
Abstract
The rehabilitation approach has changed with the appearance of robots. As a results the rehabilitation costs significantly decrease but also time for both the patient [1], who does not have to commute for long time to the office and medical professionals. Nowadays medicine, computer science, electronics, and engineering, in general, are strongly connected. A group of specialists is working on newer and newer solutions to improve both diagnosis and therapy. This article provides an overview of basic rehabilitation robotic solutions used in the rehabilitation of upper limb functions.
The literature used is based on PubMed and Scopus databases included articles published between 1999 and 2021. Eligibility criteria included upper limb exoskeletons for rehabilitation of both the wrist, elbow, and shoulder joints.
This paper provides an overview of an important research subject and highlights the current knowledge in the field. Despite extensive attempts to develop rehabilitation systems, exoskeletons are primarily uncommercialised despite a large number of prototypes.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others

Keywords
- Upper limb exoskeleton
- Robots rehabilitation
- Limb functions upper
- Drive units
- Kinematic chain of exoskeleton
- Review of robots
1 Introduction
We live in an aging society, with an increasing number of diseases, in particular CNS diseases, and with other diseases leading to impaired efficiency, such as atherosclerosis, diabetes, osteoarthritis, etc. Taking into account the CNS, at least 450 million people worldwide suffer from neurodegenerative diseases (around 50 million people suffer from neurodegenerative diseases). Other brain diseases include i.e. stroke (15 million), traumatic brain injury (TBI), and brain tumors, which affect about 1.5 million people. In total, it is about 0.5 billion people affected by brain diseases. According to WHO, the third on the list of civilization diseases leading to disability is stroke. An indispensable element in the process of treating strokes is rehabilitation, the effectiveness of which is very strongly dependent on the time of its implementation after the occurrence of a stroke. Treatment of these diseases and conditions, which largely contribute to motor impairment, is lengthy (situation-dependent), costly and involves many people, including healthcare professionals and family members.
Currently, drug treatment in the form of injections, suppositories, tablets and ointments is the most common. This treatment often leads only to a reduction of pain and only partial recovery. Moreover, the effects of such treatment are not permanent. It is impossible to imagine modern medical treatment without rehabilitation and physiotherapy, whose aim is to restore full and permanent functional capacity. It must be admitted that sometimes it is necessary to carry out surgical - orthopedic treatment, which, however, in order to achieve full success requires the effect of postoperative rehabilitation.
Performing therapeutic exercises requires great commitment from the physiotherapist and is very time consuming. To achieve the expected effect the exercises have to be repeated many times individually (patient - therapist). Group exercises are more beneficial in organisational and economic terms, but unfortunately they are not equivalent and do not lead to the expected effects of therapy. The constant repetition of the therapeutic movement sequences leads to the therapist's weariness, which may result in less accurate execution of the exercise or shortening the duration of the exercises. The solution to the problem may be the use of robots to relieve the physiotherapist from monotonous and exhausting physical work, at the same time allowing for the implementation of trainings with many patients by one physiotherapist. In addition, a rehabilitator using a robot obtains a diagnostic tool, because the robot's sensors can, for example, measure ranges of mobility in a given joint, or the strength of selected muscles.
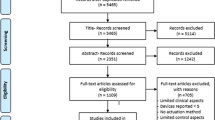
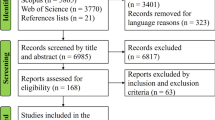
In this review the literature used is based on PubMed and Scopus databases including articles published between 1999 and 2021. A search was used based on the following keywords: “upper limb”, “robot” “rehabilitation”. The total number of results was 1700, including 156 reviews. The review was narrowed down to full text of publications available without charge and review papers and systematic reviews, which numbered 94. Next, the database was searched using the keywords “(exoskeleton) AND (upper limb)”, and the area was also narrowed down to full text of publications, the number of which was 20. From among the available articles, only those focused on the presentation of exoskeletons that can be rehabilitated in all 3 joints (wrist and hand joints, elbow joint, shoulder and clavicle joint) were selected.
As it turns out, the information found in the searched database would not allow the presentation that would be 100% satisfactory to the readers, because key technical information is often not described in publications. Taking into account, for example, one of the main parameters that distinguishes selected robots, i.e. degrees of freedom, it was necessary to additionally search manufacturers’ websites or additional materials found on the Internet, which made it difficult to create the review.
1.1 The Importance of Anthropometric Values for the Upper Limb
The upper limb plays a very important role in human daily life. It enables people to perform grabbing and cognitive activities. Due to the number and variety of tasks performed, the upper limb is particularly vulnerable to injury. This is the reason of study for physicians and physiotherapists as well as biomechanists [2,3,4].
One of the main research conducted on the upper limb are anthropometric tests, whose purpose is to provide an objective and accurate data, which are used to create rehabilitation equipment. The mentioned measurements: total limb length - measured from the acromion process to the styloid process of the elbow bone or the end of the middle finger; arm length - measured from the acromion process to the lateral epicondyle of the humerus; forearm length - measured from the ulnar process to the epicondyle process of the ulnar bone; and circumferences of the upper limb segments. As we know, the upper limb is characterised by a large range of motion, which results directly from its anatomical structure. In the shoulder joint, three movements take place on three planes: the sagittal plane is flexion - straightening (in the range of 60° of expansion and 180° of flexion), the coronal plane is abduction - adduction (in the range of 90° of abduction, 180° of abduction with the shoulder blade, 20° of adduction) and the transverse plane is external rotation - internal rotation (in the range of 98° of internal rotation and 90° of external rotation). In the other joints of the upper limb, movement takes place in only two planes. In the elbow joint, the movement is in the sagittal plane, in which flexion-straightening (150° flexion and 0° extension), and in the transverse plane, which is a rotation of the forearm (80° supination and 90° pronation). At the wrist, the movement takes place in the sagittal plane, flexion-extension (palmar flexion 70° and dorsiflexion 80°), and in the frontal plane, inversion-adduction movement (radial flexion 20° and ulnar flexion 40°).
2 Robots
The world is changing, therefore there is a need for new inventions, robots, and new solutions to support treatment. An aging population presents a new challenge. A challenge when it comes to treatment.
Scientists have found that particular activities of the brain can be transferred to a different location in the brain, and this is known as neuroplasticity. Repetitive motions for the impaired limbs allow the brain to develop new neural pathways and, ultimately, restore full or partial control of motor functions. Using a rehabilitation robot could trigger neuroplasticity by providing a repetitive exercise for the impaired functions.
The authors decided to present selected robots and briefly describe the construction and operation.
2.1 ARMin
In 2007 the first multi-armed upper limb rehabilitation device ARMin was developed [5, 6]. It was developed at the University of Zurich in cooperation with the Hocoma company and therapeutic doctors from Zurich's Balgrist clinic. Originally, it featured six degrees of freedom, four of which were propelled and the other two were passive. In that way, a kinematic scheme from the shoulder joint to the forearm was realised. The next version added two more degrees of freedom to allow movement of the forearm and wrist. The device is driven by Maxon RE series motors, which are DC motors with graphite brushes. The motors are paired with harmonic gears. An interesting feature of this device is the solution providing internal and external rotation of the shoulder. It is achieved by a special rotating module, made of two semi-cylinders. The inner element is guided by ball bearings mounted in the outer element. The drive is realised by steel cables mounted to the ends of the inner half-cylinder, which roll over the motor drive shaft. It should also be mentioned that the device can adapt to different lengths and sizes of the upper limb. Although the device in this form allows performing almost all basic and complex exercises, it does not allow to perform Proprioceptive Neuromuscular Facilitation (PNF) exercises due to the limited range of its performance.
2.2 ArmeoPower
Based on ARMin, the ArmeoPower (https://www.hocoma.com) device was developed in 2011, which is one of the first commercialised robots designed for upper limb rehabilitation. The device is intended for patients who have completely lost or have significant reduction of functionality of the upper limb due to neurological problems or injuries of the nervous system. The device has six degrees of freedom, where each degree of freedom is equipped with an independent motor and two force sensors. The device can be adapted to the patient thanks to the adjustment of the column height and length of the arm and forearm parts of the exoskeleton. The device is capable of performing the movements as shown in Table 1.
The robot continues to be refined and successfully used in clinical trials. A recent paper by Meyer et al. [7] presents to assess feasibility, safety, and potential efficacy of a new intensive focused arm-hand BOOST program and to investigate whether there is a difference between early vs. late delivery of the program in the sub-acute phase post stroke.
2.3 Armeo®Spring
Armeo®Spring is another device for upper-limb neurorehabilitation from the Armeo® family. Armeo is a commercial replica of the T-WREX device that was developed in the USA in 2004 [10]. The rehabilitation is based on working with an orthosis (exoskeleton) whose system of springs supports the rehabilitated limb and supports training. The orthosis is designed for patients with limited or lost arm function. Dysfunctions caused by injuries to the central or peripheral nervous system are treated by training that includes exercises to increase muscle strength, range of motion of the limb, and motor skills. This device has five degrees of freedom, where three are at the shoulder joint, and one each at the elbow and wrist joints. The device is characterized by the fact that it is a passive device with no drives, but it has an advanced spring mechanism that relieves the upper limb during exercises and supports training. There is also Armeo Spring Pediatric [8] - a version designed for children who require rehabilitation of the upper limb. It is based on the Armeo Spring design but the length of the brace and strain relief are adapted to the needs of children aged 4 to 12 years old. Recently, new techniques based on robotic-assistive devices have been increasingly beneficial [9]. The latest research has shown that even a short-term, two-week training program with new technologies had a positive effect and significantly recovered Stroke Patients functional level in self-care, upper limb motor ability (dexterity and movements, kinematic data, grip strength), visual constructive abilities (memory, visuo spatial abilities, attention, and complex commands).
Armeo® devices increase the effectiveness and intensity of the therapy by including even chronically ill patients self-initiated movements and motivate them to train with high intensity during the rehabilitation process [11].
2.4 Renus
The next device is the Polish project called Renus-1. It is a mechatronic system supporting motoric rehabilitation of the upper limb in patients after strokes or orthopedic diseases. The device was realised as a project in Industrial Research Institute for Automation and Measurements PIAP in Warsaw, coordinated by Institute of Exploitation Technology from Radom in the years 2006–2010 and 2013–2014 [15]. The system consists of a mechanical part - manipulator, control system, and software. The manipulator makes it possible to create a spatial trajectory of motion of the patient's hand and upper limb. The manipulator arm consists of two rigid elements connected by joints and is articulated to the ambulance moving on a vertical sled attached to a fixed column. The articulation axes of the manipulator’s arm are vertical. From the kinematics point of view, the mechanical structure of the device is a mechanism with three degrees of freedom, which allows the hand grip to be moved up/down, left/right, to/from each other. At the end of the arm there is the mechanical interface of the manipulator equipped with a multi-axis force and torque sensor. The drive system is based on three servo drives, which are synchronous motors from Mitsubishi Electric. The motors have integrated 17-bit encoders and cooperate with planetary gears of Alpha company. The largest of them is responsible for the Z-axis drive and has a power of 100W while the other two have a power of 50W. RENUS is described in detail in 3 items [12,13,14], where you will find a detailed description of the system design or software. The RENUS system has been tested for its therapeutic purposes and performance properties under domestic conditions.
There is also a version of the device for rehabilitation of the lower limb known as Renus-2.
2.5 ALEx
A representative of an advanced rehabilitation robot that enables the implementation of training multifaceted is also a device called ALEx by Kinetek, developed in 2013 at PERCRO Lab in Italy. The robot enables operation in a configuration for one or two arms simultaneously. Each arm is equipped with four active degrees of freedom equipped with actuators and two passive ones equipped only with sensors. Four BLDC brushless motors are with integrated optical incremental encoders. In addition, the device is equipped with absolute angle encoders, which are mounted directly at the point of rotation. The unique feature of this design is the patented implementation of an arm rotation mechanism that uses a remote rotation center. The movement from the motor to the driven connection is realized using a linkage gear. The arm of the exoskeleton weighs only 4.5 kg. ALEx device is a medical device with CE class IIa certification and can operate in 3 modes (passive, assistive and assisted when needed). In passive mode the patient moves the upper limb, and the robot measures the movements. In assistive mode the robot guides the patient's upper limb. In the so-called “assisted when needed” mode, the robot guides the rehabilitated person's arm to the target position if the user does not initiate the movement in less than three seconds.
2.6 Harmony
An interesting project of an exoskeleton used for rehabilitation of upper limbs mainly after stroke is the Harmony device. The work on it began in 2011 at the University of Texas, USA. It is the first-ever rehabilitation robot capable of rehabilitating both arms simultaneously. Each arm has seven active degrees of freedom, and a total of 14. The robot is equipped with SEA (series elastic actuators) drives, based with brushless DC motors Maxon Motor (EC flat series) combined with Harmonic Drive wave gears. Additionally, the device is equipped with four multi-axis force and torque sensors. Exoskeleton segment lengths can be customized for the individual patient.
2.7 IntelliArm
The IntelliArm is an exoskeleton designed and developed in 2007 in the USA. It is designed for upper limb rehabilitation of patients with neurological disorders. The project is based on MIT-Manus device developed at Boston Institute of Technology in 1997. The device has seven active degrees of freedom: four at the shoulder joint responsible for abduction/adduction, flexion/extension, internal/external rotation, and vertical movement of the shoulder joint. The next two degrees of freedom are at the elbow joint and one degree at the wrist [16]. In addition, the device has two passive degrees of freedom, which allow for posterior/anterior as well as medial and lateral displacement of the shoulder joint. Three multi-axial force sensors are mounted on the exoskeleton at each joint. Interesting mechanisms were used while designing of the device. Adduction/abduction and bending/straightening movement of the shoulder joint is transmitted from the actuator via cables. In the case of bending/straightening of the shoulder joint, the motor shaft is connected to a drum by a set of two cables, and another set of cables transmits the movement from the drum to the bending axis. The cables are tensioned by a tensioner. The arm and forearm rotation is performed by a mechanism using circular guides and a cable mechanism. Another interesting solution in this device is the wrist drive mechanism. The axis of the motor has been tilted 90 degrees using a bevel gear mechanism. Two cables wrap in the opposite direction around the motor axis are respectively mounted to drums 1 and 2. In the case of this device, it was possible to find information not only about the ranges of motion but also information about the maximum speeds and torques occurring during performing specific motions.
2.8 Aramis
Another device for upper limb rehabilitation is the Aramis system, developed in 2007 in Italy. It consists of two symmetric exoskeletons that interact with each other [17].
Each exoskeleton has six degrees of freedom and adjustment mechanisms allowing the exoskeleton to be perfectly adjusted to the arm length, forearm length, and height of the patient. The device allows for operation in a mode where the healthy limb forces the movement of the exoskeleton, which is replicated on the second exoskeleton, which forces the movement of the limb with paresis. The robot is built using DC brush motors with planetary gears Maxon Motor and optical encoders.
2.9 BONES
BONES developed at the Biomechatronics Lab - University of California Irvine. is an upper limb rehabilitation device with four degrees of freedom pneumatically actuated [18]. BONES is based on a parallel mechanism that moves the upper arm by means of two passive sliding rods that rotate relative to a fixed structural frame. Four mechanically grounded pneumatic actuators are located behind the main structural frame to control the movement of the arm through the sliding rods, while a fifth cylinder located on the structure was used to control elbow flexion/extension. The device supports a wide range of human arm motion while achieving low inertia and the ability to generate force directly on the arm. A key achievement of this is the ability to generate internal/external rotation of the arm without any circular bearing element.
2.10 ARM-100, ARM-200
Parallel to the above mentioned robots, in the years 2007–2009 in the Institute of Medical Technology and Equipment in Zabrze, a project of a device for multi-surface rehabilitation of the upper limb ARM-100 was realized (Fig. 1). The device was created in cooperation with the Upper Silesian Rehabilitation Centre “Repty” and Silesian University of Technology. The ARM-100 robot was created to support the rehabilitation of people with paresis of the upper limbs after diseases such as stroke, central nervous system injuries or rheumatoid arthritis. Rehabilitation with the ARM-100 robot is based on the PNF method (proprioceptive neuromuscular movement training). The device has seven degrees of freedom and allows for rehabilitation of the whole limb, both in the shoulder joint and in the elbow and wrist joints. A training session using the ARM-100 robot consists of two stages. The first stage involved “teaching” the robot the rehabilitation movement. In this stage, after gripping the patient’s hand in the device, the rehabilitation therapist performs the rehabilitation movement by guiding the patient’s hand. Based on signals from force sensors measuring the pressure exerted by the patient's limb on elements of the robotic arm, the device moves appropriate elements of its structure and, at the same time, memorizes their successive positions in the computer system. In the next stage of training, the robot reproduces the memorised model movement with the required speed and number of repetitions, testing at the same time whether the acceptable forces on the patient are not exceeded.
In addition to the passive rehabilitation described above, the device has also been designed for active rehabilitation with resistance, in which the patient himself carries out the movements and the device can put up defined resistance.
Work is currently underway to design a new ARM-200 device. The device is expected to have a greater range of motion and be ready for commercialisation.

ARM-100. Own source (www.itam.lukasiewicz.gov.pl)
A comprehensive review on robot-assisted therapy for handtreatment can be found in Lum et al. [19] whether e.g. Babaiasl [20] and Kim et al. [21]. In other publications [22], the authors Heo et al. presented a broad survey on hand exoskeleton innovations for rehabilitation and assistance. Unfortunately, most of these devices have low wearability. Piazza et al. [23] have investigated novel solutions for assistive robotic tools to be used at home by chronic stroke patients. However, despite the large number of emerging solutions, only a small part is used in rehabilitation. It seems that the topic of how to speed up the deployment process and how to enable the safety usage of more and more robots would need to be addressed.
3 Summary
Publications indexed in the PubMed database on upper limb function improvement were reviewed. Table 2 summarizes the characteristics of the rehabilitation robots.
Despite a large number of publications on the rehabilitation of upper limb function, the number of papers on the usage of rehabilitation robots for this purpose is very small. Considering that rehabilitation robotics has been developing rapidly over the last 20 years and may represent a breakthrough in upper limb function rehabilitation, publications in this area still represent a small percentage. As well as the number of robots used for clinical research and rehabilitation is appallingly small.
References
Huang, V.S., Krakauer, J.W.: Robotic neurorehabilitation: a computational motor learning perspective. J. Neuroeng. Rehabil. 6, 5 (2009). https://doi.org/10.1186/1743-0003-6-5
Guzik, A., Michnik, R., Rycerski, W.: The estimation of rehabilitation Progress in patients with psychomotor diseases of upper limb based on modeling and experi-mental research. Acta Bioeng. Biomech. 8(2), 79–87 (2006)
Van Andel, C.J., Wolterbeek, N., Doorenbosch, C.A.M., Veeger, D., Harlaar, J.: Complete 3D kinematics of upper extremity functional tasks. Gait Posture 27, 120 (2008)
Tejszerska, D., Świtoński, E., Gzik, M.: Biomechanika narządu ruchu człowieka. Wydawnictwo Naukowe Instytutu Technologii Eksploatacji -PIB, Radom (2011)
Nef, T., Mihelj, M., Riener, R.: ARMin: a robot for patient-cooperative arm therapy. Med. Bio. Eng. Comput. 45, 887–900 (2007). https://doi.org/10.1007/s11517-007-0226-6
Nef, T., Colombo, G., Riener, R.: ARMin – Roboter für die Bewegungstherapie der oberen Extremitäten (ARMin – Robot for Movement Therapy of the Upper Extremities). auto. 53, 597–606 (2005). https://doi.org/10.1524/auto.2005.53.12.597
Meyer, S., Verheyden, G., Kempeneers, K., Michielsen, M.: Arm-hand boost therapy during inpatient stroke rehabilitation: a pilot randomized controlled trial. Front. Neurol. 12, 652042 (2021). https://doi.org/10.3389/fneur.2021.652042
Roberts, H., et al.: Constraint induced movement therapy camp for children with hemiplegic cerebral palsy augmented by use of an exoskeleton to play games in virtual reality. Phys. Occup. Ther. Pediatr. 41, 150–165 (2021). https://doi.org/10.1080/01942638.2020.1812790
Adomavičienė, A., Daunoravičienė, K., Kubilius, R., Varžaitytė, L., Raistenskis, J.: Influence of new technologies on post-stroke rehabilitation: a comparison of armeo spring to the kinect system. Medicina 55, 98 (2019). https://doi.org/10.3390/medicina55040098
Housman, S.J., Le, V., Rahman, T., Sanchez, R.J., Reinkensmeyer, D.J.: Arm-training with T-WREX after chronic stroke: preliminary results of a randomized controlled trial. In: 2007 IEEE 10th International Conference on Rehabilitation Robotics. pp. 562–568. IEEE, Noordwijk, Netherlands (2007). https://doi.org/10.1109/ICORR.2007.4428481
