods have been adjusted in the total energy intake to calculate the PDP index. Odds ratios (ORs) and 95% confidence intervals (CIs) adjusted for confounding variables were also expressed using logistic regression by SPSS software.
Results
In the crude and adjusted models, we observed that the odds of CRC decreased significantly in the 3rd and last quartile of PDP compared to the 1st quartile (Q) (Crude model: Q3: OR = 0.36, 95% CI: 0.17 − 0.79, P-value = 0.011 and Q4: OR = 0.33, 95% CI: 0.14 − 0.79, P-value = 0.012 - Adjusted model: Q3: OR = 0.41, 95% CI: 0.18 − 0.94, P-value = 0.035 and Q4: OR = 0.35, 95% CI: 0.14 − 0.87, P-value = 0.025).
Conclusions
Based on the results of the present case-control study in the Iranian population, it was concluded that PDP, which involves consuming vegetables, fruits, cereals, dairy products, and low meat consumption, reduces the odds of CRC. In conclusion, adherence to PDP is associated with a decreased odds of CRC.
Similar content being viewed by others

Introduction
Colorectal cancer (CRC) is an invasive and malignant disease in which the rectum and colon cells grow out of control [1]. In the world, CRC is the second and third most frequent cancer among women and men, respectively [2]. Even though there are more screening tests (mainly colonoscopies), CRC is still the third leading cause of cancer-related death worldwide [3]. CRC is also the third most common cause of death in Iran and has been on an upward trend over the past 25 years, particularly in younger populations [4].
Lifestyle factors, diet, age, and family history have been found to play a role in the pathogenesis of CRC [1]. Modifiable lifestyle factors contributing to the risk of CRC include consuming fewer fruits and vegetables, consuming more red meat, drinking more alcohol, smoking, consuming less calcium, being inactive, and having other diseases like obesity and type 2 diabetes [5]. To determine nutritional status, dietary patterns that include different food groups and their interactions between themselves and not individual foods should be used [6].
Nowadays, people are becoming more interested in the pro-vegetarian dietary pattern (PDP), which is based on consuming more plant- and less animal-based foods [7]. PDP and plant-based diets are known to be beneficial for non-communicable diseases such as cardiovascular disease [8], hypertension [9], type 2 diabetes [10], and cancer [11]. To assess adherence to a PDP distinct from complete vegetarianism, an overall PDP index was created for the first time, weighing both animal- and plant-derived foods [12]. Due to decreased meat consumption (especially red and processed meat) and increased high-fiber foods, PDP may be associated with a lower risk of CRC [13]. Additionally, plant-based diets are associated with lower body mass index (BMI) [14, 15], and there is strong evidence linking higher adiposity to an increased risk of CRC [16]. However, plant-based diets in Britain have not been associated with reduced CRC incidence [17]. Additionally, studies have shown that vegetarian diets are associated with lower rates of gastrointestinal cancers and overall cancer incidence but not with lower overall cancer death rates [18, 19]. On the other hand, the results of a previous cohort study showed that meat consumption was associated with an increased risk of colon cancer. In contrast, legume consumption was associated with a lower risk [15].
Examining dietary patterns rather than individual nutrients is recommended to clarify the relationship between diet and health [20]. Also, most available studies on cancers and dietary patterns have been collected from developed countries, with almost two-thirds of these studies being conducted in Europe or North America [21]. To our knowledge, no study has examined the association between PDP and CRC globally or among Iranians. Therefore, our matched case-control study aimed to investigate the association between PDP and CRC in the Iranian population.
Methods
Study population
The present research was a case-control study that was conducted in 19 CRC surgery departments of Imam Khomeini Hospital’s Cancer Organization and three general hospitals in Tehran, Iran (from September 2008 to January 2010). Participants who had the following conditions were included in the study as cases (convenience sampling): definite diagnosis of CRC for six months before the interview, ages between 40 and 75 years at the time of diagnosis, no history of inflammatory bowel disease and familial adenomatous polyposis and other cancers.
The subjects of the control group were randomly selected from the patients hospitalized in the same hospitals due to acute and non-neoplastic disorders such as joint and disc disorders, sprains, and fractures. Each case was age- and sex-matched with two control subjects.
