
Abstract
The effects of sevoflurane or isoflurane on arterial blood gas, arterial oxyhaemoglobin saturation and end-tidal CO2 tension were monitored during induction and maintenance of anaesthesia in 10 premedicated New Zealand White (NZW) rabbits.
For induction, the anaesthetic agents were delivered via a face-mask. After induction was completed, an endotracheal tube was introduced for maintenance of anaesthesia for a period of 90 minutes. Changes in heart rate, respiratory rate, arterial blood gas, arterial oxyhaemoglobin saturation, blood pH and end-tidal CO2 tension were recorded. Although sevoflurane and isoflurane produce similar cardiopulmonary effects in premedicated rabbits, sevoflurane provides a smoother and faster induction because of its lower blood/gas partition coefficient. Thus sevoflurane is probably a more suitable agent than isoflurane for mask induction and maintenance. Its lower blood solubility also makes sevoflurane more satisfactory than isoflurane for maintenance of anaesthesia because it allows the anaesthetist to change the depth of anaesthesia more rapidly.
Similar content being viewed by others
Introduction
Sevoflurane is a rapid-acting, inhaled anaesthetic used frequently in human beings and increasingly in animal patients in clinical practice. It has emerged as the most promising agent for inhalation induction in human patients [12, 1]. Due to its low blood solubility (its blood/gas partition coefficient is 0.68), induction and emergence are rapid [13, 14, 1, 4]. Sevoflurane has a pleasant, non-pungent odour which permits a smooth and rapid induction by inhalation; it has made mask induction more attractive [12, 1].
Continuous monitoring of end-tidal CO2 (ETCO2) tension and arterial oxyhaemoglobin saturation by pulse oximetry (SpO2) has been considered the minimal standard of care during anaesthesia. The technology to objectively and non-invasively assess gas exchange in anaesthetised animals has recently become readily available. Because of the potential problems associated with hypoventilation, it is important to closely monitor the ventilation status of animals during inhalation anaesthesia by assessing PaCO2 [8]. Capnography and pulse oximetry allow for continuous and non-invasive monitoring of ventilation and oxygenation, respectively, in anaesthetised animals [5]. Arterial blood gas analysis is an invasive monitoring procedure. However, analysis of carbon dioxide and oxygen in an arterial blood sample defines sufficiency of gaseous exchange.
The cardiovascular effects of sevoflurane appear to be comparable to those of isoflurane. However, the effects of this agent on blood gas, arterial oxyhaemoglobin saturation and end-tidal CO2 tension in rabbits have not been well studied.
The purposes of this study were to determine the effects of sevoflurane on arterial blood gas, arterial oxyhaemoglobin saturation, end-tidal CO2 tension and physiological parameters in rabbits and to compare these effects with those induced by isoflurane.
Materials and methods
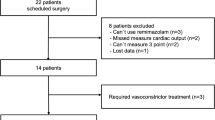
Twenty (10 male, 10 female) young New Zealand White rabbits, aged six to 12 months and weighing 4.2 ± 0.6 kg (mean ± 1 SD) were obtained from a research centre for breeding test animals in Uludag University (Turkey) and were free from recognised respiratory pathogens (Pasteurella and Bordetella spp). The rabbits were floorhoused in groups, on dust-free shavings and autoclaved hay. They were fed a commercial pelleted diet (Ankara Feedstuff Industry, Turkey) and water ad libitum. No animal was used more than once.
All experiments were conducted in accordance with the Animal Research Ethics Committee at the Uludag University of Turkey.
Apparatus
A small plastic face-mask (Kruuse [Veterinary Equipment] Ltd, Marslev, Denmark) and a Jackson-Rees modification of the Ayre's T-piece were used for induction. Isoflurane was delivered from an Isoflurane A-3 vaporiser (Kimura Medical Co., Tokyo, Japan) and sevoflurane from a temperature and flow compensated vaporiser (Blease, Genuine Part, England). Both agents were delivered in 100% oxygen at 4 L/minute. Electrodes were placed on the rabbit's skin, on the medial aspects of the upper forelegs and of the upper left hindleg, and the electrocardiogram was recorded by connecting the electrodes to an electronic monitoring apparatus (Burdick Medic-5, Burdick Inc., USA). Pulse oximetry (SpO2) readings and pulse rate were obtained with a pulse oximeter (Vet/OXTM 4403, SDI, USA) with the probe placed on the tongue. End-tidal CO2 (ETCO2) tension and respiratory rate were monitored continuously with a sidestream-sampling capnograph (Normocap 200, Datex-Ohmeda). During the induction period, the sampling adapter (AMS CO2 absorber for veterinary purpose, AMS Company, Ankara, Turkey) was connected between the face-mask and the Jackson-Rees modification of the Ayre's T-piece. During the maintenance period, the sampling adapter was connected between the endotracheal tube and the Jackson-Rees modification of the Ayre's T-piece in a similar manner. A catheter (22 g, IV cannula, Transplastics, Germany) was inserted into the ear artery for blood gas analysis. Arterial blood samples were collected in heparinised capillary tubes, and blood pH, PaO2 and PaCO2 were measured by blood gas analyser (RapidLab 248, Chiron Diagnostic Ltd, Halstead, Essex, UK). Lactated Ringer's solution (10 ml/kg per hour) was administered into the other ear vein.
