
Abstract
Background
Cardiometabolic conditions are major contributors to the global burden of disease. An emerging body of evidence has associated access to and surrounding public open spaces (POS) and greenspace with cardiometabolic risk factors, including obesity, body mass index (BMI), hypertension (HTN), blood glucose (BG), and lipid profiles. This systematic review aimed to synthesize this evidence.
Methods
This systematic review was conducted based on the PRISMA guidelines. Four electronic databases including Web of Science, PubMed, Scopus, and Google Scholar were searched for eligible articles published until July 2023. All observational studies which assessed the association of greenspace and POS with cardiometabolic risk factors including obesity, BMI, HTN, BG, and lipid profiles were included and reviewed by two authors independently. Heterogeneity between studies was assessed using the I2 index and Cochrane’s Q test. Random/fixed effect meta-analyses were used to combine the association between greenspace exposure with cardiometabolic risk factors.
Results
Overall, 118 relevant articles were included in our review. The majority of the articles were conducted in North America or Europe. In qualitative synthesis, access or proximity to greenspaces or POS impacts BMI and blood pressure or HTN, BG, and lipid profiles via various mechanisms. According to the random effect meta-analysis, more access to greenspace was significantly associated with lower odds of HTN (odds ratio (OR): 0.81, 95% confidence intervals (CIs): 0.61–0.99), obesity (OR: 0.83, 95% CIs: 0.77–0.90), and diabetes (OR:0.79, 95% CI: 0.67,0.90).
Conclusions
Findings of this systematic review and meta-analysis suggested that greenspace accessibility is associated with some cardiometabolic risk factors. Improving greenspace accessibility could be considered as one of the main strategies to reduce cardiometabolic risk factors at population level.
Similar content being viewed by others


Introduction
Cardiometabolic risk factors (CMRFs) including obesity, hypertension, dysglycaemia, and dyslipidemia are among the main risk factors based on the latest global burden of disease report. Resulting in tremendous expenses and a significant amount of morbidity and mortality worldwide. Thus preventive measures to reduce the imposing threats of CMRFs are highly desirable [1].
Greenspace is hypothesized to improve cardiometabolic health by increasing physical activity, reducing stress, and minimizing exposure to air pollution and noise [2]. Greenspaces are usually defined as a land that is partly or completely covered with grass, trees, shrubs, or other vegetation); such as parks, community gardens, and cemeteries [3].
According to World Health Organization (WHO) reports, in 2016, about 39% of adults over 18 years of age (39% men and 40% women) were reported as overweight [4]. Obesity, as we know, is caused by the imbalance of energy intake and the amount of energy consumed through basic metabolic processes and physical activities [4]. Since pharmacological or surgical treatments for obesity are commonly pricey, complicated, and inaccessible to all patients and they are also not lasting solutions. recent research has focused on environmental risk factors that have contributed to obesity and the modulation of these risk factors [5,6,7,8]. According to a recent review of the evidence supporting a link between access to greenspace and weight, nearly 70% of studies found a positive or weak association between greenspace and obesity-related health indicators [9].
The next leading cause of CVDs is hypertension (HTN) [7]. Community-level behavioral interventions are suggested to be important tools for controlling HTN at the population level [10, 11]. In recent years, an increasing number of epidemiological studies have looked into the link between greenspace and BP [10, 12,13,14,15,16,17,18]. While some studies have reported that more greenspace is associated with lower BP [12], others have been inconclusive [19,20,21].
Dyslipidemia (abnormalities in blood lipids) is another major risk factor for atherosclerotic cardiovascular disease [22]. Dyslipidemia is a global problem and continues to rise in prevalence [23]. Previous studies have shown that higher exposure to greenspaces is likely to reduce the risk of dyslipidemia [23,24,25]. Some epidemiological studies have also looked into the relationship between greenness and blood lipids, but the results have been inconsistent [26, 27].
Type 2 diabetes (T2DM) is another CMRF. In most studies regarding T2DM, most of the attention has been given to individual risk factors such as social determinants [28], health-related behaviors [29], and biological attitudes [30], with little attention paid to the role of the residential environment [31]. Previous research has found a link between the abundance of residential greenspace and a lower risk of T2DM [32,33,34,35,36,37].
It has been previously examined whether greenspace and CMRFs of CVDs are linked independently or simultaneously in a single population or as a systematic review evaluating one of these risk factors [9, 38,39,40,41,42]. To the best of our knowledge, no systematic review has addressed the relationship between greenspace and all of the mentioned CMRFs simultaneously and thoroughly (for example the association between HTN, BG, or lipid profile and greenspace were not evaluated in a systematic review article; hence, an adequate review of recent studies on these CMRFs would be valuable to determine the prognostic effect of greenspace on them as well as CVDs.
Hence, we aimed to systematically review and synthesize the available evidence on the associations between greenspace and CMRFs including obesity, hypertension, diabetes, and dyslipidemia. Moreover, all types of variables (continuous and qualitative) were included in the systematic review.
Materials and methods
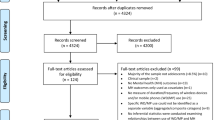
We conducted our systematic review and meta-analyses based on the Preferred Reporting Items for Systematic revReviewsd Meta-analyses (PRISMA) guidelines [43, 44] and all steps were followed according to a predefined protocol. We searched PubMed/MEDLINE, Web of Sciences (ISI), Scopus, and Google Scholar for articles published until July 2023. The main root of search strategies developed based on Exposure to greenspace either by “Proximity”, or “Accessibility” to “greenspace” with CMRFs as continuous (BMI, WC, BP, BG, TG, LDL, HDL, Cholesterol) and categorical outcomes (“obesity, HTN, “diabetes”, “high total cholesterol”, “high triglyceride”, “high LDL, low HDL, dyslipidemia)” (Fig. 1and Table 1). The reference list of relevant articles was reviewed as well to retrieve further eligible studies that were not found through our search.

PRISMA diagram for selection of primary studies about CMRFs and greenspaces
Inclusion and exclusion criteria
We included all observational studies that (1) assessed the link between greenspace with CMRFs such as overweight or obesity; blood pressure or HTN; BG or diabetes; lipid profiles or dyslipidemia. regardless of time, language, methodology, date of publication, and target groups;(2) assessed greenspace exposure using an objective measure (e.g., normalized difference vegetation index [NDVI], a vegetation index that assesses chlorophyll calculated as the ratio of near-infrared minus red light divided by near-infrared plus red light and measured distance to the nearest greenspace) or subjective measure (e.g., self-reported proximity to the nearest park and frequency of visits to parks/greenspaces). Non-human research, review articles or those with duplicate citations were excluded.
Data extraction and quality assessment
The results of the searching process were exported to Endnote X9 (Clarivate Analytics, USA) software. All records’ titles, and abstracts were assessed for relevancy at first, and the irrelevant articles were omitted; then the full texts of the remaining articles were evaluated. The consolidated standards of the Newcastle-Ottawa quality assessment scale (NOS) were used to assess the quality of study design, sampling strategy, and measurement quality [45].
Data were extracted as follows: first author’s name, publication year, place of study, type of study, population, total sample size, mean age, type of measure, and other complementary information. Two independent research experts followed all searches, refinements, quality assessments, and data extraction processes. Any disagreements were resolved through consensus with the third investigator (Kappa statistic for agreement for quality assessment; 0.92).
Statistical analysis
Meta-analysis was performed to estimate the combined effect sizes of (1) proximity, (2) access/availability, and (3) greenspace NDVI on CMRFs. A combined effect size was estimated in cases of more than two reports of the same exposure, outcome, and measure. To combine the association of the aforementioned variables with CMRFs as a dichotomous variable, first the ORs were standardized, and only standardized ORs and their 95% confidence interval (CI) were used as the effect size in the meta-analysis. We standardized the ORs to a 0.1 increase in NDVI, and for proximity to a 1000 m (1 Km) distance to green space by using the formulas described previously by Zhao et al. [46] Heterogeneity was assessed by the I2 and Cochran’s Q tests; if heterogeneity was statistically significant (Cochran’s Q P-value < 0.1), a random-effect model was adopted; otherwise, a fixed-effects was used for analysis. Publication bias was assessed using Egger’s test; if publication bias was significant, sensitivity analysis (trim fill analysis) (16) was performed. A two-tailed p-value below 0.05 was considered statistically significant. Stata version 17 (StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp) was used to analyze the data.
