
Abstract
Background
IgG4-related disease mainly manifests as organomegaly and is accompanied by tissue fibrosis (Mimori, Mod Rheumatol 29(2):213, 2019) which is frequently confused with tumour (Dawei et al., J Gastroenterol Hepatol 29(12):1375–8, 2020). There are few reports with of IgG4-related disease with the first clinical manifestation involving the stomach.
Case presentation
We present the case of 46-year-old male patient with a “stomach tumour” as the first manifestation of IgG4-related disease. Gastroscopy showed a mass in the stomach, however, the pathology result was chronic inflammation with IgG4 positivity. CT scans of abdomen showed that the stomach wall was thick, the head of the pancreas was swollen, and retroperitoneal fibrosis was severe.The serum IgG4 level was 75 g/L (normal range 0.03–2.01 g/L).After treatment with methylprednisolone for one month, the symptoms were greatly relieved.
Conclusions
To reduce the suffering of patients and relieve their financial burden, we should consider the possibility of IgG4-related disease when the initial manifestation is a stomach mass.
Similar content being viewed by others

Background
IgG4-related disease is immune-mediated chronic inflammation that is diagnosed by clinicopathological presentations of enlarged organs, elevation of serum concentrations of IgG4 and pathological findings such as a typical dense lymphoplasmacytic infiltration enriched in IgG4-positive plasma cells, storiform fibrosis, and obliterative phlebitis [1, 2]. Pancreas, kidney, and retroperitoneum are often affected [3]. However, there are few reports of IgG4-related disease involving the stomach.This article analysed a patient with IgG4-related disease who had a “stomach tumor” as the initial manifestation.
Case presentation
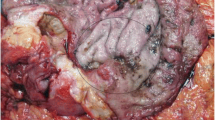
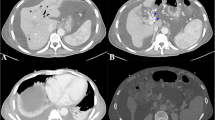
A 46-year-old male patient came to the hospital with discomfort of stomach for half a year and 10 kg weight loss. The patient had no long-term history of heavy alcohol or smoking consumption, and he had no history of hypertension, diabetes, coronary heart disease, or hepatitis, or allergic diseases. The patient had no corresponding family history. Physical examination revealed pigmentation on left anterior tibia skin and swelling of right parotid gland. Patient’s body mass index (BMI) was 18.32 kg/m2. Gastroscopy showed a mass in the stomach (Fig. 1), and the pathology result of the stomach mass biopsy was chronic inflammation with plasmacyte IgG4 positivity (Fig. 2).CT scans of the abdomen showed that the stomach wall was notably thick (Fig. 3), the head of the pancreas was swollen (Fig. 4), and retroperitoneal fibrosis was severe (Fig. 5). The serum IgG4 level was 75 g/L (normal range 0.03–2.01 g/L). The laboratory result showed hemoglobin (Hb), albumin (ALB), alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (AKP), eosinophil (EO) were not in normal range (Table 1).Hepatitis B surface antigen and hepatitis A antibody, hepatitis C antibody, hepatitis E antibody, human immunodefciency virus antibody, anti-nuclear anti-bodies (ANA), anti-smooth muscle antibodies, anti-liver and kidney microsome antibodies, anti-mitochondrial antibodies, anti-myocardial antibodies, anti-parietal cell antibodies and anti-neutrophil cytoplasmic antibodies were all negative. T-spot, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), prothrombin time, D-dimer, white blood cell (WBC), platelet, lymphocyte were all normal. Later, biopsies of the right parotid gland (Fig. 6) and left anterior tibia skin (Fig. 7) were performed. The pathology results showed that tissue fibrosis was obvious in parotid gland and skin. Immunohistochemistry showed more than 50 IgG4-positive plasma cells/HPF. Methylprednisolone (40 mg) was given orally once a day for 2 weeks,and then 32 mg were given orally once a day for the next 2 weeks. After treatment, the patient’s stomach symptoms improved significantly and he gained weight (7.5 kg).Gastroscopy showed that the stomach mass was smaller than before methylprednisolone treatment (Fig. 8), and abdomeninal CT scans showed that the stomach wall was thin (Fig. 9),the head of the pancreas was normal (Fig. 10),and the retroperitoneal fibrosis was significantly reduced (Fig. 11).The serum IgG4 level decreased to 6.55 g/L.The HB, ALB, ALT, AST, AKP and EO level become nomal.

