
Abstract
Physical assistive robotics are oriented to support and improve functional capacities of people. In physical rehabilitation, robots are indeed useful for functional recovery of affected limb. However, there are still open questions related to technological aspects. This work presents a systematic review of upper limb rehabilitation robotics in order to analyze and establish technological challenges and future directions in this area. A bibliometric analysis was performed for the systematic literature review. Literature from the last six years, conducted between August 2020 and May 2021, was reviewed. The methodology for the literature search and a bibliometric analysis of the metadata are presented. After a preliminary search resulted in 820 articles, a total of 66 articles were included. A concurrency network and bibliographic analysis were provided. And an analysis of occurrences, taxonomy, and rehabilitation robotics reported in the literature is presented. This review aims to provide to the scientific community an overview of the state of the art in assistive robotics for upper limb physical rehabilitation. The literature analysis allows access to a gap of unexplored options to define the technological prospects applied to upper limb physical rehabilitation robotics.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.1 Introduction
Disabilities affect people’s quality of life and limit the development of physical activities related to their impairment [1]. According to statistics from the World Health Organization (WHO), more than one billion people over the world have a disability, of which 16.5% suffer of motor impairments. These numbers may increase due to aging, chronic diseases, and musculoskeletal disorders [2]. Motor impairment is the partial or total loss of a body part function, usually the lower or upper limbs, due to diseases and pathologies that affect bones, muscles, or joints. Injuries can have different origins as neurological, vascular, or infectious, and can be degenerative diseases [2]. A high level of demand in the execution of repetitive or high-impact activities, or an accident at work, home, or traffic can also be the cause of motor impairments [1, 3, 4]. Thus, the most frequent alterations occur in the ligamentous or tendinous structures, such as carpal tunnel syndrome, tendinitis, soreness (e.g., bursitis), and traumas (e.g., fractures) [5, 6].
In all cases, a physical rehabilitation process is required to restore a person socially, physically, and occupationally, after suffering any musculoskeletal disorder [7,8,9]. Thus, physiotherapy focuses on improving the patient’s motor functions. To regain limb functionality, the patients undergo treatments that include exposing the muscular tissues to stress progressively and appropriately, increasing the range of mobility and muscle strength, and preventing the appearance of chronic pain [10,11,12,13,14,15,16]. As part of the rehabilitation process, assistive robotics support physiotherapy, meeting the needs of the exercises and patients to provide an adequate intervention depending on the level of affection [17, 18]. The use of these technologies has increased in the last few years due to the use of instrumentation to quantify variables such as range of movement, velocities, muscle activity, and force [19,20,21].
Robotic technologies can be applied in health and medical areas. Several applications have emerged to support clinical processes such as surgery procedures and diagnostic studies [22], logistics and monitoring [23, 24], social robots in mental health [25], physical rehabilitation [26, 27], and assistive devices for the support of user´s daily activities or day-to-day tasks [28]. In the case of rehabilitation, robots are used to assist the physiotherapy processes or to replace or support the performance of the functions associated with a limb [29, 30]. Then, rehabilitation robotics include prostheses, orthoses, and rehabilitation systems that are divided into exoskeleton-type systems and end-effector-type systems [31,32,33]. The devices in this domain can also be classified by their expected role (i.e., the same robotic device can be used for different purposes in health care, depending on the patient’s prognosis and the device design and functionalities). Rehabilitation robots may be used for recovery or compensatory purposes, physical training or other applications whose purpose is improving the rehabilitation processes and the quality of life of a person in the shortest possible time [8]. However, it is important to determine how robotic systems provide help according to the principles of rehabilitation (A: Avoid aggravation, T: Timing, C: Compliance, I: Individualization, S: Specific sequencing, I: Intensity, T: Total patient) [7,8,9]. Therefore, one of the most important challenges is related to the definition of physical interactions between humans and robots. Additionally, there is a need for a framework to characterize and systematize criteria for the design, evaluation, and quantification methods that robotic systems employ in rehabilitation.
Rehabilitation robots can work with different assistance levels. For example, according to the force applied to the patient’s level of progress, the assistance can be divided into: (1) Passive, which implies total robot intervention [34, 35], (2) active-assistive, which requires partial robot intervention, (3) isotonic, which means no robot intervention in motion [21, 35, 36], (4) isometric, in which there is robotic-supplied static muscle level contraction, and (5) resistive, where there is a robotic-supplied dynamic muscle strengthening [21, 37]. The assistance modes allow the parameterization of the exercises according to the patients’ condition, being one of the design criteria together with the need for accurate measurements such as ranges of motion and force to evaluate the patients’ progress, as well as to acquire the necessary information for the robot control system and the definition of control strategies [21, 33]. The definition of qualitative variables associated with rehabilitation has been a great challenge [38, 39]. Even if the inclusion of rehabilitation robots in conventional processes has gradually increased [21], the quantification of variables increases the complexity of these types of systems due to the number of sensors required or the computational consumption of deep estimation algorithms [40].
In addition to variable quantification, control strategies have been extensively proposed for rehabilitation robotic systems, such as impedance controls or admittance controls. For example, EXO-UL8 use assistance modes and high transparency in the physical human-robot interaction through admittance controls [41]. Control strategies like impedance and admittance controls have diversified as new strategies that seek naturally moderate intensity of intervention when required. It also provides continuous monitoring of the patient’s condition [35, 42,43,44]. Moreover, the development of technologies for assistive robotics is sought to make a integral monitoring of processes to adapt the conditions of execution of a conventional routine with an added value. For example, [45] has developed an exoskeleton-type system (ANYexo), where the range of movement (ROM) and the control strategies are optimized to mimic the interaction of therapists using impedance controls. Assistive systems have become an increasingly popular option over the last few years. There are assistive systems commercially available that have been widely used in physical rehabilitation. For instance, the rehabilitation kit for upper limbs developed by Hocoma [46] or the end-effector-based rehabilitation system InMotion [47]. Other commercial systems like ALEx kinetek, has incorporated virtual reality systems as part of the rehabilitation process [48]. Nevertheless, despite the commercial robotic systems, it still being a challenge the positioning of robotics as permanent support in all kinds of medical processes [49].
The human-robot interaction in the field of robotics applied to physical rehabilitation is progressively improving. However, despite the existence of substantial evidence in assistive robotic systems, to the best of our knowledge, there is no assistive system that can comprehensively provide all the necessary tools to the therapist to carry out a complete monitoring in the rehabilitation process, to improve therapy times and recovering the patient’s quality of life and functionality. This may be due to the fact that, during rehabilitation, training is often based on the subjective perception and observation of the specialist. Along with the difference in fatigue perception, as patients find it difficult to correctly express the actual fatigue state. In addition, patients’ responses are diversified and more features should be extracted to reflect additional details of the patient’s compensation and condition. The greatest challenge is positioning robotics as permanent support in all kinds of medical processes [49]. In this work, we develop a systematic review for upper limb rehabilitation systems. The purpose of this manuscript is to review the state of the art related to physical assistive robotics through active human-machine interaction, analyze the technologies that have been recently developed, and identify gaps in the research and justifies future research in this area.
A systematic review of the scientific literature constitutes the first step for understanding the current scientific progress. The purpose of this manuscript is to review the state of the art related to physical assistive robotics through active human-machine interaction for upper limb rehabilitation and analyze technologies that have been recently developed. This study focuses on aspects related to physical robotic assistive systems for upper limb rehabilitation. We exclude works related to lower limb and devices without any active actuation. We analyze control strategies, quantification and instrumentation methods, integration of complementary technological methods, and integration of virtual reality systems.
A rigorous methodology allows the systematic review of the literature and the selection of publications for extracting the information. First, we describe the methodology used to carry out the search based on the keyword’s selection and the exclusion criteria. Afterward, we present the bibliometric results, including three aspects: (1) A bibliographic analysis of the metadata, which describes the evolution of the publication by years, journals, and countries; (2) an analysis of the occurrences with the metadata extracted from the selected articles; (3) the taxonomy used to sort the upper limb assistive robotics devices and technologies for physical rehabilitation. Then, we analyze the works reported in the literature in control strategies, quantification of monitoring variables, complementary instrumentation, and integration of virtual reality systems. Finally, we discuss the main topics in the extracted works, and we give some conclusions and prospects regarding the analysis carried out in this review.
2 Methodology
In this section, we present the bibliometric analysis conducted for the systematic review of the literature. We begin with the keywords selection and the query string construction from a hierarchical organization. Subsequently, we assign Boolean operators to the keywords according to their level of importance. Afterward, we collected the articles from the search in the databases, and we filtered them using inclusion and exclusion criteria related to the focus of this review. The literature review was conducted from August 2020 to April 2021 and is carried out considering the last six years because we intend to report and analyze the latest advances in this field. The results from older works usually serve as a reference for the consolidation of the improvements in works presented in this article.