Ethical considerations
The present study was approved by the ethical committee of the Alborz University of Medical Science. All included studies are cited in all reports and complementary extracted publications. We contacted the corresponding author whenever we needed more information about a certain study.
Results
Study selection process and study characteristics
The flowchart summarizes the study selection process for review (Fig. 1). The initial search of the database yielded 3839 hits (PubMed: 2543, Scopus: 936, ISI: 360). Duplicate studies through all databases were removed (n = 2926). After excluding ineligible articles through screening titles and abstracts, a total of 913 articles underwent a full-text evaluation. Finally, 118 articles met the inclusion criteria and were included in our review (i.e.,67 studies evaluated the association between greenspace and BMI, 30 evaluated the relationship between greenspace and HTN, 16 investigated the association between greenspace and BG, and 8 reviewed the association between greenspace and lipid profile or dyslipidemia). A summary description of included studies is presented in Table 1. All articles were published between 2005 and 2023 (50 in the last 5 years) The majority were published in North America (n = 43) [17, 26, 47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87], followed by Europe(n = 41) [12, 16, 21, 25, 88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124], Asia (n = 18) [13,14,15, 23, 27, 32, 35, 125,126,127,128,129,130,131,132,133,134,135], Oceania(n = 9) [136,137,138,139,140,141,142,143,144], South America(n = 6) [145,146,147,148,149,150] and Africa (n = 1) [132]. These studies had sample sizes ranging from 73 to 97,574,613 individuals (total number of participants = 112,719,774). A majority of included studies used cross-sectional design (n = 79, 66.9%), followed by prospective or retrospective cohort designs (n = 29, 24.5%), and some without mentioning the study type (n = 9, 8%). Almost 1/3 of the studies in this review (n = 37, 31.9%) included children as their target group while 45.7% of studies (n = 54) focused on adults. It should be noted that Browning’s study [54], which has the largest population (n = 97,574,613), used data from the US Centers for Disease Control and Prevention. Out of 118 reviewed studies, it has been shown that 49 studies only studied urban areas and 5 studies only include rural areas. 27 studies include both urban and rural areas. 4 studies have focused on urban and suburban areas. Only one study, in addition to the urban and rural areas, had also examined the suburbs. 32 studies have not mentioned the scope of the study as urban and rural and the scope of one study was unknown (Table 1).
Characterizing exposure to greenspace
The majority of studies included in this review considered the proximity(distance to nearest greenspace) of the parks and greenspaces (n = 39, 37.8%) or (accessibility/availability) to greenspaces (n = 39, 37.8%); eighteen studies evaluated greenness and its density using normalized difference vegetation index (NDVI) [23, 27, 52, 54, 75, 83, 84, 112,113,114,115,116, 130,131,132,133, 143, 151]; The most commonly used methods to measure the greenspace characteristics were Geographic Information System (GIS), and Global Positioning System (GPS) (n = 53, 51.4%).
The association between greenspace and weight status
Accessibility or greenness of greenspace and weight status
Overall, 31 articles (46.2%) [48,49,50, 52,53,54, 58, 61,62,63,64, 66,67,68,69, 75, 77, 78, 82, 92, 93, 96, 97, 102, 104, 108, 127, 138, 140, 147, 150] assessed accessibility to greenspace as a measurement, and these studies looked at the relationship between accessibility to greenspace and BMI in distinct target populations. Eight of the 31 studies (25.8%) [52, 54, 63, 67, 77, 97, 104, 140] found a negative association between BMI and access to greenspace Accessibility. Other studies in this review found no significant association between access to greenspace and BMI, as shown in the table (Supplementary Table 1). Some reviewed studies revealed varying effect sizes for subgroups such as men and women, low-income versus high-income populations, and various BMI sub-groups.
Proximity to greenspace and weight status
Proximity to nearby greenspaces was reported in 34 (50.7%) of the reviewed studies on BMI. Eight (23.5%) of the studies looked at the proximity of greenspace within a one-kilometer radius of the participant’s homes, and these studies found a negative correlation between BMI and proximity to greenspace [51, 59, 65, 70, 71, 76, 128, 141].
The association between greenspace and HTN
Accessibility or greenness of greenspace and HTN
Eleven articles evaluated accessibility to greenspace as a parameter [12,13,14, 16, 18, 25, 26, 47, 89, 90, 139], and these studies assessed the relationship between accessibility to greenspace and HTN in different target groups. Almost all of these studies revealed a negative relationship between HTN and access to greenspace (Supplementary Table 2).
Proximity to greenspace and HTN
Three (n = 3) [15, 17, 137] of the five studies [15, 17, 88, 129, 137] that examined the relationship between proximity to greenspaces and HTN or cardiovascular health status found a positive relationship between lower proximity and higher blood pressure.
The association between greenspace and blood glucose
Among all included studies (n = 16) that investigated the association between greenspace and BG levels or diabetes mellitus (DM), thirteen studies (81.2%) used the diagnosis criteria for DM by fasting plasma glucose(FPG) or HbA1c level, and the remaining studies reported incidence or mortality attributed to DM (Supplementary Table 3).
Proximity, accessibility to greenspace or greenness and blood glucose
Eleven studies that assessed the association of BG or diabetes with greenspace (i.e., proximity, greenness or accessibility) showed a negative association between greenspace and blood glucose level or diabetes status, and three studies found a positive association between these variables [31, 139, 152].
The association between greenspace and lipids
Four studies (50.0%) among eight included studies assessed the relationship between public greenspaces and dyslipidemia, while the remaining studies investigated the association of greenspaces with a mean level of lipid profile (Supplementary Table 4).
Accessibility or greenness of greenspace and blood lipids
Five studies that assessed the association of dyslipidemia with greenspace (i.e., proximity, greenness or accessibility) showed a negative association between greenspace and dyslipidemia [23, 26, 27, 132, 151], and two studies found a positive association between these variables [116, 139].
Quantitative synthesis
The combined standardized ORs of the association between greenspace and CMRFs are shown in Table 2. Our meta-analysis indicated that access to green space was associated with decreased the odds of DM by 21% (OR:0.79 95% CI (0.67,0.90)), HTN by 19% (OR:0.81 95%CI (0.61,1.00)) and obesity by 17% (OR:0.83 95%CI (0.77,0.90)). Moreover, 0.1-unit change in the mean NDVI and 1Km difference in NDVI decreased the odds of HTN by 9 and 21%, (OR: 0.91 95%CI (0.88,0.94)) and (OR:0.79 95%CI (0.61,0.98)) respectively. Proximity of 1Km and 15-minute walk to green space decreased the odds of obesity by 3% (OR: 0.97 95% CI (0.94,0.99)) and 51% (OR: 0.49 95%CI (0.02,0.99)) respectively.
Publication bias
Publication bias was assessed across studies assessing greenspace and CMRFs. However, no publication bias was seen among the studies (P > 0.05).
