
Abstract
Establishing specific reference intervals (RIs) of serum 25-hydroxyvitamin D3 [25(OH)D] for children is essential for improving the accuracy of diagnosis and prognosis monitoring of diseases such as rickets and growth retardation. The study including 6,627 healthy children was conducted to establish specific RIs of 25(OH)D for children in Nanning area of China. The results showed that there were statistically significant differences among age, season, and gender of serum 25(OH)D levels, and the age-specific RIs of serum 25(OH)D were 20.3 ~ 53.6 ng/mL for 0 ~ ≤ 1 year and 18.9 ~ 49.6 ng/mL for 2 ~ ≤ 3 years. The age-, season-specific RIs of serum 25(OH)D for 4 ~ ≤ 6 years in spring–summer and autumn–winter were 15.8 ~ 42.6 ng/mL and 15.2 ~ 37.7 ng/mL, respectively. The age-, gender-specific RIs of serum 25(OH)D for 7 ~ ≤ 18 years for males and females were 12.1 ~ 36.1 ng/mL and 10.8 ~ 35.3 ng/mL, respectively. This study successfully established the RIs of serum 25(OH)D, which may help to improve disease diagnosis and monitoring for children in the Nanning area of China.
Similar content being viewed by others

Introduction
Vitamin D is a fat-soluble steroid vitamin that is essential for the absorption of calcium from the gut and its deposition in the bones [1]. Deficiency of vitamin D in children is associated with a multitude of health problems, including skeletal dysplasias, autoimmune diseases, and neurological disorders [2, 3]. 25-hydroxyvitamin D3 [25(OH)D] is the primary circulating form of vitamin D with a relatively high blood content and half-life of 2–3 weeks, which is the most reliable biological marker to assess vitamin D levels [4]. According to previous studies, a variety of elements can influence the 25(OH)D level, such as dietary habits, exposure to sunlight, demographic information (e.g., age and gender), and geographical elements (e.g., season and latitude) [5, 6]. Appropriate reference intervals (RIs) of serum 25(OH)D for children would provide more accurate evidence for the clinical diagnosis and prognostic monitoring of diseases, such as rickets, growth retardation, muscle weakness, and periodontitis. However, there is a lack of appropriate 25(OH)D RIs for children currently, and numerous clinical laboratories still apply RIs determined from adults or from other countries' populations. Accordingly, this study was performed to investigate the influence of age, season, and gender on 25(OH)D levels, and established specific RIs of 25(OH)D for children in Nanning, China.
Materials and methods
Participants and recruitment
Referring to the Clinical and Laboratory Standards Institution (CLSI) [7], the research project recruited participants aged 0–18 years old from the Nanning area of China who had received regular physical examinations, nutritional surveillance, and growth monitoring at the Guangxi International Zhuang Medicine Hospital from August 2018 to May 2021. Data for the study was collected by indirect sampling methods to gather information from the hospital's Laboratory Information System (LIS). The criteria for exclusion from the study were as follows: (1) individuals with metabolic diseases, including rickets, obesity, thyroid disease, and Cushing's syndrome; (2) those with recent acute or chronic illnesses related to the heart, liver, lung, kidney, or musculoskeletal system; (3) a family history of diabetes, malignant tumors, parathyroid, and calcium-regulated diseases; (4) those who had recently undergone surgery; (5) those who had recently taken medications that affect the absorption and metabolism of vitamin D, such as vitamin D supplements, glucocorticoids, anticonvulsants, and HAART (AIDS Treatment); (6) laboratory test results that were out of standard ranges, including body mass index (BMI) (0 ~ ≤ 1 year: 14.0–18.0 kg/m2; 2 ~ ≤ 3 years: 13.0–18.5 kg/m2; 4 ~ ≤ 6 years: 14.0–18.5 kg/m2; 7 ~ ≤ 18 years: 14.0–23.8 kg/m2), serum parathyroid hormone (PTH) (15–68.3 pg/mL), serum ionized calcium (Ca2+) (2.15–2.55 mmol/L), serum thyroid stimulating hormone (TSH) (0.35–4.94 µIU/mL), and serum procalcitonin (PCT) (0–0.5 µg/L). Outliers were removed using Tukey's formula [Q1—1.5 × IQR, Q3 + 1.5 × IQR]. A total of 6,627 apparently healthy individuals were included in the study, with 4,979 being employed to establish RIs and 1,648 being utilized for validating RIs. The healthy individuals were categorized into four age groups: 0 ~ ≤ 1 year (infancy); 2 ~ ≤ 3 years (toddlers); 4 ~ ≤ 6 years (preschool age); and 7 ~ ≤ 18 years (adolescence). Additionally, it was divided into two gender groups: male and female, and four season groups: spring (March ~ May), summer (June ~ August), autumn (September ~ November), and winter (December ~ February). The research protocol was approved by the Guangxi International Zhuang Medicine Hospital (No. 2022-047-01).