2.1 Keyword Selection
We proceed to perform the keyword selection. Figure 1 shows the hierarchical keyword selection diagram, where three main levels were considered. In first level, a preliminary selection of works related to the main area was carried out using the query “Assistive robotics for upper limb rehabilitation” in IEEE database. After this process, we select the most relevant keywords related to the findings and according to terms of thesaurus defined by IEEE [50]. Therefore, the main keywords selected were: “rehabilitation”, “upper limb”, and “robotics”.

Hierarchical Keyword Selection Diagram
Another additional terminology was included on the second level, according to different areas of interest related to the human-machine interaction. As a result, other keywords were included in the research process: “rehabilitation robotics”, “technology”, “virtual reality”, “control”, and “diagnosis”. The third level includes synonyms and complementary words to the second level, including “assistive devices”, “assistive robotics”, “devices”, “haptics”, “adaptive control”, “robust control”, and “diagnostic”. Synthesizing, the hierarchy allows to build the search query in a more organized way by distributing the most relevant keywords to the topic located in the first level, and from there, a set of complementary keywords located in the second level, and a set of synonyms are placed at the third level, that as well defines the Boolean relation between the keywords. The first level contains the main words that are mandatory to be included and therefore, the “AND” operator is assigned. The second level includes the complementary words of the main field of study and therefore the “OR” operator is assigned. The third level contains synonyms and complements of the higher levels and the “OR” operator is also assigned, but these words are concatenated in the words of the second level. The third level contains terms that can refine the search. We can choose not to include them if generalization is desired. The fourth level corresponds to the excluded words with the logical operator “NOT”, but in this case, it is not considered. Therefore, the final search query corresponds to: {“Rehabilitation” AND “Robotics” AND “Upper limb” AND (“Rehabilitation robotics” OR (“Assistive devices” OR “Assistive robotics”) OR “Technology” OR (“Devices”) OR “Virtual reality” OR (“Haptics”) OR “Control” OR (“Adaptive control” OR “Robust control”) OR “Diagnosis” OR (“Diagnostic”))}.
2.2 Search Strategy
An extensive search was carried out using constructed query string with keywords chosen from Figure 1. Only indexed journals in English were considered. The databases used for the search were IEEE Xplore®, Scopus (Elsevier), Science Direct, and Web of Science. The Medline/PubMed database handles more practical and medical aspects that focus on presenting clinical validations of systems already developed using clinical trials, randomized controlled trials, systematic reviews, and meta-analysis of the literature. We intend to analyze technological aspects of engineering for robotic systems applied to physical rehabilitation. For this reason, this database was not considered in this review.
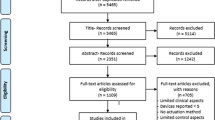
Our search strategy aims to identify and analyze technological features regarding upper limb rehabilitation robotic systems. We intend to study the latest developments of control strategies, quantification methods, complementary instrumentation, and virtual reality integration. Our objective with this review is to identify issues still unexplored in the literature that will allow us to develop criteria to systematize evaluation methods, in order to make a comparison of studies that lead to the development of robotic systems that provide integral assistance as a permanent support to physical rehabilitation processes. Articles are included when: (1) Upper limb rehabilitation systems are used and based on end-effector or exoskeletons devices; (2) proposed control strategies for improving the robot-patient experience; (3) virtual reality is included as a support to the rehabilitation robotic systems; (4) complementary instrumentation and measurement methods are used for the quantification of therapy assessment variables; (5) mechanical designs are developed and proposed to increase ROM (range of motion) and (6) systems with active actuation only. The formulation of the search strategy was based on the PRISMA statement for reporting systematic reviews as shown in Figure 2.

Systematic review flow chart
2.3 Exclusion Criteria
This study is limited to health care-type technologies that are focused on upper limb rehabilitation and strategies for recovering the functionality of the affected joint. We consider practical aspects of the technologies used for upper limb rehabilitation. The systematic review excludes articles related to rehabilitation technologies applied to lower limbs, and articles related to prostheses and orthosis without any contribution of active functionality. Only works in English were included in this systematic review.
3 Search Results
In this section, we describe the results of the data extraction phases and the analysis performed. We include a bibliographic analysis of the publications’ evolution by year, journal, and the two principal countries that publish works in this topic. Finally, we analyze the concurrences and the taxonomy of the literature.
Following the search strategy of the scheme defined in Figure 2, the preliminary search in the four databases resulted in 820 articles: 101 from IEEE Xplore, 314 from Scopus, 235 from ScienceDirect, and 170 from Web of Science. As mentioned previously, we consider the articles published from 2015 to 2021. After removing duplicate articles and subsequently reviewing titles and abstracts, a total of 203 articles were obtained. Then, after reading the full texts and applying the inclusion criteria, 137 articles were excluded, resulting in a total of 66 articles for the review (see Figure 2). We analyzed the concurrency network based on the metadata obtained from the articles included in this review. The metadata were obtained, classified, and encoded through the bibliographic administrator Mendeley.
3.1 Bibliographic Analysis
In this section, we present a bibliographic analysis of the metadata. We describe the evolution of publications by year, journal, countries.
1) Evolution of publications by year, journal and countries: The articles were selected and classified according to the number of publications in journals related to assistive robotics for upper limb rehabilitation. Based on the literature review, the highest number of articles on assistive robotics for upper limb rehabilitation was published in 2018 (13 articles) followed by 2019 (11 articles). The journals with the highest number of publications in upper limb assistive robotic systems are Robotics and Autonomous Systems (7 articles), IEEE/ASME Transactions on Mechatronics (6 articles) and IEEE Transactions on Neural Systems and Rehabilitation Engineering (6 articles). The countries with more articles in this field are China and Italy with 21 and 9 articles respectively. In terms of content, 34 articles were reviewed to deal with rehabilitation methods, therapeutic exercise execution and trajectory generation, mechanical design, and kinematic-dynamic analysis, and 12 articles present control strategies for assistive robotics systems for rehabilitation. The remaining 20 articles address quantification and instrumentation techniques, and systems that use virtual reality.
3.2 Occurrence Network
From the extracted articles, we carried out an occurrence analysis to identify the most used keywords in the bibliography. We used the bibliographic manager Mendeley to compile and organize the extracted articles, since the list of keywords is usually very extensive. Using this software, we extracted a .RIS file to generate a concurrence map using the VOSviewer tool, to find the relationship between the articles included. In this way, we obtained a relation of concurrence. The most relevant terms are: “rehabilitation robotics” (21 occurrences), “upper limb” (15 occurrences), “stroke” (11 occurrences), “exoskeleton” (9 occurrences), “rehabilitation” (9 occurrences), “human-robot interaction” (7 occurrences) and wearable robotics (6 occurrences). The concurrence network in Figure 3 shows the frequency of occurrence of the keywords and their matching network. It is worth to mention that only the terms with 3 or more connections are shown. The terms were divided into clusters considering the similarity measures and the distance between them. Thus, the keywords “rehabilitation robotics” (red), “upper limb”, “stroke” (blue), “exoskeleton” (yellow), “wearable robotics” (green), were the most frequent terms. This network also groups by coloring keywords with the highest number of associations between them, showing the keywords with more links. For example, “rehabilitation robotics” (red) is associated with terms “upper limb”, “stroke” and “exoskeleton”, but it is not directly associated with terms “bilateral” and “robot-assisted” (purple) because they are not widely used and are separate from the other terms in the concurrence network. With these correlations obtained from Figure 3, we can deduce that the literature mainly addresses aspects associated with exoskeletons, impedance control, force control, wearable robotics, kinematic analysis, iterative learning control, haptic interfaces, virtual reality, therapeutic exercises, assessment, activities of daily living, elbow and bilateral rehabilitation.

Concurrence network diagram
4 Rehabilitation Robotics Reported in the Literature
We present a general overview of upper limb assistive robotic systems reported in the literature. We address issues related to therapeutic exercise execution and trajectory generation, mechanical design optimization and kinematic-dynamic analysis. Then, we discuss specific topics such as control techniques, quantification or estimation techniques and instrumentation, and virtual reality inclusion as part of rehabilitation processes.
The classification of keywords and occurrences in this study suggests different classes and sub-classes. For this reason, a taxonomy is built from keywords with the support of the resulting concurrence network from Figure 3. The taxonomy of the literature is presented in Figure 4. Notice that several subcategories of the main classes are identified, but the main ones are upper limb and rehabilitation robotics.

Taxonomy of literature
Based on the technologies associated with upper limb support and rehabilitation and supported by taxonomy from Figure 4, we propose the classification presented in Table 1. We extracted, organized and categorized some important aspects such as name of the device, aim joints for rehabilitation, physical movements performed, type of device (exoskeleton, end-effector or robot arm) and number of degrees of freedom (DoF), sensing or measurement variables, disease to be treated, control technique used, virtual reality systems, first author, and year of publication. Note that if more than one work by the same author is found, the information is crossed and collected in the same row as a whole.