Discussion
In this paper to the best of our knowledge, we reviewed for the first time studies based on access to greenspaces and public open spaces (POS) and their associations to cardiometabolic risk factors such as obesity, HTN, dyslipidemia and diabetes. Considering we are experiencing an epidemic of cardiometabolic risk factors, primarily in metropolitan regions with fewer outside activities, this is a novel study that examines the relationship between access to POS and greenspaces and CMRFs. This is indeed a new area of research, so this report pointed out exclusively 118 papers, nearly half (n = 57, 55.3%) of which were published in the last six years (2016_2022). All the other studies, except for eleven [49, 52, 53, 58, 60, 80,81,82, 97, 104, 108] were carried out over the last decade. This matter demonstrates that, given the worldwide obesity epidemic and the hot topic of the related cause of this epidemic, our review topic depicted one associated probable environmental etiology of obesity. In this review, we also looked at HTN as a leading cause of cardiovascular disease and major mortality, as well as the impact of greenspace and POS on other important CMRFs like BG, diabetes, lipid profile levels and dyslipidemia. This systematic review comprised 118 studies from 13 countries, with developed countries accounting for 91.3% (74 papers). More than half of the articles reviewed (51.1%) identify and analyze correlations between greenspace and obesity or being overweight. The current review is among the first systematic reviews to look at the effect of greenspace proximity or accessibility on individuals’ BMI, HTN, DM, and dyslipidemia in recent years (Fig. 2). Around half of the papers (36 out of 67) observed no significant relationship or some weak or mixed corroboration of an association between greenspace and BMI, 19 out of 67 confirmed a negative relation with BMI, and 6 papers revealed a positive association with BMI (Fig. 3a).

Association between greenspace exposure and cardiometabolic risk factors in reviewed articles. NS/NR = not significant/not reported

a: Association between greenspace and Body mass index (BMI), b: Association between greenspace and Hypertension (HTN),c: Association between greenspace and blood glucose(BG),d: Association between greenspace and lipid profiles in reviewed articles
Moreover, eleven studies found a negative relationship between HTN and greenspace; five studies found a positive relationship (Fig. 3b). Furthermore, eleven studies found a negative relationship between BG or DM and greenspace, three studies found a positive relationship, and the remaining studies that assessed BG or DM found no significant relationship between these two indicators (Fig. 3c). These papers with uncertain results were removed from the review during the study selection process, or if they met the inclusion criteria, they did not provide strong evidence of the relationship between greenspace and BMI or HTN. By the results of our meta-analysis, green space access reduced the odds of diabetes mellitus by 21%, hypertension by 19%, and obesity by 17%.
Health and food literacy and association with greenspace accessibility
The findings revealed that parents with a low Health literacy were nearly twice as likely to report that their newborn spent time in front of the television, and three times more likely to report excessive daily “tummy time [153].”
The study found that adolescents who were members of sports groups had a greater health literacy than nonmembers, independent of age or gender [153].
The majority of the studies reviewed found a positive connection between health literacy and physical activity, which can be explained by the fact that people with higher levels of health literacy have the skills and capabilities to engage in a variety of personal health-enhancing behavior, such as regular physical activity [153,154,155]. This could also have explained the link between health literacy and greenspace utilization for physical activities and outdoor exercises.
Studies indicate that children’s and parents’ misperceptions regarding their children’s weight are caused by a lack of parent-child communication about health issues, unhealthy weight self-management behaviors, and a delayed approach to weight problems and late interventions [156, 157].
Efforts should be directed toward developing school-based programs that assess children’s weight and accurately communicate their nutritional status to both children and parents, as well as actions to improve food literacy and physical activity literacy, making better use of available green spaces and open public spaces (POS), to mitigate the youth obesity epidemic and lower cardiometabolic risk factors.
The resemblance with systematic reports and viewpoints
Greenspaces and BMI
Seven prior pieces of the literature identified a connection between greenspace and overweight/obesity [38, 39, 41, 158,159,160] (Fig. 3a). Dunton et al. published a systematic review of the relationship between the physical environment and childhood obesity in 2009 [39]. In two cross-sectional studies of 245,000 Australian adults over 45 years old, an increasing proportion of land in the neighborhood covered by greenspace was associated with a lower risk of overweight, obesity, and diabetes [10]. Only 13 studies were found to evaluate the relationship between greenspaces and individuals’ weight status in a review study published in England, the majority of which were performed in the United States [11].
This study also determines the built and biophysical environmental variables that are linked to childhood obesity and physical activity levels. Using fifteen eligible studies on this topic, we found that childhood obesity and physical environmental variables differed depending on gender, age, socioeconomic status, population density, whether the reports were made by children themselves or their parents. Obesity outcomes in adolescents were associated with access to equipment and facilities, neighborhood patterns, and urban sprawl, according to this review. This study found no association between the number/distance to parks, as well as the presence of parks, and BMI [39]. Lachowycz et al. [9] reviewed 16 studies on greenspace and obesity. The majority of the studies reviewed in this article yielded inconclusive results regarding the relationship between greenspace access and obesity-related health indicators. Several studies have also revealed some variables that may influence this relationship, such as age, socioeconomic status, and greenspace measurement. This review looked at studies that primarily used BMI as a weight status indicator [9].
D-Mackenbach et al. published a review on obesogenic environments in 2014. Five databases were systematically searched for studies published between 1995 and 2013. This systematic review discovered two components: urban sprawl and land use mix, which are Inextricably linked to weight status [160]. Greenness and its health benefits were reviewed by James et al. in 2015 [159]. This review revealed relatively solid evidence for a positive connection between greenness and physical activity and a less consistent negative relation between greenness and body weight [159]. Maike Schulz et al. performed a systematic review of the build-up environment and health in Germany in 2018. This study examined 25 papers relating to the use of sport-related physical activities; however, it was not related to body composition [158].
Sabine Jean-Louis et al. published a systematic review of the relationship between greenspace access and obesity in 2018. This review has illustrated that 80% of the studies assessed; have shown a positive correlation between these two [41]. Ya-Na Luo et al. published a systematic review and meta-analysis on greenspace and obesity in 2020. This review looked at a total of 57 studies on the subject. More than half of these studies identified a connection between greenspace and lower levels of overweight/obesity [38]. In comparison, the study results of our systematic review point in the same direction as the findings of previous reviews. The majority of previous reviews assess levels of physical activity, but this is not the main character in our review. Other reviews have evaluated the anthropometric parameters of weight status, but the main character in our study was BMI, and other variables were not reviewed in our evaluation. As a result, we reviewed 45 studies on the relationship between greenspace and BMI. The evaluation revealed that in these studies, greenspace is defined as access to greenspace and proximity to greenery. The BMI was our primary parameter for assessing weight status in adults, adolescents, and children. Our review primarily uses OR reports to assess the relationship between BMI and greenspace. As a result, we believe that our systematic review evaluates previous studies on this topic, as well as our tables and documentation in our findings; 19 studies found a significant negative relationship between BMI and greenspace measurements [51, 52, 62, 63, 65, 67, 70,71,72, 74, 76, 77, 106, 136, 145, 149, 161, 162]. These findings indicated that increased access to greenspace could lead to lower BMI, but inconsistency in the age groups of the studies reviewed and different covariates make widespread generalization difficult. The same probably applies to previous research. Previous studies on greenspace and its effect on BMI produced contradictory results. Our findings also revealed the same inconsistency, which was most likely caused by measurement heterogeneity.