Specimen collection and quality control
Participants were required to fast for 8 h and avoid vigorous exercise for 24 h prior to the collection of a blood sample. Venous blood (2–4 mL) was collected in coagulation-promoting tubes and then centrifuged at 3,000 revolutions per minute for 10 min. The separation of the serum was tested on the Abbott ARCHITECT i2000SR system by the Chemiluminescent Microparticle Immunoassay (CMIA) method within 2 h. Additionally, to ensure the accuracy of the results, Internal Quality Control (IQC) and Performance Qualification (PQ) tests were conducted in compliance with ISO 15189 standards. The system's calibration, linearity, and precision were evaluated by the reference method. Aligning all the tests' analytical performance results with the manufacturer's requirements, the next operation can be commenced.
Establishment and verification of the RIs
According to the CLSI, the groups with statistical significance were separated, while the groups with no statistical significance were incorporated into a group to establish the RIs. The non-parametrical calculation of percentiles 2.5th and 97.5th were used to calculate the RIs with sample size ≥ 120.
A validation group of 1,648 healthy children was used to validate the accuracy of the established RIs. The validation individuals were categorized into groups according to age, season, and gender-specific RIs, with a sample size of at least 20 in each group. If the validation values are within the range of the RIs for more than 90%, the RIs can be deemed valid. Otherwise, another 20 validation individuals need to be chosen to reassess the results.
Statistical analysis
The R 4.2.2, IBM SPSS 26.0, and Microsoft Office Excel 2019 Softwares were used for statistical analysis, and all statistical processes were conducted in accordance with CLSI C28-A3 guidelines [7]. The data distribution was described using the Kolmogorov–Smirnov test, and outliers were calculated with Tukey's formula [Q1-1.5 × IQR, Q3 + 1.5 × IQR]. For the non-normally distributed data, medians with quartiles were presented. Spearman's correlation analysis was use to assess the relationship between the 25(OH)D level and age. Nonparametric data were compared by the "ggpubr" R package (version 4.2.1) using the Wilcoxon test and visualization by a violin plot. Bonferroni adjustment was applied for multiple significance tests, and statistical significance was determined by a P-value of less than 0.05. RIs were calculated by the nonparametric approach based on the 2.5th and 97.5percentiles. The validation groups were used to verify the established RIs and a passing rate of greater than 90% indicated the RIs were effective.
Results
Characteristics of the study subjects
After analyzing the clinical records of the participants and removing the outliers, a total of 6,627 healthy children were selected, with 4,979 were used to establish RIs and 1,648 were employed for validating them (Fig. 1). The characteristics of the study subjects were summarized in Table 1.

Flow diagram of establishing RIs for 25(OH)D. RIs reference intervals, 25(OH)D 25-hydroxyvitamin D3
Comparison of 25(OH)D levels among different age, season and gender subgroups
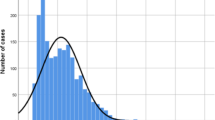
The data of serum 25(OH)D was skew distribution according to the analysis of the Kolmogorov–Smirnov test (P < 0.05), and statistics of 25(OH)D level were presented as medians with quartiles. Results of statistical analysis revealed that 25(OH)D levels declined with age increasing (r = −0.52, P < 0.05), showing statistically significant differences in the 0 ~ ≤ 1 year, 2 ~ ≤ 3 years, 4 ~ ≤ 6 years, and 7 ~ ≤ 18 years age groups (all P < 0.001, Fig. 2A, B). Additionally, there were differences between males and females in their serum 25(OH)D levels (P < 0.05, Fig. 2C). Moreover, the serum 25(OH)D levels in summer were significantly higher than in winter, while lower than in autumn (all P < 0.05). There were no statistically significant differences between the serum 25(OH)D levels in autumn and winter, or in spring and summer (all P > 0.05, Fig. 2D). Consequently, the autumn and winter groups were incorporated into an autumn–winter group, the spring and summer groups were merged into a spring–summer group.

