
Abstract
Background
The raising prevalence of type-2 diabetes mellitus and obesity has been recognized as a major problem for public health, affecting both developed and developing countries. Impaired fasting plasma glucose has been previously associated with endothelial dysfunction, higher levels of inflammatory markers and increased risk of developing insulin resistance and cardiovascular events. Besides life-style changes, the blockade of the renin-angiotensin system has been proposed as a useful alternative intervention to improve insulin resistance and decrease the number of new type-2 diabetes cases. The aim of this clinical trial is to study the effect of the treatment with Candesartan, an angiotensin II receptor antagonist, on the insulin resistance, the plasma levels of adipoquines, oxidative stress and prothrombotic markers, in a group of non diabetic, non hypertensive, dysglycemic and obese subjects.
Methods and design
A randomized, double blind, cross-over, placebo-controlled, clinical trial was designed to assess the effects of Candesartan (up to 32 mg/day during 6 months) on the Homeostasis Model Assessment (HOMA) index, lipid profile, protrombotic state, oxidative stress and plasma levels of inflammatory markers. The participants will be recruited in the "Fundación Cardiovascular de Colombia". Subjects who fullfil selection criteria will receive permanent educational, nutritional and exercise support during their participation in the study. After a 15 days-run-in period with placebo and life-style recommendations, the patients who have a treatment compliance equal or greater than 80% will be randomlly assigned to one of the treatment groups. Group A will receive Candesartan during 6 months and placebo during 6 months. Group B will receive placebo during the first 6 months, and then, Candesartan during the last 6 months. Control visits will be programed monthly and all parameters of interest will be evaluated every 6 months.
Hypothesis
Treatment with Candesartan, could improve the HOMA index, the response to the oral glucose tolerance test and reduce the plasma levels of adipoquines, oxidative stress and prothrombotic markers, in non diabetic, non hypertense subjects with dysglycemia and abdominal obesity, recruited from a population at high risk of developing insulin resistance. These effects are independent of the changes in arterial blood pressure. Trial registration: NCT00319202
Similar content being viewed by others


Background
During the second half of the 20th century the prevalence of type-2 diabetes mellitus (DM2) has increased dramatically all over the world [1]. It has been estimated that more than 171 million people suffer from this disease and that this number could increase to 366 million by 2030, of which 298 million would be from developing countries [2]. Currently, in Latin America, the DM2 prevalence ranges from 1.2% to 8%, and it is expected to increase to 38% during the next 10 years [3]. This epidemic has been related with the growing prevalence of obesity, especially abdominal [4]. Recently, we have demonstrated that the presence of cardiovascular risk factors in the Andean population is associated with a lower cut-off point of waist circumference [5, 6] than the one used for Caucasian populations [7]. We have previously described that Andean population with pathologies like metabolic syndrome, hypertension and preeclampsia, all of them associated with an increased risk of cardiovascular diseases (CVD), presents higher plasma levels of inflammatory markers such as C-reactive protein (CRP) and proinflammatory cytokines [8–11].
Patients with DM2 have an increased risk of developing coronary artery disease by 2 to 4 fold and a higher risk of presenting recurrent and/or mortal cardiovascular events by 1.5 to 3 fold [12]. Based on the risk of developing micro-vascular complications, the American Association of Diabetes (ADA) reduced the threshold for DM2 to a fasting glucose level ≥126 mg/dl [13]. Moreover, the criteria of impaired fasting glucose (IFG) was defined as fasting glucose plasma level between ≥ 100 mg/dL and <126 mg/dL, and was proposed as equivalent to the impaired glucose tolerance (IGT) category obtained by oral glucose tolerance test (OGTT) [13]. Several articles have shown that patients with IFG have an increased risk of cardiovascular morbidity and mortality [14, 15]. This association has been explained by the participation of hyperglycemia, especially postprandial, in the development of atherosclerosis due to metabolic and structural changes of the vascular wall [16]. In the long term, this condition may result in macrovascular alterations and in the increased risk of CVD [15]. According to these observations, our group has recently showed that patients with IFG, regardless of other traditional cardiovascular risk factors, presented a higher risk of luminal coronary disease [17].
The etiological factors of DM2 have not been totally elucidated, but it is well known that insulin resistance precedes the DM2 onset by 10 to 20 years [18, 19]. Individuals with insulin resistance have impaired endothelium-dependent vasodilation and a loss of the physiological vasodilation caused by insulin [20], which is primarily due to an increased expression of the endothelial nitric oxide synthase (eNOS) [21]. It is also well known that obesity, hypercholesterolemia and diabetes are related to a reduction in flow-mediated dilation (FMD) [22, 23], which is mainly caused by the endothelial production of nitric oxide (NO).
Endothelial dysfunction is a condition defined as a decrease in the production of NO and the predominance of vasoconstrictor substances that result in an increase of the the vascular tone that predisposes to a prothrombotic and proatherogenic state [24, 25].
Intra-abdominal adipocytes are directly related to hyperinsulinemia and insulin resistance [26]. Hyperinsulinemia promotes the release of free fatty acids (FFA) from the adipocytes and their hepatic transformation into oxidized LDL, which has a higher atherogenic potential. Moreover, abdominal adipocytes are an important source of proinflammatory cytokines, such as tumor necrosis factor alpha (TNF-α) and interleukin 6 (IL-6) [27], that can reduce the expression and activity of the eNOS in human cultivated umbilical endothelium cells [28] which suggests that this could be one of the mechanisms by which abdominal obesity is related to endothelial dysfunction [29]. Furthermore, we have recently demonstrated that in cultured human endothelial cells, angiotensin II (AII), through its type 1 receptor (AT1), stimulates the TNF-α production which increases the activity of matrix metalloproteinase-2 (MMP-2)[30], enzyme that affects the endothelium structure as well as the stability of the atherosclerotic plaque [31] (Figure 1).