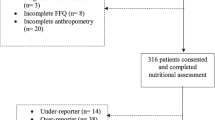
Based on the sample size obtained from the previous study [22], 89 cases and 178 controls were included in the current study. Then, after excluding 54 participants due to unwillingness to cooperate, incomplete food frequency questionnaire (FFQ), and excessive intake of total energy (out of mean ± 3 standard deviations (SDs)), 71 cases and 142 controls were included in the final analysis. Some details of the present study have been previously published [23].
Dietary intake
This study used a 168-item semi-quantitative FFQ to evaluate the participants’ dietary intake, the reliability and validity of which had been previously assessed [24]. A trained dietitian completed the questionnaire through a face-to-face interview. Participants ' dietary intake in the previous year was estimated using a valid food album and standard measurement tools [25]. Finally, after converting participants’ daily dietary intake into grams, we used Nutritionist IV (N IV) to estimate energy and nutrient intake [26].
PDP
According to the residual method, the selected plant and animal foods were adjusted in the total energy intake to calculate the PDP index. Potatoes, olive oil, nuts, cereals, legumes, vegetables, and fruits were considered as plant sources, and meat products, animal fat, eggs, fish, and dairy products were categorized as animal sources. After that, all plant and animal components were converted into a quantile score, and then a reverse score was considered for the quantiles of animal components. Finally, the value of the reverse quantile of animal sources and direct quantile of plant sources were calculated. After determining the values of these plant and animal foods, the final PDP score (between 12 and 60) was calculated [7].
Assessment of covariates
A general information checklist was used to collect the participants’ general information, including family history of CRC, history of drug use, and socio-demographic characteristics. Smoking status was classified as never, former, or current. Those who had never smoked or had smoked less than 100 cigarettes in their lifetime were considered never smokers. Former smokers were considered those who had quit smoking at the time of the interview and had smoked at least 100 cigarettes in their lifetime. Current smokers were defined as those who currently smoke and have smoked at least 100 cigarettes in their lifetime. Anthropometric parameters, including weight, height, and waist-to-hip ratio (WHR), were evaluated through standard methods. Also, each participant’s BMI was calculated. The level of physical activity was determined using an International Physical Activity Questionnaire (IPAQ), previously validated in the Iranian population [27].
Statistical analysis
Statistical analyses were performed using a statistical software package (SPSS, version 26). Also, we used R software for all the depicted figures. The dietary intake and basic characteristics of the participants were expressed as mean ± SD (for data with a normal distribution) or median (interquartile range (IQR) for data with a non-normal distribution) and number (percentage) for quantitative and qualitative data, respectively. Independent samples T-test or Mann-Whitney and chi-square were used to compare continuous and categorical variables between two groups, respectively. Analysis of variance (ANOVA) test was used to assess the PDP component intakes across the quartile of this index. Odds ratios (ORs) and 95% confidence intervals (CIs) adjusted for confounding variables were also expressed using logistic regression. The significance level for all findings was considered as a p-value less than 0.05.
Results
According to Table 1, the two case and control groups significantly differed in the history of CRC, WHR, PDP score, fiber intake, and taking aspirin, acetaminophen, and mineral supplements (P < 0.05).
According to Fig. 1, carbohydrate intake was significantly higher and polyunsaturated fatty acids (PUFAs) lower in the last quartile of the PDP score compared to the first one (P = 0.048 and P = 0.045, respectively).

Macronutrient intakes based on the PDP quartiles. PDP: pro-vegetarian dietary pattern, Q: quartile, CHO: carbohydrate, Pro: protein, SFA: saturated fatty acid, PUFA: polyunsaturated fatty acid, MUFA: monounsaturated fatty acid
The consumption of plant and animal sources based on PDP quartiles is presented in Table 2. Fruits (P<0.001), vegetables (P<0.001), nuts (P<0.001), cereals (P = 0.009), legumes (P = 0.009), olive oil (P<0.001), and potato intake (P = 0.006) were significantly higher in the last quartiles of PDP. Compared to the first quartile of the PDP score, animal fat consumption (P<0.001) was significantly lower in the last quartile.
