
Abstract
Background
Ensuring the integrity of sperm DNA is of paramount importance for the production of healthy offspring. The process of sperm formation involves intricate molecular adjustments that condense and safeguard its genetic material. However, the risk posed by sperm DNA fragmentation (SDF) can impede natural and assisted fertility and may arise from various testicular and post-testicular factors. While there are recommendations against routine SDF testing, recent research has sparked debate by demonstrating the positive impact of such testing on fertility outcomes.
Objective
To identify the factors associated with SDF among infertile individuals.
Methods and materials
The medical records of infertile men referred to our hospital were comprehensively reviewed and included in the study as they met the inclusion criteria. Patients dissatisfied with participation in the study or those with incomplete medical records were excluded. The association of SDF, sperm analysis, and demographic characteristics were evaluated for further investigation.
Results
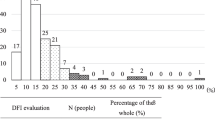
The average age of participants was 36.1 ± 8.1 years. The average semen volume was 2.5 ± 0.3 cc with a semen pH of 7.4 ± 0.2. The average sperm count was 10.9 ± 0.7 million, sperm motility was 36.9 ± 2.4%, and normal sperm morphology was 41.7 ± 2.7%. SDF levels below 15% were seen in 27.9%, between 15 and 30% in 32.4%, and above 30% in 39.7% of patients. Significant associations were found between the SDF and various factors in sperm analysis, including sperm count (P < 0.001), semen volume (P < 0.001), semen pH (P < 0.001), sperm motility (P < 0.001), normal sperm morphology (P < 0.001), and age (P < 0.001). Moreover, alcohol consumption (P = 0.04), smoking (P = 0.01), and the presence of varicocele (P = 0.03) were significantly associated with.
Conclusion
This study emphasizes the significance of SDF among individuals experiencing infertility and investigates its correlation with various sperm test parameters. It also sheds light on the vital roles played by factors such as age, smoking, alcohol consumption, and the presence of varicocele, which are highly likely to cause variations in SDF levels. The results of our research will add to the existing pool of knowledge on infertility and potentially have implications for clinical practice and the care of patients.
Similar content being viewed by others


1 Background
Infertility is a significant issue affecting reproductive-aged couples and societies. Hence, after one year of unprotected sexual intercourse, pregnancy is not achievable. Determining changes in infertility prevalence poses challenges. Potential reasons for its rise include delayed parenthood, lifestyle habits like smoking and alcohol consumption impacting semen and oocyte quality, shifts in sexual behavior, and the gradual decline of societal taboos [1]. The origin of infertility can be attributed to male, female, or both, with many cases remaining unexplained. Therefore, simultaneous evaluation of both partners is necessary [2]. Understanding the genetic basis of male-associated factors in infertility is essential for effective detection and discovering more efficient remedies for infertile couples [3, 4]. Recent research shows that 30–40% of infertility cases are due to male factors, including urinary tract abnormalities, genitourinary infections, hormonal disorders, genetic abnormalities, and immune factors [5]. Semen analysis plays a significant role in diagnosing and assessing the effectiveness of treatment. Factors such as sperm count, acidity, morphology, motility, and volume are evaluated to identify male infertility issues [6]. While the initial semen sample is essential, it may not distinguish between fertile and infertile men, underscoring the importance of cellular and nuclear factors in male infertility [7].
Sperm DNA fragmentation (SDF) results from various cellular events that damage sperm's DNA and affect fertility. These include abnormal chromatin packaging during spermatogenesis, excessive reactive oxygen species (ROS) production, reduced seminal antioxidants, and apoptotic events during sperm maturation [8, 9]. Factors like toxins, pollutants, medications, smoking, age, and varicocele may also increase the amount of SDF [10, 11]. SDF is related to reproductive failure, making it crucial in assessing infertile men. SDF is a good predictor of outcomes of assisted reproductive technology (ART) techniques, such as blastocyst formation, pregnancy, and birth rate [12]. Various methods, including the alkaline comet test, terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL), sperm chromatin dispersion (SCD), and sperm chromatin structure assay (SCSA), are employed to assess SDF, with the alkaline comet test exhibiting superior predictive ability for male infertility [13]. While SDF assessment is available, its precise clinical significance remains to be determined. Due to insufficient evidence, the routine use of SDF in evaluating male infertility has yet to be accepted [14].