Comparison of 25(OH)D levels among different age, season and gender groups. A The vioplot showed the differential expression of 25(OH)D levels among different age groups. B Identifying the correlation between 25(OH)D levels and age for healthy children. C The vioplot showed the differential expression of 25(OH)D levels between different genders. D The vioplot showed the differential expression of 25(OH)D levels among seasons. 25(OH)D 25-hydroxyvitamin D3
Differences of 25(OH)D levels among genders and seasons for the same age groups
Statistical analysis revealed that males aged 7 ~ ≤ 18 years old had significantly higher 25(OH)D levels than females (P < 0.05, Fig. 3D). However, there was no significant difference between males and females aged 0 ~ ≤ 6 years (all P > 0.05, Fig. 3A–C). Additionally, a significant difference in serum 25(OH)D level was observed between spring–summer and autumn–winter in 4 ~ ≤ 6 years (P < 0.05, Fig. 3G). No significant differences were observed between spring–summer and autumn–winter in 0 ~ ≤ 1 year, 2 ~ ≤ 3 years, and 7 ~ ≤ 18 years (all P > 0.05, Fig. 3E, F and H). As a result, the RIs among 4- ≤ 6 years were divided by seasons, while those among 7 ~ ≤ 18 years were divided by gender.

Gender and seasons differences for 25(OH)D levels in different age groups. A–D The vioplot showed the differential expression of 25(OH)D levels between different genders in different age groups. E–H The vioplot showed the differential expression of 25(OH)D levels between different seasons in different age groups. 25(OH)D 25-hydroxyvitamin D3
Establishment and verification of the RIs
The RIs were determined by the non-parametrical calculation of percentiles 2.5th and 97.5th. The age-specific RIs of serum 25(OH)D were 20.3 ~ 53.6 ng/mL for 0 ~ ≤ 1 year and 18.9 ~ 49.6 ng/mL for 2 ~ ≤ 3 years. The age-, season-specific RIs of serum 25(OH)D for 4 ~ ≤ 6 years in spring–summer and autumn–winter were 15.8 ~ 42.6 ng/mL and 15.2 ~ 37.7 ng/mL, respectively. The age-, gender-specific RIs of serum 25(OH)D for 7 ~ ≤ 18 years for males and females were 12.1 ~ 36.1 ng/mL and 10.8 ~ 35.3 ng/mL, respectively (Table 2). Subsequently, 1648 healthy subjects were selected to verify the established RIs, with more than 20 cases in each validation group. Finally, it was found that the percentages of passing rate for all validation values were greater than 90%, indicating that the RIs established in this study were effective (Table 2).
Discussion
Vitamin D deficiency has become a global health issue, especially in children [8]. Statistics from a 2017 Chinese Epidemiological Survey show that 23.2% of Chinese children suffer from Vitamin D deficiency [9]. A study conducted in England between 2008 and 2014 revealed a 15- fold rise in the number of young people with vitamin D insufficiency [10]. Similarly, a 2018 study in India showed that 41.9% of children and adolescents had inadequate levels of vitamin D [11]. Vitamin D deficiency can lead to poor bone formation and a higher risk of fractures [12]. Additionally, research has suggested that insufficient levels of vitamin D may be connected to cardiovascular disease, various kinds of cancer, and diabetes [13,14,15,16]. Early diagnosis and appropriate vitamin D supplementation can reduce the prevalence of the disease. In this research, we established gender-, age-, and season-specific RIs of serum 25(OH)D for children, providing more accurate evidence for diagnosing and treating the disease.
Our findings indicated that there were statistically significant variations in the 0 ~ ≤ 1 year, 2 ~ ≤ 3 years, 4 ~ ≤ 6 years, and 7 ~ ≤ 18 years age groups (all P < 0.001), and the serum 25(OH)D levels decreased with age increasing, which is in agreement with prior studies [17,18,19]. The trend may be attributed to the young children's daily intake of vitamin D-rich infant formula as well as fortified baby foods, while adolescents' lack of outdoor activities and inadequate vitamin D supplementation. In addition, adolescents experience a period of accelerated growth, which necessitates a considerable amount of vitamin D for the development of healthy musculoskeletal and neurological systems. Another important finding was that the level of serum 25(OH)D in males was significantly higher than in females aged 7 ~ ≤ 18 years (P < 0.05), which is consistent with the European children, southern Chinese and Iranian children [19, 20]. This can be attributed to the male hormone levels, as testosterone is believed to have a positive correlation with the levels of 25(OH)D [21, 22]. A different study, however, suggested that there was no significant distinction based on sex, race, or age [23]. These variations could be associated with lifestyle elements, such as dietary habits and outdoor activities of the studied population. It was discovered that the serum 25(OH)D levels during summer were significantly lower compared to autumn, while higher than in winter (all P < 0.001). The findings for the seasonal fluctuation in serum 25(OH) levels were close to those from other research projects carried out in the Zigong area and southern China [17, 20]. The varying levels of 25(OH)D can be explained by the amount of sunlight exposure, since it is mainly acquired through exposure to the sun's UV rays that activate its production in the skin. Compared to the autumn–winter groups, the 25(OH)D concentration for children aged 4 ~ ≤ 6 years was higher in the spring–summer groups, which could be attributed to the lack of light exposure and outdoor activities in the cold winter months.
