
Abstract
Aluminum phosphide (AlP) is a cheap solid fumigant and a highly toxic pesticide which is commonly used for grain preservation. In Iran it is known as the “rice tablet”. AlP has currently aroused interest with increasing number of cases in the past four decades due to increased use in agricultural and non-agricultural purposesand also its easy availability in the markets has increased its misuse to commit suicide. Upon contact with moisture in the environment, AlP undergoes a chemical reaction yielding phosphine gas, which is the active pesticidal component. Phosphine inhibits cellular oxygen utilization and can induce lipid peroxidation. It was reported that AlP has a mortality rate more than 50% of intoxication cases. Poisoning with AlP has usually occurred in attempts to suicide. It is a more common case in adults rather than teen agers. In some eastern countries it is a very common agent with rapid action for suicide. Up to date, there is no effective antidote or treatment for its intoxication. Also, some experimental results suggest that magnesium sulfate, N-acetyl cysteine (NAC), glutathione, vitamin C and E, beta-carotenes, coconut oil and melatonin may play an important role in reducing the oxidative outcomes of phosphine. This article reviews the experimental and clinical features of AlP intoxication and tries to suggest a way to encounter its poisoning.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Background
Aluminum phosphide (AlP) is a solid fumigant which has been extensively used since the 1940s. It is easily available and is purchased in some countries such as India under trade names e.g. Celphos, Quickphos, Synfume and Phosfume [1]. It has been registered in the USA and many other countries for the indoor fumigation of agricultural compounds, animal feeds, processed foods and also structural as well as outdoor pest control. In Iran it is known as the rice tablet [2] that can be purchased in local shops.
AlP is a solid pesticide that rapidly became one of the most commonly used grain fumigants because of its properties which are considered to be near ideal; it is toxic to all stages of insects, highly potent, does not affect seed viability, is free from toxic residues and leaves little residue on food grains [3]. This highly toxic chemical is cheap and usually formulated in tablets or pellets, granules and as a dust. Upon contact with moisture in the environment, it undergoes a chemical reaction yielding phosphine gas, which is the active pesticidal component [4]. It emerges as a poison of suicidal deaths as this pesticide has no effective antidote and is freely available in the market [5].
AlP poisoning is a common mode of suicide in the agricultural community in northern India [6]. It has currently aroused interest with increasing number of cases in the past four decades due to increased use in agricultural and non-agricultural purpose, and also its easy availability has increased its misuse to commit suicide [7, 8]. Unfortunately, it is rapidly becoming a very commonly used agent for self-poisoning in Iran [2, 9–11].
AlP forms
It is available as tablets (3 g, trade names: Phostoxin, Bhostoxin, Quickphos Phosphume Phostek) releasing 1 g PH3 or as pellets (0.6 g, Quickphos, Alphos, Cellphos). The tablets are green, brown or gray, and each tablet contains 56% AlP and 44% aluminum carbonate.
The chemistry of AlP
The toxic effects of the AlP are due to deadly phosphine gas liberated when it reacts with water or hydrochloric acid in the stomach [4]. Phosphine gas (PH3) is the active pesticide component of AlP, which is rapidly absorbed by inhalation, ingestion, and skin or mucosal contacts [4]. AlP is available in the forms of tablets or pellets. It is the active component of the mixture so aluminum carbonate is added to prevent self-ignition of phosphine (PH3) which is liberated when AlP comes in contact with moisture. Each 3 g tablet releases 1 g of phosphine and so each 0.6 g pellet 0.2 g of phosphine gas on exposure to moisture and leaves behind a non-toxic grayish residue of aluminum hydroxide. In addition to these chemical properties, phosphine may spontaneously ignite in the presence of oxygen at concentrations above a threshold limit range of 0.48-1.9% (v/v) [12]. Phosphine gas is colorless and odorless but in exposure to air it may give a foul odor (garlicky or decaying fish) due to the presence of substituted phosphines and diphosphines [3]. Although exposures to toxicologically relevant concentrations of phosphine can occur in the absence of obvious odor detection [4].
Mechanism of action
In the case of oral intake, the phosphine gas released is absorbed by the gastrointestinal tract with simple diffusion and is mainly excreted by the kidneys and lungs. Phosphine, like cyanide, inhibits mitochondrial cytochrome oxidase and cellular oxygen utilization [13–15].
Phosphine can inhibit cytochrome C oxidase in vitro but it has much less activity in vivo [16].
It can rapidly perturb mitochondrial conformation and inhibit oxidative respiration by 70%. This situation results a severe decrease in mitochondrial membrane potential [14].
In presence of AlP cellular superoxide and peroxide radicals are generated, with subsequent cellular damage by lipid peroxidation [17–20]. The higher levels of superoxide dismuatase (SOD), malonyldialdehyde (MDA) and catalase in post-mortems suggested their direct relation to mortality. Decreasing the serum levels of these biochemical parameters to a normal profiles in survivors by day 5 lead to a restriction of oxidative stress following phosphine elimination [21]. Some experimental results suggest that glutathione, melatonin, vitamin C and carotenes play an important role in reducing the effects caused by oxidative phosphine [8].
The direct toxic effects of phosphine on cardiac myocytes, fluid loss and adrenal gland can induce profound circulatory collapse [16]. Direct corrosive effects of phosphides and phosphine on body tissues have been reported [22].