Stomach mass in gastroscopy before the treatment

Gastric mucosa plasmacyte IgG4 positivity with immunohistochemistry

Thick stomach in CT before the treatment

Head pancreas swollen in CT before the treatment

Retroperitoneal fibrosis in CT before the treatment

Right parotid gland plasmacyte IgG4 positivity with immunohistochemistry

Left anterior tibia skin plasmacyte IgG4 positivity with immunohistochemistry

Stomach swollen in gastroscopy after one month treatment

Slightly thickened stomach wall in CT after one month treatment

Head pancreas normal in CT after one month treatment

Retroperitoneum normal in CT after one month treatment
Discussion and conclusions
The reason for IgG4-related disease is unknown, and the pancreas, biliary tract, lymph nodes, lungs, livers, pleura, kidneys and other organs can been involved [4]. When the digestive tract is involved, the symptoms are often complicated. Lopes [5] and Dumas-Campagna [6] reported that IgG4-related disease involving the digestive tract was diagnosed from the symptoms persent for 6 to 10 years. The manifestations of IgG4-related diseases involving the stomach is ulcers with mild inflammation of the surrounding mucosa [7]. In this case, IgG4-related disease involving the stomach was diagnosed from the symptom present for half a year,and the manifestation was bulge hyperplasia under gastroscopy. We referred to the diagnostic criteria of IgG4 in Japan in 2011 [8]: (1) diffuse or characteristic swelling and hypertrophy of single or multiple organs in clinic; (2) elevation of serum IgG4 ≥ 1.35 g/L; (3) significant in histopathological Infiltration and fibrosis of lymphocytes, with an IgG4 positive rate > 40% and > 10 IgG4-positive plasma cells/HPF. This patient met all three criteria and was diagnosed with IgG4-related disease. Zheng [9] reported that the infection rate of Helicobacter pylori in 10 cases of IgG4-related gastric disease was 20% (2/10). Helicobacter pylori was not infected in this case, and whether the level of IgG4 has an antagonistic effect on Helicobacter pylori needs further study. The treatment for IgG4-related disease is based on glucocorticoids, and prednisone 30–40 mg/d orally can induce remission [10]. After treatment with methylprednisolone for 1 month, significant organ improvement was observed. However, IgG4 disease easily recurs and can be aggravated by single glucocorticoid therapy [11]. Therefore, the therapy of this patient should be adjusted according to the patient’s condition.
When IgG4-related disease involves the stomach, the swelling of the stomach is similar to that of a tumour. The results of gastric mucosa biopsy, serum IgG4 level, and organomegaly or tissue fibrosis must be combined to confirm the diagnosis of IgG4-related disease. However, the prospective cohort study showed that Chinese IgG4 disease patients had a 2.78-fold increased risk of having malignancy, and the most common malignancy site was the gastrointestinal tract [12]. IgG4-related disease can create an immunological context that may impair the tumoral immunosurveillance and promote the pancreatic carcinogenesis [13]. Autoimmune pancreatitis was identifed as a potential risk factor for IgG4 related patients having malignancy [3]. Although autoimmune pancreatitis was not found in this patient, due to the potential for malignancy, physicians should be alert to this possibility during follow-up.
We should consider the possibility of IgG4-related disease and alert the potential for malignancy when a mass is seen in the stomach, to reduce the suffering for patients and the financial burden for their families.
Availability of data and materials
The datasets analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- IgG:
-
Immunoglobin G
- CT:
-
Computed tomography
- HPF:
-
High power field
- BMI:
-
Body mass index
- Hb:
-
Hemoglobin
- ALB:
-
Albumin
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- AKP:
-
Alkalinephosphatase
- EO:
-
Eosinophil
- ANA:
-
Anti-nuclear anti-bodies