The association between PDP score and CRC odds is shown in Table 3. In the crude and adjusted models, we observed that the odds of CRC decreased significantly in the 3rd and last quartile of PDP compared to the 1st quartile (Q) (Crude model: Q3: OR = 0.36, 95% CI: 0.17 − 0.79, P-value = 0.011 and Q4: OR = 0.33, 95% CI: 0.14 − 0.79, P-value = 0.012 - Adjusted model: Q3: OR = 0.41, 95% CI: 0.18 − 0.94, P-value = 0.035 and Q4: OR = 0.35, 95% CI: 0.14 − 0.87, P-value = 0.025).
Discussion
The present matched case-control study examined PDP as a plant-based dietary pattern to determine whether it is associated with CRC odds in the Iranian population. We observed that a PDP characterized by frequent fruit, vegetable, cereal, and dairy product consumption was associated with a decreased odds of CRC for both men and women.
Previous studies showed the beneficial effects of various plant-based diets, such as a vegetarian diet [28, 29]. However, due to the elimination of animal products in this dietary pattern, sufficient amounts of certain nutrients such as iron, vitamin B12, and long-chain fatty acids (eicosapentaenoic acid and docosahexaenoic acid) are not provided [30]. Some studies have shown a link between a decrease in the intake of the mentioned nutrients and a higher incidence of cancer [31, 32]. Therefore, a PDP diet with a certain amount of meat, fish, egg, and dairy is one of the best alternative diets that provide enough macro- and micronutrients [33].
There has been no research on the relationship between PDP and CRC, so we investigated the relationship between various types of plant-based diets and CRC, and the results of previous studies have been conflicting in this regard [34, 35]. Like our findings, Wirfält et al., in a prospective cohort study of people aged 50 to 71 years (n = 492,306), found that consuming vegetables and fruits reduced CRC risk by 15% [35]. In a case (n = 506)-control (n = 673) study conducted on the Canadian population, Chen et al. identified a plant-based dietary pattern associated with a lower odds of CRC (OR = 0.55) [36]. In the present study, a greater odds reduction was observed between PDP and CRC (OR = 0.35). Additionally, low-meat eaters had a 9% lower CRC risk than regular meat eaters in the prospective analysis of the United Kingdom Biobank study [37]. Findings from a multiethnic cohort study on men (n = 79,952) and women (n = 93,475) showed that a plant-based diet was significantly associated with a lower CRC risk only in men. Because men are more likely to suffer from CRC than women, and these two genders have different dietary habits [38]. Previous studies have shown that whole grains, cereals, or vegetables are inversely associated with cancer risk from the cecum to the rectum, indicating a close relationship between diet and CRC [39]. In line with our results, studies have shown that a healthy plant-based diet was inversely correlated with CRC incidence [40, 41]. Also, a systematic review and meta-analysis of observational studies showed a significant reduction in total cancer incidence among vegans and vegetarians as plant-based diets [42].
In contrast to our results, a case-control study on the Malaysian population (n = 264) showed no significant relationship between a plant-based diet and the risk of CRC [43]. Also, a cohort study found no association between vegetarianism and CRC risk [34]. The definitions of vegetarian and other plant-based diets and the time participants followed their respective diets also varied between studies. A clear conclusion cannot be drawn from the small number of cases of CRC in some dietary groups, such as PDP. However, a Northern German prospective cohort study of 1,404 CRC survivors also showed that compared to the 1st quartile after age and sex adjustment, those in the last quartile of a plant-based diet had lower mortality in survivors of CRC during seven years of follow-up [44].
The benefits of a plant-based diet, particularly PDP, on CRC risk can be attributed to several mechanisms. Many healthy plant foods in the PDP, such as fruits, vegetables, and cereals, contain dietary fiber, polyphenols, carotenoids, lignans, and vitamins E and C [45, 46]. Due to their antioxidant and anti-inflammatory properties, these functional nutritional components can cause tumor cells to undergo apoptosis and reduce CRC incidence [47]. Also, the fiber in the PDP may mitigate the risk of CRC by shortening the time it takes to move through the body and producing short-chain fatty acids [40, 48]. Short-chain fatty acids prevent the onset of infection and cancer by affecting the immune system and gene expression [49].
