
Abstract
Background
Patients with Alzheimer’s disease (AD) often present with apathy symptoms resembling the decreased motivation observed in depressed patients. Therefore, differentiating the initial phase of AD from late life depression may be difficult in some cases. Near-infrared spectroscopy (NIRS) is a functional neuroimaging modality that uses near-infrared light to measure changes in hemoglobin concentration on the cortical surface during activation tasks. The objective of this study was to investigate differences in brain activation associated with late life depression and with AD by means of NIRS.
Methods
NIRS was performed in 30 patients with depression, 28 patients with AD, and 33 healthy controls, all aged 60 years or older. During two tasks, a verbal fluency task and a visuospatial task, changes in oxygenated hemoglobin concentration in the frontal and parietal cortices were investigated.
Results
In the visuospatial task, cortical activation was lower in the depressed group than in the AD group, and significant differences were observed in the parietal cortex.
Conclusions
NIRS can detect differences in brain activation between patients with late life depression and those with AD. NIRS is a promising tool for the differential diagnosis of late life depression and AD.
Similar content being viewed by others

Background
Apathy in dementia is often difficult to distinguish from decreased motivation in depressed patients. Therefore, careful observation of the clinical course may be required to differentiate late life depression from the initial phase of Alzheimer’s disease (AD). Depression-related and age-related factors mutually affect each other. For this reason, late life depression tends to be accompanied by cognitive dysfunction and clinical symptoms are multifaceted, making diagnosis difficult. To discriminate depression from dementia, brain imaging may be a helpful addition to a detailed examination of the patient’s medical history and current findings. For this purpose, near-infrared spectroscopy (NIRS) may offer a means to aid the differential diagnosis of these conditions.
NIRS, a method for measuring brain function that was developed during the 1990s, is used to measure changes in regional cerebral blood flow (rCBF) associated with brain activation. Using near-infrared light, NIRS can detect rCBF changes as represented by increases in oxygenated hemoglobin concentration ([oxy-Hb]) and decreases in deoxygenated hemoglobin concentration ([deoxy-Hb]), which are considered to reflect cortical activity [1]. It has been reported that the results of NIRS correlate strongly with those of functional magnetic resonance imaging (fMRI) [2]. The advantage of NIRS over other functional neuroimaging techniques such as fMRI is that subjects can be examined more easily in the sitting position.
To date, several NIRS studies have compared findings in patients with AD with those in healthy controls. In AD, Herrmann et al.[3] reported a small increase in [oxy-Hb] in the prefrontal cortex during a verbal fluency task (VFT), while Arai et al.[4] reported decreased brain activation in both the frontal and parietal lobes during a VFT. In addition, Zeller et al.[5] found activation deficits in the parietal cortex during a visuospatial task. On the other hand, in NIRS studies of late life depression, Matsuo et al.[6] reported significantly less activation of the prefrontal cortex in AD, and several other studies have reported hypofrontality [7–9]. However, we are not aware of any studies that have used NIRS for a direct comparison of late life depression and AD. We believe that such a comparison is of clinical significance, and could potentially aid in the differential diagnosis of late life depression and AD.
Neuroimaging studies comparing the two conditions include a report on single photon emission tomography which revealed markedly decreased rCBF in the temporal and parietal lobes in AD, while in the frontal lobe, rCBF was markedly decreased in depression [10]. Previous fMRI studies have shown inconsistent results regarding the hemodynamic response in AD or depression, and none have directly compared the activation patterns of both conditions [11–18].
The objective of the present study was to investigate differences in brain activation between late life depression and AD by means of NIRS. We examined activation in the frontal and parietal cortices during two activation tasks, a VFT and a visuospatial task, in patients with AD or depression in comparison with healthy subjects as controls. Given that several lines of evidence suggest the involvement of executive deficits associated with frontal lobe dysfunction in the pathophysiology of depression [19, 20] and that both frontal and parietal dysfunctions are observed from the initial phase of AD [21–24], we hypothesized that activation in the parietal cortex would show a more marked decrease in patients with AD than in those with depression.