Rehabilitation robots have been proposed in order to guide and support physical rehabilitation processes that can easily be adapted according to the level of intervention that the patient requires in order to recover the functionality from mobility impairments or musculoskeletal disorders [51]. Notable examples of robotic systems reported in the literature highlight various innovative approaches and technologies used in rehabilitation robotics, including different control strategies, types of assistance, and levels of adaptability to patient needs (see Figure 5). We have evidenced some technologies used to implement assisted rehabilitation, such as remote rehabilitation or rehabilitation from a camera and bilateral systems, for example, the HX [52], or the CBM-Motus [53]. Devices that focus on telerehabilitation methods such as HX [52] have certain advantages such as avoiding traveling to rehabilitation centers, performing therapies from home, or having immediate access to rehabilitation. However, there are some drawbacks, such as the cost of the equipment and its maintenance. Moreover, the network connection may provide poor interaction with the specialist, which is a disadvantage because the therapist intervention is needed to monitoring the patient. Besides, the therapist can make decisions regarding the device use and the exercises that the patient should carry out, as well as the levels of assistance [52]. An uninterrupted telemonitoring strategy is needed between the patient and the specialist. Therefore, personal interaction can be more beneficial due to the continuous accompaniment of the specialist.

Examples of upper limb rehabilitation robots reported in the literature: (a) The Modified Physiotherabot [35], (b) ETS- MARSE [55], (c) HapticMaster (MOOG Inc. FCS) [58], (d) End-effector upper limb rehabilitation robot (EULRR) [60], (e) NURSE-2 [56], (f) BRANDO [94], (g) UR5 and UR10 (Universal Robots A / S) [61], (h) Armeo Power by Hocoma [46]
On the other hand, the evaluation of the strength and ROM is usually carried out as a result of the execution of passive, active, and active-assistance therapeutic exercises. The evaluation is also based on kinematics, muscle stimulation, pain relief, massage, and relaxation. Desired rehabilitation trajectories and standard training protocols are generated according to the level of recovery for task execution in the workspace. In the case of end-effector type devices, rehabilitation is performed by combined Cartesian movements. Some devices reported in the literature where these methods of evaluation and trajectory standardization have been applied for rehabilitation are for example, the Modified Physiotherabot [44], RETRAINER-ARM [54], ETS-MARSE [55], NURSE-2 [56, 57], HapticMaster (MOOG Inc. FCS) [58], BULReD [59], end-effector upper limb rehabilitation robot (EULRR) [60] and a commercial type such as UR5 and UR10 (Universal Robots A / S) [61, 62].
In literature, we find some methods to improve rehabilitation performance such as gravity compensation [63, 64], virtual impedance [65], interaction based on sEMG [66, 67], guided training and self-training [68] as implemented by Softhand X (SHX) [63], Rehand [66], EMU [64], RECUPERA [68] and TTI-Exo devices (TTI is the Toyota Technological Institute) [65]. Similarly, there are limitations regarding the lack of force sensors as in RECUPERA [63]. This may be conditioned by constraints such as the number of sensors, costs or the need of more accurate measurements. Likewise, in the literature, different actuation systems are analyzed. For instance, bio-inspired actuators based on shape memory alloys [69], cable transmission [70], adaptive and elastic mechanisms [71], variable stiffness actuation [45, 72,73,74], and alternatively, pneumatic actuation [75], used in devices like Auxilio [70], Soft-SixthFinger devices + SaeboMAS [72], parallel wrist rehabilitation robot (PWRR) [75], NeuroExos Shoulder-Elbow Module (NESM) [74] and ANYexo [45].
Another important aspect in the performance of robotic systems is the mechanical design. Systems are designed according to the biomechanical characteristics of the required joint, but anatomically it is complex to design a system that shares perfect alignment with the joint while preserving the maximum range of motion. In the literature, there are some works that seek to improve the conditions of mechanical coupling, such as Ref. [76] where tensegrity is proposed to approximate real movements more accurately, or also in Ref. [77], where mechanical postural synergies are developed to reduce the complexity of transmission mechanisms. Moreover, in Ref. [45], an exoskeleton (ANYexo) has been developed, in which the range of motion (ROM) is optimized to mimic the interaction of therapists. Another example is the TTI-Exo [65], which has adjustable link lengths to partially align the human and exoskeletal joints to avoid uncontrolled forces caused by hyperstaticity. In this case the limitation remains in the loss of mobility ranges, usually to avoid the collision of the robotic system with the patient; for example, when performing a shoulder adduction-abduction exercise [45, 78], but preserving to a greater extent the mobility ranges.
On the other hand, the selection of materials for the design of lighter and more compact systems plays an important role. It implies considering features such as lightness, robustness, hardness and durability, and are based on biomechanical characteristics for the joint to be treated. However, in the field of medicine and rehabilitation, there are standards in the selection of materials for manufacturing medical devices and equipment such as IEC 60601 [79]. Metals such as stainless steel, titanium or aluminum, ceramics, polymers, composites and biomaterials are the most widely used in the medical and rehabilitation industry under these standards [80, 81]. One of the advantages of using plastics in medicine is their relatively low cost compared to metallic materials. Plastics can be molded into useful configurations that would be difficult or impossible to duplicate in metals, and can be fabricated using technologies such as 3D printing [82,83,84,85]. Also, some composites are strong and flexible. The most commonly used resins in medical plastics are polyvinyl chloride (PVC), polyethylene, polypropylene, and polystyrene. However, polycarbonates, ABS, polyurethanes, polyamides, thermoplastic elastomers, polysulfones and polyetheretherketone (PEEK) are finding specialized applications in medical devices, especially where high performance is required [82, 83, 86, 87]. Some works reported interesting variations such as the design of lightweight devices built in 3D printing technologies [88] and lightweight exoskeletons as proposed by Ref. [89]. Other examples, such as CRUX system (Compliant Robotic Upper-extremity eXosuit) [76] and Co-Exos [90] are highlighted. Carbon-based polymer composites are increasingly being used for the design of rehabilitation robotic systems because of their ease of fabrication compared to metals. For example, the CLEVERarm [91, 92] has links made of 3D printed carbon fiber reinforced plastic for a lightweight and compact design. The use of carbon fiber reinforced links for upper limb exoskeletons has already been explored. Also, the use of carbon fiber reinforced polymer tubing is a low-cost alternative, this is used for example in ANYExo’s design [45]. The use of this material using 3D printing technologies is an advantage due to the possibility of manufacturing lightweight parts in a customized and simple way with a functional structural rigidity. Other emerging alternative materials such as NylonX, which consists of nylon reinforced with micro carbon fibers, are becoming more popular in manufacturing parts with high level of performance because it is considered as “engineering grade” material [93].
Additional to the therapy function, these technologies point to ease of prototyping parts and reduces manufacturing costs. The design of the system must guarantee perfect coupling between the robotic system and the human limbs. For instance, authors such as Ref. [65], have proposed design strategies in TTI- Exo system which has adjustable link lengths to partially align the human and exoskeletal joints in an attempt to prevent the uncontrolled forces caused by hyperstaticity.
In the following subsections, we will present specific topics to be analyzed such as control techniques employed, quantification or estimation techniques and instrumentation, and systems that include virtual reality as part of rehabilitation processes.
(1) Control techniques in assistive robotics: A critical issue of rehabilitation devices is related to the ranges of motion and the required constraints to avoid harming the user. Control strategies allow defining position and velocity constraints, as well as preventing undesired behavior due to disturbances. In this section, we include works regarding control strategies associated with assistive robotics. These works correspond to 20.75% of the reviewed literature.
The controllers’ implementation is oriented to imitate the movements carried out by a therapist and provide a certain level of support (passive, assistive, isotonic, isometric, and resistive) regarding both the joint position and the force applied. In several cases, impedance control is the most appropriated and used technique to simulate the assistance provided by the system under the concept of assist-as-needed (AAN) [43, 94,95,96], which consists of an assistance intensity control based on impedance controls. In AAN mode, the robot no longer needs to provide full support during the motion trajectory, whereas the robot can prompt patients to use their muscle forces while trying to stay with the predefined motion trajectory. Training intensity can be adjusted to meet patient needs according to the level of difficulty.
The AAN strategy is a widely rehabilitation mode assistance used in the literature. Works such as Refs. [34, 35, 43, 53, 60, 64, 65, 71, 74, 89, 95,96,97,98,99,100,101] have proposed and developed control strategies for the management of rehabilitation systems based on ANN. The advantages of employing this type of strategies are due to the nature of the formulation (based on a damped spring-mass system behavior). The implementation is geared to mimic the movements performed by a therapist and to provide a certain level of support in both joint position and applied force. However, research is needed to optimize the impedance parameters, integrating them with the clinical experience of physiotherapists, to improve the effectiveness of rehabilitation, as well as other evaluation parameters such as pain, which directly or indirectly reflect the adaptability that the control can provide at all times. On the other hand, literature reports the implementation of adaptation strategies for impedance and admittance controls, and complementary strategies such as sEMG estimation as part of the control as proposed by Ref. [102] where control methods are used to minimize muscle energy for robotic systems that support the movements of a user under unknown external disturbances, using electromyographic signals (sEMG) or in the case of Ref. [103] where an adaptive impedance control is implemented using biological signals. Similarly, in the literature, adaptive controls based on backstepping are proposed using estimation strategies [104, 105], or alternatively with inclusion of neural systems, in Ref. [97], a backstepping adaptive fuzzy based impedance controller is proposed, or neuro-fuzzy adaptive control (NFAC) strategies [97, 106, 107]. In addition, hybrid control models involving two or more strategies have been proposed, as in Refs. [108, 109], where a control based on a motion intensity perception model involving multimodal fusion between kinematic acceleration signals and heart rate signals is proposed to classify motion intensity with the support of deep neural networks.