Kleim, J.A., Jones, T.A.: Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J. Speech Lang. Hear. Res. 51 (2008). https://doi.org/10.1044/1092-4388(2008/018)
Dunaj, J., Klimasara, W.: Rozwiązania sprzętowe i programowe w sterowaniu robotami rehabilitacyjnymi Renus. Pomiary Automatyka Robotyka, pp. 100–115 (2014)
Klimasara, W., Dunaj, J., Stempnik, P., Pilat, Z.: Zrobotyzowane systemy RENUS-1 oraz RENUS-2 do wspomagania rehabilitacji ruchowej po udarach mózgu. Pomiary Automatyka Robotyka. 2, 577–589 (2009)
Mikołajewska, E., Mikołajewski, D.: Wykorzystanie robotów rehabilitacyjnych do usprawniania. Niepełnosprawność – zagadnienia, problemy, rozwiązania (2013)
Dunaj, J., Klimasara, W.J., Pilat, Z.: Human-robot interaction in the rehabilitation robot renus-1. In: Szewczyk, R., Kaliczyńska, M. (eds.) SCIT 2016. AISC, vol. 543, pp. 358–367. Springer, Cham (2017). https://doi.org/10.1007/978-3-319-48923-0_39
Park, H.-S., Ren, Y., Zhang, L.-Q.: IntelliArm: an exoskeleton for diagnosis and treatment of patients with neurological impairments. In: 2008 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics. pp. 109–114. IEEE, Scottsdale, AZ, USA (2008). https://doi.org/10.1109/BIOROB.2008.4762876
Cerasa, A., et al.: Exoskeleton-robot assisted therapy in stroke patients: a lesion mapping study. Front. Neuroinform. 12, 44 (2018). https://doi.org/10.3389/fninf.2018.00044
Milot, M.-H., et al.: A crossover pilot study evaluating the functional outcomes of two different types of robotic movement training in chronic stroke survivors using the arm exoskeleton BONES. J. NeuroEng. Rehabil. 10, 112 (2013). https://doi.org/10.1186/1743-0003-10-112
Lum, P.S., Godfrey, S.B., Brokaw, E.B., Holley, R.J., Nichols, D.: Robotic approaches for rehabilitation of hand function after stroke. Am. J. Phys. Med. Rehabil. 91, S242–S254 (2012). https://doi.org/10.1097/PHM.0b013e31826bcedb
Babaiasl, M., Mahdioun, S.H., Jaryani, P., Yazdani, M.: A review of technological and clinical aspects of robot-aided rehabilitation of upper-extremity after stroke. Disab. Rehabil. Assist. Technol. 11 (2015). https://doi.org/10.3109/17483107.2014.1002539
Kim, G., et al.: Is robot-assisted therapy effective in upper extremity recovery in early stage stroke?—a systematic literature review. J. Phys. Ther. Sci. 29, 1108–1112 (2017). https://doi.org/10.1589/jpts.29.1108
Heo, P., Gu, G.M., Lee, S., Rhee, K., Kim, J.: Current hand exoskeleton technologies for rehabilitation and assistive engineering. Int. J. Precis. Eng. Manuf. 13, 807–824 (2012). https://doi.org/10.1007/s12541-012-0107-2
Piazza, C., et al.: The SoftPro project: synergy-based open-source technologies for prosthetics and rehabilitation. In: Carrozza, M. C., Micera, S., Pons, J.L. (eds.) WeRob 2018. BB, vol. 22, pp. 370–374. Springer, Cham (2019). https://doi.org/10.1007/978-3-030-01887-0_71
Acknowledgements
This research was financed by the National Centre for Research and Development, Poland, under grant No POIR.01.02.00-00-0014/17 and was co-financed by the Ministry of Education and Science of Poland under grant No DWD/3/7/2019 - RJO15/SDW/001.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Ethics declarations
The authors have no conflict of interest to declare.
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this paper

Cite this paper
Sobiech, M., Wolański, W., Karpiel, I. (2022). Brief Overview Upper Limb Rehabilitation Robots/Devices. In: Biele, C., Kacprzyk, J., Kopeć, W., Owsiński, J.W., Romanowski, A., Sikorski, M. (eds) Digital Interaction and Machine Intelligence. MIDI 2021. Lecture Notes in Networks and Systems, vol 440. Springer, Cham. https://doi.org/10.1007/978-3-031-11432-8_29
Download citation
DOI: https://doi.org/10.1007/978-3-031-11432-8_29
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-11431-1
Online ISBN: 978-3-031-11432-8
eBook Packages: Intelligent Technologies and RoboticsIntelligent Technologies and Robotics (R0)