Toxicity
The fatal dose for a 70 kg adult is 150–500 mg [6, 8]. Permissible exposure limit (PET) is 0.3 ppm over an 8 h shift (for factory stuffs). The range of short term exposure limit (STEL) is 1 ppm and immediate danger to life and health would be 200 ppm. For lethal dose in 30 min, the range of 400–600 ppm (10 mg/Kg AlP) has been determined. It has been reported that its LD50 in mice (inhalation of fumes) is 0.68 g/m3 during 65–75 min of exposure and for rats is 1.47 g/m3 during 35–50 min of exposure. LD50 for cats is 25 ppm (2–4 h daily during 3 days) [23].
Etiology
AlP is the most common agent of poisoning in rural or sub-urban zones of some countries such as India, where it is usually ingested for suicide [5]. It is also uses as a suicide agent in Iran [24] but its poisoning in other countries may be due to occupational exposure [16]. AlP can induce rarely complications including hepatitis, acute tubular necrosis, gastroduodentitis, bleeding diathesis, corrosive like esophageal stricture and intravascular hemolysis [25–27].
Epidemiology
An epidemiological study investigated health endpoints among Indian workers engaged in fumigation of stored grains [28]. The mean duration of employment among these workers was 11.1 years, and workplace concentrations of phosphine gas ranged from 0.17 to 2.11 parts per million (ppm) during the period of investigation. In this study, workers did not use facemasks, gloves or aprons as personal protective equipment. The most frequently reported symptoms reported immediately after completing fumigation activities included headache (31.8%), dyspnea (31.8%) and chest tightness (27.3%). Physical examinations of these workers were unremarkable, and no significant abnormalities were observed in tests of motor and sensory nerve conduction [28]. Outside of the workplace, phosphide fumigants are frequently implicated in association with epidemiological reports of accidental morbidity and mortality. In a one-year study period in Allahabad (India) out of a total 13,100 admissions, 301 suspected poisoning cases (2.3%) of the total admissions were recorded. The prevalence of AlP poisoning in this period was 11.7% and male to female ratio was 2:1. Age distribution study showed peak prevalence in the age group 11–30 years (65.1%) belonged to the rural area whereas 92 cases (30.6%) belonged to the urban areas [29].
A three-year (1999–2001) analysis of childhood poisonings in India found that 9% of all cases resulted from exposure to agricultural pesticides, and AlP fumigants were the most frequently implicated classification (29.67% of cases). Most of these cases involved ingestion pathways of exposure resulting from improper storage of fumigants [30]. Medical outcomes were not reported in this study. In another longitudinal, retrospective review of acute poisoning deaths in northern India, the AlP fumigants were identified as the most commonly implicated poison associated with fatalities (65% of cases) [31]. In this investigation, the incidence of cases resulting in death from the AlP increased during the period of observation (1972–1997). Morbidity and mortality have also been reported from phosphine inhalation in association with the in-transit fumigation of ships and railways [32, 33]. In Iran, AlP poisoning has been reported frequently for suicide attept [34]. Unfortunately, the mortality rates were reported between 40 to 100%. In a four-year study period in northern Iran during 1997–2001, out of 1571 poisoning cases, 33 AlP poisoning cases (2.1%) were recorded [9] Another study in Gonbad (Iran), showed that out of 21 AlP poisoning cases, 19 cases have died. The mortality rate in this study was 90.5% [35]. Overall mortality rate of AlP poisoning was reported 31% in a retrospective 7 years study from 2000–2007 in Tehran [36]. Unpublished data from Babol town (Iran) showd 25 AlP poisoened cases out of total 1280 cases of poisoning during 2003–2009. In this study, 2 of 25 AlP posoning cases were intoxicated accidentaly and the others administered AlP for suicide. From nine cases of death, 7 were female. Age range was 15 to 70 with mean of 27.3. From 25 cases, 6 patients belonged to the rural area and 18 cases were from the urban sector. The ratio of male to female was 0.6 [37]. Although the percentage of poisoning with AlP is low, but the mortality rate of this kind of intoxication is very high. The mortality rate of AlP in some studies, were reported between 37-100% [34, 38].
Occupational exposure
Exposure to AlP is a common cause of poisoning from agricultural pesticide exposures in some parts of the world [30, 31, 39].
Chemicals like AlP, having a mortality rate more than 50% are easily available in the markets [40]. The epidemiology of occupational and environmental exposure to phosphine gas in association with phosphide fumigants has been reviewed by the National Institute of Occupational Safety and Health (NIOSH) [29]. Relevant findings in a 10-year study of 205 symptomatic exposures included the observation that 75% of cases occurred among individuals who were not directly handling or applying the fumigants. In 63% of cases among applicators, and 45% of cases among non-applicators, symptomatic exposure was reported to have occurred from the normal handling of phosphide fumigants (consistent with the product labeling). In this case series, approximately 25% of exposures to AlP among applicators occurred in the context of a misapplication (handling violations) [29]. There were no reported occupational cases occurring among individuals involved in the manufacturing process of phosphide fumigants in this series. A review of an epidemiological report demonstrates that occupational and environmental exposure to phosphine may also occur from scenarios that do not involve phosphide fumigants. Case reports of inhalation exposure to phosphine gas have been described in association with the clandestine synthesis of methamphetamine, as phosphine can be produced from phosphorous acid that is formed when iodine and red phosphorus are combined in aqueous media. Three fatalities have been reported from acute inhalation of phosphine gas, which occurred in a motel room where methamphetamine was being synthesized [41]. The other study described a case of transient symptoms of dizziness, headache, cough and diarrhea in a law enforcement official who was investigating a clandestine methamphetamine laboratory [42]. In this case, the affected individual was exposed to phosphine gas at a concentration of 2.7 ppb for 20–30 min [4].