Moreover, red meat can cause cancer because it contains protein, fat, iron, or heat-induced mutagenic substances [50]. In processed meat, in addition to the mentioned items, salt and nitrite are added during processing [51]. Also, there is evidence that red meat and processed meats produce genotoxic free radicals and lipid peroxidation, which are associated with altered colonic flora and increased risk of CRC [52]. In addition, excessive fat intake can cause weight gain and insulin resistance [50]. As a result, blood sugar, insulin, and insulin-like growth factor 1 (IGF-1) increase, which causes the proliferation of precancerous cells and stops apoptosis [53].
Some studies show the effect of smoking and being overweight on cancer risk [54, 55]. In our research, all participants were overweight (differences between the BMI of the case and control were not significant), and the impact of BMI and smoking were adjusted in the second model. The association between PDP and CRC was still significant despite considering smoking and BMI in the adjusted model. Therefore, further research is needed to understand the mechanisms underlying our findings.
Strengths and limitations
To our knowledge, this is the first study to address the association between PDP and CRC in an Iranian population and provides up-to-date information to inform public health action for primary prevention. Also, instead of using a single nutrient/food approach as dietary intake and nutritional status indicators, food group analysis was used to investigate dietary patterns.
Selection bias and recall bias were two limitations of case-control studies, so in the present study, we matched both groups based on age and gender to control bias. Although the present study had a relatively small sample size, we selected twice as many people from the control group as the case group. Recall bias was also reduced by a validated FFQ and trained interviewers who were unaware of the study’s hypotheses.
In this study, assessing the long-term effects of risk factors on CRC rates was impossible. A cohort or longitudinal study is a better way to determine the association of lifestyle factors with long-term diseases such as cancer. Also, one of the main limitations of the current study was its hospital-based design.
Conclusions
Based on the results of the present case-control study in the Iranian population, it was concluded that PDP, which includes the consumption of vegetables, fruits, cereals, and dairy products and low meat consumption, reduces the odds of CRC. In conclusion, adherence to PDP is associated with a reduced odds of CRC.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Gupta S. Screening for Colorectal Cancer. Hematol Oncol Clin N Am. 2022;36(3):393–414.
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. Cancer J Clin. 2022;72(1):7–33.
Morgan E, Arnold M, Gini A, Lorenzoni V, Cabasag C, Laversanne M, Vignat J, Ferlay J, Murphy N, Bray F. Global burden of Colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut. 2023;72(2):338–44.
Arani SH, Kerachian MA. Rising rates of Colorectal cancer among younger iranians: is diet to blame? Curr Oncol. 2017;24(2):131–7.
Clinton SK, Giovannucci EL, Hursting SD. The world cancer research fund/American institute for cancer research third expert report on diet, nutrition, physical activity, and cancer: impact and future directions. J Nutr. 2020;150(4):663–71.
Veettil SK, Wong TY, Loo YS, Playdon MC, Lai NM, Giovannucci EL, Chaiyakunapruk N. Role of Diet in Colorectal Cancer incidence: Umbrella Review of Meta-analyses of prospective observational studies. JAMA Netw open. 2021;4(2):e2037341.
Martínez-González MA, Sánchez-Tainta A, Corella D, Salas-Salvado J, Ros E, Arós F, Gómez-Gracia E, Fiol M, Lamuela-Raventós RM, Schröder H. A provegetarian food pattern and reduction in total mortality in the Prevención Con Dieta Mediterránea (PREDIMED) study. Am J Clin Nutr. 2014;100(suppl1):320S–8.
Lee S, Quiambao AL, Lee J, Ro J, Lee E-S, Jung S-Y, Sung M-K, Kim J. Dietary inflammatory index and risk of Breast cancer based on hormone receptor status: a case-control study in Korea. Nutrients. 2019;11(8):1949.
Kim H, Rebholz CM, Garcia-Larsen V, Steffen LM, Coresh J, Caulfield LE. Operational differences in plant-based diet indices affect the ability to detect associations with incident Hypertension in middle-aged US adults. J Nutr. 2020;150(4):842–50.