Greenspaces and HTN
This review compiled indications of the associations between greenspace and HTN (or blood pressure). We evaluated 30 articles on the topic of HTN and greenspace in this review. A systematic review of greenspace and health in Mainland China investigated the association between health status, mental health, weight status, cardiometabolic outcomes, and greenspace. Seven of the 14 studies in this review looked at HTN as a cardiometabolic outcome, and all of the cross-sectional studies found a negative relationship between HTN and greenspace measurements [42] (Fig. 3b). Almost all of the articles reviewed were published within the last four years (2016–2020). Furthermore, more than half of the studies (n = 9, 60%) were conducted in Europe or The United States, while one-third were conducted in Asia or Oceania. (n = 5, 33.3%) One study included in this review assessed pregnant women and their children and followed them up to the age of eight years [17]. According to Jimenez et al. study Living one mile farther away from a greenspace at birth was associated with 5.6 mmHg higher adult SBP (95%CI: 0.7, 10.5), and 3.5 mmHg higher DBP in adjusted models (95%CI: 0.3, 6.8). One more greenspace in the neighborhood at birth was also associated with lower DBP in adulthood (− 0.2 mmHg, 95%CI: −0.4, − 0.02) [17]. In addition, two studies looked at the relationship between greenspace and HTN in children [15, 110]. The remaining articles focused on adult populations as target groups. Abbasi et al. discovered lower SBP and DBP in children who lived near greenspaces (− 0.08mmHg and − 0.09 mmHg, respectively), but these findings were not statistically significant in the ORs reported for isolated elevated SBP, DBP, and HTN. This could imply that more research is needed to determine whether the results are supportive or not [15]. In the study by Markevych et al., they also evaluated children aged 10 years old and discovered that lower residential greenness was positively associated with higher blood pressure in 10-year-old children living in urban areas. This finding requires further investigation to confirm the theory of greenspace’s effect on children’s blood pressure and to assist policymakers in providing more public open spaces and greenspace for children in urban areas to reduce the risk of HTN in their adulthood [110]. A study by Bijnens et al. focused on twins aged 18 to 25 years old to see if there was an association between HTN and greenness in this population. They discovered that a 3.59 mmHg (95% CI:-0.6 to -1.23; p = 0.005) decrease in adult night systolic blood pressure was associated with an interquartile increase in residential greenness exposure (1000 m radius). Night-time blood pressure was inversely related to residential greenness in adulthood and residential greenness in childhood in twins who lived at a different address than their birth address at the time of the measurement (n = 181, 65.1%) [12]. This could clarify the effect of greenness in the living area regardless of age. Since the majority of the reviewed articles assessed accessibility to greenspace, these articles primarily discovered a negative association between HTN and accessibility to greenspace, as detailed in Supplementary Table 2. Studies that evaluated greenspace based on their proximity [15, 16, 88, 137] found a positive relationship between proximity to greenspaces and higher SBP, DBP, or HTN [15, 16, 88, 137]. This review included a study evaluating the effect of HTN and greenspace in early pregnancy. This study found a positive association between proximity to greenspaces and HTN in pregnant women [88]. As previous studies showed that women in their first trimester of pregnancy are an appropriate group for the study of hypertensive disorders because, while changes in pregnancy cause increased stress on the cardiovascular system, such effects primarily occur from the second trimester of pregnancy [163]. As a result, blood pressure during the first trimester of pregnancy is primarily caused by external factors [88, 163].
Greenspace and BG
This review compiled indications of the associations between greenspace and blood glucose levels or DM. We evaluated 16 articles on the topic of BG or DM and greenspace in this review. Almost all of the studies applied greenness as a greenspace measurement, and 11 of them found a negative association between BG levels, DM diagnosis, or the prevalence of T2DM, while three found a positive association [31, 139, 152] (Fig. 3c).
Ruijia Li et al. showed that an increase in the NDVI within a 500 m buffer radius is associated with a 13.4% decrease in FBG with an odds ratio (OR) of 0.866 and 14.2% (OR: 0.858) decreased risk of T2DM [130].
According to Ngam et al., greenspaces with sports facilities have a significant relationship to cerebrovascular diseases; the most distant population had an 11% higher prevalence rate ratio (PRR) of cardiovascular diseases (CVD) than the nearest, as well as a 9% higher diabetes risk (PRR) than the nearest [152].
Liao et al. found that living in areas with more greenspace was associated with lower maternal glucose values and a lower risk of incident maternal impaired glucose tolerance (IGT) and gestational diabetes mellitus (GDM) [131].
Dadvand et al. revealed an inverse correlation between time spent in greenspaces, specifically natural greenspaces, and FBG levels; and an increase in total time spent in greenspaces of 1.83 h was associated with a 0.5 mg/dl decrease in FBG levels in children aged 7–18 years [35].
Greenspace and lipids
This review collected information on the associations between greenspace and lipid profile levels, also known as dyslipidemia. In this review, we focused on 8 articles about lipid profile levels or dyslipidemia and greenspace. Greenness was used as a greenspace measurement in all of the studies, and four of them found a negative association between lipid profile levels and dyslipidemia, while one found a positive association [116] (Fig. 3d).
According to Iyer et al., a 0.11 unit increase in NDVI was associated with lower BMI and diabetes, but there was no association between NDVI and hypertension or cholesterol [132]. Residential greenness was associated with an increased risk of dyslipidemia in Chinese rural-dwelling adults, particularly among males, according to a study by Jiang et al. [116].
Probable mechanisms
Despite widespread agreement that physical environments and access to public open spaces such as vegetation play an important role in people’s weight status, a large body of research has failed to identify direct associations between greenspace and obesity. Here are some hypotheses that could explain this association. Greenspace can boost physical activity through both walking and cycling routes, as well as places to exercise and play [164]. Greenery is strongly correlated with more outdoor playing in children [165]. In addition, the risk of ambient air Pollution and noise may be reduced by vegetation. There is evidence of the possibility of obesity due to air pollution [25]. According to recent studies, the availability to greenspace and exposure to mixed bacteria may help to prevent obesity as an inflammatory disease by balancing the immune system to prevent inflammatory processes like obesity [24, 166]. Individuals’ stress levels may be reduced, and their social cohesion may be increased if they have easy access to greenspace [25]. This finding lends credence to the Glonti et al. study’s finding that people with higher levels of social cohesion have a lower risk of obesity [167].
Although the mechanisms by which greenery improves health and HTN remain unknown, several biopsychosocial pathways have been proposed [25]. Stress reduction and recovery, increased physical activity, social cohesion endorsement, and reduced exposure to air pollution and noise have all been suggested as possible mechanisms in the green-health pathway, all of which could be essential in evaluating the risk of HTN in urban populations [12, 26, 168,169,170,171]. According to facts, adiposity, a well-documented risk factor for HTN, appears to be reduced in green environments. The findings support this hypothesis, which shows that BMI mediated a large portion of the association between greenness and blood pressure [172]. Greenness has also been associated with lower noise and heat exposure, enhanced social cohesion, greater and more diverse microbial exposure, and lesser psychological and physiological stress [24, 25].
Using greenspaces in a neighborhood can be beneficial for physical activity. This means that it should be easily accessible and promoted for active use [115]. Despite these findings, the relationship between greenspace exposure and incident diabetes is not fully understood. Besides physical activity, other explanations may exist, for example, the benefits of exposure to nature for immunological regulation [24].
While the biological mechanisms underlying greenness’s beneficial effect on blood lipids are unclear, previous research has suggested several biopsychosocial pathways, including reduced levels of air pollution [151, 173, 174] and increased physical activity [23, 175, 176], which could reduce lipid peroxidation products and oxidative stress markers and further improve lipid profiles [23].
Limitations and strengths
Various limitations should be implied for proper interpretation of our systematic review. First, data in included studies in terms of exposure and outcome definition and measurement was severely heterogeneous, which could bias the final interpretation. Second, there was not enough data from developing countries, and due to the increasing growth of obesity, diabetes, HTN and dyslipidemia in these nations and also different socioeconomic and geographic information, these results cannot be generalized to these nations. Third, statistical modeling methods differed significantly, with several cofounding factors evaluated by different studies. As a result, some studies may have over-adjusted or under-adjusted for confounding factors, resulting in biased effect estimates. Fourth, only anthropometric measures representing weight status in studies were used in this systematic review, including BMI, which may bias the results. Other anthropometric characteristics may more accurately represent weight status. Fifth, the majority of the studies reviewed in this article were cross-sectional, which may impact the possible association in case follow-up, whether retrospectively or prospectively. Despite the limitations mentioned, this article has systematically studied the effects of greenspace on the CMRFs of the people studied in various articles. The general population provided a sufficient sample size, and despite the lack of sufficient data from developing countries, the studies examined were successful. Therefore, our results may be helpful for experts in the field of greenspace overweight/obesity, and policymakers in the field of developing a strategic plan to mitigate the burden of obesity.
Almost all of the studies reviewed in this article related to HTN were conducted within the last four years, but further research in different age groups is needed to confirm the findings of the relationship between HTN and greenspace. Only three studies, two with a target population of children [15, 110] and one with a target population of pregnant women [88], were chosen for this article to evaluate the association between blood pressure and greenspace. More research is needed to generalize these studies’ findings. In addition, four studies [47, 89, 90, 137] focused on cardiovascular events and health status in general as an outcome of the research. The results were not specific enough for this review article to evaluate greenspace’s effect on blood pressure.