Methods
Participants
Participants were male and female patients aged 60 years or older receiving inpatient or outpatient care at the Department of Psychiatry, Shinshu University Hospital, Japan. In total, 33 patients met the Diagnostic and Statistical Manual of Mental Disorders-IV diagnostic criteria for depression and 32 other patients met that for AD. Patients who met the diagnostic criteria for both depression and AD were excluded from the study. All patients had been diagnosed by psychiatrists. In addition, 33 healthy subjects aged 60 years or over who were members of municipal physical fitness clubs, who had no history of psychiatric or neurological disease, and were no taking psychotropics were enrolled as controls (Table 1). All participants were right-handed. All patients were taking psychotropic medication. Patients with depression were treated with antidepressants (5 with amitriptyline, 1 with maprotiline, 6 with sertraline, 2 with fluvoxamine, 3 with escitalopram, 10 with duloxetine, 2 with milnacipran, 3 with mirtazapine, and 1 with mianserin), and patients with AD were treated with anti-dementia drugs (27 with donepezil, 4 with memantine, and 1 with galantamine). Head MRI was conducted for all patients, and those with findings that would affect rCBF, such as gross cerebral infarction or cerebral aneurysm, were excluded. Also excluded were patients with endocrine, metabolic, or neurological disorders.
Ethics
This study was approved by the Ethics Committee of Shinshu University School of Medicine (No. 1488), and all participants provided written informed consent. For patients with AD, written consent was also obtained from their guardians.
Clinical evaluation
All participants were assessed using the 21-item Hamilton Rating Scale for Depression (HAMD) [25], Clinical Dementia Rating (CDR) [26], Mini Mental State Examination (MMSE) [27], and Frontal Assessment Battery (FAB). The FAB assesses decreases in frontal lobe function and comprises 6 test items [28]. All tests were conducted by a single trained clinical psychotherapist.
NIRS measurements
Changes in [oxy-Hb] and [deoxy-Hb] were measured using an NIRS system (FOIRE-3000; Shimadzu Corporation, Kyoto, Japan). Absorption was measured at three wavelengths of near-infrared light (780, 805, and 830 nm), and [oxy-Hb] and [deoxy-Hb] levels were calculated according to the Lambert-Beer law based on the differences in absorption between the three wavelengths. The NIRS system can measure changes in hemoglobin concentrations at a range of approximately 2-3 cm from the surface of the skull. The distance between each pair of emission and detector probes was 3.0 cm, and the measurement area between each pair was defined as a ‘channel (CH)’. In total, 22 channels were positioned in a 6 × 12 cm area covering the frontal and parietal cortices, with CH 1-22 corresponding to the frontal cortex and CH 23-44 to the parietal cortex. The lowest probes in the frontal cortex were positioned along the Fp1-Fp2 line according to the International 10-20 system. Probes for the parietal cortex were positioned such that Pz was located at the center.
Activation tasks
The NIRS study was performed with the participants sitting relaxed in a chair and facing the screen of a desktop computer. NIRS measurement was performed using a block design. A 30-s rest period was established, followed by a 60-s task period and another 30-s rest period. This sequence was repeated 3 times in succession. Based on previous studies [5, 29], we applied the VFT and a visuospatial task (Benton Judgment of Line Orientation). The latter is a standardized test assessing the ability to recognize the angle of two lines, and it has been reported that task performance is decreased in AD [30]. A 2-3-min interval was established between the VFT and visuospatial task. During the rest period of the VFT, participants repeated the Japanese syllables “a, i, u, e, o” (corresponding to “A, B, C…” in English) as a control. During the task period, participants were asked to respond with as many words as possible beginning with the Japanese morae (syllables) “ki”, “o”, “i”, “sa”, “ta”, “a”, “ku”, “u”, and “ko”. The task was performed starting with words beginning with “ki”, and oral instructions were given every 20 s to change to words beginning with the next mora. Participants were asked to perform an active control task during the rest period so that the NIRS signal caused by vocalization could be subtracted from the NIRS signal during the task period. Task performance was scored as the number of words spoken during the VFT. In the visuospatial task, participants were asked to repeat 11 random numbers displayed on the screen during the rest period. Then, during the task period, the Benton Judgment of Line Orientation was displayed on the computer, with the next task displayed after the subject responded. Task performance was scored as the number of correct responses. While these tasks were being performed, changes in hemoglobin concentrations were measured using the 44-channel NIRS.
Data analysis
Clinical data were compared between controls, depressed patients, and patients with AD by analysis of variance (ANOVA) or the Krusksal-Wallis test for continuous variables and the Chi-squared test for categorical variables. Post hoc comparisons were performed using Tukey’s honestly significant difference test for ANOVA and the Mann-Whitney U-test for the Kruskal-Wallis test.