title. Physiopathological mechanisms relating abdominal adiposity, angiotensin II, insulin resistance and cardiovascular events. For description see text.Foot note. FFA: Free Fatty Acids, FAS:, GDPH:, IL-6: Interleukine 6, IL1β: Interleukine 1β, TNFα: Tumoral Necrosis Factor α, AI: Angiotensin I, AII: Angiotensin II, ACE: Angiotensin Converting Enzime, eNOS: endothelial Nitric Oxide Sintase, CPKII: Creatinphosphokinase-II, IRS-1: Type 1 Insulin Soluble Receptor IRS-2: Tipe 2 Insulin Soluble Receptor, GLUT-4: Type 4 Glucose Membrane Trasnporter, MMP2: Matrix Metalloproteinase-2, NO: Nitric Oxide, UPC-2: Uncoupling Portein 2, PPARs: Peroxisome Proliferator-Activated Receptors, DM2: Tipe 2 Diabetes Mellitus, CVE: Cardiovascular Events, scater line: Inhibition or delay, filled line: Activation or increment.
All of them, angiotensin receptors (AT1 and AT2 types), angiotensin converting enzyme (ACE) and angiotensinogen, are widely expressed in the human adipose tissue [32, 33]. Furthermore, the angiotensinogen gene expression is directly related to the degree of abdominal obesity [34]. Moreover, a direct correlation between body mass index and the circulating levels of angiotensinogen and AII has been reported [35]. These results demonstrate that the visceral adipocyte is both, a generator and a target tissue of the AII through the activation of AT1 and AT2 receptors. AII has regulatory functions in the adipogenesis and the size of the fat reservoir. Experiments in vitro have shown that AII indirectly induces the transformation of adipocytes precursor cells into mature fat cells [36], suggesting that this is one of the mechanisms by which AII stimulates the accumulation of the adipose tissue. In studies realized in rodents, the treatment with AII Receptor Blockers (ARBs), caused a reduction in the weight and in the size of the adipocytes independently of the food intake [37]. It is normally accepted that AT2 receptors are the most commonly and widely distributed receptors of AII, however, effects of AII mediated by AT1 receptors on the storage of triglycerides and on the activity of key lipogenic enzymes such as fatty acid synthase (FAS) and glycerol-2 dehydrogenate phosphate (GDPH) have also been demonstrated in cultured cells [38].
The increase in the production and storage of FFA induces insulin resistance through the inhibition of the transportation and phosphorylation of glucose in skeletal muscle, which produces a reduction of the glycogen synthesis and glucose oxidation rates [39]. Additionally, it has been suggested that FFA interfere with the stimulation of the expression of the glucose transporter GLUT-4 and the hexokinase activity [39]. AII and insulin share signal transduction pathways. Thus, insulin activates proteinkinase C (PKC) through the tyrosine phosphorilation of insulin receptor substrate type 1 and 2 (IRS-1 and IRS-2) and stimulates the MAP-kinase pathway signaling, whereas the AII inhibits PKC that alters the intracellular signaling of insulin [40].
All also has a stimulating effect on the transcription rate of the ob gene in human adipocytes, which codifies leptin, inhibiting appetite and regulating thermogenesis [41]. The sustained increase in leptin levels leads to leptin-resistance, moreover, high levels of leptin produce a greater expression of the uncoupling protein 2 (UPC-2) mediated by peroxisome proliferator-activated receptors (PPARs). UPC-2 interferes with the mitochondrial respiratory chain of the pancreatic β-cells, reducing the ATP generation and blocking the first peak of insulin secretion and favoring the onset of hyperglycemia [42]. Contrary to the results obtained in in vitro experiments [43], the infusion of AII to animals causes no effect over leptine expression [44]. This contradictory result could be explained by the activation of the sympathetic nervous system, which impedes the stimulating effect of AII on leptin production. Furthermore, high concentrations of leptin increase blood pressure, through sympathetic nervous activation and the sodium retention in the kidneys contributing to the development of hypertension in obese subjects [45]. The administration of ARBs in animal models, increase adiponectin plasma levels [46], which stimulate glucose utilisation and fatty-acid oxidation by activation of AMP-kinase [47]. In fact, the administration of Candesartan, an antagonist of AT1 receptor, to a group of hypertense subjects caused a reduction of adiponectin, C-reactive protein and markers of insulin resistance, such as the QUICKI index [48]. Furthermore, TNFα, another proinflammmatory cytokine, down-regulates the expression of adiponectin gene, impairs signal transduction of insulin in muscles [49] and it is proposed as a factor involved in the etiology of obesity related insulin resistance syndrome.
All acts also as a pro-oxidant substance by regulating the activity of the enzyme NADPH oxidase that catalyzes the production of reactive oxygen species (ROS), such as the superoxide anion and peroxynitrite[50]. ROS are substances that are directly related to the development of atherosclerotic plaque not only by inactivating NO but also by increasing the expression of cellular adhesion molecules that favor the migration of monocytes and leukocytes to the vascular wall [51] and by stimulating the growth, the remodeling and the migration of smooth muscle cells [52]. Moreover, AII has a procoagulant effect by stimulating the production of Plasminogen Activator Inhibitor-1 (PAI-1) [53], which is the principal endogenous inhibitor of fibrinolysis "in vivo" and is associated with atherosclerosis [54].
The treatment with ACE inhibitors (ACEIs) and ARBs has been shown to improve the peripheral insulin resistance in both, animal [55] and clinical models [56]. The mechanism by which the renin-angiotensin-aldosterone system (RAS) blockade has a beneficial effect on the responsiveness to insulin has not been totally clarified. Some changes in peripheral insulin sensitivity after treatment with ACEIs or ARBs might be partially mediated by changes in local blood flow to sites of glucose uptake [57]. However, a variety of non-haemodinamic effects have also been reported. In obese Zucker-type rats, it was demonstrated that the chronic administration of a selective ARBs produced a significant increase in the GLUT-4 expression in skeletal muscle, a reduction in the concentrations of plasma fatty acids and an improvement in the responsiveness to insulin [58]. Moreover AII also increases the expression of Hexokinase, a key enzyme in glucose metabolism of skeletal muscle [59].