Experimental protocol
The animals were prepared as described above. After a five to 10 minute period, baseline measurements were recorded. Xylazine (3 mg/kg: Rompun®, Bayer, Turkey) was injected intramuscularly, for premedication. The animals were restrained manually by gently positioning the operator's arms on either side of the animal's body. After placement of the face-mask, 100% oxygen was provided for two to three minutes at a fresh gas flow rate of 4 L/minute. Any struggling was noted by an observer, and this was used to assess the quality of induction. After this initial period, sevoflurane (Sevorane®, Abbott, UK) at a vaporiser setting of 6%, or isoflurane (Forane®, Abbott, UK) at a vaporiser setting of 4%, was delivered in the oxygen stream in a similar manner. The anaesthetic gas concentration was maintained at this level until induction was completed. When induction was complete, an endotracheal tube was inserted using a premature baby laryngoscope and the non-rebreathing system was attached to it. The anaesthetic vaporiser was then turned to a setting of 3% (sevoflurane) or 2% (isoflurane) for maintenance of anaesthesia for a 90 minute period.
Cardiopulmonary responses (heart rate, respiratory rate, rectal temperature, arterial oxyhaemoglobin saturation and end-tidal CO2 tension) and blood gas values were recorded every 15 minutes from the time of induction to the beginning of recovery. After anaesthesia, all rabbits were extubated and observed in the post-anaesthesia care unit for a further hour.
Data analysis
All data were expressed as mean ± 1 SD. The cardiopulmonary variables and values for time to event were compared between groups using one-way analysis of variance (ANOVA) for repeated measures. If statistically significant effects were found, Tukey's post hoc test was applied to the differences between groups. The changes within each anaesthetic group were compared using one-way ANOVA for repeated measures, followed by Tukey's post hoc test when appropriate. Values of P < 0.05 were considered statistically significant.
Results
Cardiopulmonary data recorded during mask induction and maintenance of anaesthesia with sevoflurane and isoflurane are summarised in Table 1. Pre-induction values for each variable in conscious and premedicated animals were not significantly different between the sevoflurane group and the isoflurane group. Intramuscular administration of xylazine induced moderate sedation in both groups. Placement of the face-mask and administration of oxygen did not cause any change in respiratory rate. Exposure to sevoflurane caused very little aversion and relatively few bouts of struggling behaviour. In contrast, isoflurane induced excessive struggling in all animals, necessitating very firm restraint, in spite of sedation.
Times to loss of the palpebral reflex and to successful tracheal intubation were significantly shorter with sevoflurane (126 seconds ± 36) than with isoflurane (150 seconds ± 31). None of the rabbits given sevoflurane had episodes of induction-related complications (struggling, ataxia or excitement).
Cardiopulmonary effects of sevoflurane and isoflurane, during the induction and maintenance periods, were similar with the exception of a slightly decreased heart rate in the sevoflurane group. The heart rate values during anaesthesia with isoflurane were slightly higher than pre-induction rates, although they were still within the physiological reference range.
A decrease in respiratory rate compared with the pre-induction rate was observed during induction and maintenance with both agents. An associated respiratory acidosis, characterised by an increase in PaCO2, was observed in both groups. The respiratory depressant effects, characterised by increased PaCO2 and decreased blood pH values, were associated with decreases in respiratory rate. Arterial PaCO2 rose from 30.5 mmHg (±7.0) to a peak of 50.6 mmHg (±10.2) in the sevoflurane group and from 33.6 mmHg (±5.4) to a peak of 51.5 mmHg (±11.7) in the isoflurane group. Blood pH values were normal in all animals prior to induction and fell to 7.25 ± 0.11 during sevoflurane anaesthesia and to 7.16 ± 0.09 during isoflurane anaesthesia. These changes were significant (P < 0.05). Time to recovery of righting reflex also differed significantly between treatment groups: 219 seconds (±103) in the sevoflurane group versus 615 seconds (±326) in the isoflurane group. The recovery was smooth and uneventful in all rabbits.