A complete understanding of factors influencing SDF might be helpful with the aim of restoring fertility. This study aimed to assess SDF amounts in the sperm analysis of infertile individuals and the factors influencing it. By examining outcomes associated with each SDF result in sperm parameters, we aim to identify the factors related to SDF among infertile individuals.
2 Methods and materials
This cross-sectional descriptive study was conducted at Azad University hospitals from January 2020 to December 2021. The study enrolled 68 men referred to our hospitals due to infertility. Men were included in the study using a convenience sampling method, their SDF factor, and semen analysis results. Demographic information was also obtained through a comprehensive medical examination and history taking. The study included men diagnosed with infertility who had at least one year of unprotected intercourse without contraceptive intervention, aged between 20 and 48 years. Patients [1] dissatisfied with participation in the study, [2] those with incomplete medical records, [3] significant systemic illness, [4] the background of radiation therapy, chemotherapy, inflammation of the testicles, exposure to harmful substances, injury, torsion, and [5] long-term medication use were excluded.
Semen samples were obtained from 68 infertile patients undergoing treatment at the ART center. Within one year of intercourse without contraception in sexually active couples, the inability to conceive served as infertility. Based on the amount of SDF in the sperm of each individual, they were assigned to three subpopulations. Subpopulation A included patients with SDF < 15%, subpopulation B had SDF between 15–30%, and subpopulation C included those with SDF > 30%. Following 2–6 days of not having sex, the antegrade technique was applied for sample collection. Analysis was performed according to the World Health Organization criteria [15, 16]. Liquid nitrogen was used for SCSA to freeze the small amount of semen obtained from each patient. However, fresh semen samples were used to perform the other tests [13]. The Ethics Committee of Azad University of Medical Sciences, Tehran, Iran, approved the research. The study complied with the ethical standards outlined in the 1964 Declaration of Helsinki, as revised in 2000 (Approval code: IR.IAU.TMU.REC.1400.296). All participants signed informed written consent before the study. Data analysis was performed using SPSS software (version 26.0). Quantitative variables were described with mean ± SD (standard deviation), and frequency was used to describe qualitative variables. The ANOVA test was used to compare quantitative variables across multiple qualitative groups, exceeding two in number. The Chi-square test was utilized to analyze qualitative variables. A significance level of P-value < 0.05 was used to determine statistical significance.
3 Results
Herein, 68 men were analyzed. Primary analysis revealed that the average age of the patients was 36.1 ± 8.1 years, with the youngest being 20 years and the oldest being 48 years. The average height of the patients was 175.5 ± 4.6 cm, with the shortest being 168 cm and the tallest being 184 cm. The average weight of the patients was 73.5 ± 11.5 kg, with the lightest being 56 kg and the heaviest being 93 kg. Demographic characteristics are summarized in (Fig. 1) based on subpopulations. The average semen volume in the patients was 2.5 ± 0.3 mL, with the lowest volume of 2 mL and the highest volume of 3.2 mL. The mean pH of semen was 7.40 ± 0.2, with the lowest level being 7.2 and the highest level being 7.9. Regarding sperm characteristics, the average sperm count was 20.9 ± 0.7 million, with the lowest count being 10.1 million and the highest count being 30.7 million (Table 1).

Demographic characteristics
The analysis also showed a significant relationship between varicocele and SDF percentage, with patients with varicocele showing a higher SDF percentage (P = 0.03). Additionally, a meaningful association was found between alcohol consumption and SDF percentage, with patients who consumed alcohol having a higher SDF percentage (P = 0.04). Similarly, a significant relationship was found between tobacco consumption and SDF percentage, with patients who consumed tobacco showing a higher SDF percentage (P = 0.01).