(2) Quantification or estimation techniques in assistive robotics: Estimation is a process that physiotherapists often employ when assessing the patient for diagnosis or rehabilitation. The availability of measurement tools can decrease the need of estimation. However, the only variable that the physiotherapist can measure is angular position or range of motion in addition to functional tests. Other variables such as strength and pain are based on qualitative scales like Daniels or Oxford force scale [110] and Visual Analog Scale (EVA) [111] that give a numerical approach. The therapist requires information on the rehabilitation processes and improvement of the patient’s condition to make decisions based on quantitative pointers. Thus, monitoring the rehabilitation process is a key feature of assistive robotic systems.
In this context, quantifying evaluation variables associated with monitoring and tracing processes in rehabilitation is necessary. This section includes works directly related to quantification and estimation techniques incorporated into assistive robotics. These works correspond to 20.75% of the literature reviewed. The quantification strategies allow quantifying the variables associated with the evaluation of the patient’s condition. Some variables are obtained through the estimation using mathematical models or approximate measurement signals.
Estimation techniques have been proposed to a large extent to reduce the number of sensors used in an assistive system. The literature reports joint estimation techniques for human arm joints in rehabilitation tasks [112, 113], other works report rehabilitation by electrical stimulation estimation with sEMG to enhance joint movements [114,115,116,117,118], fatigue compensation and measurements from sEMG [119]. Additionally, continuous decoding methods based on multiple linear regression have been developed for myoelectric control, functional joint assessment for muscle force quantification, and definition of interaction force and level of involvement, [96, 118, 120,121,122], and other non-conventional methods such as the implementation of virtual sensors for force estimation and movement or through virtual reality game scenarios or even the influence on the emotional state of the user in virtual therapies [94, 98, 99].
A novel and interesting tool to measure pain is the one proposed by Ref. [107]. Pain estimation is used to control the robot through a decision support system based on fuzzy logic. The muscle contraction, resistance force, and mobility angles reached are used in this strategy. This idea can be used to explore other variables associated with pain, such as temperature or even heart rate.
Finally, some devices that include quantification techniques in the rehabilitation processes are PUParm [112], ReROBOT [119], Universal Haptic Pantograph (UHP) [34, 98], BRANDO [94], UR10 (Universal Robots A/S, Den- mark) [120], Armeo power (Hocoma) [46], powered variable-stiffness exoskeleton device (PVSED) [116] and SIMeRiON [113]. Robotic exoskeletons, such as Armeo Power [121], can provide repetitive and repeatable goal-directed rehabilitation movements more efficiently than manual therapy.
(3) Assistive robotics including virtual reality: Virtual reality applied to rehabilitation seeks training and improvement of the patient’s motor capacity, as well as monitoring the evolution throughout the therapy [21]. The use of virtual reality in rehabilitation supports therapies with long and repetitive sessions, making them fun and motivating without losing rigor and adherence to the therapy process [123,124,125]. Thus, virtual reality increases the degree of commitment of the patient to carrying out rehabilitation exercises. In the same way, it facilitates access to therapies for patients. Virtual reality can be used to distract patients from unpleasant sensations such as pain, although it is necessary to evaluate to what extent a system is considered immersive and whether it is sufficient to manage pain in rehabilitation routines. In this section, we include physical assistive robotics that use virtual reality for the rehabilitation process. These technologies provide activities through serious games with spaces, colors, and scores to create adherence of patients to the rehabilitation processes. These works correspond to 20.75% of the literature reviewed. Some devices that use virtual reality for rehabilitation are HX [52], PUParm [112], Amadeo (Tyromotion GmbH) [95], Universal Haptic Pantograph (UHP) [34, 98], HapticMaster (MOOG Inc. FCS) [58], BRANDO [94], Physiobot [99], end-effector upper limb rehabilitation robot (EULRR) [60], Armeo power (by Hocoma) [46] and other devices as Refs. [67, 77, 97, 118, 122]. Virtual reality can be used to instigate adverse situations to which the patient is exposed through virtual therapy, which can be psychologically adaptive and trigger a physiological effect that the body can reduce, mitigate or even eliminate pain sensations. In summary, virtual reality can be an important tool to improve the effectiveness and adherence to rehabilitation therapy, but further research is needed to investigate its use in this field of robotic rehabilitation.
5 Discussion
We have presented a review of assistive robotics associated with upper limb rehabilitation to understand the literature and the latest advances in this field of engineering applied to health care and rehabilitation. Studies present upper limb exoskeletons and end-effector type devices from 1-DoF to 27-DoF. The decision of designing and building systems with n degrees of freedom depends on the type of injury or pathology to be treated. In Refs. [45, 55, 68, 76, 77, 100, 104, 106], the authors approach the design of exoskeleton-like systems coupled to the physiology of the body and try to mimic as many movements as possible. However, this increases the complexity of the mathematical models, but at the same time allows the systems to adapt more appropriately to biomechanical movements. The evidence suggests that the design of devices and application techniques for upper limb rehabilitation depends on the affected joint and the diagnosed disease. Some studies focus on the rehabilitation of a single joint [52, 66, 69, 71, 72, 75, 95, 97, 115, 116, 119, 120, 126], while others are focused on the rehabilitation of the whole motor function of the upper limb’s main joints, i.e., shoulder, elbow and wrist [34, 53, 55, 61, 62, 67, 68, 76, 77, 88, 90, 98, 100, 104, 106, 112, 121, 127]. The latter usually focus on monitoring the process by estimating and obtaining evaluation parameters such as joint positions, velocities, forces and torques, and muscle stimulation or activation with EMG signals.
We consider that studies focusing on all joints of the upper limb will be an approach to systems that can contribute to the generalization and personalization of conditions and their ease of treatment. However, quantification of rehabilitation processes has proven to be a challenge for rehabilitation robotics. This process depends on the interdisciplinarity between applied sciences and health sciences, implementation costs, and the accuracy of measurements and monitoring [128,129,130,131,132,133,134]. Quantification methods provide the specialist with a tool for continuous monitoring and improvement of the rehabilitation process. Some strategies can be derived from the instrumentation of the device, and may also include more variables in addition to those usually considered (position, velocity, force and torque). For example, variables associated with the evaluation and monitoring of rehabilitation processes, such as muscle atrophy index, pain level based on sEMG, heart rate or even anthropometric measurements (height, weight, body mass index, etc.) can be considered.
There are great advances in assistive robotics for rehabilitation and quantification technologies [34, 55, 67, 68, 76, 98, 100, 104, 106, 121]. However, more reliable methods are still required to quantify the endpoints and to assess the patient’s progress in the rehabilitation process. This implies real-time monitoring so that the system can adapt to the patient’s conditions, leading to the definition and implementation of control strategies.
Regarding control strategies, in Refs. [34, 35, 43,44,45, 53, 64, 65, 71, 74, 89, 97, 99, 100, 103], the authors implemented impedance controls. The nature of these types of controls allows the adaptation of the system to the patient’s needs and the level of assistance required in the rehabilitation process. For example, in Refs. [104, 105, 129], the authors worked extensively with the ETS-MARSE robot to provide a passive rehabilitation trajectory that mimics human movement. They also present a robust control with external force adaptation based on backward control in order to estimate the user’s force. Then, the integration of an optimization approach to select the control parameters and the combination of model-based switching functions with existing vibration reduction techniques can be proposed as future work, to reduce unwanted external forces during therapy. This has some affinity with AAN strategies for smooth trajectories with the possibility of resorting to assistive forces that will be available when the patient’s movement is delayed from the desired trajectory; an example of this is the commercial Armeo Power system from Hocoma [46]. From this mode, different strategies have been adopted, so this method promises to be the most suitable option for systems focused on physical assistance based on the level of intensity or intervention. However, the diversity of proposals that arise from this control strategy, gives rise to propose new strategies such as hybrid impedance controls with the option of adaptability through automatic learning systems, such as neural networks based on the evaluation of measurements obtained to adjust the difficulty and intensity of training based on medical expertise to meet the patients’ needs.
Research is needed on the optimization of impedance parameters, integrating them with the clinical experience of physiotherapists, to improve the effectiveness of rehabilitation. On the other hand, interesting techniques have been proposed in the integration of several control methods implementing hybrid model integration analysis where perception models are complementarily used, together with models based on neural networks, these methods seek the optimization of trajectories and automatic learning of the rehabilitation schemes defined as the one proposed by Refs. [108, 109]. However, it is necessary to establish a margin of comparison of control methods to determine which one gives better results.