NIRS data with significant artifacts were excluded from the analysis. Thus, data from 30 patients with depression, 28 patients with AD, and 33 healthy controls were analyzed. Although [oxy-Hb], [deoxy-Hb], and total hemoglobin concentrations can be measured by NIRS, we concentrated on [oxy-Hb], which correlates best with changes in rCBF [31]. After averaging the results of three consecutive runs of the same task for each participant, a baseline correction was performed setting the amount of change in [oxy-Hb] at the start of the task as zero. We defined cortical activation as the difference between average [oxy-Hb] during the pre-task period and that during the task period. NIRS measurements were the product of the change in hemoglobin concentration and the optical path length; however, the optical path length differed according to measurement site. Consequently, because all channels were independent, the cortical activation in each of the 44 channels was comparatively analyzed. Since none of the cortical activation data followed a normal distribution as determined by the Shapiro-Wilk test, the data were compared between the three groups using the Kruskal-Wallis test. Post hoc comparisons between the groups were performed using the Mann-Whitney U-test. Because data were analyzed for 44 channels, the false discovery rate (FDR) was used to correct for multiple comparisons [32]. A corrected p-value of less than 0.05 was considered significant. Spearman’s rank correlation coefficient was used to analyze correlations between clinical data and the cortical activation observed in each channel, and FDR was used to correct for multiple comparisons. Stepwise logistic regression analysis was performed for patients with depression and those with AD to determine the optimal model for predicting patients with depression. Stepwise analysis was conducted as a forward stepping procedure based on a likelihood ratio test, with p < 0.05 for variable inclusion and p > 0.1 for variable exclusion from the model. The cortical activations of the 44 channels were used as potential predictor variables. Nagelkerke’s coefficient of determination was used to approximate the percent of variance explained by the model [33]. The area under the receiver operating characteristic curve (AUC) was also used to determine the predictive power of the logistic model. The predicted probability with the highest Youden index was selected as the optimal cut-off point. SPSS software (Version 20.0) was used for statistical analysis.
Results
Clinical data
MMSE and FAB scores were decreased in the order of healthy controls, patients with depression, and patients with AD, confirming a decrease in cognitive function (Table 1). MMSE and CDR scores confirmed that the patients with AD were in the initial phase of the disease. HAMD scores indicated the severity of depression was mild [34]. Task performance in both patient groups was not significantly different (p = 0.963 in the VFT and p = 0.779 in the Benton Judgment of Line Orientation). The results of head MRI showed temporal and parietal lobe atrophy in all patients with AD. No patients with depression presented notable pathological findings.
NIRS data
General cortical activation patterns
Figure 1 shows the topography of cortical activation of each group.

General cortical activation in the three participant groups. Superimposed images on 3-D MRI represent cortical activation in the verbal fluency task (a) and visuospatial task (b). Upper figures show the activation of the frontal cortex, and lower figures show the activation of the parietal cortex. The color bar indicates [oxy-Hb] (mM·cm). Note that the scale of the color bar differs between figures (a) and (b). Abbreviations: HC, healthy controls; D, depression; AD, Alzheimer’s disease; [oxy-Hb], oxygenated hemoglobin concentration.
Cortical activation in the VFT
The Kruskal-Wallis test revealed significant differences in CH 1 (p = 0.030), CH 2 (p = 0.050), CH 3 (p = 0.016), CH 12 (p = 0.029), CH 13 (p = 0.021), CH 30 (p = 0.014), CH 34 (p = 0.005), CH 35 (p = 0.001), CH 36 (p = 0.045), CH 39 (p = 0.022), and CH 43 (p = 0.031). The Mann-Whitney U-test showed significant differences only between the healthy controls and patients with depression. Cortical activation in the depressed group was decreased in comparison with healthy controls (Figure 1a). Significant differences were observed in CH3 of the frontal lobe (p = 0.043) and in CH 30 (p = 0.043), CH 34 (p = 0.041), CH 35 (p = 0.008), CH 39 (p = 0.043), and CH 43 (p = 0.043) of the right parietal lobe (p-values are FDR corrected) (Figure 2).

Comparison of VFT results between the depressed group and healthy control. Upper panels: The locations of the 44 channels on the head are indicated by yellow dots. The frontal cortex is on the left; the parietal cortex on the right. Significant differences are observed in 6 of the 44 channels indicated by red circles. Lower panels: Grand average waveforms of changes in [oxy-Hb] of CH 3 (left) and CH 34 (right) in the three groups, both of which show significant differences. Blue line, healthy controls; red line, AD group; black line, depressed group. In all three groups, during the rest period from -30 to 0 s, there are slight changes in [oxy-Hb], and during the task period from 0 to 60 s, [oxy-Hb] associated with brain activation is increased. At 60 s (when the task concluded), [oxy-Hb] is decreased. Abbreviations: D, depression; AD, Alzheimer’s disease.