ARBs have also been associated with an increase of the PPARγ activity [60] which plays an important role in the regulation of insulin action, by controlling the transcription of multiple genes involved in the metabolism of lipids and glucose [61]. Even in absence of AT1 receptors, ARBs were shown to promote the activation of PPARγ in human adipose cells, which supports the existence of additional mechanisms by which ARBs improve the responsiveness to insulin [61, 62].
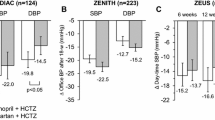
Some clinical trials have demonstrated that ACEI and ARBs reduce the number of new-onsets DM2 when compared with other anti-hypertensive therapies [63, 64]. In the study SCOPE [65] the use of Candesartan as an antihipertensive treatment, was associated with a relative reduction in new-onset diabetes by 19% (95% IC- 2 to 42%, p = 0.09) during a mean follow-up period of 3.7 years. This result is consistent with observations in other studies using blockers of the RAS in subjects with hypertension [66] including the LIFE study that compared Losartan and atenolol [67], the ALPINE study that compared Candesartan and hydroclorotiazide HCT [68], and the VALUE study that compared Amlodipine and Valsartan[63]. Moreover, results from studies conducted in normotense subjects, like the CHARM study [69], in which ARBs, caused a reduction in new-onsets DM2, suggest that the observed effects of these medications over the development of DM2 are independent of their effects over blood pressure. However, to this day, we lack results from clinical trials aimed specifically at describing the effects of the ARBs over dysglicemia/IGT in normotense non diabetic and obese subjects.
Although the mechanisms are still speculative, the results discussed above suggest that AII produced in the adipocytes of subjects with abdominal obesity is associated with insulin resistance syndrome and dysglycemia, and support the conduction of clinical trials oriented to demonstrate the beneficial effect of ARBs in the insulin sensitivity of individuals at high risk of developing CVD and DM2.
Hypothesis
Candesartan (32 mg/day during 6 months) has a beneficial effect on fasting plasma glucose, proinflammmatory, prothrombotic and oxidative stress markers in non diabetic, non hypertense subjects, with dysglicemia and abdominal obesity. The improvement of these markers is independent of changes in arterial blood pressure.
Methods/design
General objective
To evaluate the effect of Candesartan 32 mg/d during 6 months on the sensibility to insulin, the concentration of inflammatory adipoquines and the prothrombotic and oxidative stress markers in non diabetic, non hypertense subjects with dysglycemia and abdominal obesity, recruited from a population with high risk of developing metabolic syndrome and insulin resistance.
Specific objectives
▪ To establish the effect of the administration of Candesartan on the insulin resistance assessed through the HOMA index, fasting plasma glucose, OGTT, and HbA1c levels.
▪ To study the effect of Candesartan 32 mg/d administrated during 6 months on fasting plasma levels of adipoquines such as leptin, resistin, adiponectin, IL-6 and CRP.
▪ To evaluate the effect of Candesartan on prothrombotic markers, such as D dimer, tPA/PAI-1 ratio.
▪ To determine whether the administration of Candesartan decreases the concentration of oxidative stress markers such as plasma oxidized/reduced glutathione ratio, total oxidative capability, malonaldehyde and urinary 8-Isoprostanes.
▪ To determine whether the effects of Candesartan on the insulin sensibility, adipoquines and oxidative stress, are independent of its effect upon the blood pressure.
Study design
Randomized, double blind, placebo-controlled, cross-over clinical trial (Figure 2).

title. Study design.
Study treatments
▪ Treatment A: Candesartan 16 mg (one tablet per day) taken with breakfast during 4 weeks and then increased to the optimal dose of 32 mg/d (two tablets) during the next 20 weeks, depending on the subjects' tolerance.
▪ Treatment B: Placebo tablets administered similarly to treatment A, one tablet daily during 4 weeks and then 2 tablets per day during the next 20 weeks.
All the subjects will be included in a therapeutic life-style change program (TLC: educational, nutritional and exercise support) during the study.
Study groups
The study embraces two arms (Figure 2):
▪ Group 1: will receive the treatment A during the first 24 weeks and then the treatment B during the last 24 weeks.
▪ Group 2: will receive the treatment B during the first 24 weeks and then the treatment A during the last 24 weeks.
Population
Participants will be non diabetic non hypertense individuals of both genders, older than 18 years with abdominal obesity and dysglycemia and/or IGT. Inclusion and exclusion criteria are shown in Table 1
Sample size
A sample size of 84 subjects was estimated, considering a crossover clinical trial design as proposed by Hills and Armitage [70], accepting a type I error of 0.05, a power of 90%, and assuming a difference of 20 % in the HOMA index after 6 months of treatment with Candesartan (3 to 2.4) and a maximum standard deviation of 1.5. The final size of the sample, adjusted for a drop-out of 8%, is 100 subjects (50 in each group). The sample size ensures a power of 90% to detect differences in fasting glycemia of at least 8 mg/dL (0.44 mMol/L) with a standard deviation (SD) of 20 mg/dL (1.1 mMol/L), or a difference of 14 mg/dL (0.77 mMol/L) in the 2 hours post load glycemia with a SD of 40 mg/dl (2.2 mMol/L).
Procedures
Enrollment
This study will be realized in an adult population with a maximum enrollment period of one year. Screening visit will include a semi-structured interview, anthropometry and blood pressure evaluation. Eligible subjects will be scheduled one week later for "Visit A", to perform a new interview, a physical examination and to withdraw blood samples, after a 10 hour fasting period, to determine plasma glucose levels, lipid profile, hepatic and kidney function and OGTT. Those who fulfill screening criteria will be included in a run-in phase to receive placebo and the standard treatment with TLC. The patients will be blinded during this phase, which will last 2 weeks. The patients with a compliance equal or greater than 80% during this "Run in" phase will be included in the study.
Baseline assessments
Visit B will include measurements of blood pressure, anthropometric parameters, OGTT and electrocardiogram. A fasting blood sample and a 24 hour urine sample will be taken and stored (-70°C) to determine glucose, HbA1c, insulin, IL-6, leptin, resistin, adiponectin, tisular plasminogen activator (tPA), PAI-1, oxidized/reduced glutathione, malonaldehyde and 8-isoprostanes in urine. Once the patient completes the foregoing steps, during visit 1 he/she will be randomized to one of the arms of the treatment. For this purpose, a randomization system by blocks of 4 will be used. New tests will be performed at the end of each treatment, according to the study flowchart (Table 2). Randomization and preparation of medication/placebo will be done by AstraZeneca at Mölndal, Sweden.