In summary, control strategies for rehabilitation systems should modulate human-robot interaction, and should encourage the active participation of the patient during training. This implies considering also a synergy with other assessment parameters, such as pain, that directly or indirectly reflect the adaptability that the control can provide at all times.
Regarding the mechanical design, in Ref. [45], the ANYexo robotic system compensates for the dynamics by precisely aligning the robot with the patient. The lightweight structure, the precise dynamic model, the optimized handling and the high performance of the torque control actuators are achieved by the lightweight and versatile design of the links. This device prompts research for a future generation of more autonomous and highly dynamic rehabilitation robots. On the other hand, the design of wearable exoskeletons that seek to ensure perfect connections between the exoskeleton and human limbs have been proposed. In Ref. [65], the exoskeleton links lengths are designed to be adjustable in order to partially align the human and exoskeleton joints in an attempt to prevent uncontrolled forces caused by hyperstaticity. Finally, decreasing unwanted interaction loads caused by exoskeleton incompatibility continues to be a huge challenge in ergonomic exoskeleton design, as we evidenced in Ref. [130]. To achieve hegemony in rehabilitation robots, a generalization towards all upper limb joints and their respective movements, it is necessary to design robotic systems capable of covering the anatomical ranges of mobility of the affected limb. The exercises that are usually performed for shoulder rehabilitation are internal/external rotation, adduction/abduction, flexion-extension, for elbow rehabilitation are flexion/extension and for the wrist rehabilitation are ulnar/radial deviation, flexion/extension, and pronation/supination. Commercial devices such as the UR5 and UR10 (Universal Robots A/S) and Armeo power (by Hocoma) [46, 61, 62, 121], include motions of these joints. A major limitation to the standardization and the development of exercise-specific metrics for the interpretation of kinematic data, especially in complex exercises, is the absence of strict instructions for making decisions on how to set up the system for each patient. The effectiveness of the training may depend on the experience of the therapist. Furthermore, it is preferred to establish training trajectories only from the selected plane as in Ref. [61], whereas common rehabilitation routines may prefer training trajectories in three-dimensional space. It is also important to apply real-time adaptive trajectories to immediately modify the training routine when there is a potential risk to the patient in mobility, force and pain.
On the other hand, virtual reality in assistive devices is another feature that requires further study. Although some assistive devices described in the literature include virtual reality, it is often used in a non-immersive state through games or tasks that the patient has to perform with a low degree of immersion. This aspect is important to distract patients from unpleasant sensations such as pain, but it is necessary to assess to what extent a system is considered immersive and whether it is sufficient to manage pain in rehabilitation routines. Virtual reality provides distraction and adherence to the therapy, and in the literature has been implemented frequently. However, the systems analyzed in the literature have generally been limited to visual and auditory feedback using monitors or directly VR glasses.
Some methods that can be used in combination with virtual reality to achieve greater active participation of patients in their treatment are, for example, gamification, augmented reality (AR), music-based therapy, among others. However, it is important to remark that not all of these methods are suitable for all patients or all treatments. Therefore, health professionals are the ones who must evaluate the needs and preferences of each patient before using any complementary technological method of therapy.
One of the best-known systems that implements virtual reality is the Armeo power [46], however, it does not use immersive technologies. Other works where virtual reality has been applied are Refs. [34, 52, 58, 67, 77, 94, 95, 97, 99, 112, 121]. These virtual reality systems are usually limited to tasks or games through haptic activity, and sometimes they require expensive elements to reach immersive environments. Nevertheless, new studies incorporate portable devices such as cell phones or computers. The challenge is to maintain adherence despite the loss of immersivity. Regarding immersive systems, future research could strengthen and characterize the extent to which an immersive system is able to block unpleasant sensations such as pain. And how the adverse situations to which the patient is subjected through virtual reality can be instigated and even psychologically adaptive and subsequently trigger a physiological effect that the body is able to reduce, mitigate or even eliminate the sensations of pain. An important aspect rescued from Ref. [94] regarding experimentation with virtual reality as the perception of the sensation produced by the virtual representation towards the injured limbs. This would lead to the incorporation of new proprioceptive biofeedback exercises. Therefore, it is necessary to incorporate other technologies such as sensors for the accurate assessment of other kinesthetic aspects such as compensatory movements. In addition, the inclusion of games may involve cognitive skills, but not necessarily kinesthetic performance. Correlation is also needed to optimize the performance of routines or tasks with physical and cognitive requirements.
After this review, questions related to the evaluation variables associated with upper limb rehabilitation arise. Although most of the available devices fulfill extensive functions to rehabilitate and provide evaluation parameters, it is necessary to parameterize and consider other variables related to physical evaluation. Moreover, research on immersive virtual reality and its inclusion in rehabilitation processes to motivate the patient requires some effort. Some questions that give rise to future research are: What additional variables can be considered for rehabilitation monitoring? What control strategies are the most suitable for applying them in rehabilitation systems? What are the requirements for those control strategies? What is the effect of improving mechanical systems with more degrees of freedom to obtain a generalization for the treatment of more physical diseases? What advantages would immersive virtual reality have in the rehabilitation processes compared to conventional virtual reality systems?
It is important to define a global model or an architecture that allows complete and comprehensive monitoring of the rehabilitation processes. This feature provides support also for the diagnosis. The results generated from comprehensive monitoring and quantification could allow a breakthrough in this particular field of knowledge and provide a starting point for diagnostic and physical rehabilitation processes, as well as a more accurate picture related to clinical rehabilitation procedures and support diagnosis of upper limb pathologies.
In addition, we have compiled some of the most recent reviews on assistive robotics as Refs. [24, 135,136,137,138,139,140,141,142,143]. We have addressed future directions and perspectives to direct future research in this field of robotics applied to physical rehabilitation. A comparative graph is presented in Figure 6, where the left side summarizes trends and contributions identified in the analysis of the articles reviewed (blue), and the right side shows the trends and directions that we propose (green) to direct future research that can give a clearer vision of the implementation of assistive robotics to achieve the definitive acceptance of these technologies in clinical processes.

Latest trends and directions identified in upper limb assistive robotics
6 Conclusions
This review allows understanding the state of the art related to physical assistance technologies through human-machine interaction. We have analyzed current technologies for physical rehabilitation. This study is focused on practical aspects related to robotic systems for physical rehabilitation. We classified the reviewed articles into main topics, i.e., control strategies, quantification and integral monitoring of rehabilitation processes, integration of complementary methods to conventional rehabilitation, and possible integration of virtual reality systems.
The analysis of the bibliography presented in this review includes several upper limb physical rehabilitation systems. Through this analysis, we have given an insight of the current systems. This review provides a tool to identify where and how to improve some associated features of upper limb rehabilitation systems regarding several aspects. Some of these features are mechanical optimization and performance, the degrees of freedom (DoF), lightness, the durability of materials, ergonomics, and portability. Another key feature is the inclusion of quantification variables for more comprehensive and complete monitoring of rehabilitation processes. It is possible to acquire variables that define various conditions in the patient, such as the level of muscle atrophy, the presence of pain, heart rate, temperature, and mood. There is also the definition of appropriate control strategies according to therapy needs and the possibility to propose control strategies based on the most common ones, such as adaptive controls, impedance controls, admittance controls, and combinations. Finally, it is also possible to include immersive virtual reality technologies as part of the therapy, such as visual, auditory, and tactile or force systems.
This review aims to provide an overview of the state of the art in this field of knowledge. We analyze the current technology to move forward in the theoretical strengthening of assistive robotics. Future work should be oriented to resolve issues related to quantifying subjective variables as pain, for example, monitoring of rehabilitation processes through assistive systems, and in a complementary manner, evaluate the incorporation of technologies such as virtual reality and its correlation in the improvement of rehabilitation processes. The consequence of using this type of technology would be reflected in reducing the therapy and recovery times in the short, medium, and long term. The interdisciplinary between professionals of health sciences and engineering will allow progress in this field of study.
Data availability
The data used in this article are results of previously published studies and are available in the databases [IEEE, scopus, sciencedirect and web of science] from which they were extracted. The specific data extracted from these studies and used for the analysis are available in the original publications. No new data were generated during the course of this review. All data supporting the findings of this study are available within the paper.
References
T Jabeen, S Kazmi, A Rehman, et al. Upper and lower limbs disability and personality traits. Journal of Ayub Medical College, Abbottabad: JAMC, 2016, 26(2): 348-352.
WHO. World report on disability, tech. rep., World Health Organization, 2011.
F D Dick, R A Graveling, W Munro, et al. Workplace management of upper limb disorders: A systematic review. Occupational Medicine, 2010, 61(1): 19-25.
K Fagher, J Lexell. Sports-related injuries in athletes with disabilities. Scandinavian Journal of Medicine & Science in Sports, 2014, 24(5): e320-e331.
V Occhionero, L Korpinen, F Gobba. Upper limb musculoskeletal disorders in healthcare personnel. Ergonomics, 2014, 57(8): 1166-1191.
J T da Costa, J S Baptista, M Vaz. Incidence and prevalence of upper-limb work related musculoskeletal disorders: A systematic review. Work, 2015, 51(4): 635-644.