Cortical activation in the visuospatial task
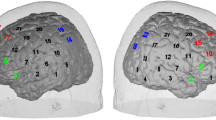
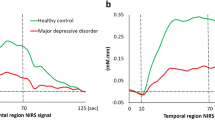
The Kruskal-Wallis test revealed significant differences in CH 15 (p = 0.033), CH 17 (p = 0.046), CH 18 (p = 0.036), CH 24 (p = 0.006), CH 25 (p = 0.006), CH 26 (p = 0.017), CH 28 (p = 0.031), CH 31 (p = 0.002), CH 32 (p = 0.011), CH 34 (p = 0.039), CH 38 (p = 0.002), and CH 41 (p = 0.042). The Mann-Whitney U-test showed significant differences only between the depressed group and the AD group, where cortical activation was relatively decreased in the depressed group (Figure 1b). Significant differences were observed in CH 24 (p = 0.037), CH 25 (p = 0.020), CH 31 (p = 0.020), CH 32 (p = 0.035), and CH 38 (p =0.014) of the parietal lobe (p-values are FDR corrected) (Figure 3).

Comparison of visuospatial task results between the depressed group and AD group. Significant differences are seen in 5 of the 44 channels indicated by red circles. The graphs show the grand average waveforms of changes in [oxy-Hb] of CH 32 and CH 38 in the three groups, 2 of the 5 channels which showed significant differences.
Correlations between cortical activation and clinical data
Cortical activation did not correlate significantly with age, task performance, or score on the MMSE, FAB, CDR, or HAMD in any of the participant groups.
Results of logistic regression analysis
The only channel with significance for predicting diagnosis during the visuospatial task was CH 38. Nagelkerke’s coefficient of determination showed a variance of 29.6% in the model. The total AUC was 0.769. The optimal cut-off point of cortical activation measured by CH 38, as determined using the Youden index, was 0.0015. The sensitivity and specificity for differentiating patients with depression from those with AD were 71.5% and 70.0%, respectively. Cortical activation during the VFT did not significantly predict diagnosis.
Discussion
The objective of this study was to investigate the differences in brain activation between late life depression and AD. The results revealed that cortical activation in a visuospatial task was significantly lower in the parietal cortex of the depressed group than in that of the AD group. Similar but non-significant tendencies were seen in the VFT. Contrary to our hypothesis, parietal activation was lower in the depressed group than in the AD group. This was due to the fact that the activation was decreased in the depressed group in both the frontal and parietal cortices, while in the AD group, cortical activation was maintained. Figure 1 shows the general cortical activation patterns of the NIRS measurement area. Differences in cortical activation between the three groups were observed across the whole measurement area, suggesting an overall decrease in [oxy-Hb] change across the whole brain in patients with depression but not in those with AD. The cortical activation of the superior parietal lobe and precuneus was significantly higher in patients with AD than in those with depression. Superior parietal lobe is associated with spatial orientation and plays a role in maintaining the internal representation of the body's state [35]. Precuneus is involved in a variety of functions including visuo-spatial imagery, episodic memory retrieval, and self-processing operations [36]. The present results may reflect the difference in these functions between patients with AD and those with depression.
Previous NIRS studies have reported decreased frontal activation in patients with depression compared with healthy controls [6, 9]. However, to our knowledge, no studies have examined the activation of the parietal cortex in patients with depression. The present study showed decreased activation in the parietal cortex, as well as in the frontal cortex. In the VFT, significant decreases were observed in the right parietal cortex in comparison with healthy controls.
On the other hand, cortical activation was maintained in the AD group. Parietal dysfunction in AD is observed from the initial phase of the disease [21–23]. As a result, parietal activation was expected to be more decreased in the AD group than in the depressed group, but we actually found that parietal activation was significantly decreased in the depressed group, despite the virtually equivalent task performance scores. Although NIRS measures changes in rCBF associated with neural activity, based on the theory of neurovascular coupling [37], we believe that changes in rCBF do not necessarily correspond to task performance and cognitive function in patients. Two fMRI studies demonstrated that the parietal region was more activated in normal individuals at high risk for AD than in low-risk individuals, although the level of task performance was identical in both groups [17, 18]. Accordingly, these studies speculated that greater cognitive effort was required by the high-risk group to achieve the same level of performance as the low-risk group. A positron emission tomography activation study showed that brain activity may increase to compensate for the declined cognitive function in patients with AD [38]. In the present study, the AD group with decreased cognitive function may have required more cognitive effort to achieve the same task performance as the depressed group, possibly resulting in relatively greater parietal activation in the AD group.