Almost all of the studies reviewed in this article related to DM or dyslipidemia were conducted within the last four years, but further research in different age groups is needed to confirm the findings of the relationship between DM or dyslipidemia and greenspace. The obscured mechanism linking greenspaces and diabetes or dyslipidemia by increasing physical activity could be due to measurement error in exposure and outcome, residual confounding between greenspace and diabetes risk, and the fact that we had an overall measure of physical activity rather than just that done in greenspace [23].
Almost all of the studies reviewed in this paper were conducted in Urban regions and metropolitan areas so there are some limitations for comparing rural and urban areas for association of CMRFs and access to greenspaces. And also since there is more access to POS in urban areas with better socioeconomic conditions and people with better socioeconomic conditions in major metropolitan cities possibly access to better health literacy and leads to more physical activities [155]. So in this reviewed we have limitations for interpretations of the association of access to greenspaces and CMRFs in metropolitan cities.
Recommendation for forthcoming reviews and studies
According to the limitations of our review, we recommend that future articles on this topic follow these steps to properly imply an association between weight status, HTN, diabetes, dyslipidemia and greenspace availability. First, future articles could assess the effect of greenspace on individuals’ physical activity and support the theory that better access to greenspace may lead to higher physical activity and, as a result, lower BMI and lower blood pressure. Future studies can also be conducted in different age groups, focusing on pregnant women and the effect of greenspace availability on their health status to determine whether access to greenspace is more effective in older or younger age groups. Finally, data from developing countries may alter the effect of greenspace on obesity and HTN and assist researchers in generalizing the relationship.
Conclusions
According to the findings of this review, greater access to greenspace is associated with lower SBP/DBP or lower risk of HTN, as well as a lower chance of being overweight or obese with a lower BMI and lower BG levels and lipid profiles. Regardless, a firm conclusion cannot be drawn due to a large number of articles with no significant results, the extensive interplay between-study heterogeneity, and the small number of accessible studies.
Data availability
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- BG:
-
Blood glucose
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- DBP:
-
Diastolic blood pressure
- HTN:
-
Hypertension
- SBP:
-
Systolic blood pressure
References
Mezhal F, et al. High prevalence of cardiometabolic risk factors amongst young adults in the United Arab Emirates: the UAE healthy future study. BMC Cardiovasc Disord. 2023;23(1):137.
Hartig T, et al. Nat Health Annual Rev Public Health. 2014;35(1):207–28.
Hutto D Jr, Barrett K. DO OPEN SPACES WITHIN AN URBAN MATRIX INCREASE ANURAN ABUNDANCE? Herpetological Conserv Biology. 2022;17(3):582–92.
Bull FC, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–62.
Bohdjalian A, et al. Sleeve gastrectomy as sole and definitive bariatric procedure: 5-year results for weight loss and ghrelin. Obes Surg. 2010;20(5):535–40.
Dietrich MO, Horvath TL. Limitations in anti-obesity drug development: the critical role of hunger-promoting neurons. Nat Rev Drug Discovery. 2012;11(9):675–91.
Wadden TA, et al. Lifestyle modification for obesity: new developments in diet, physical activity, and behavior therapy. Circulation. 2012;125(9):1157–70.
Swinburn BA, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378(9793):804–14.
Lachowycz K, Jones AP. Greenspace and obesity: a systematic review of the evidence. Obes Rev. 2011;12(5):e183–9.
Jiang J et al. Do exposures to green space reduce the risk of hypertension? 2020.
Leong DP, et al. Reducing the global burden of cardiovascular disease, part 2: prevention and treatment of cardiovascular disease. Circul Res. 2017;121(6):695–710.
Bijnens EM, et al. Blood pressure in young adulthood and residential greenness in the early-life environment of twins. Environ Health. 2017;16(1):1–8.
Jiang J et al. Does long-term green space exposure improve hypertension and blood pressure? The Henan rural cohort study. The Henan Rural Cohort Study (8/3/2020), 2020.
Yang B-Y, et al. Community greenness, blood pressure, and hypertension in urban dwellers: the 33 communities Chinese health study. Environ Int. 2019;126:727–34.
Abbasi B et al. Subjective proximity to green spaces and blood pressure in children and adolescents: the CASPIAN-V study. J Environ Public Hea. 2020;2020.
Dzhambov AM, Markevych I, Lercher P. Greenspace seems protective of both high and low blood pressure among residents of an Alpine valley. Environ Int. 2018;121:443–52.
Jimenez MP, et al. Associations of types of green space across the life-course with blood pressure and body mass index. Environ Res. 2020;185:109411.
Moreira S, et al. Associating physical activity levels to stress, high blood pressure, and high blood glucose risks in Green Park users. J Exerc Physiol. 2013;16(3):51–8.
Moreira TC, et al. Green spaces, land cover, street trees and hypertension in the megacity of São Paulo. Int J Environ Res Public Health. 2020;17(3):725.
Bloemsma LD, et al. Green space, air pollution, traffic noise and cardiometabolic health in adolescents: the PIAMA birth cohort. Environ Int. 2019;131:104991.
Jendrossek M, et al. Residential air pollution, road traffic, greenness and maternal hypertension: results from GINIplus and LISAplus. Int J Occup Environ Med. 2017;8(3):131.
Kopin L. C Lowenstein. Dyslipidemia. Ann Intern Med. 2017;167(11):ITC81–96.
Fan S, et al. Associations between residential greenness and blood lipids in Chinese uyghur adults. Environ Int. 2020;142:105903.
Rook GA. Regulation of the immune system by biodiversity from the natural environment: an ecosystem service essential to health. P Natl Acad Sci. 2013;110(46):18360–18367.
Markevych I, et al. Exploring pathways linking greenspace to health: theoretical and methodological guidance. Environ Res. 2017;158:301–17.
Brown SC, et al. Neighborhood greenness and chronic health conditions in medicare beneficiaries. Am J Prev Med. 2016;51(1):78–89.
Kim H-J, et al. Parks and green areas are associated with decreased risk for hyperlipidemia. Int J Environ Res Public Health. 2016;13(12):1205.
Agardh E, et al. Type 2 diabetes incidence and socio-economic position: a systematic review and meta-analysis. Int J Epidemiol. 2011;40(3):804–18.
Hu FB, et al. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N Engl J Med. 2001;345(11):790–7.
Barroso I. Genetics of type 2 diabetes. Diabet Med. 2005;22(5):517–35.
Müller G, et al. Regional and neighborhood disparities in the odds of type 2 diabetes: results from 5 population-based studies in Germany (DIAB-CORE Consortium). Am J Epidemiol. 2013;178(2):221–30.
Astell-Burt T, Feng X, Kolt GS. Is neighborhood green space associated with a lower risk of type 2 diabetes? Evidence from 267,072 Australians. Diabetes Care. 2014;37(1):197–201.
Feng X, Astell-Burt T. Does area of residence influence weight loss following a diagnosis of type 2 diabetes? Fixed effects longitudinal analysis of 54,707 middle-to-older aged Australians. Diabetes Res Clin Pract. 2016;116:123–6.
Sørensen M, et al. Long-term exposure to road traffic noise and incident diabetes: a cohort study. Environ Health Perspect. 2013;121(2):217–22.
Dadvand P, et al. Use of green spaces and blood glucose in children; a population-based CASPIAN-V study. Environ Pollut. 2018;243:1134–40.
Fan S, et al. Associations of residential greenness with diabetes mellitus in Chinese uyghur adults. Int J Environ Res Public Health. 2019;16(24):5131.
Tian Z, et al. Gender-specific associations of body mass index and waist circumference with type 2 diabetes mellitus in Chinese rural adults: the Henan rural cohort study. J Diabetes Complicat. 2018;32(9):824–9.
Luo YN, et al. Greenspace with overweight and obesity: a systematic review and meta-analysis of epidemiological studies up to 2020. Obes Rev. 2020;21(11):e13078.
Dunton GF, et al. Physical environmental correlates of childhood obesity: a systematic review. Obes Rev. 2009;10(4):393–402.