- ESR:
-
Erythrocyte sedimentation rate
- CRP:
-
C-reactive protein
- WBC:
-
White blood cell
References
Umehara H, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD). Mod Rheumatol. 2011;22:21–30.
Zhang W, Stone JH. Management of IgG4-related disease. Lancet Rheumatol. 2019;1:e55–65.
Liu Y, Jiangnan Fu, Ning X, et al. Malignancy risk of immunoglobin G4-related disease: evidence from a large cohort multicenter retrospective study. Rheumatol Ther. 2021;8(3):1207–21. https://doi.org/10.1007/s40744-021-00326-8.
Wallace ZS, Zhang Y, Perugino CA, et al. Clinical phenotypes of IgG4-related disease: an analysis of two international cross-sectional cohorts. Ann Rheum Dis. 2019;78(3):406–12. https://doi.org/10.1136/annrheumdis-2018-214603.
Lopes J, Hochwald SN, Lancia N, et al. Autoimmune esophagitis: IgG4-related tumor of the esophagus. J Gastrointest Surg. 2010;14(16):1031–4. https://doi.org/10.1007/S11605-010-1172-4.
Dumas-campagna M, Bouchard S, Soucy G, et al. IgG4-related esophageal disease presenting as esophagitis dissecans superficialis with chronic stricture. J Clin Med Res. 2014;6(4):295–8. https://doi.org/10.14740/jocmrl845w.
Tang C, Sivarasan N, Griffin N. Abdominal manifestations of IgG4-related disease: a pictorial review. Insights Imaging. 2018;9(4):437–48. https://doi.org/10.1007/a13244-018-0618-1.
Research Committee to establish diagnostic criteria and development of treatment for systemic IgG4-related disease; Research Committee to establish a new clinical entity, IgG4-related multi-organ lymphoproliferativesydrome(IgG4 4-MOLPS). Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Research Program of Intractable Disease provided by the Ministry of Health, Labor, and Welfare of Japan [Article in Japanese]. Nippon Naika Gakkai Zasshi. 2012;101(3):795–804.
Songbai Z, Xiaowen Li, Li X, et al. Clinical analysis of IgG4-related gastropathy. Chin J Gastroenterol. 2015;20(12):735–9.
Hart PA, Topazian MD, Witzig TE, et al. Treatment of relapsing autoimmune pancreatitis with immunomodulators and rituximab:the Mayo clinic experience. Gut. 2013;62(11):1607–15. https://doi.org/10.1136/gutjnl-2012-302886.
Kamisawa T, Okazaki K, Kawa S, et al. Amendment of the Japanese consensus guidelines for autoimmune pancreatitis. 2013III. Treatment and prognosis of autoimmune pancreatitis. J Gastroentrol. 2014;49(6):981–970. https://doi.org/10.1007/s00535-014-0945-z.
Tang H, Yang H, Zhang P, et al. Malignancy and IgG4-related disease: the incidence, related factors and prognosis from a prospective cohort study in China. Sci Rep. 2020;10(1):4910. https://doi.org/10.1038/s41598-020-61585-z.
Poddighe D. Autoimmune pancreatitis and pancreatic cancer: Epidemiological aspects and immunological considerations. World J Gastroenterol. 2021;27(25):3825–36. https://doi.org/10.3748/wjg.v27.i25.3825.
Acknowledgements
We thank Mr Fu-Long Zhang for his contribution to the data collection and manuscript editing.
Funding
The authors have no source of support or funding to report.
Author information
Authors and Affiliations
Contributions
YDZ and QN W conceptualized and designed the case presentation. JX, YS and XCX performed the data collection. FLZ analyzed and interpreted the data. FLZ and JX drafted and critically revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol conformed to the ethical guidelines of the Declaration of Helsinki and was approved by the ethics review committee of HangZhou XiXi Hospital (202105111003000112851). Written informed consent was obtained from the patient and from all individual participants included in the study. Neither the transplant donor nor the recipient was from a vulnerable population.
Consent for publication
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, F., Xu, J., Zhu, Y. et al. “Stomach mass” as the first manifestation of IgG4-related disease: a case report. BMC Gastroenterol 21, 442 (2021). https://doi.org/10.1186/s12876-021-02013-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-021-02013-y