Clinical manifestations
Vomiting, abdominal pain, loose motions, restlessness have been observed. Cardiovascular complications include thread pulse, tachycardia, tachypnoea, acidosis, marked hypotension, palpitation, and unresponsive shock to conventional treatment. Patients remain mentally clear till cerebral anoxia due to shock supervenes resulting in drowsiness, delirium and coma [28]. Some common complications of AlP poisoning include hemorrhage, acute renal failure, disseminated intravascular coagulation and arrhythmias. Several ECG changes ranging from ST segment elevation/depression, PR and QRS interval prolongation, complete heart block to ectopic pace making and also fibrillation have been reported following ALP poisoning. Reversible myocardial injury has been described as well [28]. In the case of AlP poisoning patients can present anteroinferior wall ischaemia with incomplete right bundle branch block (RBBB) which is progressed to idioventricular rhythm, complete RBBB, and T-wave flattening simulating myocardial ischaemia. These changes were due to toxic injury to myocardium [43].
Pulmonary edema, dyspnoea, cyanosis, & altered sensorium may be discovered in AlP poisoning. Other rare effects include hepatitis, disseminated intravascular coagulation, and acute tubular necrosis. The complications noticed are pericarditis, congestive cardiac failure, acute gastrointestinal haemorrhage and acute respiratory arrest [6, 44].
Diagnosis
Laboratory & clinical
Diagnosis is made by laboratory and clinical tests. The factors of positive history of ingestion, symptoms compatible with AlP ingestion and chemical test for phosphine positive in gastric aspirate and breath alone or in combination would help the diagnosis. The breath of AlP intoxicated patients has a garlic-like odor. The plan of diagnosis is based on the patient’s history and a positive result (blackening) on tests of the patient's breath with paper moistened with fresh silver nitrate solution due to exhalation of PH3 or by biochemical analysis of blood or gastric aspirate for phosphine [45–47].
Using filters impregnated with silver nitrate [48] and ion chromatographic methods [49] were recruited to determine phosphine in the bio-samples. Gas chromatographic procedure in survivors [50–52] and post-mortem specimens [53] has been developed for the measurement of phosphine levels.
Gas chromatographic technique using a nitrogen phosphorus detector has been introduced for phosphine measurement in post mortem stomach contents, blood, and liver specimens [54].
Laboratory assessment is mainly done to obtain the prognosis. Leucopenia indicates severe AlP toxicity. Increased serum glutamic oxaloacetic transaminase (SGOT) or serum glutamic pyruvic transaminase (SGPT) and induced metabolic acidosis indicate moderate to severe AlP overdose. Decreased plasma magnesium level has been reported while potassium might have been increased or decreased [55]. Plasma raised level of renin is significant as its level has a direct relationship with mortality and proportion to the dose of AlP. The serum level of cortisol is usually decreased in severe AlP poisoning [56].
It has been demonstrated that AlP can induce hepatotoxicity. The main findings were sinosoid conjestion, fatty liver changes, central vein conjestion, destruction of neucleos of hepatocytes and centrilubolar necrosis. Manifestations of hepatotoxicity usually develop 72 hours after AlP intoxication. Death due to acute hepatocellular toxicity and fulminant hepatic failure has also been reported in acute intoxication.
Cardiovascular and respiratory system changes can also lead to death [16, 57]. In myocardial tissue, AlP induces conjestion, necrosis and leucocytes infiltration [38]. ECG shows various manifestations such as ST depression or elevation, bundle branch block, ventricular tachycardia, ventricular fibrillation [28, 58–60]. Wall motion abnormalities, decreased ejection fraction, generalized hypokinesia of the left ventricle, and pericardial effusion can be seen in echocardiography [61].
Edema, congestion, hemorrhage, athlectasia, capilary vasodialation and alveolar wall thikening were the most pulmonary complications of AlP intoxication [38]. Chest X-ray may represent hilar or perihilar congestion, when ARDS occurs [58].
Patients may demonstrate hyperglycemia and metheomoglubinemia [24, 62]. Development of refractory shock, ARDS, aspiration pneumonitis, anaemia, metabolic acidosis, electrolyte imbalance, coma, severe hypoxia, gastrointestinal bleeding, and pericarditis may be observed following acute AlP poisoning but these manifestations are associated with poor prognosis. The outcome of intoxication correlates best with the number of vomiting the patient gets after ingestion and the severity of hypotension the patient develops [44].
Simplified Acute Physiology Score II (SAPSII) was proposed to better estimating the outcome of paitients with acute AlP poisoning requiring ICU admission. Based on a study, SAPSII calculated within the first 24 hours was recognized as a good prognostic indicator [63].
Postmortem findings
Biochemical and histopathological findings in post-mortem cases revealing pulmonary oedema, asphyxic lesions in the pulmonary parenchyma, gastrointestinal mucosal congestion, and petechial haemorrhages on the surface of liver and brain. Desquamation of the lining epithelium of the bronchioles, vacuolar degeneration of hepatocytes, dilatation and engorgement of hepatic central veins, sinusoids and areas showing nuclear fragmentation [64, 65].