Feng J, et al. The built environment and obesity: a systematic review of the epidemiologic evidence. Health Place. 2010;16(2):175–90.
Jean-Louis S. The effects of access to green space on obesity: an integrative review. Am Acad Pediatrics. 2018.
Rahimi-Ardabili H, et al. Green space and health in mainland China: a systematic review. Int J Environ Res Public Health. 2021;18(18):9937.
Moher D, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Peterson J, et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute; 2011. pp. 1–12.
Zhao Y et al. Association between greenspace and blood pressure: a systematic review and meta-analysis. Sci Total Environ. 2022:152513.
Yeager R, et al. Association between residential greenness and cardiovascular disease risk. J Am Heart Association. 2018;7(24):e009117.
Hinojosa AMO, et al. Influence of school environments on childhood obesity in California. Environ Res. 2018;166:100–7.
Oreskovic NM, et al. Obesity and the built environment among Massachusetts children. Clin Pediatr. 2009;48(9):904–12.
Alexander DS, et al. The association between recreational parks, facilities and childhood obesity: a cross-sectional study of the 2007 national survey of children’s health. J Epidemiol Commun Health. 2013;67(5):427–31.
Bai H, et al. Perceptions of neighborhood park quality: associations with physical activity and body mass index. Ann Behav Med. 2013;45(SUPPL1):S39–48.
Bell JF, Wilson JS, Liu GC. Neighborhood greenness and 2-year changes in body mass index of children and youth. Am J Prev Med. 2008;35(6):547–53.
Brown BB, et al. Mixed land use and walkability: variations in land use measures and relationships with BMI, overweight, and obesity. Health & place; 2009;15(4):1130–41.
Browning MH, Rigolon A. Do income, race and ethnicity, and sprawl influence the greenspace-human health link in city-level analyses? Findings from 496 cities in the United States. Int J Environ Res Public Health. 2018;15(7):1541.
Goldsby TU et al. Urban park development and pediatric obesity rates: a quasi-experiment using electronic health record data. Int J Environ Res Public Health. 2016;13(4).
Hoehner C, et al. Built environment features in the home and worksite neighborhood are associated with cardiorespiratory fitness. J Sci Med Sport. 2012;15:S100.
James P, et al. Interrelationships between walkability, air pollution, greenness, and body mass index. Epidemiology (Cambridge, Mass.). 2017;28(6):780.
Li F, et al. Built environment, adiposity, and physical activity in adults aged 50–75. Am J Prev Med. 2008;35(1):38–46.
Li X, Ghosh D. Associations between body mass index and urban green streetscape in Cleveland, Ohio, USA. Int J Environ Res Public Health. 2018;15(10):2186.
Liu GC, et al. Green neighborhoods, food retail and childhood overweight: differences by population density. Am J Health Promotion. 2007;21(4suppl):317–25.
Lovasi GS, et al. Is the environment near home and school associated with physical activity and adiposity of urban preschool children? J Urb Health. 2011;88(6):1143–57.
Mathis AL, et al. Neighborhood influences and BMI in urban older adults. J Appl Gerontol. 2017;36(6):692–708.
Nesbit KC, et al. Proximal and distal environmental correlates of adolescent obesity. J Phys Activity Health. 2014;11(6):1179–86.
Norman GJ, et al. Community design and access to recreational facilities as correlates of adolescent physical activity and body-mass index. J Phys Activity Health. 2006;3(s1):S118–28.
Rundle A, et al. Associations between body mass index and park proximity, size, cleanliness, and recreational facilities. Am J Health Promotion. 2013;27(4):262–9.
Singh GK, Siahpush M, Kogan MD. Neighborhood socioeconomic conditions, built environments, and childhood obesity. Health Aff. 2010;29(3):503–12.
Sullivan SM, et al. Neighborhood environments and obesity among Afro-Caribbean, African American, and non-hispanic white adults in the United States: results from the National Survey of American Life. Prev Med. 2014;61:1–5.
Vaccaro JA, Zarini GG, Huffman FG. Parental perceptions of child’s medical care and neighborhood and child’s behavioral risk factors for obesity in U.S. children by body mass index classification. J Environ Public Hea. 2019;2019.
Veitch J, et al. Park availability and physical activity, TV time, and overweight and obesity among women: findings from Australia and the United States. Health Place. 2016;38:96–102.
Wall MM, et al. Patterns of obesogenic neighborhood features and adolescent weight: a comparison of statistical approaches. Am J Prev Med. 2012;42(5):e65–75.
Wen M, Kowaleski-Jones L. The built environment and risk of obesity in the United States: racial-ethnic disparities. Health Place. 2012;18(6):1314–22.
Wolch J, et al. Childhood obesity and proximity to urban parks and recreational resources: a longitudinal cohort study. Health Place. 2011;17(1):207–14.
Yang Y, et al. A cross-sectional study of the influence of neighborhood environment on childhood overweight and obesity: variation by age, gender, and environment characteristics. Prev Med. 2018;108:23–8.
Zhang X, et al. Associations between the built environment and body mass index in the Mexican American Mano A Mano Cohort. Sci Total Environ. 2019;654:456–62.
Benjamin-Neelon SE, et al. Greenspace, physical activity, and BMI in children from two cities in northern Mexico. Prev Med Rep. 2019;14:100870.
Bird M, et al. A park typology in the QUALITY cohort: implications for physical activity and truncal fat among youth at risk of obesity. Prev Med. 2016;90:133–8.
Davidson Z, Simen-Kapeu A, Veugelers PJ. Neighborhood determinants of self-efficacy, physical activity, and body weights among Canadian children. Health Place. 2010;16(3):567–72.
Hughey SM, et al. Green and lean: is neighborhood park and playground availability associated with youth obesity? Variations by gender, socioeconomic status, and race/ethnicity. Prev Med. 2017;95:S101–8.
Nies MA, et al. Spatial and census data to evaluate obese persons and their environment (SCOPE). Am J Health Behav. 2015;39(4):582–8.
Potestio ML et al. Is there an association between spatial access to parks/green space and childhood overweight/obesity in Calgary, Canada? Int J Behav Nutr Phys Activity. 2009;6.
Potwarka LR, Kaczynski AT, Flack AL. Places to play: association of park space and facilities with healthy weight status among children. J Community Health. 2008;33(5):344–50.
Veugelers P, et al. Neighborhood characteristics in relation to diet, physical activity and overweight of Canadian children. Int J Pediatr Obes. 2008;3(3):152–9.
Doubleday A, et al. Neighborhood greenspace and risk of type 2 diabetes in a prospective cohort: the multi-ethncity study of atherosclerosis. Environ Health. 2022;21(1):1–10.
Clark C, et al. Association of long-term exposure to transportation noise and traffic-related air pollution with the incidence of diabetes: a prospective cohort study. Environ Health Perspect. 2017;125(8):087025.
Ulmer JM, et al. Multiple health benefits of urban tree canopy: the mounting evidence for a green prescription. Health Place. 2016;42:54–62.
Riggs DW, et al. Residential proximity to greenness mitigates the hemodynamic effects of ambient air pollution. Am J Physiol Heart Circ Physiol. 2021;320(3):H1102–11.
Poulsen MN, et al. Association of greenness with blood pressure among individuals with type 2 diabetes across rural to urban community types in Pennsylvania, USA. Int J Environ Res Public Health. 2021;18(2):614.
Grazuleviciene R, et al. The influence of proximity to city parks on blood pressure in early pregnancy. Int J Environ Res Public Health. 2014;11(3):2958–72.
Bilal U, et al. Population cardiovascular health and urban environments: the heart healthy hoods exploratory study in Madrid, Spain. BMC Med Res Methodol. 2016;16(1):1–12.
Picavet HSJ, et al. Greener living environment healthier people? Exploring green space, physical activity and health in the Doetinchem Cohort Study. Prev Med. 2016;89:7–14.
Burgoine T et al. Associations between BMI and home, school and route environmental exposures estimated using GPS and GIS: do we see evidence of selective daily mobility bias in children? Int J Health Geogr. 2015;14(1).