According to the compensation hypothesis [39], older adults with impaired cognitive function perform equivalently to younger adults but display overactivation in the brain cortex at a lower level of task demand; at a higher level of task demand, the brain cortex becomes underactivated and the performance becomes impaired in older adults compared with younger adults. A similar mechanism may explain the difference in the cortical activation between the AD and depressed groups. The significant differences in cortical activation during the visuospatial task between these groups may be explained by overactivation of the brain in the cognitively-impaired AD group caused by the visuospatial task, which is a low-level task. The differences in cortical activation, however, cannot be completely explained by the compensation hypothesis, because neurovascular coupling may be disrupted in patients with AD [40, 41].
Previous NIRS studies have reported that parietal activation was decreased in patients with AD compared with healthy controls [4, 5]. In the present study, however, no significant differences were observed between the two groups. Such inconsistency may be due to the differences in the type and duration of the tasks performed, as well as disease severity. Furthermore, the significant difference in age between the patients with AD and healthy controls may have influenced the results, because neurovascular coupling is also known to be altered by normal aging [41]. Vermeij et al.[42] reported that the effects of aging on the time course of the hemodynamic response in the prefrontal cortex must be taken into account when interpreting the results of neuroimaging studies.
A few points could be improved in the present study. The first is that NIRS could have been used to measure blood flow in the scalp in addition to rCBF [43–45]. The extent to which scalp blood flow is included in our data is unknown; therefore, future studies should examine systemic parameters such as heart rate, blood pressure, end-tidal CO2, skin conductance, and scalp blood flow in order to separate the effects of systemic blood flow from NIRS signals due to neural activity [44, 46]. Second, the effects of drugs cannot be ruled out. Previous studies have shown that acetylcholine-esterase inhibitors influence neurovascular coupling [47]. Other studies have reported that administration of antidepressants have influence on [oxy-Hb] changes [48–50]. However, a review of neuroimaging studies on bipolar disorder by Phillip et al.[51] reported neither significant nor ameliorative effects of psychotropic medications on abnormal structural and functional neuroimaging measures. Furthermore, several studies showed no significant correlations between cortical activation measured by NIRS and the dose of psychotropic medications [52–54]. Third, the participants in this study were not matched by age. We know that in the frontal cortex, the cortical activation patterns change with age [42, 55]. However, in our data, no significant correlations were found between age and cortical activation, and the effects due to age differences are considered to be minor. Fourth, the effect of cerebrocortical atrophy in AD cannot be ruled out. When the layer of cerebrospinal fluid thickens due to cerebral atrophy, the sensitivity of NIRS measurements decreases [56]. Fifth, the depressed group comprised patients with partially or fully remitted symptoms of depression with low HAMD scores. It remains to be elucidated whether the present findings apply during severe depressive episodes. Lastly, depression rating scales validated for use with elderly patients, such as the Geriatric Depression Scale [57], are possible alternatives to the HAMD. Further studies are required to investigate these issues.
Conclusions
NIRS revealed differences in brain activation between late life depression and AD. NIRS is a promising tool to assist in the differential diagnosis of these conditions.
Abbreviations
- AD:
-
Alzheimer’s disease
- ANOVA:
-
Analysis of variance
- AUC:
-
Area under the receiver operating curve
- CDR:
-
Clinical dementia rating
- CH:
-
Channel
- [deoxy-Hb]:
-
Deoxygenated hemoglobin concentration
- FAB:
-
Frontal assessment battery
- FDR:
-
False discovery rate
- fMRI:
-
Functional magnetic resonance imaging
- HAMD:
-
Hamilton rating scale for depression
- MMSE:
-
Mini mental state examination
- NIRS:
-
Near-infrared spectroscopy
- [oxy-Hb]:
-
Oxygenated hemoglobin concentration
- rCBF:
-
Regional cerebral blood flow
- VFT:
-
Verbal fluency task.