Experimental study
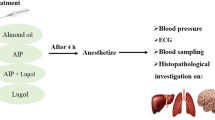
Many studies were done to obtain possible antidote or treatment of AlP intoxication [44, 66–68]. Magnesium content is decreased by AlP poisoning and it is believed that to compensate the magnesium levels can deteriorate the AlP poisoning outcomes [67, 69]. AlP poisoning was intensity induced in mice to achieve an antidote [34]. In that study, male albino mice were intoxicated by AlP (10, 20 and 40 mg/kg) and its LD50, histopathological effects on heart, lung, kidney and liver were studied. The dose 40 mg/kg of AlP was considered as the LD50. The mice that were exposed to this dose died during 35 ± 15 min. Pathologic findings showed common microscopic changes in the liver. Trying to achieve an antidote, showed that also pretreatment of sodium selenite has not affected mortality latency, but it decreased the pulmonary and hepatic complications (Table 1). This result is consistent with previous studies [70, 71]. N-acetyl systeine (NAC) in dose 50–100 mg/kg also improved the hepatic manifestations and prevented hepatic necrosis. This finding is in agreement to some other investigations [28, 72]. The NAC also delayed the mortality latency time up to 138 ± 13 min. Vitamin C (500–1000 mg/kg) delayed mortality latency time up to 250 ± 70 min. Based on this study pretreatment of sodium selenite does not improve the mortality rate except the pathologic findings, but the NAC delays the mortality latency time and can prevent hepatic complications [34]. It is suggested that the NAC can be administered as an effective treatment in AlP poisoned patients. Since sodium selenite can inhibit free radicals production and prevent oxidative stress [73–75], should be considered as a possible treatment in the case of AlP poisoning.
Role of exposure route
The presenting symptoms depend on the route of administration. Poisoning by inhalation produces irritation of the mucous membrane, dizziness, easy fatigability, nausea, vomiting, headache and diarrhea in mild exposure. Ataxia, numbness, paraesthesia, muscle weakness, paralysis, diplopia and jaundice result from a moderate degree of exposure. In severe cases of inhalational poisoning, the patient presents with acute respiratory distress syndrome (ARDS), congestive cardiac failure, convulsion and coma. Nausea, vomiting and abdominal pain are the earliest symptoms that appear after ingestion. Gastrointestinal manifestations which present in moderate to severe intoxication are abdominal pain, epigastric tenderness and excessive thirst while cardiovascular abnormalities seen are profound hypotension, dry pericarditis, myocarditis, acute congestive heart failure and arrhythmias. Involvement of the respiratory system may lead to dyspnoea, which may progress to Type I or II respiratory failure. Nervous system manifestations include headache, dizziness, altered mental status, convulsion, acute hypoxic encephalopathy and coma. Renal and hepatic failures are the other manifestations. Some rare findings in AlP poisoning are muscular weakness, wasting, tenderness in proximal lower limb muscles, bleeding diathesis due to capillary damage, acute adrenocortical insufficiency and the pseudoshock syndrome due to impaired fluid distribution which results in micro-circulatory failure [76].
Mortality
The specified fatal dose of AlP is 0.15-0.5 g. However, most of the patients present with ingestion of three or more tablets which invariably results in death [3]. The average time interval between ingestion of AlP and death is three hours (1–48 hours), 95% of the patients die within 24 hours and the commonest cause of death in this group is cardiac dysrhythmia. Severity of poisoning depends upon type of compound consumed. Fresh and active compounds (tablets) commonly affect heart, lungs, GI tract and kidneys; causing severe metabolic acidosis and high mortality. Broken or granular forms of tablets cause mild hypotension and ECG changes; mild metabolic acidosis and low mortality as activity of compound is less. Powder form of tablets is inactive; cause no systemic effects & no mortality [77]. Death after 24 hours is usually due to shock, acidosis, ARDS and cardiac dysrhythmia. Mortality depends upon dose of poison, severity of poisoning, duration of shock, failure of response of shock to resuscitative measures & severity of hypomagnesaemia [78]. Non-survivors have more severe hypotension and metabolic acidosis than the survivors who have more severe vomiting [44]. The mortality rate is highly variable, ranging from 37-100% and can reach more than 60% even in experienced and well equipped hospitals [3].
Management
General
Managing AlP poisoning, should be started as soon as possible. For confirmatory diagnosis getting history and clinical examination should not be delayed [79]. To reduce the absorption of phosphine gastric lavage with potassium permanganate (1:10,000) is done. Potassium permanganate (1:10000) is used as it oxidizes PH3 to form non-toxic phosphate. This is followed by slurry of activated charcoal (approximately 100 g) given through a nasogastric tube. Some cathartic (liquid paraffin) is given to accelerate the excretion of AlP and phosphine. Antacids and proton pump blockers are added for symptomatic relief [61, 76]. Correction of plasma glucose level can help the patient to get better [24, 79, 80].
The most important factor for success is resuscitation of shock and institution of supportive measures as soon as the patient’s arrival. IV line should be established and 2–3 liters of normal saline should be given within the first 8–12 h guided by central venous pressure (CVP) and pulmonary capillary wedge pressure (PCWP). The aim is to keep the CVP at around 12–14 cm of water [81]. Some reports have recommended rapid infusion of saline (3–6 liters) in the initial 3 hr. 24 Low dose dopamine (4–6 μg/kg/min) is given to keep systolic blood pressure >90 mm Hg. Hydrocortisone 200–400 mg every 4–6 h is given intravenously to combat shock, reduce the dose of dopamine, check capillary leakage in lungs (ARDS) and to potentiate the responsiveness of the body to endogenous and exogenous atecholamines [10–12]. Oxygen is given for hypoxia. ARDS requires intensive care monitoring and mechanical ventilation. Phosphine excretion can be increased by maintaining adequate hydration and renal perfusion with intravenous fluids and low dose dopamine (4–6 μg/kg/min). Diuretics like furosemide can be given if systolic blood pressure is >90 mm Hg to enhance excretion as the main route of elimination of phosphine is renal [82]. All types of ventricular arrhythmias are seen in these patients and the management is the same as for arrhythmias in other situations [82]. Bicarbonate level less than 15 mEq/L requires sodabicarb in a dose of 50–100 mEq intravenously every 8 hour till the bicarbonate level rises to 18–20 mEq/L. Patients may require up to 300–500 ml of sodium bicarbonate [59]. Dialysis may be required for severe acidosis and acute renal failure [3].