Active follow-up
Seven days after beginning the treatment, and every month thereafter, the subjects will be asked to return for a visit in order to verify compliance, evolution of blood pressure and occurrence of adverse events. In the months 1 and 3 of each treatment, new fasting glucose determination will be done in all subjects. All basal measurements will be repeated at the end of each treatment (every 6 months).
Passive follow-up
All the subjects will undergo a passive follow-up (telephonic follow-up) 30 days after concluding the treatment.
Blood samples
In fasting conditions (at least 10 hours), blood samples will be taken from the antecubital vein, with appropriate conditions of asepsia and antisepsia, using 3 vacutainer tubes, one dry, another with citrate, and the other containing EDTA. After 10 minutes in vertical position, all samples will be centrifugated at 3000 rpm during 15 minutes to extract the serum or plasma. Part of the samples obtained during visits B, 5 and 9 will be stored in Ependorf vials at -70°C until the end of the study.
Anthropometrical measurements
All anthropometrical measurements will be taken first thing in the morning after urine elimination, with the subject using light clothing and no shoes.
Weight: will be measured with the patient standing and then registered after rounding it to the nearest 200 grams. The weight scale will be calibrated to 0 before each measurement.
Height: will be measured using a metric tape with the patient standing against the wall in Frankfort's position, and the value marked by a ruler placed horizontally on the head of the patient.
Heart rate: number of beats per minute will be measured in the radial artery.
Blood pressure: will be taken twice (with a difference of 5 minutes between the measurements) using a mercury sphygmomanometer in 2 occasions on the right arm, with the patient comfortably seated, after a 5 minute rest. Systolic blood pressure (SBP) will be determined by the first audible sound (Korotkoff phase 1). Diastolic blood pressure (DBP) will be registered when the sound disappears (Korotkoff phase 5). The patient should not have smoked 30 minutes prior to the blood pressure measurement. The pneumatic arm cuff must cover 2/3 of the upperarm's length; its inferior border must be 2–3 cm over the antecubital space; the cuff will be slowly deflated. The mean blood pressure (MBP), will be calculated using the following formula [SBP+(2*DBP)]/3
Waist circumference: will be measured in 2 occasions with the patient in a standing position, with the arms on the sides and using a measuring tape adhered to a dynamometer that exerts a force of 750 gr. The measuring tape will be placed horizontally in a middle point between the iliac crest and the anterior costal border. The difference between the two measurements should not be more than 0.5 cm.
Hip circumference: will be measured in 2 occasions with the patient in a standing position with the arms on the sides of the body, using a measuring tape adhered to a dynamometer that exerts a force of 750 gr. The hip circumference will be assessed over the major trochanters. The difference between the two measurements should not be more than 0.5 cm.
Waist-Hip Relation (W/H-R): will be obtained from the ratio between the waist and hip circumferences.
Antero-posterior diameter: will be measured twice with the patient in a decubitus supine position, using a ruler perpendicular to the bed and registering the cutting point with the tape applied horizontally on the abdomen. The difference between the two measurements should not be more than 0.5 cm.
Body Mass Index (BMI): This index will be estimated using the weight in kilograms divided by the second power of the height expressed in meters.
Biochemical markers
Routine clinical test and inflammation markers will be processed in the Clinical Research Laboratory from the "Fundación Cardiovascular de Colombia" (Floridablanca, Colombia). The measurement of oxidative stress markers will be processed in the laboratories of Complutense University (Madrid, Spain).
Glycemia, Lipid profile, Serum Creatinine, Hepatic enzymes (AST/ALT) will be quantified by a routine colorimetric method. (Biosystems BTS-303 Photometric, España).
Glycosylated Hemoglobin A1c: Will be determined with a quantitative automated technique GlycoHemoglobin Analyzer (DCA 2000+ Bayer®.) using a whole blood sample.
Insulin, High-sensitivity C-Reactive Protein and Interleukin 6: will be determined by high sensitivity chemoluminescent inmunoassay technique (IMMULITE ® Automated Analyzer, Diagnostic Products Corporation, Los Angeles, USA).
Leukocyte count and differential formula: will be determined by an automated counter (Baker System 9120 AX ®, Biochem Inmunosystem, USA).
Glucose Tolerance Test: will be done after a fasting period of at least 10 hours. After urine elimination, an intravenous catheter will be placed in the antecubital vein and blood samples will be withdrawn to assess the baseline blood glucose, then, a glucose load equivalent to 75 gr diluted in 300 mL of water will be administered to each study subject within a period of no more than 10 minutes. Then, after 2 hours, a new blood sample will be withdrawn to assess glycemia. Patients should not eat anything or do any exercise during the test.
Serum Leptin, resistin and adiponectin: will be measured by ELISA technique.
HOMA Index: Will be obtained from a mathematical model using the following formula:
Quality assurance systems
The inter- and intra-assay variation coefficient will be determined for all measurements. In order to eliminate the inter-assay error, all biochemical determinations will be performed at once.
Data processing and quality assurance
All study data will be collected by trained personnel. These data will be recorded on forms previously designed for such purpose (Case Report Form-CRF). After completing the CRF, a monitor will review them to assure that they are correctly filled and legible. All corrections will be done by the monitor according to the Good Clinical Practice guidelines. Then, the information will be typed and stored twice in independent data base. A computer program (Epi-Info 2000) will be used to compare both database. Every discrepancy will be printed and corrected using the original CRF as reference.
Data monitoring
The study coordinator will make sure that data is adequately collected. He/she will register the study visits and the time of data collection and the different procedures, as well as the compliance to the treatment.