References
Hock C, Villringer K, Muller-Spahn F, Wenzel R, Heekeren H, Schuh-Hofer S, Hofmann M, Minoshima S, Schwaiger M, Dirnagl U, Villringer A: Decrease in parietal cerebral hemoglobin oxygenation during performance of a verbal fluency task in patients with Alzheimer’s disease monitored by means of near-infrared spectroscopy (NIRS)–correlation with simultaneous rCBF-PET measurements. Brain Res. 1997, 755: 293-303. 10.1016/S0006-8993(97)00122-4.
Cui X, Bray S, Bryant DM, Glover GH, Reiss AL: A quantitative comparison of NIRS and fMRI across multiple cognitive tasks. Neuroimage. 2011, 54: 2808-2821. 10.1016/j.neuroimage.2010.10.069.
Herrmann MJ, Langer JB, Jacob C, Ehlis AC, Fallgatter AJ: Reduced prefrontal oxygenation in Alzheimer disease during verbal fluency tasks. Am J Geriatr Psychiatry. 2008, 16: 125-135. 10.1097/JGP.0b013e3180cc1fbc.
Arai H, Takano M, Miyakawa K, Ota T, Takahashi T, Asaka H, Kawaguchi T: A quantitative near-infrared spectroscopy study: a decrease in cerebral hemoglobin oxygenation in Alzheimer’s disease and mild cognitive impairment. Brain Cogn. 2006, 61: 189-194. 10.1016/j.bandc.2005.12.012.
Zeller JB, Herrmann MJ, Ehlis AC, Polak T, Fallgatter AJ: Altered parietal brain oxygenation in Alzheimer’s disease as assessed with near-infrared spectroscopy. Am J Geriatr Psychiatry. 2010, 18: 433-441. 10.1097/JGP.0b013e3181c65821.
Matsuo K, Onodera Y, Hamamoto T, Muraki K, Kato N, Kato T: Hypofrontality and microvascular dysregulation in remitted late-onset depression assessed by functional near-infrared spectroscopy. Neuroimage. 2005, 26: 234-242. 10.1016/j.neuroimage.2005.01.024.
Onishi Y, Kikuchi S, Watanabe E, Kato S: Alterations in prefrontal cortical activity in the course of treatment for late-life depression as assessed on near-infrared spectroscopy. Psychiatry Clin Neurosci. 2008, 62: 177-184. 10.1111/j.1440-1819.2008.01752.x.
Pu S, Matsumura H, Yamada T, Ikezawa S, Mitani H, Adachi A, Nakagome K: Reduced frontopolar activation during verbal fluency task associated with poor social functioning in late-onset major depression: multi-channel near-infrared spectroscopy study. Psychiatry Clin Neurosci. 2008, 62: 728-737. 10.1111/j.1440-1819.2008.01882.x.
Matsuo K, Kato T, Fukuda M, Kato N: Alteration of hemoglobin oxygenation in the frontal region in elderly depressed patients as measured by near-infrared spectroscopy. J Neuropsychiatry Clin Neurosci. 2000, 12: 465-471. 10.1176/appi.neuropsych.12.4.465.
Hanada K, Hosono M, Kudo T, Hitomi Y, Yagyu Y, Kirime E, Komeya Y, Tsujii N, Hitomi K, Nishimura Y: Regional cerebral blood flow in the assessment of major depression and Alzheimer’s disease in the early elderly. Nucl Med Commun. 2006, 27: 535-541. 10.1097/00006231-200606000-00010.
Remy F, Mirrashed F, Campbell B, Richter W: Mental calculation impairment in Alzheimer’s disease: a functional magnetic resonance imaging study. Neurosci Lett. 2004, 358: 25-28. 10.1016/j.neulet.2003.12.122.
Prvulovic D, Hubl D, Sack AT, Melillo L, Maurer K, Frolich L, Lanfermann H, Zanella FE, Goebel R, Linden DE, Dierks T: Functional imaging of visuospatial processing in Alzheimer’s disease. Neuroimage. 2002, 17: 1403-1414. 10.1006/nimg.2002.1271.
Okada G, Okamoto Y, Morinobu S, Yamawaki S, Yokota N: Attenuated left prefrontal activation during a verbal fluency task in patients with depression. Neuropsychobiology. 2003, 47: 21-26. 10.1159/000068871.
Harvey PO, Fossati P, Pochon JB, Levy R, Lebastard G, Lehericy S, Allilaire JF, Dubois B: Cognitive control and brain resources in major depression: an fMRI study using the n-back task. Neuroimage. 2005, 26: 860-869. 10.1016/j.neuroimage.2005.02.048.