Specific therapy
The clinical management of intoxication from AlP is mainly supportive. The administration of H2 receptor antagonists has been recommended after AlP ingestion to reduce the gastric acidity and prevent further liberation of phosphine gas. Hypo-magnesemia is a common outcome of acute poisoning of phosphine gas exposure [66] and intracellular magnesium plays an important role as a co-factor in the synthesis and activity of glutathione and other antioxidants, the administration of intravenous magnesium has been investigated in cases of AlP poisoning. In a trial of 50 patients, individuals receiving repeated doses of intravenous magnesium had significant improvement in indicators of oxidative stress and a lower incidence of mortality (20%) in comparison to control subjects (44% mortality) [74]. Oral administration of the anti-ischemic drug trimetazidine, which works through a metabolic mechanism of decreasing the production of oxygen-derived free radicals and stimulating the oxidative metabolism of glucose [83, 84] has been suggested. It was temporally associated with clinical improvement in a case report of occupational inhalation exposure to phosphine gas from AlP [85]. Magnesium sulphate use (both high and low dose) did not improve survival in controlled clinical trials. Hence using it is not recommended [86]. Administration of sorbitol solution (at a dose of 1-2 ml/kg) as a cathartic and vegetable oils and liquid paraffin as inhibitor of phosphine release from the overdosed AlP has been suggested [87]. It was reported that coconut oil has a role in managing acute AlP poisoning even 6 h post ingestion [80]. Digoxin has been suggested for treatment of cardiogenic shock induced by acute AlP intoxication [88].
Conclusion
Exposure to phosphine gas released from ALP fumigants increases risks of major morbidity and mortality. There is an increasing need for improved knowledge of these risks with an emphasis on recognition, management and prevention. The fast progression to life-threatening symptoms, ineffective therapeutic ways to solve its intoxication and limited data on the efficacy of therapeutic interventions pose challenges to the clinicians and emergency staffs. People handling this fumigant must be aware of its lethal aspects. They should be prohibited from keeping and using this poison at the home. They should be advised to cover the tablets in open fields after use. They should keep their tablets away from the reach of children and other family members. Official health care system should restrict the open sales of this pesticide. Vendors and shop keepers should not sell the tablets to young people and children without proper verification and confirmation. Dealers not following the health system instructions should be punished. The manufacturers better be advised to make small packs of 2 – 3 tablets with suitable container. If possible all of the phosphide derivatives compounds should be forbidden forever for everyone.
References
Chopra JS, Kalra OP, Malik VS, Sharma R, Chandna A: Aluminium phosphide poisoning: a prospective study of 16 cases in one year. Postgrad Med J. 1986, 62: 1113-1115. 10.1136/pgmj.62.734.1113.
Mehrpour O, Singh S: Rice tablet poisoning: a major concern in Iranian population. Hum Exp Toxicol. 2010, 29: 701-702. 10.1177/0960327109359643.
Wahab A, Rabbani MU, Wahab S, Khan RA: Spontaneous self-ignition in a case of acute aluminium phosphide poisoning. Am J Emerg Med. 2009, 27: 752-756.
Sudakin DL: Occupational exposure to aluminium phosphide and phosphine gas? A suspected case report and review of the literature. Hum Exp Toxicol. 2005, 24: 27-33. 10.1191/0960327105ht496oa.
Singh D, Dewan I, Pandey AN, Tyagi S: Spectrum of unnatural fatalities in the Chandigarh zone of north-west India–a 25 year autopsy study from a tertiary care hospital. J Clin Forensic Med. 2003, 10: 145-152. 10.1016/S1353-1131(03)00073-7.
Ranga GS, Dwivedi S, Agarwal M, Kumar D: Aluminium phosphide poisoning in a young adult: a suicidal cardiotoxin simulating myocardial ischaemia. J Ind Acad Clin Med. 2004, 5: 369-
Bajpai SR: Aluminium phosphide poisoning: management and prevention. J Indian Acad Forensic Med. 2010, 32: 352-354.
Ferrer MI, Alvarez Li F, Cepero RA: Suicide by ingestion of aluminum phosphide: a case report. Emergencias. 2009, 21: 228-231.
Moghadamnia AA, Abdollahi M: An epidemiological study of poisoning in northern Islamic Republic of Iran. East Mediterr Health J. 2002, 8: 88-94.
Shadnia S, Soltaninejad K: Spontaneous ignition due to intentional acute aluminum phosphide poisoning. J Emerg Med. 2009, 40: 179-181.
Soltaninejad K, Faryadi M, Sardari F: Acute pesticide poisoning related deaths in Tehran during the period 2003–2004. J Forensic Leg Med. 2007, 14: 352-354. 10.1016/j.jflm.2006.12.011.
Kondo S, Tokuhashi K, Nagai H, Iwasaka M, Kaise M: Spontaneous ignition limits of silane and phosphine. Combustion Flame. 1995, 101: 170-10.1016/0010-2180(94)00175-R.
Rigobello MP, Scutari G, Boscolo R, Bindoli A: Induction of mitochondrial permeability transition by auranofin, a gold(I)-phosphine derivative. Br J Pharmacol. 2002, 136: 1162-1168. 10.1038/sj.bjp.0704823.
Valmas N, Zuryn S, Ebert PR: Mitochondrial uncouplers act synergistically with the fumigant phosphine to disrupt mitochondrial membrane potential and cause cell death. Toxicology. 2008, 252: 33-39. 10.1016/j.tox.2008.07.060.