Data management
The FCV Research Institute will be responsible for the data management. Once the data is correctly recorded, the means and ranges will be estimated and the relevant variables will be crossed to identify inconsistencies or extreme values which could result from errors in data management (internal consistency analysis). Any detected error will be corrected using the original form and the lab reports as references, maintaining the 2 original database untouched.
Modifications and statistical procedures during the data analysis will be documented in the Stata 9.0 program, which will allow the replication of the data analysis whenever necessary.
Statistical analysis
The study is set forth as an efficacy study of Candesartan in the improvement of the insulin sensibility and the OGTT results. The averages and proportions with their corresponding 95% confidence intervals will be obtained in a descriptive analysis for all clinically relevant variables measured during the baseline evaluation. In order to evaluate the presence of differences between the groups, the Student's paried t- test, the Wilcoxon's signed-rank test or the McNemar's test will be used according to the variable's characteristics. Linear multiple regression will be used with the purpose of comparing the results of the treatments. The analysis will be performed by the intention-to-treat approach. A p value under 0.05 will be considered as statistically significant.
The primary endpoint for the analysis will be the change in the value of HOMA index, fasting glucose and post-charge glucose plasma levels. The secondary endpoint for the analysis will include the changes in serum insulin, leptin, adiponectin, resistin, CRP, IL-6, tPA/PAI-1 ratio, Oxidized/Reduced glutathione ratio, malonaldehyde and 8-isoprostanes.
Treatment safety will be evaluated by the clinical history review and the statistics of the reported adverse events.
Safety committee and events assignation committee
A safety and events assignation committee will be created, according to the Harmonized Tripartite Guidelines of the International Conference of Harmonization for Good Clinical Practice.
Ethical aspects
The clinical trial will be conducted according to the Helsinki's Declaration, the Good Clinical Practice Guidelines and the Colombian legislation (Resolution 8430/93 of the Ministery of Health). The patient will provide written informed consent in a form designed for such purpose. The information generated by the study will be confidential and strictly limited to the purposes stipulated in the protocol. The patient may refuse to continue participating in the study at any moment after providing his/her consent. The study has been approved by FVC ethics committee. All assessments will be performed by trained staff. The blood samples will be collected in aseptic conditions by an expert bacteriologist.
Study timeline
The study will last 36 months. The initiation will be defined by the financial approval from the sponsor(Figure 3.).

title. Study Timeline.
Abbrebiations
(ACE) Angiotensin Converting Enzyme
(ACEIs) Angiotensin Converting Enzyme Inhibitors
(ADA) American Association of Diabetes
(AII) Angiotensin II
(AT 1 ) Angiotensin II Type 1 Receptor
(AT 2 ) Angiotensin II Type 2 Receptor
(BMI) Body Mass Index
(CRF) Case Report Form
(CRP) C-reactive Protein
(CVD) Cardiovascular Diseases
(DBP) Diastolic Blood Pressure
(DM2) Type-2 Diabetes Mellitus
(eNOS) Endothelial Nitric Oxide Synthase
(FAS) Fatty Acid Synthase
(FCV) Fundacion Cardiovascular de Colombia
(FFA) Free Fatty Acids
(FMD) Flow-Mediated Dilation
(GDPH) Glycerol-2 Dehydrogenate Phosphate
(HOMA) The Homeostasis Model Assessment
(IFG) Impaired Fasting Glucose
(IGT) Impaired Glucose Tolerance
(IL-6) Interleukine 6
(IRS-1 and IRS-2) Insulin Receptor Substrate Type 1 and 2
(MBP) Mean Blood Pressure
(MMP-2) Matrix Metalloproteinase-2
(NADPH) Nicotinamide Adenine Dinucleotide Phosphate Hydrogen
(NO) Nitric Oxide
(OGTT) Oral Glucose Tolerance Test
(PAI-1) Plasminogen Activator Inhibitor-1
(PKC) Proteinkinase C
(PPARs) Peroxisome Proliferator-Activated Receptors
(RAS) Renin-Angiotensin-Aldosterone System
(ROS) Reactive Oxygen Species
(SBP) Systolic Blood Pressure
(SD) Standard Deviation
(TLC) Therapeutic Life-Style Change Program
(TNF-α) Tumor Necrosis factor alpha
(tPA) Tisular Plasminogen Activator
(UPC-2) Uncoupling Protein 2
(W/H-R) Waist-Hip Relation
References
Yach D, Hawkes C, Gould CL, Hofman KJ: The global burden of chronic diseases: overcoming impediments to prevention and control. JAMA. 2004, 291: 2616-2622. 10.1001/jama.291.21.2616.
Wild S, Roglic G, Green A, Sicree R, King H: Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004, 27: 1047-1053.
Aschner P: Diabetes trends in Latin America. Diabetes Metab Res Rev. 2002, 18 Suppl 3: S27-S31. 10.1002/dmrr.280.
James PT, Rigby N, Leach R: The obesity epidemic, metabolic syndrome and future prevention strategies. Eur J Cardiovasc Prev Rehabil. 2004, 11: 3-8. 10.1097/01.hjr.0000114707.27531.48.
Perez M, Casas JP, Cubillos-Garzon LA, Serrano NC, Silva F, Morillo CA, Lopez-Jaramillo P: Using waist circumference as a screening tool to identify Colombian subjects at cardiovascular risk. Eur J Cardiovasc Prev Rehabil. 2003, 10: 328-335. 10.1097/01.hjr.0000095050.46631.6f.
Garcia RG, Cifuentes AE, Caballero RS, Sanchez L, Lopez-Jaramillo P: A proposal for an appropriate central obesity diagnosis in Latin American population. Int J Cardiol. 2006, 110: 263-264. 10.1016/j.ijcard.2005.08.017.
National Cholesterol Education Program NHLBINIH: Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001, 285: 2486-2497. 10.1001/jama.285.19.2486.
Lopez-Jaramillo P, Casas JP, Morillo CA: C-reactive protein and cardiovascular diseases in Andean population. Circulation. 2002, 105: E10-
Bautista LE, Lopez-Jaramillo P, Vera LM, Casas JP, Otero AP, Guaracao AI: Is C-reactive protein an independent risk factor for essential hypertension?. J Hypertens. 2001, 19: 857-861. 10.1097/00004872-200105000-00004.