Satija A, Bhupathiraju SN, Rimm EB, Spiegelman D, Chiuve SE, Borgi L, Willett WC, Manson JE, Sun Q, Hu FB. Plant-based dietary patterns and incidence of type 2 Diabetes in US men and women: results from three prospective cohort studies. PLoS Med. 2016;13(6):e1002039.
Hardt L, Mahamat-Saleh Y, Aune D, Schlesinger S. Plant-based diets and Cancer Prognosis: a review of recent research. Curr Nutr Rep 2022:1–22.
Martínez-González MA, Sánchez-Tainta A, Corella D, Salas-Salvadó J, Ros E, Arós F, Gómez-Gracia E, Fiol M, Lamuela-Raventós RM, Schröder H. A provegetarian food pattern and reduction in total mortality in the Prevención Con Dieta Mediterránea (PREDIMED) study. Am J Clin Nutr. 2014;100(suppl1):320S–8.
Rizzo NS, Jaceldo-Siegl K, Sabate J, Fraser GE. Nutrient profiles of vegetarian and nonvegetarian dietary patterns. J Acad Nutr Dietetics. 2013;113(12):1610–9.
Fraser GE. Diet, life expectancy, and chronic Disease: studies of Seventh-Day Adventists and other vegetarians. Oxford University Press; 2003.
Orlich MJ, Singh PN, Sabaté J, Fan J, Sveen L, Bennett H, Knutsen SF, Beeson WL, Jaceldo-Siegl K, Butler TL. Vegetarian dietary patterns and the risk of colorectal cancers. JAMA Intern Med. 2015;175(5):767–76.
Ma Y, Yang Y, Wang F, Zhang P, Shi C, Zou Y, Qin H. Obesity and risk of Colorectal cancer: a systematic review of prospective studies. PLoS ONE. 2013;8(1):e53916.
Key TJ, Appleby PN, Spencer EA, Travis RC, Roddam AW, Allen NE. Cancer incidence in vegetarians: results from the European prospective investigation into Cancer and Nutrition (EPIC-Oxford). Am J Clin Nutr. 2009;89(5):1620S–6.
Tantamango-Bartley Y, Jaceldo-Siegl K, Fan J, Fraser G. Vegetarian diets and the incidence of Cancer in a low-risk PopulationCancer and Vegetarian diets. Cancer Epidemiol Biomarkers Prev. 2013;22(2):286–94.
Orlich MJ, Singh PN, Sabaté J, Jaceldo-Siegl K, Fan J, Knutsen S, Beeson WL, Fraser GE. Vegetarian dietary patterns and mortality in Adventist Health Study 2. JAMA Intern Med. 2013;173(13):1230–8.
Safari A, Shariff ZM, Kandiah M, Rashidkhani B, Fereidooni F. Dietary patterns and risk of Colorectal cancer in Tehran Province: a case–control study. BMC Public Health. 2013;13(1):1–9.
Hajizadeh B, Rashidkhani B, Rad AH, Moasheri SM, Saboori H. Dietary patterns and risk of oesophageal squamous cell carcinoma: a case–control study. Public Health Nutr. 2010;13(7):1107–12.
Terry P, Giovannucci E, Michels KB, Bergkvist L, Hansen H, Holmberg L, Wolk A. Fruit, vegetables, dietary fiber, and risk of Colorectal cancer. J Natl Cancer Inst. 2001;93(7):525–33.
Kahrizsangi MA, Ebrahimi Z, Shateri Z, Mansouri F, Zangene A, Rajabzadeh-Dehkordi M, Nouri M, Rashidkhani B. Carbohydrate quality indices and Colorectal cancer risk: a case-control study. BMC Cancer. 2023;23(1):347.
Mirmiran P, Esfahani FH, Mehrabi Y, Hedayati M, Azizi F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 2010;13(5):654–62.
Ghaffarpour M, Houshiar-Rad A, Kianfar H. The manual for household measures, cooking yields factors and edible portion of foods. Tehran: Nashre Olume Keshavarzy. 1999;7(213):42–58.
Nutritionist I. N-squared computing. Silverton: Nutritionist IV 1998.