Discussion
This study was designed to monitor arterial blood gas, arterial oxyhaemoglobin saturation and end-tidal CO2 tension in rabbits during mask induction and maintenance of anaesthesia with sevoflurane and isoflurane. The adverse effects of halogenated volatile anaesthetics associated with mask induction, as experienced clinically in animals, are characterised by apnoea, breath-holding, laryngospasm, bronchoconstriction or body movements [7, 9, 10]. Some of these induction-related complications (e.g., struggling) also accompany mask induction in rabbits [2, 4] and dogs [8]. In this experiment, induction-related complications induced by isoflurane necessitated very firm restraint in spite of sedation whereas these complications were not evident when sevoflurane was used. This was unlike the study reported by Flecknell et al. [4]. However, none of their rabbits were premedicated.
The protocol followed for face-mask induction was identical to that used in the study by Flecknell et al. [4], which had been derived from standard veterinary anaesthetic induction and maintenance methodology. Because of the occurrence of periods of apnoea in the study by Flecknell et al. [4], inhalation of a gradually rising concentration of anaesthetic was not used here. It was thought that a technique that gives a rapid increase in the concentration of the inhaled agent during mask induction may be more appropriate than a technique that delivers a slowly increasing concentration of the agent. By rapid mask induction, it was possible to avoid long induction periods and violent struggling efforts. Surgical anaesthesia was reached faster with sevoflurane than with isoflurane because of the lower blood/gas partition coefficient.
In this study, xylazine was selected for premedication because it produced light to moderate sedation with small changes in cardiopulmonary functions in rabbits. It was clearly demonstrated that the use of xylazine improved the speed and quality of mask induction with sevoflurane. This procedure did not appear to distress the rabbits in the sevoflurane group but, as in previous studies [2, 4, 6], there was considerable evidence that rabbits resent mask induction with isoflurane, as expressed by violent struggling and pawing at their faces to remove the face-mask.
Monitoring is essential during anaesthesia. In rabbits, as with other animals, it is possible to use invasive and non-invasive procedures [8, 5]. Non-invasive techniques include capnography, pulse oximetry, assessment of heart rate, respiratory rate and rectal temperature. The invasive techniques of blood arterial gas analysis were applied in this study.
Both inhalants had similar cardiopulmonary effects during the induction and the maintenance periods, with the exception of a decreased heart rate in the sevoflurane group. The heart rate values during anaesthesia with isoflurane were higher than preinduction rates, although they were still within the physiological reference range for maintenance under isoflurane anesthesia. The difference in heart rates between two groups may have been related to more stress in rabbits anaesthetised with isoflurane because it is more irritating than sevoflurane [8, 4, 6]. [11] reported that inhalation of 1% to 4% isoflurane in anaesthetised rabbits has been shown to increase heart rate as a result of direct sympathetic stimulation, in addition to stimulation of the baroreflex elicited by a decrease in arterial blood pressure.
All volatile anaesthetic agents have been reported to cause a doserelated respiratory depression in rabbits [2–4, 11, 6]. In this study, decreased respiratory rates, which were reflected in higher end-tidal CO2 tensions, were recorded in both anaesthetic groups. The mild respiratory depression was qualitatively similar to those of previous studies in anaesthetised rabbits [4, 6]. It is possible that slowing of breathing during induction and maintenance of anaesthesia is caused by both respiratory reflexes and anaesthetic effects of the inhalants.
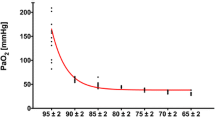
As in previous studies [4, 6], respiratory depression due to volatile anaesthetic agents produced elevations of arterial PaCO2 and end-tidal CO2 tension. However, reduction in arterial PaO2 and hypoxaemia did not occur. Arterial oxyhaemoglobin saturation was constant during the anaesthetic period with both agents predictable because of the high inspired oxygen fraction.
In conclusion, both sevoflurane and isoflurane produced similar cardiopulmonary effects in premedicated rabbits. However, sevoflurane was considered a more suitable agent for mask induction since it provided a smoother and more rapid induction, due to its lower blood/gas partition coefficient. Its lower blood solubility also makes sevoflurane more desirable for maintenance of anaesthesia than isoflurane because of the facility to change the depth of anaesthesia more rapidly and to hasten recovery.