Wang W, Winther JR, Thorpe C: Erv2p: characterization of the redox behavior of a yeast sulfhydryl oxidase. Biochemistry. 2007, 46: 3246-3254. 10.1021/bi602499t.
Proudfoot AT: Aluminium and zinc phosphide poisoning. Clin Toxicol (Phila). 2009, 47: 89-100. 10.1080/15563650802520675.
Almasieh M, Lieven CJ, Levin LA, Di Polo A: A cell-permeable phosphine-borane complex delays retinal ganglion cell death after axonal injury through activation of the pro-survival extracellular signal-regulated kinases 1/2 pathway. J Neurochem. 2011, 118: 1075-1086. 10.1111/j.1471-4159.2011.07382.x.
Hsu CH, Quistad GB, Casida JE: Phosphine-induced oxidative stress in Hepa 1c1c7 cells. Toxicol Sci. 1998, 46: 204-210. 10.1093/toxsci/46.1.204.
Lieven CJ, Levin LA: Tools for studying early events in optic neuropathies. Eye (Lond). 2007, 21 (Suppl 1): S21-24.
Nguyen SM, Alexejun CN, Levin LA: Amplification of a reactive oxygen species signal in axotomized retinal ganglion cells. Antioxid Redox Signal. 2003, 5: 629-634. 10.1089/152308603770310293.
Chugh SN, Arora V, Sharma A, Chugh K: Free radical scavengers & lipid peroxidation in acute aluminium phosphide poisoning. Indian J Med Res. 1996, 104: 190-193.
Glindemann D, Eismann F, Bergmann A, Kuschk P, Stottmeister U: Phosphine by bio-corrosion of phosphide-rich iron. Environ Sci Pollut Res Int. 1998, 5: 71-74. 10.1007/BF02986389.
Mittra S, Peshin SS, Lall SB: Cholinesterase inhibition by aluminium phosphide poisoning in rats and effects of atropine and pralidoxime chloride. Acta Pharmacol Sin. 2001, 22: 37-39.
Shadnia S, Mehrpour O, Abdollahi M: Unintentional poisoning by phosphine released from aluminum phosphide. Hum Exp Toxicol. 2008, 27: 87-89. 10.1177/0960327107086241.
Aggarwal P, Handa R, Wig N, Biswas A, Saxena R, Wali JP: Intravascular hemolysis in aluminium phosphide poisoning. Am J Emerg Med. 1999, 17: 488-489. 10.1016/S0735-6757(99)90255-3.
Gupta MS, Mehta L, Chugh SN, Malhotra KC: Aluminium phosphide poisoning. Two cases with rare presentation. J Assoc Physicians India. 1990, 38: 509-510.
Kapoor S, Naik S, Kumar R, Sharma S, Pruthi HS, Varshney S: Benign esophageal stricture following aluminium phosphide poisoning. Indian J Gastroenterol. 2005, 24: 261-262.
Katira R, Elhence GP, Mehrotra ML: A study of aluminum phosphide (AlP) poisoning with special reference to electrocardiographic changes. J Assoc Physicians India. 1990, 38: 471-473.
Kapoor AK, Shina US, Singh US, Mehtrotra R: An epidemiological study of aluminium phosphide poisoning at Allahabad. Int J Forensic Med Ther. 2006, 4: 1-7.
Gupta SK, Peshin SS, Srivastava A, Kaleekal T: A study of childhood poisoning at National Poisons Information Centre, all India Institute of Medical Sciences, New Delhi. J Occup Health. 2003, 45: 191-196. 10.1539/joh.45.191.
Singh D, Jit I, Tyagi S: Changing trends in acute poisoning in Chandigarh zone: a 25-year autopsy experience from a tertiary care hospital in northern India. Am J Forensic Med Pathol. 1999, 20: 203-210. 10.1097/00000433-199906000-00019.
Feldstein A, Heumann M, Barnett M: Fumigant intoxication during transport of grain by railroad. J Occup Med. 1991, 33: 64-65. 10.1097/00043764-199101000-00016.
Wilson R, Lovejoy FH, Jaeger RJ, Landrigan PL: Acute phosphine poisoning aboard a grain freighter. Epidemiologic, clinical, and pathological findings. JAMA. 1980, 244: 148-150. 10.1001/jama.1980.03310020024020.
Moghadamnia AA, Firoozjahi AR, Javadian SH, Dibavand N: Aluminium phosphide poisoning in mice and the procedure for its management. J Babol Univ Med Sci. 2000, 2: 25-33.
Moghadamnia AA, Haddadi MA: Study of acute poisoning in Gonbad during 1992–93. 1994, Tehran, Iran: 4th Congress of Asian and Ocean Toxicology and Poisonings Society , 1-
Shadnia S, Sasanian G, Allami P: A retrospective 7-years study of aluminum phosphide poisoning in Tehran: opportunities for prevention. Hum Exp Toxicol. 2009, 28: 209-213. 10.1177/0960327108097194.
Moghadamnia AA, Khalilian E, Mahdipour E, Salar N, Ghafouri M: Epidemiological study of poisoning in Babol. J Babol Univ Med Sci. 2012, 1-8. in press
Rahbar Taromsari M, Teymourpour P, Jahanbakhsh R: Survey the histopathological findings autopsy of poisoned patients with Rice Tablet (aluminium phosphide). J Guilan Univ Med Sci. 2010, 19: 56-63.
Abder-Rahman HA, Battah AH, Ibraheem YM, Shomaf MS, el-Batainch N: Aluminum phosphide fatalities, new local experience. Med Sci Law. 2000, 40: 164-168.