Teran E, Escudero C, Moya W, Flores M, Vallance P, Lopez-Jaramillo P: Elevated C-reactive protein and pro-inflammatory cytokines in Andean women with pre-eclampsia. Int J Gynaecol Obstet. 2001, 75: 243-249. 10.1016/S0020-7292(01)00499-4.
Garcia RG, Celedón J, Sierra-Laguado J, Alarcón M, Luengas C, Silva FA, Arenas-Mantilla M, López-Jaramillo P: Raised c-reactive protein and impaired flow mediated vasodilation precede the development of preeclampsia. A. 2006, in press:
Muhlestein JB, Anderson JL, Horne BD, Lavasani F, Allen Maycock CA, Bair TL, Pearson RR, Carlquist JF: Effect of fasting glucose levels on mortality rate in patients with and without diabetes mellitus and coronary artery disease undergoing percutaneous coronary intervention. Am Heart J. 2003, 146: 351-358. 10.1016/S0002-8703(03)00235-7.
THE EXPERT COMMITTEE ON THE DIAGNOSIS AND CLASSIFICATIONS OF DIABETES MELLITUS: Follow-up Report on the Diagnosis of Diabetes Mellitus. Diabetes Care. 2003, 26: 3160-3167.
I KOWALSKA, J PROKOP, H BACHRZEWSKAGAJEWSKA, B TLEJKO, I KINALSKAL, W KOCHMAN, W MUSIAL: Disturbances of Glucose Metabolism in Men Referred for Coronary Arteriography. Postload glycemia as a predictor for coronary atherosclerosis. Diabetes Care. 2001, 24: 897-901.
Ceriello A: Impaired glucose tolerance and cardiovascular disease: the possible role of post-prandial hyperglycemia. Am Heart J. 2004, 147: 803-807. 10.1016/j.ahj.2003.11.020.
Esposito K, Giugliano D, Nappo F, Marfella R: Regression of carotid atherosclerosis by control of postprandial hyperglycemia in type 2 diabetes mellitus. Circulation. 2004, 110: 214-219. 10.1161/01.CIR.0000134501.57864.66.
F RAMIREZ, R GARCIA, F SILVA, P LOPEZJARAMILLO, C VILLAROEL: Glicemia en ayuno alterada es el factor de riesgo mas sensible de enfermedad aterosclerótica coronaria en pacientes colombianos con angina pectoris. Acta Médica Colombiana. 2004, 29: 302-311.
Warram JH, Martin BC, Krolewski AS, Soeldner JS, Kahn CR: Slow glucose removal rate and hyperinsulinemia precede the development of type II diabetes in the offspring of diabetic parents. Ann Intern Med. 1990, 113: 909-915.
Cahill GFJ: Beta-cell deficiency, insulin resistance, or both?. N Engl J Med. 1988, 318: 1268-1270.
Steinberg HO, Chaker H, Leaming R, Johnson A, Brechtel G, Baron AD: Obesity/insulin resistance is associated with endothelial dysfunction. Implications for the syndrome of insulin resistance. J Clin Invest. 1996, 97: 2601-2610.
Kuboki K, Jiang ZY, Takahara N, Ha SW, Igarashi M, Yamauchi T, Feener EP, Herbert TP, Rhodes CJ, King GL: Regulation of endothelial constitutive nitric oxide synthase gene expression in endothelial cells and in vivo : a specific vascular action of insulin. Circulation. 2000, 101: 676-681.
Accini JL, Sotomayor A, Trujillo F, Barrera JG, Bautista L, Lopez-Jaramillo P: Colombian study to assess the use of noninvasive determination of endothelium-mediated vasodilatation (CANDEV). Normal values and factors associated. Endothelium. 2001, 8: 157-166.
Silva SY, Villamizar C, Villamizar N, Silva F, Luengas C, Casas JP, Villa-Roel C, Lopez-Jaramillo P: Colombian study to assess the use of noninvasive determination of the endothelium-mediated vasodilation (CANDEV) II: does location of the occlusion device affects the accuracy of the diagnosis?. Endothelium. 2005, 12: 107-111. 10.1080/10623320500189798.
Lopez-Jaramillo P, Casas JP: Blockade of endothelial enzymes: new therapeutic targets. J Hum Hypertens. 2002, 16 Suppl 1: S100-S103. 10.1038/sj.jhh.1001353.
P LJ, JP C: Endothelial dysfunction, angiotensin-converting enzyme inhibitors and calcium antagonists. Journal of Human Hypertension. 2002, 16: 31-37.
Hanley AJ, Williams K, Stern MP, Haffner SM: Homeostasis model assessment of insulin resistance in relation to the incidence of cardiovascular disease: the San Antonio Heart Study. Diabetes Care. 2002, 25: 1177-1184.
Maachi M, Pieroni L, Bruckert E, Jardel C, Fellahi S, Hainque B, Capeau J, Bastard JP: Systemic low-grade inflammation is related to both circulating and adipose tissue TNFalpha, leptin and IL-6 levels in obese women. Int J Obes Relat Metab Disord. 2004, 28: 993-997. 10.1038/sj.ijo.0802718.
de Frutos T, de Miguel LS, Garcia-Duran M, Gonzalez-Fernandez F, Rodriguez-Feo JA, Monton M, Guerra J, Farre J, Casado S, Lopez-Farre A: NO from smooth muscle cells decreases NOS expression in endothelial cells: role of TNF-alpha. Am J Physiol. 1999, 277: H1317-H1325.
Reusch JE: Current concepts in insulin resistance, type 2 diabetes mellitus, and the metabolic syndrome. Am J Cardiol. 2002, 90: 19G-26G. 10.1016/S0002-9149(02)02555-9.
Arenas IA, Xu Y, Lopez-Jaramillo P, Davidge ST: Angiotensin II-induced MMP-2 release from endothelial cells is mediated by TNF-alpha. Am J Physiol Cell Physiol. 2004, 286: C779-C784. 10.1152/ajpcell.00398.2003.