References
Ebert TJ, Robinson BJ, Uhrich TD, Mackenthun A, Pichotta PJ: Recovery from sevoflurane anaesthesia: A comparison of isoflurane and propofol anesthesia. Anaesthesiology. 1998, 89: 1524-1531. 10.1097/00000542-199812000-00032.
Flecknell PA, Cruz IJ, Liles JH, Whelan G: Induction of anaesthesia with halothane and isoflurane in the rabbit: a comparison of the use of a face-mask or an anaesthetic chamber. Laboratory Animals. 1995, 30: 67-74. 10.1258/002367796780744910.
Flecknell PA, Liles JH: Halothane anaesthesia in the rabbit: a comparison of the effects of medetomidine, acepromazine and midazolam on breath-holding during induction. Journal of the Association of Veterinary Anaesthetists. 1996, 23: 11-14. 10.1111/j.1467-2995.1996.tb00275.x.
Flecknell PA, Roughan JV, Hedenqvist P: Induction of anaesthesia with sevoflurane and isoflurane in the rabbit. Laboratory Animals. 1999, 33: 41-46. 10.1258/002367799780578516.
Grosenbaugh DA, Muir WW: Accuracy of noninvasive oxyhaemoglobin saturation, end-tidal carbon dioxide concentration, and blood pressure monitoring during experimentally induced hypoxemia, hypotension, or hypertension in anesthetised dogs. American Journal of Veterinary Research. 1998, 59: 205-212.
Hedenqvist P, Roughan JV, Antunes L, Orr H, Flecknell PA: Induction of anaesthesia with desflurane and isoflurane in the rabbit. Laboratory Animals. 2001, 35: 172-179. 10.1258/0023677011911561.
Mitsuhata H, Saitoh J, Shimizu R, Takeuchi H, Hasome N, Horiguchi Y: Sevoflurane and isoflurane protect against bronchospasm in dogs. Anaesthesiology. 1994, 81: 1230-1234. 10.1097/00000542-199411000-00017.
Mutoh T, Nishimura R, Kim HY, Matsunaga S, Kadosawa T, Mochizuki M, Sasaki N: Rapid inhalation induction of anaesthesia by halothane, enflurane, isoflurane and sevoflurane and their cardiopulmonary effects in dogs. Journal of Veterinary Medicinal Science. 1995, 57: 1007-1013.
Mutoh T, Kojima K, Takao K, Nishimura R, Sasaki N: Comparison of sevoflurane with isoflurane for rapid mask induction in midazolam and butorphanol sedated dogs. Journal of Veterinary Medicine Series-A. 2001, 48: 223-230. 10.1046/j.1439-0442.2001.00350.x.
Mutoh T, Kanamaru A, Tsubone H, Nishimura R, Sasaki N: Respiratory reflexes in response to upper airway administration of sevoflurane and isoflurane in anaesthetised spontaneously breathing dogs. Veterinary Surgery. 2001, 30: 87-96. 10.1053/jvet.2001.20329.
Okamoto H, Hoka S, Kawasaki T, Okuyama T, Takashashi S: Dose-dependent increases in the renal sympathetic nerve activity during rapid increase in isoflurane concentration in intact, lower airway-deafferented, and baroreceptor-deafferented rabbits. Anaesthesiology. 1996, 84: 1196-1204. 10.1097/00000542-199605000-00022.
Smith I, Ding Y, White PF: Comparison of induction, maintenance, and recovery characteristics of sevoflurane-N2O and propofol-sevoflurane-N2O with propofol-isoflurane-N2O anaesthesia. Anaesthesia and Analgesia. 1992, 74: 253-259. 10.1213/00000539-199202000-00015.
Strum DP, Eger EI: Partition coefficients for sevoflurane in human blood, saline, and olive oil. Anaesthesia and Analgesia. 1987, 66: 654-656.
Young CJ, Apfelbaum JL: Inhalation anaesthetics: Desflurane and sevoflurane. Journal of Clinical Anaesthesiology. 1995, 7: 564-577. 10.1016/0952-8180(95)00129-8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Topal, A., Gül, N. Comparison of the arterial blood gas, arterial oxyhaemoglobin saturation and end-tidal carbon dioxide tension during sevoflurane or isoflurane anaesthesia in rabbits. Ir Vet J 59, 278 (2006). https://doi.org/10.1186/2046-0481-59-5-278
Published:
DOI: https://doi.org/10.1186/2046-0481-59-5-278