However, no significant association between the SDF and height (P = 0.22), weight (P = 0.47), and employment status (P = 0.11) was discovered (Fig. 2).

Acquired variables of the patients
4 Discussion
Various environmental toxins and pollutants, certain medications, chemical exposures, cigarette smoking, certain infectious diseases, varicocele, and advancing age can contribute to increased SDF, which is one of the important causes of male infertility. Our goal is to identify the factors associated with SDF among individuals who are experiencing infertility. Generally, three major factors are discussed in male infertility: decreased sperm count, reduced motility, and abnormal sperm morphology [17]. The selection of natural and mature sperm is essential for the success of assisted reproductive techniques [18]. Improving sperm motility would enhance the success rate of a treatment cycle [19].
Armand Zini and colleagues evaluated standard sperm parameters, DNA denaturation (DD), and DNA fragmentation (DF) in healthy and infertile men. The study revealed a strong correlation between DF and DD in sperms with higher levels of sperm DNA damage in infertile individuals, indicating a relationship between male infertility and weak sperm DNA integrity [20, 21].
American Center of Reproductive Medicine explored various methods of SDF analysis. Among the methods studied were TUNEL and SCD, which were used to assess the fragmented DNA in sperm samples using microscopy or flow cytometry. Fernandez proposed a technique called SCD to measure SDF, wherein sperm DNA is exposed to an acidic solution in a culture medium, leading to chromatin dispersion, which is then visible under a fluorescent microscope. After comparing the two methods, TUNEL was more reliable and accurate when combined with semen analysis in predicting male infertility [22].
Aamir Javed also indicated that the SCD, SCSA, TUNEL, and alkaline comet assays effectively distinguish between fertility and infertility, with the alkaline comet assay being the best predictor of male infertility [13].
To investigate the effect of SDF on various sperm parameters, including volume, count, pH, morphology, and motility, Ahmad Majzob conducted sperm analysis on 100 fertile and 1168 infertile men, aimed to explore the impact of SDF and oxidation–reduction potential on male infertility. The results indicated that an increase in SDF levels correlated with higher percentages of sperm head defects, highlighting the significance of morphology among the sperm parameters and its crucial role in male infertility [23].
According to an investigation by Minh Tam Le, the relationship between body mass index (BMI) and metabolic syndrome in infertile men was studied. Sperm analysis, glucose tolerance test, and blood lipid profile were assessed. A significant association was revealed between SDF levels and obesity in infertile men [24]. However, our findings could have been more consistent with this study, as we found no significant relationship between SDF levels and BMI.
Varicocele is reported as a common cause of infertility, exhibiting lower sperm motility, concentration, and morphologic defects, culminating in an increase in SDF amounts. While some studies explored the relationship between varicocele and SDF, there is limited information regarding the potential reduction of metabolic oxidative stress in varicocele patients [25].
The present study evaluated the association of varicocele with the possible increase in sperm oxidation and SDF index among infertile men. Hence, findings from infertile men with varicocele and men with natural sperm production without varicocele were compared. Semen samples were collected and evaluated according to the guidelines, and oxidation–reduction (mV) potential was measured. The SDF index was measured using the SCSA. Only samples with a sperm concentration of more than 106 sperm per mL were included for comparison. Infertile men with varicocele had significantly lower average sperm concentration, motility, and total sperm count than the fertile control group.
In contrast, infertile men with varicocele had higher oxidation–reduction potential and more elevated average serum FSH levels and SDF levels than the fertile control group. The oxidation–reduction potential was higher in varicocele patients and positively correlated with the SDF amounts. Moreover, the oxidation–reduction potential and SDF index significantly negatively correlated with sperm parameters (sperm motility, concentration, and total sperm count) in infertile men with varicocele [23, 25].