Biernat E, Stupnicki R, Lebiedziński B, Janczewska L. Assessment of physical activity by applying IPAQ questionnaire. Phys Educ Sport. 2008;52(2):83–9.
Hargreaves SM, Rosenfeld DL, Moreira AVB, Zandonadi RP. Plant-based and vegetarian diets: an overview and definition of these dietary patterns. Eur J Nutr. 2023;62(3):1109–21.
Dybvik JS, Svendsen M, Aune D. Vegetarian and vegan diets and the risk of Cardiovascular Disease, Ischemic Heart Disease and Stroke: a systematic review and meta-analysis of prospective cohort studies. Eur J Nutr. 2023;62(1):51–69.
Burns-Whitmore B, Froyen E, Heskey C, Parker T, San Pablo G. Alpha-linolenic and linoleic fatty acids in the vegan diet: do they require dietary reference intake/adequate intake special consideration? Nutrients. 2019;11(10):2365.
Siriwardhana N, Kalupahana NS, Moustaid-Moussa N. Health benefits of n-3 polyunsaturated fatty acids: eicosapentaenoic acid and docosahexaenoic acid. Adv Food Nutr Res. 2012;65:211–22.
Parra-Soto S, Ahumada D, Petermann-Rocha F, Boonpoor J, Gallegos JL, Anderson J, Sharp L, Malcomson FC, Livingstone KM, Mathers JC. Association of meat, vegetarian, pescatarian and fish-poultry diets with risk of 19 cancer sites and all cancer: findings from the UK Biobank prospective cohort study and meta-analysis. BMC Med. 2022;20(1):1–16.
Asfura-Carrasco D, Santiago S, Zazpe I, Gómez-Donoso C, Bes-Rastrollo M, Martínez-González MÁ. Healthful and unhealthful provegetarian food patterns and micronutrient intake adequacy in the SUN cohort. Public Health Nutr. 2023;26(3):563–74.
Gilsing AM, Schouten LJ, Goldbohm RA, Dagnelie PC, van den Brandt PA, Weijenberg MP. Vegetarianism, low meat consumption and the risk of Colorectal cancer in a population based cohort study. Sci Rep. 2015;5(1):1–12.
Wirfält E, Midthune D, Reedy J, Mitrou P, Flood A, Subar AF, Leitzmann M, Mouw T, Hollenbeck AR, Schatzkin A. Associations between food patterns defined by cluster analysis and Colorectal cancer incidence in the NIH–AARP diet and health study. Eur J Clin Nutr. 2009;63(6):707–17.
Chen Z, Wang PP, Woodrow J, Zhu Y, Roebothan B, Mclaughlin JR, Parfrey PS. Dietary patterns and Colorectal cancer: results from a Canadian population-based study. Nutr J. 2015;14(1):1–9.
Watling CZ, Schmidt JA, Dunneram Y, Tong TY, Kelly RK, Knuppel A, Travis RC, Key TJ, Perez-Cornago A. Risk of cancer in regular and low meat-eaters, fish-eaters, and vegetarians: a prospective analysis of UK Biobank participants. BMC Med. 2022;20(1):1–13.
Kim J, Boushey CJ, Wilkens LR, Haiman CA, Le Marchand L, Park S-Y. Plant-based dietary patterns defined by a priori indices and Colorectal cancer risk by sex and race/ethnicity: the multiethnic cohort study. BMC Med. 2022;20(1):1–14.
Slattery ML, Curtin K, Wolff RK, Herrick JS, Caan BJ, Samowitz W. Diet, physical activity, and body size associations with rectal Tumor mutations and epigenetic changes. Cancer Causes Control. 2010;21:1237–45.
Wang F, Ugai T, Haruki K, Wan Y, Akimoto N, Arima K, Zhong R, Twombly TS, Wu K, Yin K. Healthy and unhealthy plant-based diets in relation to the incidence of Colorectal cancer overall and by molecular subtypes. Clin Translational Med. 2022;12(8):e893.
Wang L, Lo C-H, He X, Hang D, Wang M, Wu K, Chan AT, Ogino S, Giovannucci EL, Song M. Risk factor profiles differ for cancers of different regions of the colorectum. Gastroenterology. 2020;159(1):241–56. e213.