Pokhrel D, Pant S, Pradhan A, Mansoor S: A comparative retrospective study of poisoning cases in central, zone and district hospitals. Kathmandu Univ J Sci Eng Tech. 2008, 1: 40-48.
Willers-Russo LJ: Three fatalities involving phosphine gas, produced as a result of methamphetamine manufacturing. J Forensic Sci. 1999, 44: 647-652.
Burgess JL: Phosphine exposure from a methamphetamine laboratory investigation. J Toxicol Clin Toxicol. 2001, 39: 165-168. 10.1081/CLT-100103833.
Mathur A, Swaroop A, Aggarwal A: ECG changes in aluminium phosphide and organo phosphorus poisoning. Indian Pract. 1999, 52: 249-252.
Singh S, Singh D, Wig N, Jit I, Sharma BK: Aluminum phosphide ingestion–a clinico-pathologic study. J Toxicol Clin Toxicol. 1996, 34: 703-706. 10.3109/15563659609013832.
Chugh SN, Ram S, Chugh K, Malhotra KC: Spot diagnosis of aluminium phosphide ingestion: an application of a simple test. J Assoc Physicians India. 1989, 37: 219-220.
Khosla SN, Nand N, Khosla P: Aluminium phosphide poisoning. J Trop Med Hyg. 1988, 91: 196-198.
Mital HS, Mehrotra TN, Dwivedi KK, Gera M: A study of aluminium phosphide poisoning with special reference to its spot diagnosis by silver nitrate test. J Assoc Physicians India. 1992, 40: 473-474.
Demange M, Elcabache JM, Grzebyk M: Phosphine sampling and analysis using silver nitrate impregnated filters. J Environ Monit. 2000, 2: 476-482. 10.1039/b001990i.
Carlson M, Thompson RD: Determination of phosphine residues in whole grains and soybeans by ion chromatography via conversion to phosphate. J AOAC Int. 1998, 81: 1190-1201.
Gras R, Luong J, Hawryluk M, Monagle M: Analysis of part-per-billion level of arsine and phosphine in light hydrocarbons by capillary flow technology and dielectric barrier discharge detector. J Chromatogr A. 2009, 1217: 348-352.
Norman KN, Leonard K: Gas chromatography–mass spectrometry determination of phosphine residues in stored products and processed foods. J Agric Food Chem. 2000, 48: 4066-4070. 10.1021/jf991221v.
Roels J, Van Langenhove H, Verstraete W: Determination of phosphine in biogas and sludge at ppt-levels with gas chromatography-thermionic specific detection. J Chromatogr A. 2002, 952: 229-237. 10.1016/S0021-9673(02)00084-5.
Musshoff F, Preuss J, Lignitz E, Madea B: A gas chromatographic analysis of phosphine in biological material in a case of suicide. Forensic Sci Int. 2008, 177: e35-38. 10.1016/j.forsciint.2007.12.007.
Chan LT, Crowley RJ, Delliou D, Geyer R: Phosphine analysis in post mortem specimens following ingestion of aluminium phosphide. J Anal Toxicol. 1983, 7: 165-167.
Chugh SN, Juggal KL, Sharma A, Arora B, Malhotra KC: Magnesium levels in aluminium phosphide poisoning [Abstract]. J Assoc Physicians India. 1990, 38: 32-
Chugh SN, Ram S, Sharma A, Arora BB, Saini AS, Malhotra KC: Adrenocortical involvement in aluminium phosphide poisoning. Indian J Med Res. 1989, 90: 289-294.
Gupta MS, Malik A, Sharma VK: Cardiovascular manifestations in aluminium phosphide poisoning with special reference to echocardiographic changes. J Assoc Physicians India. 1995, 43 (773–774): 779-780.
Jain SM, Bharani A, Sepaha GC, Sanghvi VC, Raman PG: Electrocardiographic changes in aluminium phosphide (ALP) poisoning. J Assoc Physicians India. 1985, 33: 406-409.
Singh RB, Rastogi SS, Singh DS: Cardiovascular manifestations of aluminium phosphide intoxication. J Assoc Physicians India. 1989, 37: 590-592.
Siwach SB, Singh H, Jagdish , Katyal VK, Bhardwaj G: Cardiac arrhythmias in aluminium phosphide poisoning studied by on continuous holter and cardioscopic monitoring. J Assoc Physicians India. 1998, 46: 598-601.
Chugh SN, Mittal A, Seth S, Chugh K: Lipid peroxidation in acute aluminium phosphide poisoning. J Assoc Physicians India. 1995, 43: 265-266.
Shadnia S, Soltaninejad K, Hassanian-Moghadam H: Methemoglobinemia in aluminum phosphide poisoning. Hum Exp Toxicol. 2010, 30: 250-253.
Shadnia S, Mehrpour O, Soltaninejad K: A simplified acute physiology score in the prediction of acute aluminum phosphide poisoning outcome. Indian J Med Sci. 2011, 64: 532-539.
Anger F, Paysant F, Brousse F: Fatal aluminum phosphide poisoning. J Anal Toxicol. 2000, 24: 90-92.
Misra UK, Tripathi AK, Pandey R, Bhargwa B: Acute phosphine poisoning following ingestion of aluminium phosphide. Hum Toxicol. 1988, 7: 343-345. 10.1177/096032718800700408.
Chugh SN, Kumar P, Aggarwal HK, Sharma A, Mahajan SK, Malhotra KC: Efficacy of magnesium sulphate in aluminium phosphide poisoning–comparison of two different dose schedules. J Assoc Physicians India. 1994, 42: 373-375.