Hobbs M, et al. Neighbourhood typologies and associations with body mass index and obesity: a cross-sectional study. Prev Med. 2018;111:351–7.
Van Der Zwaard BC, et al. Does environment influence childhood BMI? A longitudinal analysis of children aged 3–11. J Epidemiol Commun Health. 2018;72(12):1110–6.
Mason KE, Pearce N, Cummins S. Do neighbourhood characteristics act together to influence BMI? A cross-sectional study of urban parks and takeaway/fast-food stores as modifiers of the effect of physical activity facilities. Soc Sci Med. 2020;261:113242.
Coombes E, Jones AP, Hillsdon M. The relationship of physical activity and overweight to objectively measured green space accessibility and use. Soc Sci Med. 2010;70(6):816–22.
Cummins S, Fagg J. Does greener mean thinner? Associations between neighbourhood greenspace and weight status among adults in England. Int J Obes. 2012;36(8):1108–13.
Ellaway A, Macintyre S, Bonnefoy X. Graffiti, greenery, and obesity in adults: secondary analysis of European cross sectional survey. BMJ. 2005;331(7517):611–2.
Gose M, et al. Longitudinal influences of neighbourhood built and social environment on children’s weight status. Int J Environ Res Public Health. 2013;10(10):5083–96.
Klompmaker JO, et al. Green space definition affects associations of green space with overweight and physical activity. Environ Res. 2018;160:531–40.
Müller G et al. Inner-city green space and its association with body mass index and prevalent type 2 diabetes: a cross-sectional study in an urban German city. BMJ Open. 2018;8(1).
Schüle SA, Fromme H, Bolte G. Built and socioeconomic neighbourhood environments and overweight in preschool aged children. A multilevel study to disentangle individual and contextual relationships. Environ Res. 2016;150:328–36.
Putrik P, et al. Neighborhood environment is associated with overweight and obesity, particularly in older residents: results from cross-sectional study in Dutch municipality. J Urb Health. 2015;92(6):1038–51.
Toftager M, et al. Distance to green space and physical activity: a Danish national representative survey. J Phys Activity Health. 2011;8(6):741–9.
Nielsen TS, Hansen KB. Do green areas affect health? Results from a Danish survey on the use of green areas and health indicators. Health & place. 2007;13(4):839–50.
Dadvand P, et al. Risks and benefits of green spaces for children: a cross-sectional study of associations with sedentary behavior, obesity, asthma, and allergy. Environ Health Perspect. 2015;122(12):1329–35.
Pereira M, Nogueira H, Padez C. The role of urban design in childhood obesity-a case study in Lisbon, Portugal. Am J Hum Biol. 2019.
Nicolle-Mir L. Influence of the surrounding green spaces on the risk of overweight in preschool-age children in the city of Kaunas, Lithuania. Environ Risques et Sante. 2018;17(6):547–8.
Björk J, et al. Recreational values of the natural environment in relation to neighbourhood satisfaction, physical activity, obesity and wellbeing. J Epidemiol Commun Health. 2008;62(4):e2.
Dempsey S, Lyons S, Nolan A. Urban green space and obesity in older adults: evidence from Ireland. SSM-population Health. 2018;4:206–15.
Markevych I, et al. A cross-sectional analysis of the effects of residential greenness on blood pressure in 10-year old children: results from the GINIplus and LISAplus studies. BMC Public Health. 2014;14(1):1–11.
Picavet HS, et al. Greener living environment healthier people? Exploring green space, physical activity and health in the Doetinchem Cohort Study. Prev Med. 2016;89:7–14.
Rodriguez-Loureiro L, et al. Long-term exposure to objective and perceived residential greenness and diabetes mortality: a census-based cohort study. Sci Total Environ. 2022;821:153445.
Ponjoan A, et al. Impact of residential greenness on myocardial infarction in the population with diabetes: a sex-dependent association? Environ Res. 2022;205:112449.
Bodicoat DH, et al. The association between neighbourhood greenspace and type 2 diabetes in a large cross-sectional study. BMJ open. 2014;4(12):e006076.
Dalton AM, et al. Residential neighbourhood greenspace is associated with reduced risk of incident diabetes in older people: a prospective cohort study. BMC Public Health. 2016;16(1):1–10.
Jiang J, et al. Is residential greenness associated with dyslipidemia and lipid levels in Chinese rural-dwelling adults? The Henan rural cohort study. Environ Sci Pollut Res. 2022;29(4):5852–62.
Tamosiunas A, et al. Accessibility and use of urban green spaces, and cardiovascular health: findings from a Kaunas cohort study. Environ Health. 2014;13(1):1–11.
Sarkar C, Webster C, Gallacher J. Neighbourhood walkability and incidence of hypertension: findings from the study of 429,334 UK Biobank participants. Int J Hyg Environ Health. 2018;221(3):458–68.
Ribeiro AI, et al. Association between neighbourhood green space and biological markers in school-aged children. Findings from the Generation XXI birth cohort. Environ Int. 2019;132:105070.
Plans E, et al. Density of green spaces and cardiovascular risk factors in the city of Madrid: the heart healthy hoods study. Int J Environ Res Public Health. 2019;16(24):4918.
Madhloum N, et al. Neonatal blood pressure in association with prenatal air pollution exposure, traffic, and land use indicators: an ENVIRONAGE birth cohort study. Environ Int. 2019;130:104853.
de Keijzer C, et al. Long-term exposure to greenspace and metabolic syndrome: a Whitehall II study. Environ Pollut. 2019;255:113231.
Brazienė A, et al. The influence of proximity to city parks and major roads on the development of arterial hypertension. Scand J Public Health. 2018;46(6):667–74.
Bauwelinck M, et al. Residential urban greenspace and hypertension: a comparative study in two European cities. Environ Res. 2020;191:110032.
Manandhar S, Suksaroj TT, Rattanapan C. The association between green space and the prevalence of overweight/ obesity among primary school children. Int J Occup Environ Med. 2019;10(1):1–10.
Akpinar A. Urban green spaces for children: a cross-sectional study of associations with distance, physical activity, screen time, general health, and overweight. Urban For Urban Gree. 2017;25:66–73.
Mowafi M, et al. Is access to neighborhood green space associated with BMI among egyptians? A multilevel study of Cairo neighborhoods. Volume 18. Health & place; 2012;18(2):385–90.
Li G et al. Multiple environmental exposures and obesity in eastern China: An individual exposure evaluation model. Chemosphere. 2022:134316.
Li G, et al. Associations of combined exposures to ambient temperature, air pollution, and green space with hypertension in rural areas of Anhui Province, China: a cross-sectional study. Environ Res. 2022;204:112370.
Li R, et al. Residential green and blue spaces and type 2 diabetes mellitus: a population-based health study in China. Toxics. 2021;9(1):11.
Liao J, et al. Effect of residential exposure to green space on maternal blood glucose levels, impaired glucose tolerance, and gestational diabetes mellitus. Environ Res. 2019;176:108526.
Iyer HS, et al. Neighborhood greenness and burden of non-communicable diseases in Sub-Saharan Africa: a multi-country cross-sectional study. Environ Res. 2021;196:110397.
Markevych I, et al. Residential greenness and blood lipids in children: a longitudinal analysis in GINIplus and LISAplus. Environ Res. 2016;151:168–73.
Leng H, et al. Exploring the relationship between green space in a neighbourhood and cardiovascular health in the winter city of China: a study using a health survey for harbin. Int J Environ Res Public Health. 2020;17(2):513.
Aliyas Z. Physical, mental, and physiological health benefits of green and blue outdoor spaces among elderly people. Int J Environ Health Res. 2021;31(6):703–14.
Astell-Burt T, Feng X, Kolt GS. Greener neighborhoods, slimmer people evidence from 246 920 Australians. Int J Obes. 2014;38(1):156–9.
Astell-Burt T, Feng X, Kolt GS. Large-scale investment in green space as an intervention for physical activity, mental and cardiometabolic health: study protocol for a quasi-experimental evaluation of a natural experiment. BMJ open. 2016;6(4):e009803.
Feng X, Astell-Burt T. Residential green space quantity and quality and symptoms of psychological distress: a 15-year longitudinal study of 3897 women in postpartum. BMC Psychiatry. 2018;18(1):1–11.
Paquet C, et al. Food environment, walkability, and public open spaces are associated with incident development of cardio-metabolic risk factors in a biomedical cohort. Health Place. 2014;28:173–6.
Pearson AL, et al. Associations between neighbourhood environmental characteristics and obesity and related behaviours among adult new zealanders. BMC Public Health. 2014;14(1):1–13.
Pereira G, et al. The association between neighborhood greenness and weight status: an observational study in Perth Western Australia. Environ Health. 2013;12(1):1–9.
Müller G, et al. Inner-city green space and its association with body mass index and prevalent type 2 diabetes: a cross-sectional study in an urban German city. BMJ open. 2018;8(1):e019062.
Chong S, et al. Neighbourhood greenspace and physical activity and sedentary behaviour among older adults with a recent diagnosis of type 2 diabetes: a prospective analysis. BMJ open. 2019;9(11):e028947.
Mazumdar S, et al. Which green space metric best predicts a lowered odds of type 2 diabetes? Int J Environ Res Public Health. 2021;18(8):4088.
De Assis MM, et al. Overweight, perceived environment, and social deprivation: a study on the perception of parents or guardians. Revista Paulista De Pediatria. 2018;36(4):466–73.
Mena C, et al. Role of access to parks and markets with anthropometric measurements, biological markers, and a healthy lifestyle. Int J Environ Health Res. 2015;25(4):373–83.
Mendes LL et al. Individual and environmental factors associated for overweight in urban population of Brazil. BMC Public Health. 2013;13(1).
Moreira S, et al. Associating physical activity levels to stress, high blood pressure, and high blood glucose risks in green park users. J Exerc Physiol Online. 2013;16(3):51–8.
Rossi CE, et al. Body mass index and association with use of and distance from places for physical activity and active leisure among schoolchildren in Brazil. Cross-sectional study. Sao Paulo Med J. 2018;136(3):228–36.
Velásquez-Meléndez G, Mendes LL, Padez CMP. Built environment and social environment: associations with overweight and obesity in a sample of Brazilian adults. Cadernos De Saude Publica. 2013;29(10):1988–96.
Yang B-Y, et al. Residential greenness and blood lipids in urban-dwelling adults: the 33 communities Chinese health study. Environ Pollut. 2019;250:14–22.
Ngom R, et al. Type and proximity of green spaces are important for preventing cardiovascular morbidity and diabetes—a cross-sectional study for Quebec, Canada. Int J Environ Res Public Health. 2016;13(4):423.
Buja A, et al. Health literacy and physical activity: a systematic review. J Phys Activity Health. 2020;17(12):1259–74.
Nutbeam D. The evolving concept of health literacy. Soc Sci Med. 2008;67(12):2072–8.
Boldovskaia A, et al. Physical literacy assessment in adults: a systematic review. PLoS ONE. 2023;18(7):e0288541.
Lotrean LM, et al. Actual weight, perceived weight and desired weight of Romanian school children by parents and children. Medicina. 2021;57(4):333.
Valea A et al. Morbid child obesity with possible Rohhadnet-Rohhad syndrome. Case report. Acta Endocrinol (1841 – 0987). 2014;10(3).
Schulz M, Romppel M, Grande G. Built environment and health: a systematic review of studies in Germany. J Public Health (Oxf). 2018;40(1):8–15.
James P, et al. A review of the health benefits of greenness. Curr Epidemiol Rep. 2015;2(2):131–42.
Mackenbach JD, et al. Obesogenic environments: a systematic review of the association between the physical environment and adult weight status, the SPOTLIGHT project. BMC Public Health. 2014;14(1):233.
Dempsey S, Lyons S, Nolan A. Urban green space and obesity in older adults: evidence from Ireland. SSM Popul Health. 2018;4:206–15.
Morgan Hughey S, et al. Green and lean: is neighborhood park and playground availability associated with youth obesity? Variations by gender, socioeconomic status, and race/ethnicity. Prev Med. 2017;95:S101–8.
Yoder SR, Thornburg LL, Bisognano JD. Hypertension in pregnancy and women of childbearing age. Am J Med. 2009;122(10):890–5.
Hartig T, et al. Nature and health. Annu Rev Public Health. 2014;35:207–28.
Mota J, et al. Perceived neighborhood environments and physical activity in adolescents. Prev Med. 2005;41(5–6):834–6.
Lim J, et al. Diet-induced obesity, adipose inflammation, and metabolic dysfunction correlating with PAR2 expression are attenuated by PAR2 antagonism. FASEB J. 2013;27(12):4757–67.
Glonti K, et al. Psychosocial environment: definitions, measures and associations with weight status–a systematic review. Obes Rev. 2016;17:81–95.
Estes MG Jr, et al. Use of remotely sensed data to evaluate the relationship between living environment and blood pressure. Environ Health Perspect. 2009;117(12):1832–8.
Khajavi A, et al. Impact of short-and long-term exposure to air pollution on blood pressure: a two-decade population-based study in Tehran. Int J Hyg Environ Health. 2021;234:113719.
Lane KJ, et al. Associations between greenness, impervious surface area, and nighttime lights on biomarkers of vascular aging in Chennai, India. Environ Health Perspect. 2017;125(8):087003.
Organization WH. A global brief on hypertension: silent killer, global public health crisis: World Health Day 2013. World Health Organization; 2013.
Sarkar C. Residential greenness and adiposity: findings from the UK Biobank. Environ Int. 2017;106:1–10.
Hirabayashi S, Nowak DJ. Comprehensive national database of tree effects on air quality and human health in the United States. Environ Pollut. 2016;215:48–57.
Crouse DL, et al. Complex relationships between greenness, air pollution, and mortality in a population-based Canadian cohort. Environ Int. 2019;128:292–300.
Gordon LA, et al. Effect of exercise therapy on lipid profile and oxidative stress indicators in patients with type 2 diabetes. BMC Complement Altern Med. 2008;8(1):1–10.
Lin X, et al. Effects of exercise training on cardiorespiratory fitness and biomarkers of cardiometabolic health: a systematic review and meta-analysis of randomized controlled trials. J Am Heart Association. 2015;4(7):e002014.
Li G, et al. Multiple environmental exposures and obesity in eastern China: an individual exposure evaluation model. Chemosphere. 2022;298:134316.
Markevych I et al. A cross-sectional analysis of the effects of residential greenness on blood pressure in 10-year old children: results from the GINIplus and LISAplus studies. BMC Public Health. 2014;14(1).
Bilal U et al. Population cardiovascular health and urban environments: the heart healthy hoods exploratory study in Madrid, Spain. BMC Med Res Methodol. 2016;16(1).
Rodriguez-Loureiro L et al. Long-term exposure to objective and perceived residential greenness and diabetes mortality: a census-based cohort study. Sci Total Environ, 2022: p. 153445.
Lee H, et al. Influence of urban neighbourhood environment on physical activity and obesity-related diseases. Public Health. 2015;129(9):1204–10.
Acknowledgements
This study was approved by Alborz University of Medical Sciences.
Funding
This study was funded by Alborz University of Medical Sciences.
Author information
Authors and Affiliations
Contributions
YS, SS, MP, and MQ participated in the study design, drafting of the paper, and had a significant role in the development of the selection criteria and data extraction process. YSH, SS, MEs, MEb, NRG, SD, and MQ developed the search strategy and performed the qualitative data synthesis and quality assessments and meta-analysis. YS, BG, ZNG and MQ participated in a critical review. All authors read, provided feedback, and approved the final paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
not applicable.
Consent for publication
not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sharifi, Y., Sobhani, S., Ramezanghorbani, N. et al. Association of greenspaces exposure with cardiometabolic risk factors: a systematic review and meta-analysis. BMC Cardiovasc Disord 24, 170 (2024). https://doi.org/10.1186/s12872-024-03830-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-024-03830-1