Jones CB, Sane DC, Herrington DM: Matrix metalloproteinases: a review of their structure and role in acute coronary syndrome. Cardiovasc Res. 2003, 59: 812-823. 10.1016/S0008-6363(03)00516-9.
Engeli S, Gorzelniak K, Kreutz R, Runkel N, Distler A, Sharma AM: Co-expression of renin-angiotensin system genes in human adipose tissue. J Hypertens. 1999, 17: 555-560. 10.1097/00004872-199917040-00014.
Karlsson C, Lindell K, Ottosson M, Sjostrom L, Carlsson B, Carlsson LM: Human adipose tissue expresses angiotensinogen and enzymes required for its conversion to angiotensin II. J Clin Endocrinol Metab. 1998, 83: 3925-3929. 10.1210/jc.83.11.3925.
Giacchetti G, Faloia E, Sardu C, Camilloni MA, Mariniello B, Gatti C, Garrapa GG, Guerrieri M, Mantero F: Gene expression of angiotensinogen in adipose tissue of obese patients. Int J Obes Relat Metab Disord. 2000, 24 Suppl 2: S142-S143.
Bluher M, Kratzsch J, Paschke R: Plasma levels of tumor necrosis factor-alpha, angiotensin II, growth hormone, and IGF-I are not elevated in insulin-resistant obese individuals with impaired glucose tolerance. Diabetes Care. 2001, 24: 328-334.
Darimont C, Vassaux G, Ailhaud G, Negrel R: Differentiation of preadipose cells: paracrine role of prostacyclin upon stimulation of adipose cells by angiotensin-II. Endocrinology. 1994, 135: 2030-2036. 10.1210/en.135.5.2030.
DL C, HE H, BD S, JG K: Developmental aspects of the adipose tissue renin-angiotensin system: therapeutic implications. Drug Dev Res. 1994, 32: 117-125.-
Jones BH, Standridge MK, Moustaid N: Angiotensin II increases lipogenesis in 3T3-L1 and human adipose cells. Endocrinology. 1997, 138: 1512-1519. 10.1210/en.138.4.1512.
Shulman GI: Cellular mechanisms of insulin resistance. J Clin Invest. 2000, 106: 171-176.
Velloso LA, Folli F, Sun XJ, White MF, Saad MJ, Kahn CR: Cross-talk between the insulin and angiotensin signaling systems. Proc Natl Acad Sci U S A. 1996, 93: 12490-12495. 10.1073/pnas.93.22.12490.
Margetic S, Gazzola C, Pegg GG, Hill RA: Leptin: a review of its peripheral actions and interactions. Int J Obes Relat Metab Disord. 2002, 26: 1407-1433. 10.1038/sj.ijo.0802142.
Krauss S, Zhang CY, Scorrano L, Dalgaard LT, St Pierre J, Grey ST, Lowell BB: Superoxide-mediated activation of uncoupling protein 2 causes pancreatic beta cell dysfunction. J Clin Invest. 2003, 112: 1831-1842. 10.1172/JCI200319774.
Kim S, Urs S, Massiera F, Wortmann P, Joshi R, Heo YR, Andersen B, Kobayashi H, Teboul M, Ailhaud G, Quignard-Boulange A, Fukamizu A, Jones BH, Kim JH, Moustaid-Moussa N: Effects of high-fat diet, angiotensinogen (agt) gene inactivation, and targeted expression to adipose tissue on lipid metabolism and renal gene expression. Horm Metab Res. 2002, 34: 721-725. 10.1055/s-2002-38263.
Ran J, Hirano T, Fukui T, Saito K, Kageyama H, Okada K, Adachi M: Angiotensin II infusion decreases plasma adiponectin level via its type 1 receptor in rats: an implication for hypertension-related insulin resistance. Metabolism. 2006, 55: 478-488. 10.1016/j.metabol.2005.10.009.
Hall JE, Hildebrandt DA, Kuo J: Obesity hypertension: role of leptin and sympathetic nervous system. Am J Hypertens. 2001, 14: 103S-115S. 10.1016/S0895-7061(01)02077-5.
Clasen R, Schupp M, Foryst-Ludwig A, Sprang C, Clemenz M, Krikov M, Thone-Reineke C, Unger T, Kintscher U: PPARgamma-activating angiotensin type-1 receptor blockers induce adiponectin. Hypertension. 2005, 46: 137-143. 10.1161/01.HYP.0000168046.19884.6a.
Yamauchi T, Kamon J, Minokoshi Y, Ito Y, Waki H, Uchida S, Yamashita S, Noda M, Kita S, Ueki K, Eto K, Akanuma Y, Froguel P, Foufelle F, Ferre P, Carling D, Kimura S, Nagai R, Kahn BB, Kadowaki T: Adiponectin stimulates glucose utilization and fatty-acid oxidation by activating AMP-activated protein kinase. Nat Med. 2002, 8: 1288-1295. 10.1038/nm788.
Koh KK, Quon MJ, Han SH, Chung WJ, Lee Y, Shin EK: Anti-inflammatory and metabolic effects of candesartan in hypertensive patients. Int J Cardiol. 2006, 108: 96-100. 10.1016/j.ijcard.2005.07.040.
Togashi N, Ura N, Higashiura K, Murakami H, Shimamoto K: The contribution of skeletal muscle tumor necrosis factor-alpha to insulin resistance and hypertension in fructose-fed rats. J Hypertens. 2000, 18: 1605-1610. 10.1097/00004872-200018110-00011.
Onozato ML, Tojo A, Goto A, Fujita T, Wilcox CS: Oxidative stress and nitric oxide synthase in rat diabetic nephropathy: effects of ACEI and ARB. Kidney Int. 2002, 61: 186-194. 10.1046/j.1523-1755.2002.00123.x.
Sowers JR: Hypertension, angiotensin II, and oxidative stress. N Engl J Med. 2002, 346: 1999-2001. 10.1056/NEJMe020054.
Griendling KK, Ushio-Fukai M, Lassegue B, Alexander RW: Angiotensin II signaling in vascular smooth muscle. New concepts. Hypertension. 1997, 29: 366-373.