One of the fundamental issues affecting fertility is the lack of sperm motility or poor progressive motility [26].
A study reported that none of the sperm parameters, including motility, count, and morphology, are considered individually as the sole disruptive factor; instead, all three elements are involved in fertility outcomes [27].
Investigations on DNA damage suggest a significant and inverse association between SDF and embryo formation, blastocyst development, and fertility [28].
The etiology of sperm DNA damage is multi-factorial and may result from internal factors, such as deficient protamine levels, excessive ROS, and apoptosis. External factors, including medications, chemotherapies, smoking, inflammation of the reproductive system, increased testicular temperature (e.g., hot baths, saunas, certain occupations like welding, bakeries), improper diet, alcohol consumption, obesity, prolonged driving, and varicocele [28,29,30]. Increased ROS leads to cellular membrane damage and impairs sperm motility, possibly correlating with SDF [31]. However, even in men with normal sperm motility and other normal semen parameters, SDF levels exceeding 30% can still be observed. Apart from helping to investigate infertility origin in a couple, SDF analysis can aid in decision-making when ART is needed [32, 33]. It has been shown that intrauterine insemination is unsuccessful in men with a 30% DNA Fragmentation Index (DFI). Therefore, laboratory-assisted techniques such as intracytoplasmic sperm injection (ICSI) or in vitro fertilization (IVF) should be used [20, 21].
Assessing sperm DNA damage in infertile couples, even when a male partner has a standard analysis of semen, is recommended for selecting the most appropriate ART. Studies investigating sperm DNA damage before and after varicocelectomy have shown that patients with varicocele have significantly higher sperm DNA damage than the control group. It has also been demonstrated that varicocelectomy has increased sperm DNA integrity following the procedure [34, 35].
Regarding the limited data available from studies, further research is required to elucidate SDF’s clinical significance on sperm DNA damage. Currently, varicocelectomy is a suitable option to reduce the amounts of SDF and, thus, a practical approach to restore or improve fertility. SDF analysis may also be appropriate for monitoring post-surgical outcomes following varicocele repair [35].
The small sample size is one of the limitations of this study, necessitating further research with a larger sample size. Larger sample sizes can enhance statistical accuracy and provide more reliable results. Similar case–control studies can be conducted to explore the impact of SDF on infertility.
5 Conclusion
This study emphasizes the significance of SDF among individuals experiencing infertility and investigates its correlation with various sperm test parameters. It also sheds light on the vital roles played by factors such as age, smoking, alcohol consumption, and the presence of varicocele, which are highly likely to cause variations in SDF levels. The results of our research will add to the existing pool of knowledge on infertility and potentially have implications for clinical practice and the care of patients.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Brugo-Olmedo S, Chillik C, Kopelman S (2001) Definition and causes of infertility. Reprod Biomed Online 2(1):41–53
Krausz C, Riera-Escamilla A (2018) Genetics of male infertility. Nat Rev Urol 15(6):369–384
Shaoqin G, Zhenghui Z, Xueqian Z, Yuan H (2014) Epigenetic modifications in human spermatozoon and its potential role in embryonic development. Yi Chuan 36(5):439–446
Stein D, Ukogu C, Ganza A, Gounko D, Lee J, Bar-Chama N et al (2019) Paternal contribution to embryonic competence. Cent Eur J Urol 72(3):296–301
Zeqiraj A, Beadini S, Beadini N, Aliu H, Gashi Z, Elezaj S et al (2018) Male infertility and sperm DNA Fragmentation. Open Access Maced J Med Sci 6(8):1342–1345
van der Horst G, Skosana B, Legendre A, Oyeyipo P, du Plessis SS (2018) Cut-off values for normal sperm morphology and toxicology for automated analysis of rat sperm morphology and morphometry. Biotech Histochem 93(1):49–58
Denomme MM, Mann MR (2013) Maternal control of genomic imprint maintenance. Reprod Biomed Online 27(6):629–636
Kuchakulla M, Narasimman M, Khodamoradi K, Khosravizadeh Z, Ramasamy R (2021) How defective spermatogenesis affects sperm DNA integrity. Andrologia 53(1):e13615
Gosálvez J, López-Fernández C, Fernández JL, Esteves SC, Johnston SD (2015) Unpacking the mysteries of sperm DNA fragmentation: ten frequently asked questions. J Reprod Biotechnol Fertility 4:2058915815594454
Sharma R, Biedenharn KR, Fedor JM, Agarwal A (2013) Lifestyle factors and reproductive health: taking control of your fertility. Reprod Biol Endocrinol 11:66
Lafuente R, Garcia-Blaquez N, Jacquemin B, Checa MA (2016) Outdoor air pollution and sperm quality. Fertil Steril 106(4):880–896
Korshunov MN, Korshunova ES, Darenkov SP (2020) Sperm DNA fragmentation: etiology, pathogenesis, the influence on reproductive function. UroRep 10(4):337–345
Javed A, Talkad MS, Ramaiah MK (2019) Evaluation of sperm DNA fragmentation using multiple methods: a comparison of their predictive power for male infertility. Clin Exp Reprod Med 46(1):14–21
Tatem AJ, Brannigan RE (2017) The role for sperm DNA damage testing in 2017. Transl Androl Urol 6(Suppl 4):S448–S449
Blickenstorfer K, Voelkle M, Xie M, Frohlich A, Imthurn B, Leeners B (2019) Are WHO recommendations to perform 2 consecutive semen analyses for reliable diagnosis of male infertility still valid? J Urol 201(4):783–791
WHO manual for the standardized investigation (2001) diagnosis and management of the infertile male. Urology 57(1):208
Panahi A, Mirza Ahmadi S, Asaadi TG (2022) Comparison between SPATA18 and P53 Gene Expressions in the sperm cells obtained from normospermic and asthenospermic samples: a case-control study. Int J Fertil Steril 16(2):122–127
Ghasemi A, Amjadi F, Masoumeh Ghazi Mirsaeed S, Mohammad Beigi R, Ghasemi S, Moradi Y et al (2019) The effect of Myo-inositol on sperm parameters and pregnancy rate in oligoasthenospermic men treated with IUI: a randomized clinical trial. Int J Reprod Biomed. 17(10):749–756
Timar M, Banaei S, Mehraban Z, Salimnejad R, Golmohammadi MG (2022) Protective effect of saponin on sperm DNA fragmentation of mice treated with cyclophosphamide. Andrologia 54(2):e14336
Dutta S, Henkel R, Agarwal A (2021) Comparative analysis of tests used to assess sperm chromatin integrity and DNA fragmentation. Andrologia 53(2):e13718
Zini A, Bielecki R, Phang D, Zenzes MT (2001) Correlations between two markers of sperm DNA integrity, DNA denaturation and DNA fragmentation, in fertile and infertile men. Fertil Steril 75(4):674–677
Panner Selvam MK, Agarwal A (2018) A systematic review on sperm DNA fragmentation in male factor infertility: laboratory assessment. Arab J Urol 16(1):65–76
Majzoub A, Arafa M, Mahdi M, Agarwal A, Al Said S, Al-Emadi I et al (2018) Oxidation-reduction potential and sperm DNA fragmentation, and their associations with sperm morphological anomalies amongst fertile and infertile men. Arab J Urol 16(1):87–95
Le MT, Nguyen DN, Le DD, Tran NQT (2020) Impact of body mass index and metabolic syndrome on sperm DNA fragmentation in males from infertile couples: a cross-sectional study from Vietnam. Metabol Open 7:100054
Tanaka T, Kobori Y, Terai K, Inoue Y, Osaka A, Yoshikawa N et al (2022) Seminal oxidation-reduction potential and sperm DNA fragmentation index increase among infertile men with varicocele. Hum Fertil (Camb) 25(1):142–146