This study investigated the age-, season- and gender-specific RIs of serum 25(OH)D for healthy children (0–18 years old) in the Nanning area, which is located in 22.5° north latitude. The levels of serum 25(OH)D in Nanning (22.5° north) were found to be higher than those in Shanghai (30.5° north) and Sichuan (27.5° north), which could be attributed to the difference in geographical latitudes [24, 25]. As the reports suggest, the further away from the equator, the lower the concentrations of 20(OH)D and the higher the prevalence of Vitamin D insufficiency presenting in children due to the decreased amount of sunlight [26]. In addition, the higher serum 25(OH)D levels in our study may be explained by the differences in detection methods, as the metabolites in the serum will increase cross-reactivity with the antibodies in the CMIA, whereas the liquid chromatography tandem mass spectrometry (LC–MS/MS) method is less affected by the metabolites. Moreover, the serum 25(OH)D RIs in this research were more precise and different from the reagent manufacturer's recommended levels (≥ 20 ng/mL), which can be attributed to the age range, ethnic group, and geographical area of the sample population, as the sample of the reagent manufacturer comprises of African-American, Hispanic, and Caucasian adults from the 48 contiguous states of the U.S. In the validation test, the passing rates for all validation groups were greater than 90%, indicating that the established RIs in the current study were effective, which will be more accurate and significant for clinical diagnosis of diseases in children. However, one major limitation of this research is that there are no specific RIs of 25(OH)D for other special populations, such as elderly and pregnant women. Therefore, further researches based on a wider range of people should be performed to establish more comprehensive RIs.
Availability of data and materials
The dataset generated and/or analyzed during this study are available from the corresponding author on reasonable request.
References
Randev S, Kumar P, Guglani V (2018) Vitamin D supplementation in childhood - a review of guidelines. Indian J Pediatr 85(3):194–201
Li Y, Wang J, Cai Y et al (2023) Association of serum vitamin D with periodontal disease. Int Dent J 73(5):777–783
Chibuzor MT, Graham-Kalio D, Osaji JO et al (2020) Vitamin D, calcium or a combination of vitamin D and calcium for the treatment of nutritional rickets in children. Cochrane Database Syst Rev 4(4):CD012581
Brett NR, Lavery P, Agellon S et al (2016) Dietary vitamin D dose-response in healthy children 2 to 8 y of age: a 12-wk randomized controlled trial using fortified foods. Am J Clin Nutr 103(1):144–152
Yousef S, Manuel D, Colman I et al (2021) Vitamin D status among first-generation immigrants from different ethnic groups and origins: an observational study using the Canadian health measures survey. Nutrients 13(8):2702–2725
Yousef S, Elliott J, Manuel D et al (2019) Study protocol: Worldwide comparison of vitamin D status of immigrants from different ethnic origins and native-born populations-a systematic review and meta-analysis. Syst Rev 8(1):211–216
Clinical and Laboratory Standards Institute(CLSI) (2010) Defining, establishing, and verifying reference intervals in the clinical laboratory; Approve guideline-Third Edition CLSI document EP28-A3c[S]. Wayne USA
Hu Y, Chen J, Wang R et al (2017) Vitamin D nutritional status and its related factors for Chinese children and adolescents in 2010–2012. Nutrients 9(9):1024–1033
Wang S, Shen G, Jiang S et al (2017) Nutrient status of vitamin D among Chinese children. Nutrients 9(4):319–328
Basatemur E, Horsfall L, Marston L et al (2017) Trends in the diagnosis of vitamin D deficiency. Pediatrics 139(3):e20162748
Mustafa A, Shekhar C (2021) Concentration levels of serum 25-Hydroxyvitamin-D and vitamin D deficiency among children and adolescents of India: a descriptive cross-sectional study. BMC Pediatr 21(1):334–343