S K Hillman. Core concepts in athletic training and therapy with web resource. Annals of Internal Medicine, 2012.
H H Kessler. The principles and practices of rehabilitation. Physical Therapy, 1950, 30(3): 126-127.
ACP. Physiotherapy: Its principles and practice. Annals of Internal Medicine, 1932, 6(2): 298.
G McHugh, I D Swain, D Jenkinson. Treatment components for upper limb rehabilitation after stroke: A survey of UK national practice. Disability and Rehabilitation, 2013, 36(11): 925-931.
K A Wattchow, M N McDonnell, S L Hillier. Rehabilitation interventions for upper limb function in the first four weeks following stroke: A systematic review and meta-analysis of the evidence. Archives of Physical Medicine and Rehabilitation, 2018, 99(2): 367-382.
A M Bruder, N Shields, K J Dodd, et al. Prescribed exercise programs may not be effective in reducing impairments and improving activity during upper limb fracture rehabilitation: A systematic review. Journal of Physiotherapy, 2017, 63(4): 205-220.
C Milicin, E Sirbu. A comparative study of rehabilitation therapy in traumatic upper limb peripheral nerve injuries. NeuroRehabilitation, 2018, 42(1): 113-119.
R Prosser, W B Conolly. Rehabilitation of the hand upper limb. Oxford: Butterworth-Heinemann, 2003.
D H Gates, L S Walters, J Cowley, et al. Range of motion requirements for upper-limb activities of daily living. American Journal of Occupational Therapy, 2015, 70(1): 7001350010p1-7001350010p10.
D Bankson. Clinical tests for the musculoskeletal system: Examination-signs-phenomena. Physical Therapy, 2006, 86(7): 1042.
N Linda, M Maia, L Hennen, et al. Assistive technologies for people with disabilities - part II: Current and emerging technologies. European Parliament, 2018.
O A Olanrewaju, A A Faieza, K Syakirah. Application of robotics in medical fields: Rehabilitation and surgery. International Journal of Computer Applications in Technology, 2015, 52(4): 251-256.
R Ballantyne, P M Rea. A game changer: ‘the use of digital technologies in the management of upper limb rehabilitation’. Advances in Experimental Medicine and Biology, 2019, 1205: 117-147.
F Molteni, G Gasperini, G Cannaviello, et al. Exoskeleton and end-effector robots for upper and lower limbs rehabilitation: Narrative review. PM R, 2018, 10(9): S174-S188.
M Munih, T Bajd. Rehabilitation robotics. Technology and Health Care, 2011, 19(6): 483-495.
A Zemmar, A M Lozano, B J Nelson. The rise of robots in surgical environments during COVID-19. Nature Machine Intelligence, 2020, 2: 566-572.
J Guiochet, M Machin, H Waeselynck. Safety-critical advanced robots: A survey. Robotics and Autonomous Systems, 2017, 94: 43-52.
E D Oña, J M Garcia-Haro, A Jardón, et al. Robotics in health care: Perspectives of robot-aided interventions in clinical practice for rehabilitation of upper limbs. Applied Sciences, 2019, 9(13): 2586.
A A Scoglio, E D Reilly, J A Gorman, et al. Use of social robots in mental health and well-being research: Systematic review. Journal of Medical Internet Research, 2019, 21(7): e13322.
J Holland, L Kingston, C McCarthy, et al. Service robots in the healthcare sector. Robotics, 2021, 10(1): 47.
I Hafidz, D Adiputra, B Montolalu, et al. IoT-based logistic robot for real-time monitoring and control patients during COVID-19 pandemic. Jurnal Nasional Teknik Elektro, 2020, 9(3): 182.
A Karam, F Alnajjar, M Gochoo. Assistive and rehabilitation robotics for upper limb impairments in post-stroke patients: Evaluation criteria for the design and functionality. 2020 Advances in Science and Engineering Technology International Conferences (ASET), 2020: 1-4.
A Frisoli. Chapter 6 - exoskeletons for upper limb rehabilitation. Rehabilitation Robotics, 2018: 75-87.
R Colombo. Chapter 8 - performance measures in robot assisted assessment of sensorimotor functions. Rehabilitation Robotics, 2018: 101-115.
S Macovei, I Doroftei. A short overview of upper limb rehabilitation devices. IOP Conference Series: Materials Science and Engineering, 2016, 145: 052014.
H I Krebs, B T Volpe. Rehabilitation robotics. Handbook of Clinical Neurology, 2013, 110: 283-294.
I Carrera, H M Avalos, R Saltaren, et al. Road: Domestic assistant and rehabilitation robot. Medical Biological Engineering Computing, 2011, 49(7): 1201-1211.
A Mancisidor, A Zubizarreta, I Cabanes, et al. Inclusive and seamless control framework for safe robot-mediated therapy for upper limbs rehabilitation. Mechatronics, 2019, 58: 70-79.
E Akdogan. Upper limb rehabilitation robot for physical therapy: Design, control, and testing. Turkish Journal of Electrical Engineering Computer Sciences, 2016, 24(1): 911-934.
R Trochimczuk, T Huscio, S Grymek, et al. Rehabilitation device supporting active and passive upper limb exercises. Current Science, 2018, 115(9): 868-873.
M E Stoykov, J W Stinear. Active-passive bilateral therapy as a priming mechanism for individuals in the subacute phase of post-stroke recovery: A feasibility study. American Journal of Physical Medicine & Rehabilitation, 2010, 89: 873-878.
G Kwakkel, B J Kollen, H I Krebs. Effects of robot-assisted therapy on upper limb recovery after stroke: A systematic review. Neurorehabilitation and Neural Repair, 2007, 22(2): 111-121.
O Boubaker. Medical robotics. Control Theory in Biomedical Engineering, 2020: 153-204.
L M S do Nascimento, L V Bonfati, M L B Freitas, et al. Sensors and systems for physical rehabilitation and health monitoring - A review. Sensors, 2020, 20: 4063.
Y Shen, J Sun, J Ma, et al. Admittance control scheme comparison of EXO-UL8: A dual-arm exoskeleton robotic system. 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), 2019: 611-617.
K Leuenberger, R Gonzenbach, S Wachter, et al. A method to qualitatively assess arm use in stroke survivors in the home environment. Medical & Biological Engineering & Computing, 2016, 55(1): 141-150.
S H Chen, W M Lien, W W Wang, et al. Assistive control system for upper limb rehabilitation robot. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 2016, 24(11): 1199-1209.
E Akdogan, M E Aktan, A T Koru, et al. Hybrid impedance control of a robot manipulator for wrist and forearm rehabilitation: Performance analysis and clinical results, Mechatronics, 2018, 49: 77-91.
Y Zimmermann, A Forino, R Riener, et al. ANYexo: A versatile and dynamic upper-limb rehabilitation robot. IEEE Robotics and Automation Letters, 2019, 4(4): 3649-3656.
G Galeoto, A Berardi, M Mangone, et al. Assessment capacity of the Armeo® power: Cross-sectional study. Technologies, 2023, 11(5): 125.
Y W Hsieh, K C Lin, C Y Wu, et al. Comparison of proximal versus distal upper-limb robotic rehabilitation on motor performance after stroke: A cluster controlled trial. Scientific Reports, 2018, 8(1): 2091.
E D’Antonio, E Galofaro, F Patané, et al. A dual arm haptic exoskeleton for dynamical coupled manipulation. 2021 IEEE/ASME International Conference on Advanced Intelligent Mechatronics (AIM), 2021: 1237-1242.
J Cornejo, J A C Aguilar, J P P Villarroel. International innovations in medical robotics to improve the patient management in Peru. Revista de la Facultad de Medicina Humana, 2019, 19: 105-113.
2021 IEEE thesaurus, IEEE, 2021, 577.
P Edition. Prosthetics and orthotics, vocabulary-part 1: General terms for external limb prostheses and external orthoses. ISO, 1989.
G A Farulla, D Pianu, M Cempini, et al. Vision-based pose estimation for robot-mediated hand telerehabilitation. Sensors, 2016, 16(2): 208.
D Simonetti, L Zollo, L Vollero, et al. A modular telerehabilitation architecture for upper limb robotic therapy. Advances in Mechanical Engineering, 2017, 9(2): 1-13.
E Ambrosini, M Russold, M Gfoehler, et al. A Hybrid robotic system for arm training of stroke survivors: Concept and first evaluation. IEEE Transactions on Biomedical Engineering, 2019, 66(12): 3290-3300.
B Brahmi, M Saad, M H Rahman, et al. Cartesian trajectory tracking of a 7-DOF exoskeleton robot based on human inverse kinematics. IEEE Transactions on Systems, Man, and Cybernetics: Systems, 2019, 49(3): 600-611.
B D Chaparro-Rico, D Cafolla, M Ceccarelli, et al. NURSE-2 DoF device for arm motion guidance: Kinematic, dynamic, and FEM analysis. Applied Sciences, 2020, 10(6): 2139.