Alizadeh A, Mirzaahmadi S, Asaadi Tehrani G, Jabbara N (2022) A comparative assessment of RNF38 and P53 genes expression in the sperm samples obtained from males with normozoospermia and asthenospermia: a case-control study. Int J Reprod Biomed 20(12):1019–1028
Javanmard F, Bidmeshkipour A, Ghasemian YJ (2022) Ceratonia siliqua L improved cryodamage of asthenozoospermic specimens: an experimental study. Int J Reprod Biomed 20(12):1029–1038
Dadgar Z, Shariatzadeh SMA, Mehranjani MS, Kheirolahi A (2023) The therapeutic effect of co-administration of pentoxifylline and zinc in men with idiopathic infertility. Ir J Med Sci 192(1):431–439
Schisterman EF, Sjaarda LA, Clemons T, Carrell DT, Perkins NJ, Johnstone E et al (2020) Effect of folic acid and zinc supplementation in men on semen quality and live birth among couples undergoing infertility treatment: a randomized clinical trial. JAMA 323(1):35–48
Sharma R, Agarwal A, Rohra VK, Assidi M, Abu-Elmagd M, Turki RF (2015) Effects of increased paternal age on sperm quality, reproductive outcome and associated epigenetic risks to offspring. Reprod Biol Endocrinol 13:35
Evenson DP, Djira G, Kasperson K, Christianson J (2020) Relationships between the age of 25,445 men attending infertility clinics and sperm chromatin structure assay (SCSA(R)) defined sperm DNA and chromatin integrity. Fertil Steril 114(2):311–320
Sabbaghian M, Hosseinifar H, Rafaee A, Gilani MAS (2022) Assessment of the impact induced by different incubation time, storage time, storage medium and thawing methods on sperm DNA fragmentation assay: a before-after study. J Hum Reprod Sci 15(4):377–381
Peng T, Liao C, Ye X, Chen Z, Li X, Lan Y et al (2023) Machine learning-based clustering to identify the combined effect of the DNA fragmentation index and conventional semen parameters on in vitro fertilization outcomes. Reprod Biol Endocrinol 21(1):26
Chen YW, Niu YH, Wang DQ, Li H, Pokhrel G, Xu H et al (2018) Effect of adjuvant drug therapy after varicocelectomy on fertility outcome in males with varicocele-associated infertility: systematic review and meta-analysis. Andrologia 50(8):e13070
Qiu D, Shi Q, Pan L (2021) Efficacy of varicocelectomy for sperm DNA integrity improvement: a meta-analysis. Andrologia 53(1):e13885
Acknowledgements
We are grateful for the efforts of the staff of the Azad University hospitals in Tehran, Iran.
Funding
There is no funding received for this article.
Author information
Authors and Affiliations
Contributions
R.V: project development, supervision, review and editing manuscript. B.N: supervision, review and editing manuscript, data collection and management S.J: writing and editing original draft, data collection and management M.D: writing and editing original draft, data collection and management. MM.D: writing and editing original draft, data collection and management. P.TN: writing and editing original draft, data collection and management. N.R: supervision, analyzing data, data collection and management. HR.M: supervision, analyzing data, writing and editing original draft, data collection and management.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee of Azad University of Medical Sciences, Tehran, Iran, approved the research. The study complied with the ethical standards outlined in the 1964 Declaration of Helsinki, as revised in 2000 (approval code: IR.IAU.TMU.REC.1400.296). All participants signed informed written consent before the study.
Consent for publication
Identifiable information/ images in open access journal was obtained from all study participants.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Valipour, R., Narouie, B., Jadidi, S. et al. Evaluation of sperm DNA fragmentation index among infertile individuals: a comprehensive analysis of the associated factors—a cross-sectional study. Afr J Urol 30, 37 (2024). https://doi.org/10.1186/s12301-024-00439-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-024-00439-w