Dinu M, Abbate R, Gensini GF, Casini A, Sofi F. Vegetarian, vegan diets and multiple health outcomes: a systematic review with meta-analysis of observational studies. Crit Rev Food Sci Nutr. 2017;57(17):3640–9.
Abd Rashid AA, Ashari LS, Shafiee NH, Raja Ali RA, Yeong Yeh L, Shahril MR, Jan Mohamed HJ. Dietary patterns associated with Colorectal cancer risk in the Malaysian population: a case–control study with exploratory factor and regression analysis. BMC Public Health. 2023;23(1):1386.
Ratjen I, Enderle J, Burmeister G, Koch M, Nöthlings U, Hampe J, Lieb W. Post-diagnostic reliance on plant-compared with animal-based foods and all-cause mortality in omnivorous long-term Colorectal cancer survivors. Am J Clin Nutr. 2021;114(2):441–9.
Heber D. Vegetables, fruits and phytoestrogens in the prevention of Diseases. J Postgrad Med. 2004;50(2):145.
Zhao Y, Jiang Q. Roles of the polyphenol–gut microbiota interaction in alleviating Colitis and preventing colitis-associated Colorectal cancer. Adv Nutr. 2021;12(2):546–65.
Alam MN, Almoyad M, Huq F. Polyphenols in colorectal cancer: current state of knowledge including clinical trials and molecular mechanism of action. BioMed research international 2018, 2018.
Aune D, Chan DS, Lau R, Vieira R, Greenwood DC, Kampman E, Norat T. Dietary fibre, whole grains, and risk of Colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ 2011, 343.
Smith PM, Howitt MR, Panikov N, Michaud M, Gallini CA, Bohlooly-y M, Glickman JN, Garrett WS. The microbial metabolites, short-chain fatty acids, regulate colonic Treg cell homeostasis. Science. 2013;341(6145):569–73.
Corpet DE. Red meat and colon Cancer: should we become vegetarians, or can we make meat safer? Meat Sci. 2011;89(3):310–6.
Song M, Fung TT, Hu FB, Willett WC, Longo VD, Chan AT, Giovannucci EL. Association of animal and plant protein intake with all-cause and cause-specific mortality. JAMA Intern Med. 2016;176(10):1453–63.
Farvid MS, Sidahmed E, Spence ND, Mante Angua K, Rosner BA, Barnett JB. Consumption of red meat and processed meat and cancer incidence: a systematic review and meta-analysis of prospective studies. Eur J Epidemiol. 2021;36:937–51.
Spencer EA, Key TJ, Appleby PN, Dahm CC, Keogh RH, Fentiman IS, Akbaraly T, Brunner EJ, Burley V, Cade JE. Meat, poultry and fish and risk of Colorectal cancer: pooled analysis of data from the UK dietary cohort consortium. Cancer Causes Control. 2010;21:1417–25.
Arnold M, Leitzmann M, Freisling H, Bray F, Romieu I, Renehan A, Soerjomataram I. Obesity and cancer: an update of the global impact. Cancer Epidemiol. 2016;41:8–15.
Brown KF, Rumgay H, Dunlop C, Ryan M, Quartly F, Cox A, Deas A, Elliss-Brookes L, Gavin A, Hounsome L. The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. Br J Cancer. 2018;118(8):1130–41.
Acknowledgements
We sincerely thank all field investigators, staff, and participants of the present study.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
E.T.N, E.M, F.S, M.M, M.V. and M.N; Contributed to writing the first draft. M.V and A.R; Contributed to all data and statistical analysis, and interpretation of data. Z.S. and B.R.; Contributed to the research concept, supervised the work, and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki. Also, this research was approved by the Medical Research and Ethics Committee of the Shiraz University of Medical Sciences (IR.SUMS.SCHEANUT.REC.1401.011). Informed consent was obtained from all subjects and their legal guardian(s).
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nejad, E.T., Moslemi, E., Souni, F. et al. The association between pro-vegetarian dietary pattern and risk of colorectal cancer: a matched case-control study. BMC Res Notes 16, 326 (2023). https://doi.org/10.1186/s13104-023-06606-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13104-023-06606-6