B D M Chaparro-Rico, D Cafolla, M Ceccarelli, et al. Experimental characterization of NURSE, a device for arm motion guidance. Journal of Healthcare Engineering, 2018, 8: 1-15.
N Norouzi-Gheidari, P S Archambault, J Fung. Robot-assisted reaching performance of chronic stroke and healthy individuals in a virtual versus a physical environment: A pilot study. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 2019, 27(6): 1273-1281.
Q Miao, M Zhang, A McDaid, et al. A robot-assisted bilateral upper limb training strategy with subject-specific workspace: A pilot study. Robotics and Autonomous Systems, 2020, 124: 103334.
L Zhang, S Guo, Q Sun. Development and assist-as-needed control of an end-effector upper limb rehabilitation robot. Applied Sciences, 2020, 10: 6684.
Q Miao, A McDaid, M Zhang, et al. A three-stage trajectory generation method for robot-assisted bilateral upper limb training with subject-specific adaptation. Robotics and Autonomous Systems, 2018, 105: 38-46.
B Sheng, S Xie, L Tang, et al. An industrial robot-based rehabilitation system for bilateral exercises. IEEE Access, 2019, 7: 151282-151294.
A S Ciullo, J M Veerbeek, E Temperli, et al. A novel soft robotic supernumerary hand for severely affected stroke patients. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 2020, 28(5): 1168-1177.
V Crocher, J Fong, T J Bosch, et al. Upper limb deweighting using underactuated end-effector-based backdrivable manipulanda. IEEE Robotics and Automation Letters, 2018, 3(3): 2116-2122.
B Ugurlu, M Nishimura, K Hyodo, et al. Proof of concept for robot-aided upper limb rehabilitation using disturbance observers. IEEE Transactions on Human-Machine Systems, 2015, 45(1): 110-118.
D Wang, Q Meng, Q Meng, et al. Design and development of a portable exoskeleton for hand rehabilitation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 2018, 26(12): 2376-2386.
Y Bouteraa, I B Abdallah, A Elmogy. Design and control of an exoskeleton robot with EMG-driven electrical stimulation for upper limb rehabilitation. Industrial Robot, 47(4): 489-501.
S Kumar, H Wohrle, M Trampler, et al. Modular design and decentralized control of the RECUPERA exoskeleton for stroke rehabilitation. Applied Sciences, 2019, 9(4): 626.
D Copaci, F Martin, L Moreno, et al. SMA based elbow exoskeleton for rehabilitation therapy and patient evaluation. IEEE Access, 2019, 7: 31473-31484.
I Gaponov, D Popov, S J Lee, et al. Auxilio: A portable cable-driven exosuit for upper extremity assistance. International Journal of Control, Automation and Systems, 2017, 15(1): 73-84.
H C Hsieh, D F Chen, L Chien, et al. Design of a parallel actuated exoskeleton for adaptive and safe robotic shoulder rehabilitation. IEEE/ASME Transactions on Mechatronics, 2017, 22(5): 2034-2045.
I Hussain, G Salvietti, G Spagnoletti, et al. A soft supernumerary robotic finger and mobile arm support for grasping compensation and hemiparetic upper limb rehabilitation. Robotics and Autonomous Systems, 2017, 93: 1-12.
Y Liu, S Guo, H Hirata, et al. Development of a powered variable-stiffness exoskeleton device for elbow rehabilitation. Biomedical Microdevices, 2018, 20(3): 64.
E Trigili, S Crea, M Moise, et al. Design and experimental characterization of a shoulder-elbow exoskeleton with compliant joints for post-stroke rehabilitation. IEEE/ASME Transactions on Mechatronics, 2019, 24: 1485-1496.
L Zhang, J Li, Y Cui, et al. Design and performance analysis of a parallel wrist rehabilitation robot (PWRR). Robotics and Autonomous Systems, 2020, 125: 103390.
S Lessard, P Pansodtee, A Robbins, et al. A soft exosuit for flexible upper-extremity rehabilitation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 2018, 26(8): 1604-1617.
K Liu, C H Xiong, L He, et al. Postural synergy-based design of exoskeleton robot replicating human arm reaching movements. Robotics and Autonomous Systems, 2018, 99: 84-96.
M R Islam, B Brahmi, T Ahmed, et al. Exoskeletons in upper limb rehabilitation: A review to find key challenges to improve functionality. Control Theory in Biomedical Engineering, 2020: 235-265.
C Gibson, F Eubanks, F Hobson. 4.2.3 A systems approach to medical device compliance with IEC 60601–1: 2005. INCOSE International Symposium, 2012, 22(1): 505-516.
A Festas, A Ramos, J Davim. Medical devices biomaterials – A review. Proceedings of the Institution of Mechanical Engineers, Part L: Journal of Materials: Design and Applications, 2019, 234: 218-228.
T Hanawa. Research and development of metals for medical devices based on clinical needs. Science and Technology of Advanced Materials, 2012, 13: 064102.
L Toth, A Schiffer, M Nyitrai, et al. Developing an anti-spastic orthosis for daily home-use of stroke patients using smart memory alloys and 3d printing technologies. Materials & Design, 2020, 195: 109029.
C Lunsford, G Grindle, B Salatin, et al. Innovations with 3-dimensional printing in physical medicine and rehabilitation: A review of the literature. PM&R, 2016, 8: 1201-1212.
T Dinon, M Caimmi, A Chiavenna, et al. DUALarm: An open-source and 3D-printable device for upper limb neurorehabilitation. Journal of Rehabilitation and Assistive Technologies Engineering, 2018, 5: 205566831774998.
J Vertongen, D Kamper. Design of a 3d printed hybrid mechanical structure for a hand exoskeleton. Current Directions in Biomedical Engineering, 2020, 6(2): 20202003.
A Biesiekierski, K Munir, Y Li, et al. Material selection for medical devices, metallic biomaterials processing and medical device manufacturing. Woodhead Publishing Series in Biomaterials, 2020: 31-94.
N Kapadia, M Myers, K Musselman, et al. 3-dimensional printing in rehabilitation: Feasibility of printing an upper extremity gross motor function assessment tool. BioMedical Engineering OnLine, 2021, 20(1).
R Merchant, D C Ortiz, M B Escamilla, et al. Integrated wearable and self-carrying active upper limb orthosis. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, 2018, 232(2): 172-184.
K Y Wu, Y Y Su, Y L Yu, et al. A 5-degrees-of-freedom lightweight elbow-wrist exoskeleton for forearm fine-motion rehabilitation. IEEE/ASME Transactions on Mechatronics, 2019, 24(6): 2684-2695.
L Zhang, J Li, P Su, et al. Improvement of human–machine compatibility of upper-limb rehabilitation exoskeleton using passive joints. Robotics and Autonomous Systems, 2019, 112: 22-31.
A Zeiaee, R S Zarrin, A Eib, et al. CLEVERarm: A lightweight and compact exoskeleton for upper-limb rehabilitation. IEEE Robotics and Automation Letters, 2021, 7(2): 1880-1887.
A Zeiaee, R S Zarrin, R Langari, et al. Design and kinematic analysis of a novel upper limb exoskeleton for rehabilitation of stroke patients. 2017 International Conference on Rehabilitation Robotics (ICORR), 2017.
F Calignano, M Lorusso, I Roppolo, et al. Investigation of the mechanical properties of a carbon fibre-reinforced nylon filament for 3D printing. Machines, 2020, 8(3): 52.
M A P Castañeda, E Sotgiu, M Barsotti, et al. An orthopaedic robotic-assisted rehabilitation method of the forearm in virtual reality physiotherapy. J. Healthc. Eng., 2018: 7438609.
X Huang, F Naghdy, G Naghdy, et al. The combined effects of adaptive control and virtual reality on robot-assisted fine hand motion rehabilitation in chronic stroke patients: A case study. Journal of Stroke and Cerebrovascular Diseases, 2018, 27(1): 221-228.
H J Asl, M Yamashita, T Narikiyo, et al. Field-based assist-as-needed control schemes for rehabilitation robots. IEEE/ASME Transactions on Mechatronics, 2020, 25: 2100-2111.
J Bai, A Song, T Wang, et al. A novel backstepping adaptive impedance control for an upper limb rehabilitation robot. Computers and Electrical Engineering, 2019, 80: 106465.
A Mancisidor, A Zubizarreta, I Cabanes, et al. Virtual sensors for advanced controllers in rehabilitation robotics. Sensors, 2018, 18(3): 1-15.
B F Villar, P F Viñas, J P Turiel, et al. Influence on the user’s emotional state of the graphic complexity level in virtual therapies based on a robot-assisted neuro-rehabilitation platform. Computer Methods and Programs in Biomedicine, 2020, 190: 105359.
Q Wu, H Wu. Development, dynamic modeling, and multi-modal control of a therapeutic exoskeleton for upper limb rehabilitation training. Sensors, 2018, 18(11): 3611.
Q Miao, Y Peng, L Liu, et al. Subject-specific compliance control of an upper-limb bilateral robotic system. Robotics and Autonomous Systems, 2020, 126: 103478.
J Lee, M Kim, K Kim. A control scheme to minimize muscle energy for power assistant robotic systems under unknown external perturbation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 2017, 25(12): 2313-2327.
Z Li, Z Huang, W He, et al. Adaptive impedance control for an upper limb robotic exoskeleton using biological signals. IEEE Transactions on Industrial Electronics, 2017, 64(2): 1664-1674.
B Brahmi, M Saad, C O Luna, et al. Adaptive tracking control of an exoskeleton robot with uncertain dynamics based on estimated time-delay control. IEEE/ASME Transactions on Mechatronics, 2018, 23(2): 575-585.
B Brahmi, M Driscoll, I K E Bojairami, et al. Novel adaptive impedance control for exoskeleton robot for rehabilitation using a nonlinear time-delay disturbance observer. ISA Transactions, 2021, 108: 381-392.
Q Wu, X Wang, B Chen, et al. Development of an RBFN-based neural-fuzzy adaptive control strategy for an upper limb rehabilitation exoskeleton. Mechatronics, 2018, 53: 85-94.
Y Bouteraa, I B Abdallah, K Alnowaiser, et al. Smart solution for pain detection in remote rehabilitation. Alexandria Engineering Journal, 2021, 60: 3485-3500.
W Wang, J Zhang, X Wang, et al. Motion intensity modeling and trajectory control of upper limb rehabilitation exoskeleton robot based on multi-modal information. Complex and Intelligent Systems, 2022, 8: 2091-2103.
W Wang, J Zhang, D Kong, et al. Research on control method of upper limb exoskeleton based on mixed perception model. Robotica, 2022, 40: 3669-3685.
N Ciesla, V Dinglas, E Fan, et al. Manual muscle testing: A method of measuring extremity muscle strength applied to critically ill patients. Journal of Visualized Experiments, 2011, (50): 2632.
D A Delgado, B S Lambert, N Boutris, et al. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. JAAOS: Global Research and Reviews, 2018, 2: e088.
A B Motos, L D Lledó, J A Díez, et al. Estimation of human arm joints using two wireless sensors in robotic rehabilitation tasks. Sensors, 2015, 15(12): 30571-30583.
C Amici, F Ragni, M Ghidoni, et al. Multi-sensor validation approach of an end-effector-based robot for the rehabilitation of the upper and lower limb. Electronics, 2020, 9: 1751.
B Gao, C Wei, H Ma, et al. Real-time evaluation of the signal processing of sEMG used in limb exoskeleton rehabilitation system. Applied Bionics and Biomechanics, 2018: 1-6.
M Tiboni, A Borboni, R Faglia, et al. Robotics rehabilitation of the elbow based on surface electromyography signals. Advances in Mechanical Engineering, 2018, 10(2): 1-14.
Z Yang, S Guo, Y Liu, et al. An intention-based online bilateral training system for upper limb motor rehabilitation. Microsystem Technologies, 2020, 27: 211-222.
W D Wang, H H Li, M H Xiao, et al. Design and verification of a human–robot interaction system for upper limb exoskeleton rehabilitation. Medical Engineering & Physics, 2020, 79: 19-25.
Q Wu, Y Chen. Development of an intention-based adaptive neural cooperative control strategy for upper-limb robotic rehabilitation. IEEE Robotics and Automation Letters, 2021, 6: 335-342.
S Huang, S Cai, G Li, et al. SEMG-Based detection of compensation caused by fatigue during rehabilitation therapy: A pilot study. IEEE Access, 2019, 7: 127055-127065.
B Sheng, L Tang, O M Moosman, et al. Development of a biological signal-based evaluator for robot-assisted upper-limb rehabilitation: A pilot study. Australasian Physical and Engineering Sciences in Medicine, 2019, 42(3): 789-801.
W Wu, J Fong, V Crocher, et al. Modulation of shoulder muscle and joint function using a powered upper-limb exoskeleton. Journal of Biomechanics, 2018, 72: 7-16.
C N Smith, V Mehrabi, S F Atashzar, et al. A multi-functional lower- and upper-limb stroke rehabilitation robot. IEEE Transactions on Medical Robotics and Bionics, 2020, 2: 549-552.
M Smits, J B Staal, H van Goor. Could virtual reality play a role in the rehabilitation after COVID-19 infection? BMJ Open Sport & Exercise Medicine, 2020, 6(1): e000943.
K Threapleton, A Drummond, P Standen. Virtual rehabilitation: What are the practical barriers for home-based research? Digital Health, 2016, 2: 205520761664130.
A Asadzadeh, T S Soltani, Z Salahzadeh, et al. Effectiveness of virtual reality-based exercise therapy in rehabilitation: A scoping review. Informatics in Medicine Unlocked, 2021, 24: 100562.
M R Islam, M Assad-Uz-Zaman, A A Z Swapnil, et al. An ergonomic shoulder for robot-aided rehabilitation with hybrid control. Microsystem Technologies, 2020, 2: 159-172.
J Liu, Y Ren, D Xu, et al. EMG-based real-time linear-nonlinear cascade regression decoding of shoulder, elbow, and wrist movements in able-bodied persons and stroke survivors. IEEE Transactions on Biomedical Engineering, 2020, 67(5): 1272-1281.
Y Vandermeeren, M Y Doost, B Herman, et al. Bimanual motor skill learning and robotic assistance for chronic hemiparetic stroke: A randomized controlled trial. Neural Regeneration Research, 2021, 16(8): 1566.
C Fallaha, M Saad, J Ghommam, et al. Sliding mode control with model-based switching functions applied on a 7-DOF exoskeleton arm. IEEE/ASME Transactions on Mechatronics, 2020, 26(1): 539-550.
J Li, Q Cao, M Dong, et al. Compatibility evaluation of a 4-DOF ergonomic exoskeleton for upper limb rehabilitation. Mechanism and Machine Theory, 2021, 156: 104146.
J Sun, Y Shen, J Rosen. Sensor reduction, estimation, and control of an upper-limb exoskeleton. IEEE Robotics and Automation Letters, 2021, 6: 1012-1019.
F Yakub, A Z M Khudzari, Y Mori. Recent trends for practical rehabilitation robotics, current challenges and the future. International Journal of Rehabilitation Research, 2014, 37: 9-21.
R Iandolo, F Marini, M Semprini, et al. Perspectives and challenges in robotic neurorehabilitation. Applied Sciences, 2019, 9: 3183.
R S Zarrin, A Zeiaee, R Langari, et al. Challenges and opportunities in exoskeleton-based rehabilitation, 2017.
S K Manna, V N Dubey. Comparative study of actuation systems for portable upper limb exoskeletons. Medical Engineering & Physics, 2018, 60: 1-13.
M Gandolla, A Antonietti, V Longatelli, et al. The effectiveness of wearable upper limb assistive devices in degenerative neuromuscular diseases: A systematic review and meta-analysis. Frontiers in Bioengineering and Biotechnology, 2020, 7: 450.
S K Subramanian, M K Cross, C S Hirschhauser. Virtual reality interventions to enhance upper limb motor improvement after a stroke: Commonly used types of platform and outcomes. Disability and Rehabilitation: Assistive Technology, 2022, 17(1): 107-115.
M R Islam, B Brahmi, T Ahmed, et al. Exoskeletons in upper limb rehabilitation: A review to find key challenges to improve functionality. Control Theory in Biomedical Engineering, 2020, 235-265.
R M Hakim, B G Tunis, M D Ross. Rehabilitation robotics for the upper extremity: Review with new directions for orthopaedic disorders. Disability and Rehabilitation: Assistive Technology, 2016, 12: 765-771.
J Cornejo, D Huamanchahua, S H Vizconde, et al. Mechatronic exoskeleton systems for supporting the biomechanics of shoulder-elbow-wrist: An innovative review. 2021 IEEE International IOT, Electronics and Mechatronics Conference (IEMTRONICS), 2021: 1-9.
F Molteni, G Gasperini, G Cannaviello, et al. Exoskeleton and end-effector robots for upper and lower limbs rehabilitation: Narrative review. PM&R, 2018, 10: S174-S188.
A S Niyetkaliyev, S Hussain, M H Ghayesh, et al. Review on design and control aspects of robotic shoulder rehabilitation orthoses. IEEE Transactions on Human-Machine Systems, 2017, 47: 1134-1145.
M A Gull, S Bai, T Bak. A review on design of upper limb exoskeletons. Robotics, 2020, 9: 16.
Funding
Supported by Militar Nueva Granada University of Colombia (Grant No. IMP-ING-3127).
Author information
Authors and Affiliations
Contributions
AG designed the study, gathered and analyzed data from databases, and wrote the manuscript; LS performed data analytics and findings; AV performed the interpretation of data and have substantively revised; LP performed substantively adjustments to content and form; All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing financial interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Guatibonza, A., Solaque, L., Velasco, A. et al. Assistive Robotics for Upper Limb Physical Rehabilitation: A Systematic Review and Future Prospects. Chin. J. Mech. Eng. 37, 69 (2024). https://doi.org/10.1186/s10033-024-01056-y
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10033-024-01056-y