Matsuo K, Glahn DC, Peluso MA, Hatch JP, Monkul ES, Najt P, Sanches M, Zamarripa F, Li J, Lancaster JL, Fox PT, Gao JH, Soares JC: Prefrontal hyperactivation during working memory task in untreated individuals with major depressive disorder. Mol Psychiatry. 2007, 12: 158-166. 10.1038/sj.mp.4001894.
Barch DM, Sheline YI, Csernansky JG, Snyder AZ: Working memory and prefrontal cortex dysfunction: specificity to schizophrenia compared with major depression. Biol Psychiatry. 2003, 53: 376-384. 10.1016/S0006-3223(02)01674-8.
Smith CD, Andersen AH, Kryscio RJ, Schmitt FA, Kindy MS, Blonder LX, Avison MJ: Women at risk for AD show increased parietal activation during a fluency task. Neurology. 2002, 58: 1197-1202. 10.1212/WNL.58.8.1197.
Bookheimer SY, Strojwas MH, Cohen MS, Saunders AM, Pericak-Vance MA, Mazziotta JC, Small GW: Patterns of brain activation in people at risk for Alzheimer’s disease. N Engl J Med. 2000, 343: 450-456. 10.1056/NEJM200008173430701.
Alexopoulos GS: Role of executive function in late-life depression. J Clin Psychiatry. 2003, 64 (Suppl 14): 18-23.
Herrmann LL, Goodwin GM, Ebmeier KP: The cognitive neuropsychology of depression in the elderly. Psychol Med. 2007, 37: 1693-1702.
Hof PR, Vogt BA, Bouras C, Morrison JH: Atypical form of Alzheimer’s disease with prominent posterior cortical atrophy: a review of lesion distribution and circuit disconnection in cortical visual pathways. Vision Res. 1997, 37: 3609-3625. 10.1016/S0042-6989(96)00240-4.
Lineweaver TT, Salmon DP, Bondi MW, Corey-Bloom J: Differential effects of Alzheimer’s disease and Huntington’s disease on the performance of mental rotation. J Int Neuropsychol Soc. 2005, 11: 30-39.
Geldmacher DS: Visuospatial dysfunction in the neurodegenerative diseases. Front Biosci. 2003, 8: e428-e436. 10.2741/1143.
Lee DY, Choo IH, Jhoo JH, Kim KW, Youn JC, Lee DS, Kang EJ, Lee JS, Kang WJ, Woo JI: Frontal dysfunction underlies depressive syndrome in Alzheimer disease: a FDG-PET study. Am J Geriatr Psychiatry. 2006, 14: 625-628. 10.1097/01.JGP.0000214541.79965.2d.
Hamilton M: A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960, 23: 56-62. 10.1136/jnnp.23.1.56.
Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL: A new clinical scale for the staging of dementia. Br J Psychiatry. 1982, 140: 566-572. 10.1192/bjp.140.6.566.
Folstein MF, Folstein SE, McHugh PR: “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975, 12: 189-198. 10.1016/0022-3956(75)90026-6.
Dubois B, Slachevsky A, Litvan I, Pillon B: The FAB: a frontal assessment battery at bedside. Neurology. 2000, 55: 1621-1626. 10.1212/WNL.55.11.1621.
Suto T, Fukuda M, Ito M, Uehara T, Mikuni M: Multichannel near-infrared spectroscopy in depression and schizophrenia: cognitive brain activation study. Biol Psychiatry. 2004, 55: 501-511. 10.1016/j.biopsych.2003.09.008.
Ska B, Poissant A, Joanette Y: Line orientation judgment in normal elderly and subjects with dementia of Alzheimer’s type. J Clin Exp Neuropsychol. 1990, 12: 695-702. 10.1080/01688639008401012.
Hoshi Y, Kobayashi N, Tamura M: Interpretation of near-infrared spectroscopy signals: a study with a newly developed perfused rat brain model. J Appl Physiol. 2001, 90: 1657-1662.
Singh AK, Dan I: Exploring the false discovery rate in multichannel NIRS. Neuroimage. 2006, 33: 542-549. 10.1016/j.neuroimage.2006.06.047.
Nagelkerke N: A note on a general definition of the coefficient of determination. Biometrika. 1991, 78: 691-692. 10.1093/biomet/78.3.691.
Zimmerman M, Martinez JH, Young D, Chelminski I, Dalrymple K: Severity classification on the Hamilton depression rating scale. J Affect Disord. 2013, 150: 384-388. 10.1016/j.jad.2013.04.028.