Vaughan DE, Lazos SA, Tong K: Angiotensin II regulates the expression of plasminogen activator inhibitor-1 in cultured endothelial cells. A potential link between the renin-angiotensin system and thrombosis. J Clin Invest. 1995, 95: 995-1001.
Hamsten A, de Faire U, Walldius G, Dahlen G, Szamosi A, Landou C, Blomback M, Wiman B: Plasminogen activator inhibitor in plasma: risk factor for recurrent myocardial infarction. Lancet. 1987, 2: 3-9. 10.1016/S0140-6736(87)93050-9.
Navarro-Cid J, Maeso R, Perez-Vizcaino F, Casal MC, Cachofeiro V, Ruilope LM, Tamargo J, Lahera V: Effects of antihypertensive drugs on blood pressure and metabolic alterations in the fructose-induced hypertensive rat. Am J Hypertens. 1996, 9: 669-674. 10.1016/0895-7061(96)00024-6.
Frossard M, Joukhadar C, Steffen G, Schmid R, Eichler HG, Muller M: Paracrine effects of angiotensin-converting-enzyme- and angiotensin-II-receptor- inhibition on transcapillary glucose transport in humans. Life Sci. 2000, 66: L147-L154. 10.1016/S0024-3205(99)00679-7.
Henriksen EJ, Jacob S: Angiotensin converting enzyme inhibitors and modulation of skeletal muscle insulin resistance. Diabetes Obes Metab. 2003, 5: 214-222. 10.1046/j.1463-1326.2003.00265.x.
Henriksen EJ, Jacob S, Kinnick TR, Teachey MK, Krekler M: Selective angiotensin II receptor receptor antagonism reduces insulin resistance in obese Zucker rats. Hypertension. 2001, 38: 884-890.
Jacob S, Henriksen EJ, Fogt DL, Dietze GJ: Effects of trandolapril and verapamil on glucose transport in insulin-resistant rat skeletal muscle. Metabolism. 1996, 45: 535-541. 10.1016/S0026-0495(96)90021-9.
Schupp M, Clemenz M, Gineste R, Witt H, Janke J, Helleboid S, Hennuyer N, Ruiz P, Unger T, Staels B, Kintscher U: Molecular Characterization of New Selective Peroxisome Proliferator-Activated Receptor {gamma} Modulators With Angiotensin Receptor Blocking Activity. Diabetes. 2005, 54: 3442-3452.
Picard F, Auwerx J: PPAR(gamma) and glucose homeostasis. Annu Rev Nutr. 2002, 22: 167-197. 10.1146/annurev.nutr.22.010402.102808.
Schupp M, Janke J, Clasen R, Unger T, Kintscher U: Angiotensin type 1 receptor blockers induce peroxisome proliferator-activated receptor-gamma activity. Circulation. 2004, 109: 2054-2057. 10.1161/01.CIR.0000127955.36250.65.
Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L, Hua T, Laragh J, McInnes GT, Mitchell L, Plat F, Schork A, Smith B, Zanchetti A: Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet. 2004, 363: 2022-2031. 10.1016/S0140-6736(04)16451-9.
Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G: Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med. 2000, 342: 145-153. 10.1056/NEJM200001203420301.
Zanchetti A, Elmfeldt D: Findings and implications of the Study on COgnition and Prognosis in the Elderly (SCOPE) - a review. Blood Press. 2006, 15: 71-79. 10.1080/08037050600771583.
Mancia G, Grassi G, Zanchetti A: New-onset diabetes and antihypertensive drugs. J Hypertens. 2006, 24: 3-10.
Dahlof B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, de Faire U, Fyhrquist F, Ibsen H, Kristiansson K, Lederballe-Pedersen O, Lindholm LH, Nieminen MS, Omvik P, Oparil S, Wedel H: Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002, 359: 995-1003. 10.1016/S0140-6736(02)08089-3.
Lindholm LH, Persson M, Alaupovic P, Carlberg B, Svensson A, Samuelsson O: Metabolic outcome during 1 year in newly detected hypertensives: results of the Antihypertensive Treatment and Lipid Profile in a North of Sweden Efficacy Evaluation (ALPINE study). J Hypertens. 2003, 21: 1563-1574. 10.1097/00004872-200308000-00022.
Yusuf S, Ostergren JB, Gerstein HC, Pfeffer MA, Swedberg K, Granger CB, Olofsson B, Probstfield J, McMurray JV: Effects of candesartan on the development of a new diagnosis of diabetes mellitus in patients with heart failure. Circulation. 2005, 112: 48-53. 10.1161/CIRCULATIONAHA.104.528166.
Hills M, Armitage P: The two-period cross-over clinical trial. Br J Clin Pharmacol. 1979, 8: 7-20.
Acknowledgements
We would like to express our gratitude to Dr Juan Carlos Mora, and Dr Anders Ljunggren from AstraZeneca, for their contributions during the protocol development, and Jean Noël Guillemot for reviewing the english style.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have received a grant from AstraZeneca to develop the present project.
Authors' contributions
PL-J who has made substantial contributions to the conception and design of the study, will be co-responsible for the overall administration and direction of the project, the analysis and interpretation of data and will give the final approval of the version to be published. VL participated in the design of the project and will be co-responsible for the overall administration and direction of the study. FS made substantial contributions to the conception and design of the study and was involved in the draft of the manuscript. LPP and CFR-C contributed to the design of the study, were involved in drafting the manuscript, will be responsible for the recruitment and the follow-up of the patients enrolled, and will also participate in the analysis and interpretation of data. GM contributed to the design of the study, will contribute to the acquisition of data, and will be responsible for overseeing the application of the protocol by monitoring the clinical trial to ensure compliance with the Good Clinical Practice guidelines. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
López-Jaramillo, P., Pradilla, L.P., Lahera, V. et al. A randomized, double blind, cross-over, placebo-controlled clinical trial to assess the effects of Candesartan on the insulin sensitivity on non diabetic, non hypertense subjects with dysglyce mia and abdominal obesity. "ARAMIA". Trials 7, 28 (2006). https://doi.org/10.1186/1745-6215-7-28
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1745-6215-7-28