Yang G, Lee WYW, Hung ALH et al (2021) Association of serum 25(OH)Vit-D levels with risk of pediatric fractures: a systematic review and meta-analysis. Osteoporos Int 32(7):1287–1300
Liu Y, Li X, Zhao A et al (2018) High prevalence of insufficient vitamin D intake and serum 25-hydroxyvitamin D in Chinese school-age children: a cross-sectional study. Nutrients 10(7):822–834
Föcker M, Antel J, Ring S et al (2017) Vitamin D and mental health in children and adolescents. Eur Child Adolesc Psychiatry 26(9):1043–1066
Zhou A, Selvanayagam JB, Hyppönen E (2022) Non-linear Mendelian randomization analyses support a role for vitamin D deficiency in cardiovascular disease risk. Eur Heart J 43(18):1731–1739
Holick MF, Chen TC (2008) Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr 87(4):1080S-1086S
Yu J, He X, Huang S (2021) The establishment of serum 25-hydroxyvitamin D reference intervals in children aged 0–14 years in Zigong area. China J Physiol Anthropol 40(1):14–20
Qorbani M, Mahdavi GA, Ejtahed H et al (2021) Percentile values for serum levels of vitamins A and D in Iranian children and adolescents: The CASPIAN-V study. Nutrition 90:111307
Wolters M, Intemann T, Russo P et al (2022) 25-Hydroxyvitamin D reference percentiles and the role of their determinants among European children and adolescents. Eur J Clin Nutr 76(4):564–573
Cai Z, Zhang Q, Xia Z et al (2020) Determination of serum 25-hydroxyvitamin D status among population in southern China by a high accuracy LC-MS/MS method traced to reference measurement procedure. Nutr Metab (Lond) 17:8–20
Al-Daghri NM, Yakout SM, Ansari MGA et al (2021) Vitamin D metabolites and sex steroid indices in postmenopausal women with and without low bone mass. Metabolites 11(2):86–93
D’Andrea S, Martorella A, Coccia F et al (2021) Relationship of vitamin D status with testosterone levels: a systematic review and meta-analysis. Endocrine 72(1):49–61
Saenger AK, Laha TJ, Bremner DE et al (2006) Quantification of serum 25-hydroxyvitamin D(2) and D(3) using HPLC-tandem mass spectrometry and examination of reference intervals for diagnosis of vitamin D deficiency. Am J Clin Pathol 125(6):914–920
Gao Z, Xu M, Yuan M et al (2017) Preliminary investigation for the reference intervals of serum 25-hydroxyvitamin D among minors in Shanghai. Lab Med 32(4):280–283
Wang J, Li X, Gan Y et al (2022) Comparison of the serum total 25-hydroxyvitamin D concentrations using chemiluminescent immunoassay and liquid chromatography-tandem mass spectrometry in children. J Nutr Sci Vitaminol (Tokyo) 68(3):181–188
Durazo-Arvizu RA, Camacho P, Bovet P et al (2014) 25-Hydroxyvitamin D in African-origin populations at varying latitudes challenges the construct of a physiologic norm. Am J Clin Nutr 100(3):908–914
Acknowledgements
None.
Funding
Youth Project of Guangxi International Zhuang Medicine Hospital (NO. [2022]203), Discipline Project of Guangxi International Zhuang Medicine Hospital (NO. [2021]33), Research Fund of Guangxi International Zhuang Medicine Hospital (NO. RCYJ202201).
Author information
Authors and Affiliations
Contributions
The primary research plan was created by ZDY and PQL. The data analysis, chart production and manuscript writing were undertaken by ZDY, PQL, WSM, ZCL, WYH and WXM. ZDY, YST and YLL additionally provided assistance with data gathering and reference assembly. All authors participated in the article's development and gave their consent to the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Guangxi International Zhuang Medicine Hospital (No. 2022-047-01) approved the research protocol.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Zhou, Dy., Wei, Sm., Zhu, Cl. et al. Age-, season- and gender-specific reference intervals of serum 25-hydroxyvitamin D3 for healthy children (0 ~ 18 years old) in Nanning area of China. J Physiol Sci 74, 2 (2024). https://doi.org/10.1186/s12576-023-00895-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12576-023-00895-z