Siwach SB, Dua A, Sharma R, Sharma D, Mehla RK: Tissue magnesium content and histopathological changes in non-survivors of aluminium phosphide poisoning. J Assoc Physicians India. 1995, 43: 676-678.
Yazdanpanah H, Roshanzamir F, Shafaghi B, Faizi M, Elhami M, Rasekh HR: Assessment of possible protective roles of selenium, zinc, and cis-stilbene oxide against acute T-2 toxin poisoning: a preliminary report. Nat Toxins. 1997, 5: 133-135.
Siwach SB, Singh P, Dua A, Sharma D: Serum and tissue magnesium content in patients of aluminium phosphide poisoning and critical evaluation of high dose magnesium sulphate therapy in reducing mortality. J Assoc Physicians India. 1990, 42: 107-110.
Feroci G, Fini A: Study of the antioxidant effect of several selenium and sulphur compounds. J Trace Elem Med Biol. 1998, 12: 96-100. 10.1016/S0946-672X(98)80032-1.
Patteson KG, Trivedi N, Stadtman TC: Methanococcus vannielii selenium-binding protein (SeBP): chemical reactivity of recombinant SeBP produced in Escherichia coli. Proc Natl Acad Sci U S A. 2005, 102: 12029-12034. 10.1073/pnas.0505650102.
Mackenzie GG, Salvador GA, Romero C, Keen CL, Oteiza PI: A deficit in zinc availability can cause alterations in tubulin thiol redox status in cultured neurons and in the developing fetal rat brain. Free Radic Biol Med. 2011, 51: 480-489. 10.1016/j.freeradbiomed.2011.04.028.
Abder-Rahman H: Effect of aluminum phosphide on blood glucose level. Vet Hum Toxicol. 1999, 41: 31-32.
Chugh SN, Kolley T, Kakkar R, Chugh K, Sharma A: A critical evaluation of anti-peroxidant effect of intravenous magnesium in acute aluminium phosphide poisoning. Magnes Res. 1997, 10: 225-230.
Schelble T: Phosphine and phosgene. Clinical management of poisoning and drug overdose. Edited by: Haddad LM, Winchester JF. 1990, Philadelphia: W. B. Saunders Co, 1235-1240. 2
Grover A, Bansal S: Aluminium phosphide poisoning. Manual of medical emergencies. 1997, New Delhi: M M Healthcare
Chugh SN, Arora V, Kaur S, Sood AK: Toxicity of exposed aluminium phosphide. J Assoc Phys Ind. 1993, 41: 569-570.
Chugh SN, Chugh K, Ram S, Malhotra KC: Electrocardiographic abnormalities in aluminium phosphide poisoning with special reference to its incidence, pathogenesis, mortality and histopathology. J Indian Med Assoc. 1991, 89: 32-35.
Gurjar M, Baronia AK, Azim A, Sharma K: Managing aluminum phosphide poisonings. J Emerg Trauma and Shock. 2011, 4: 378-384. 10.4103/0974-2700.83868.
Shadnia S, Rahimi M, Pajoumand A, Rasouli MH, Abdollahi M: Successful treatment of acute aluminium phosphide poisoning: possible benefit of coconut oil. Hum Exp Toxicol. 2005, 24: 215-218. 10.1191/0960327105ht513oa.
Siwach SB, Jagdish K, Katyal VK, Dhall A, Bhardwaj G: Prognostic indices in aluminium phosphide poisoning observations on acidosis & central venous pressure. J Assoc Physicians India. 1997, 45: 693-695.
International Programme on Chemical Safety: Environmental health criteria 73: phosphine and selected metal phosphides. 1998, Geneva: World Health Organization, Available from: http://www.who.int/ipcs/publications
de Leiris J, Boucher F: Rationale for trimetazidine administration in myocardial ischaemia-reperfusion syndrome. Eur Heart J. 1993, Suppl G: 34-40.
Lopaschuk GD: Treating ischemic heart disease by pharmacologically improving cardiac energy metabolism. Am J Cardiol. 1998, 82: 14K-17K. 10.1016/S0002-9149(98)00532-3.
Duenas A, Perez-Castrillon JL, Cobos MA, Herreros V: Treatment of the cardiovascular manifestations of phosphine poisoning with trimetazidine, a new antiischemic drug. Am J Emerg Med. 1999, 17: 219-220.
Siwach SB, Singh P, Ahlawat S, Dua A, Sharma D: Serum & tissue magnesium content in patients of aluminium phosphide poisoning and critical evaluation of high dose magnesium sulphate therapy in reducing mortality. J Assoc Physicians India. 1994, 42: 107-110.
Goswami M, Bindal M, Sen P, Gupta SK, Avasthi R, Ram BK: Fat and oil inhibit phosphine release from aluminium phosphide-its clinical implication. Indian J Exp Biol. 1994, 32: 647-649.
Mehrpour O, Farzaneh E, Abdollahi M: Successful treatment of aluminum phosphide poisoning with digoxin: a case report and review of literature. Int J Pharmacol. 2011, 7: 761-764. 10.3923/ijp.2011.761.764.
Acknowledgment
The author thanks the staffs of emergency departments of Shahid Beheshti and Yahyanejad hospitals of Babol city for their kind assistance to get access the new databank of poisoned patients.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The author have no competing of interest.
Authors’ contribution
AAM contributed solely to whole study and the paper.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Moghadamnia, A.A. An update on toxicology of aluminum phosphide. DARU J Pharm Sci 20, 25 (2012). https://doi.org/10.1186/2008-2231-20-25
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2008-2231-20-25