Wolpert DM, Goodbody SJ, Husain M: Maintaining internal representations: the role of the human superior parietal lobe. Nat Neurosci. 1998, 1: 529-533. 10.1038/2245.
Cavanna AE, Trimble MR: The precuneus: a review of its functional anatomy and behavioural correlates. Brain. 2006, 129: 564-583. 10.1093/brain/awl004.
Fox PT, Raichle ME: Focal physiological uncoupling of cerebral blood flow and oxidative metabolism during somatosensory stimulation in human subjects. Proc Natl Acad Sci U S A. 1986, 83: 1140-1144. 10.1073/pnas.83.4.1140.
Backman L, Andersson JL, Nyberg L, Winblad B, Nordberg A, Almkvist O: Brain regions associated with episodic retrieval in normal aging and Alzheimer’s disease. Neurology. 1999, 52: 1861-1870. 10.1212/WNL.52.9.1861.
Reuter-Lorenz PA, Cappell KA: Neurocognitive aging and the compensation hypothesis. Curr Dir Psychol Sci. 2008, 17: 177-182. 10.1111/j.1467-8721.2008.00570.x.
Girouard H, Iadecola C: Neurovascular coupling in the normal brain and in hypertension, stroke, and Alzheimer disease. J Appl Physiol (1985). 2006, 100: 328-335. 10.1152/japplphysiol.00966.2005.
D’Esposito M, Deouell LY, Gazzaley A: Alterations in the BOLD fMRI signal with ageing and disease: a challenge for neuroimaging. Nat Rev Neurosci. 2003, 4: 863-872. 10.1038/nrn1246.
Vermeij A, van Beek AH, Olde Rikkert MG, Claassen JA, Kessels RP: Effects of aging on cerebral oxygenation during working-memory performance: a functional near-infrared spectroscopy study. PLoS ONE. 2012, 7: e46210-10.1371/journal.pone.0046210.
Takahashi T, Takikawa Y, Kawagoe R, Shibuya S, Iwano T, Kitazawa S: Influence of skin blood flow on near-infrared spectroscopy signals measured on the forehead during a verbal fluency task. Neuroimage. 2011, 57: 991-1002. 10.1016/j.neuroimage.2011.05.012.
Kirilina E, Jelzow A, Heine A, Niessing M, Wabnitz H, Bruhl R, Ittermann B, Jacobs AM, Tachtsidis I: The physiological origin of task-evoked systemic artefacts in functional near infrared spectroscopy. Neuroimage. 2012, 61: 70-81. 10.1016/j.neuroimage.2012.02.074.
Heinzel S, Haeussinger FB, Hahn T, Ehlis AC, Plichta MM, Fallgatter AJ: Variability of (functional) hemodynamics as measured with simultaneous fNIRS and fMRI during intertemporal choice. Neuroimage. 2013, 71: 125-134.
Vermeij A, den Abeelen AS M-v, Kessels RP, van Beek AH, Claassen JA: Very-low-frequency oscillations of cerebral hemodynamics and blood pressure are affected by aging and cognitive load. Neuroimage. 2014, 85 Pt 1: 608-615.
Rosengarten B, Paulsen S, Burr O, Kaps M: Neurovascular coupling in Alzheimer patients: effect of acetylcholine-esterase inhibitors. Neurobiol Aging. 2009, 30: 1918-1923. 10.1016/j.neurobiolaging.2008.02.017.
Kohmura K, Iwamoto K, Aleksic B, Sasada K, Kawano N, Katayama H, Noda Y, Noda A, Iidaka T, Ozaki N: Effects of sedative antidepressants on prefrontal cortex activity during verbal fluency task in healthy subjects: a near-infrared spectroscopy study. Psychopharmacology (Berl). 2013, 226: 75-81. 10.1007/s00213-012-2885-8.
Matsubara T, Matsuo K, Nakashima M, Nakano M, Harada K, Watanuki T, Egashira K, Watanabe Y: Prefrontal activation in response to emotional words in patients with bipolar disorder and major depressive disorder. Neuroimage. 2014, 85 (Pt 1): 489-497.
Noda T, Yoshida S, Matsuda T, Okamoto N, Sakamoto K, Koseki S, Numachi Y, Matsushima E, Kunugi H, Higuchi T: Frontal and right temporal activations correlate negatively with depression severity during verbal fluency task: a multi-channel near-infrared spectroscopy study. J Psychiatr Res. 2012, 46: 905-912. 10.1016/j.jpsychires.2012.04.001.
Phillips ML, Travis MJ, Fagiolini A, