
Abstract
Background
As patient exposure to ionizing radiation raises concern about malignancy risks, this study evaluated the effect of ionizing radiation on patients undergoing myocardial perfusion imaging (MPI) using the comet assay, a method for detection of DNA damage.
Methods
Patients without cancer, acute or autoimmune diseases, recent surgery or trauma, were studied. Gated single-photon myocardial perfusion imaging was performed with Tc-99m sestamibi. Peripheral blood was collected before radiotracer injection at rest and 60–90 min after injection. Single-cell gel electrophoresis (comet assay) was performed with blood lymphocytes to detect strand breaks, which determine a “comet tail” of variable size, visually scored by 3 observers in a fluorescence microscope after staining (0: no damage, no tail; 1: small damage; 2: large damage; 3: full damage). A damage index was calculated as a weighted average of the cell scores.
Results
Among the 29 individuals included in the analysis, age was 65.3 ± 9.9 years and 18 (62.1%) were male. The injected radiotracer dose was 880.6 ± 229.4 MBq. Most cells (approximately 70%) remained without DNA fragmentation (class 0) after tracer injection. There were nonsignificant increases of classes 1 and 2 of damage. Class 3 was the least frequent both before and after radiotracer injection, but displayed a significant, 44% increase after injection.
Conclusion
While lymphocytes mostly remained in class 0, an increase in class 3 DNA damage was detected. This may suggest that, despite a probable lack of biologically relevant DNA damage, there is still a need for tracer dose reductions in MPI.
Similar content being viewed by others

Background
Medical imaging- and, particularly, cardiac imaging- grew steadily from late 1980s to early 2000s, raising concern about patients´ exposure to ionizing radiation and carcinogenesis [1,2,3]. The 2019 National Council on Radiation Protection and Measurements (NCRP) Report, which updated medical radiation exposure information with data collected between 2006 and 2016, showed that Nuclear Medicine still accounted for 15% of the radiation burden, even though a decrease was noted [4]. While current practice is generally aligned with patient-centered imaging and radiation safety, the effects of ionizing radiation from imaging studies still merit attention.
To understand the potentially harmful effects of ionizing radiation from medical imaging, several studies have, for a long time, tried to make correlations between radiation exposure in medical, occupational and accidental contexts and cytogenetic alterations. However, radiation doses vary largely among studies and are sometimes very large when compared to actual medical imaging [5,6,7,8]. More recent studies are unable to fill all the knowledge gaps in this field, either due to limited number of subjects or specific conditions (e.g., pediatric populations) [9, 10]. Additionally, many variables influence radiation sensitivity, including cell sensitivity to induction of DNA damage, differences in DNA repair, in cell growth and in proportions of cells in different phases of the cell cycle [11]. Therefore, there is an open field for the continuous evaluation of the effects of ionizing radiation on human DNA.
This study aimed to evaluate the occurrence of DNA damage in patients undergoing myocardial perfusion imaging (MPI) using the comet assay (alkaline single-cell gel electrophoresis). The assay is based on the lysis of the cell membrane, followed by the induction of electrophoretic migration in an agarose matrix [12], resulting in the transport of DNA fragments out of the nucleus. The image of DNA migration obtained resembles a comet with a head and a tail, hence the term comet assay [12, 13]. Using microscope evaluation, it is possible to observe and grade the proportion of DNA strands or fragments which migrated, classifying the degree of damage and turning this relatively easy and low-cost procedure an interesting option to detect DNA lesions in individual cells. Thus, the study may add data to the continuum of knowledge gained on that subject, with a focus on a largely employed diagnostic imaging method.
Methods
Patients ≥ 18 years undergoing MPI at a single Nuclear Medicine laboratory were considered eligible for the study. Exclusion criteria were current or prior malignant neoplasm; autoimmune diseases; significant trauma, major surgery or exposure to radiation (diagnostic, therapeutic or occupational) in the past 3 months; acute infectious diseases or any acute disease with significant compromise of organs or systems (e.g. acute myocardial infarction, pulmonary embolism etc.).
The study was approved by the Ethics Committee of the Instituto Nacional de Cardiologia (# CAAE 6716971.6.0000.5272), and all patients provided written informed consent before participation in the study.
Myocardial perfusion imaging
Gated single-photon emission computed tomography (SPECT) MPI was performed with Tc-99m sestamibi (8 MBq/kg) in a 2-day protocol. For this study, to avoid possible stress-induced effects on the DNA, patients were evaluated only in the rest phase of the MPI study, with the stress phase performed on a subsequent date to avoid any residual DNA damage from prior radiotracer injection. The first peripheral blood sample (4 ml) was collected before tracer injection, and the second, immediately before the patient left the Nuclear Cardiology laboratory after image acquisition (60–90 min after tracer injection). Images were acquired in a 2-head gamma camera (Infinia Hawkeye 4, General Electric Healthcare, WI, USA).
Comet assay
The comet assay was performed according to the protocol described by Singh et al. [13]. Agarose-covered slides were prepared in duplicates (two with blood collected before, and two with blood collected after tracer injection). Each slide received a mixture of 5.0 µL of blood and 120.0 µL of low melting agarose, was covered with a coverslide, then refrigerated for five minutes for solidification, and thereafter the coverslides were removed. The slides were incubated in a lysis solution (1%Triton X-100, 10% dimethyl sulfoxide, 2.5 M NaCl, 100 mM ethylenediaminetetraacetic acid [EDTA], 10 mM Tris) for two hours, kept refrigerated and protected from light. Peripheral blood lymphocytes, which became nucleoid structures after lysis, were studied.
The alkaline unwinding, electrophoresis and neutralization steps were performed as described by Hartmann and Speit [14], with minor modifications. The slides were removed from the lysis solution and placed in the electrophoresis chamber, which was then filled with freshly made alkaline buffer (300 mM NaOH and 1 mM EDTA, pH 12.6). The cells were exposed to alkali for 40 min to allow for DNA unwinding and the expression of alkali-labile sites. Subsequently, the DNA was submitted to electrophoresis for 30 min at 300 mA and 25 V in an ice bath. All the above steps (preparation of slides, lysis and electrophoresis) were conducted without direct light in order to prevent additional DNA damage.
Positive controls were performed with 200 ml of whole human blood, incubated for 2 h at 37 °C with 50 ml of methyl methanesulfonate (final concentrations of 0.08 mM and 0.016 mM). The two concentrations were used to demonstrate different levels of damage and to ascertain the assay sensitivity.
After electrophoresis, the slides were placed in a horizontal position and washed three times (5 min each) with 0.4 M Tris buffer, pH 7.5, to neutralize the excess alkali. Finally, slides were fixed with absolute ethanol, stained with GelRed 1:500 (Biotium) and analyzed using a fluorescence microscope (Zeiss Axioplan with AxioCam MRc5 camera).
The degree of DNA damage (strand breaks) was classified according to the size and intensity of the tails of the comets, into 4 classes: 0 (no damage- no tail), 1 (small damage, small tail), 2 (larger damage, large tail), and 3 (complete damage, with a small comet head and most of the DNA in the tail) (Fig. 1). The analysis was performed by 3 observers, who evaluated 100 cells in each slide; the mean of the scores from the 3 observers was used to calculate the damage index (DI), as shown below (where a = number of cells scored 0 by observer 1, and so on):

Fluorescence microscopy images (× 400) showing examples of patterns of DNA damage in the comet assay. Left panel: Nucleoid structures depicting class 0 of damage (no tail) and class 1 (small tail). Middle panel: class 2 of damage (larger tail). Right panel: class 3 of damage (profound fragmentation, very large tail)
Damage class | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
Observer 1 | a | D | G | J |
Observer 2 | b | E | H | K |
Observer 3 | c | F | I | l |
Final score | A (mean of a, b, c) | B (mean of d,e,f) | C (mean of g,h,i) | D (mean of j, k, l) |
The mean of the DI from the duplicate slides was used as the final value for each patient. Additionally, the frequency of the damage classes (0–3) was calculated from the total number of evaluated cells.
One hundred and twenty slides were evaluated, corresponding to the 30 patients with two slides from blood samples collected before tracer injection and two slides from the blood samples collected after tracer injection. One of the slides (sample 12) was removed from the final data analysis due to processing error.
Statistical analysis
Variables with a normal distribution were demonstrated as mean and standard deviation; otherwise, they were demonstrated as medians interquartile ranges. Categorical variables were compared with chi-square, and continuous variables were compared with the Wilcoxon´s test. A value of p < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS™ (version 22).
Results
Patient population
Among the 29 individuals included in the analysis, age was 65.3 ± 9.9 years (47–85 years), 18 (62.1%) were male, 28 (96.6%) were hypertensive, 13 (44.8%) were diabetic, 14 (48.3%) were dyslipidemic, 16 (55.2%) were former smokers, 7 (24.1%) had prior myocardial infarction, 13 (44.8%) had a history of myocardial revascularization (percutaneous or surgical), and 5 (17.2%) had stable, angiographically confirmed coronary artery disease undergoing medical treatment. The injected radiotracer dose was 880.6 ± 229.4 MBq.
Comet assay
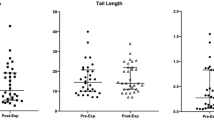
Overall, the medians of the DI before and after tracer injection were 22.7 and 27.8, respectively (p < 0.001) (Fig. 2 A). Figure 2B shows the DI of each patient.

Damage index before and after radiotracer injection. A Means, medians and interquartile ranges. B Values of damage index from each patient
Table 1 depicts the frequency of the damage classes before and after tracer injection. Most of the cells (approximately 70%) remained without DNA fragmentation (class 0) after tracer injection. There were nonsignificant increases of classes 1 and 2 of damage. Class 3 was the least frequent both before and after radiotracer injection, but displayed a significant, 44% increase after injection.
Discussion
Several types of stress, either environmental or organic, have genotoxic effects [15]. Ionizing radiation may promote oxidative stress, induce DNA strand breaks and affect cell components, even a few hours after irradiation [16, 17]. In medical imaging, radiation effects are considered stochastic, and mainly of two kinds, malignancy or heritable disease [18]. These effects are dose-dependent and follow a linear no-threshold model [19]. However, there is no direct evidence of cancer risk from cardiac imaging, but only projections from the epidemiological studies [20]. On the opposite end of this, studies at the “bench” level try to provide different types of evidence to help elucidate this issue.
The comet assay (single-cell gel electrophoresis) is one of the methods of choice for the evaluation and measurement of DNA damage. It is a simple, fast, precise, low-cost technique, in which cells are incorporated into an agarose matrix and then have their membranes lysed for the generation of nucleoid structures. Thereafter, DNA is untwined and undergoes electrophoresis. If there are bond breaks, the highly negative molecules move towards the anode [21, 22]. After staining and through visualization in a fluorescence microscope, a comet shape appears, with the nucleus in the head of the comet and the tail consisting of DNA strands or fragments which migrated to the anode. The relative intensity of the tail increases according to the intensity of damage caused by any agent, either ionizing radiation or chemical agents, for example [23].
In this study, even before exposure to ionizing radiation, 24% of the cells had evidence of some DNA damage, what recalls the variety of other factors that may lead to damage, such as smoking, diabetes, and indeed all currently recognized cardiovascular risk factors [24,25,26]. Importantly, even though there was an increase of the damage index and of classes 1–3 of damage, most cells remained in class 0. Shirazi et al. [9], also using the comet assay, showed that patients who received Tc-99m sestamibi or thallium-201 injections for MPI had evidence of DNA damage, compared to controls; however, repeated evaluations in the same patients (before/after radiotracer injection) were not available, and therefore a clear inference on the effect of ionizing radiation cannot be made. In the study by Varol et al. [10], among 27 children who underwent Tc-99m DMSA scintigraphy, DNA damage increased after the test, returning to normal levels after a week. Rief et al. [27] showed, by immunofluorescence, that strand breaks appeared after Tc-99m sestamibi injection for MPI and disappeared after 24 h. In the current study, a decrease of DNA damage with time could not be demonstrated, as patients were not re-evaluated later.
Additionally, even though DNA damage may occur, there are counteractive, self-protective mechanisms that contribute to reduce radiation effects. In fact, in response to DNA damage, cells activate repair genes [15]. Cheng et al. [28] have demonstrated that, after exposure to different types of ionizing radiation, the lymphocyte expression of mRNA of several repair genes was increased compared to controls. Won et al. [29] observed the activation of DNA repair pathways in patients who underwent MPI, by evaluating the phosphorylation of histone 2AX, protein p53 or serine/threonine protein kinase (ATM) in peripheral blood T lymphocytes by flow cytometry and immunohistochemistry, as well as the mRNA expression of repair genes such as BCL2 associated X, damage specific DNA binding protein 2, or Tp53 (a tumor-suppressing gene). Therefore, the biological consequences of DNA damage may be reduced by these mechanisms, helping minimize concerns about the effects of ionizing radiation used in MPI. Finally, new imaging protocols, using stress-only strategies, or new imaging hardware and software, which allow the use of very small radiotracer doses, may lead to further reductions in radiation-induced DNA damage from MPI.
Limitations
As the collection of the second blood sample was relatively “early” regarding the half-life of Tc-99m sestamibi, the extent of DNA damage induced by the tracer might have been underestimated. This timing was due to the presence of the patients in the Nuclear Medicine laboratory, which typically lasts for up to 90 min. Nonetheless, as Rief et al. have described after performing multiple blood sample analyses, strand breaks can be detected as early as 5 min after radiotracer injection, without major difference when compared to the 1-h sample [27]. Therefore, we believe that our data may be representative of near-maximal radiation effects on the DNA. Additionally, as pointed by Azqueta et al. [30], DNA repair mechanisms can also occur very quickly, and experiments assessing DNA damage should take care to avoid repair of strand breaks; so, in this context, a shorter timing may also be desirable. Furthermore, due to the cross-sectional nature of this study, a return of damage levels to baseline could not be assessed, as other blood samples were not collected later. Finally, the study was performed with relatively high tracer doses, and therefore the amount of DNA damage might have been overestimated and may currently be substantially less with hardware improvement and new test protocols.
Conclusions
In this patient sample, DNA damage was demonstrated in lymphocytes from patients undergoing MPI. However, most cells remained in class 0 damage after radiotracer injection. Further studies, including the evaluation of DNA repair, may help elucidate the genotoxic effects of MPI.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available, as they have not been anonymized. However, they may be made available from the corresponding author on reasonable request.
Abbreviations
- ATM:
-
Serine/threonine protein kinase
- DI:
-
Damage index
- DMSA:
-
Dimercaptosuccinic acid
- EDTA:
-
Ethylenediaminetetraacetic acid
- MPI:
-
Myocardial perfusion imaging
- NCRP:
-
National Council on Radiation Protection and Measurements
References
National Council on Radiation Protection and Measurements. Report No. 93—Ionizing Radiation Exposure of the Population of the United States. Bethesda, MD: 1987
National Council on Radiation Protection and Measurements. Report No. 93—Ionizing Radiation Exposure of the Population of the United States. Bethesda, MD: 2009
Einstein AJ, Berman DS, Min JK, Hendel RC, Gerber TC, Carr JJ, et al. Patient-centered imaging: shared decision making for cardiac imaging procedures with exposure to ionizing radiation. J Am Coll Cardiol. 2014;63:1480–9.
National Council on Radiation Protection and Measurements. Report No. 184—Medical Radiation Exposure of Patients in The United States. Bethesda, MD: 2019
Konotop F, Mattera P, Aranha IP. Cytogenetics analysis of human lymphocytes treated with 99m-technetium and its reducing agent stannous chloride: in vitro studies. Am J Hum Genet. 1998;63:141.
Monteiro GO, Oliveira NG, Rodrigues AS, Laires A, Ferreira TC, Limbert E, Leonard A, Gerber G, Rueff J. Cytogenetic alterations and oxidative stress in thyroid cancer patients after iodine-131 therapy. Mutagenesis. 2000;15:69–75.
Balakrishnan S, Rao SB. Cytogenetic analysis of peripheral blood lymphocytes of occupational workers exposed to low levels of ionizing radiation. Mut Res. 1999;442:37–42.
Lloyd DC, Purrot RJ, Dolphin GW. Chromosome aberration dosimetry in a case of over- exposure to radiation. Nature. 1973;241:69–78.
Shirazi MM, Shabestani-Monfared A, Shahidi M, Amiri M, Abedi SM, Borzoueisileh S, et al. Radio-adaptive response in myocardial perfusion imaging induced by technetium99m. Indian J Nucl Med. 2017;32:7–10.
Varol S, Öktem F, Koçyiğit A, Demir AD, Karataş E, Aydin M, et al. The impact of technetium-99m dimercapto-succinic acid scintigraphy on DNA damage and oxidative stress in children. Int J Clin Pract. 2021;75:1–7.
Schwartz JL. Alterations in chromosome structure and variations in the inherent radiation sensitivity of human cells. Radiat Res. 1998;149:317–8.
Klaude M, Eriksson S, Nygren J, Ahnström G. The comet assay: mechanisms and technical considerations. Mutation Res/DNA Repair. 1996;363:89–96.
Singh NP, Mccoy MT, Tice RR, Schneider EL. A simple technique for quantification of low levels of DNA damage in individual cells. Exp Cell Res. 1988;175:184–91.
Hartmann A, Speit G. Genotoxic effects of chemicals in the single cell gel (SCG) test with human blood cells in relation to the induction of sister-chromatid exchanges (SCE). Mut Res. 1995;346:49–56.
Khanna KK, Jackson SP. DNA double-strand breaks: signaling, repair and the cancer connection. Nat Genet. 2001;27:247–54.
Appella E, Anderson CW. Signaling to P53: breaking the posttranslational modification code. Pathol Biol (Paris). 2000;48:227–45.
Azzam EI, Jay-Gerin JP, Pain D. Ionizing radiation-induced metabolic oxidative stress and prolonged cell injury. Cancer Lett. 2012;327:48–60.
The ICRP. recommendations of the International Commission on Radiological Protection. Ann ICRP. 2007;2007(37):1–332.
Ron E. Cancer risks from medical radiation. Health Phys. 2003;85:47–59.
Einstein AJ. Effects of radiation exposure from cardiac imaging: how good are the data? J Am Coll Cardiol. 2012;59(6):553–65.
Enciso JM, Sánchez O, Cerain AL, Azqueta A. Does the duration of lysis affect the sensitivity of the in vitro alkaline comet assay? Mutagenesis. 2015;30:21–8.
Gajskia G, Žegurab B, Ladeirac C, Novakb M, Sramkovae M, Pourrutf B, et al. The comet assay in animal models: from bugs to whales – (Part 2 Vertebrates). Mutation Res-Rev Mutation Res. 2019;781:130–64.
Collins AR. The comet assay: a heavenly method! Mutagenesis. 2015;30:1–4.
Dasgupta P, Kinkade R, Joshi B, et al. Nicotine inhibits apoptosis induced by chemotherapeutic drugs by up-regulating XIAP and surviving. Proc Natl Acad Sci USA. 2006;103:6332–7.
Kushwaha S, Vikram A, Trivedi PP, Jena GB. Alkaline, endo III and FPG modified comet assay as biomarkers for the detection of oxidative DNA damage in rats with experimentally induced diabetes. Mutat Res. 2011;726:242–50.
Manfredini V, Biancini GB, Vanzin CS, Dal Vesco AM, Cipriani F, Biasi L, et al. Simvastatin treatment prevents oxidative damage to DNA in whole blood leukocytes of dyslipidemic Type 2 diabetic patients. Cell Biochem Funct. 2010;28:360–6.
Rief M, Hartmann L, Geisel D, Richter F, Brenner W, Dewey M. DNA double-strand breaks in blood lymphocytes induced by two-day 99mtc-MIBI myocardial perfusion scintigraphy. Eur Radiol. 2018;28:3075–81.
Cheng L, Brzozowska B, Sollazzo A, Lundholm L, Lisowska H, Haghdoost S, et al. Simultaneous induction of dispersed and clustered DNA lesions compromises DNA damage response in human peripheral blood lymphocytes. PLoS ONE. 2018;12:1–16.
Won HL, Nguyen P, Hu S, Liang G, Ong S, Han L et al. Variable activation of the DNA damage response pathways in patients undergoing SPECT myocardial perfusion imaging. Circul: Cardiovasc Imaging 2015; e002851
Azqueta A, Shaposhnikov S, Collins AR. DNA oxidation: investigating its key role in environmental mutagenesis with the comet assay. Mutation Res/Genet Toxicol Environ Mutag. 2009;674:101–8.
Acknowledgements
The authors thank Dr. Adriana Xavier de Brito for support at the Nuclear Medicine Laboratory, and Dr. Francisco Romeiro for assistance in patient recruitment.
Funding
This work was supported by the FAPERJ (Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by APA, JPP, AM and GD. The first draft of the manuscript was written by ADL and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Instituto Nacional de Cardiologia (number 67169717.6.0000.5272).
Consent for publication
Not applicable.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Competing interests
None of the authors have any conflict of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Arpini, A.P., De Lorenzo, A., Moritz, A. et al. Evaluation of DNA damage induced by ionizing radiation from myocardial perfusion imaging: a pilot study. BMC Cardiovasc Disord 22, 394 (2022). https://doi.org/10.1186/s12872-022-02839-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02839-8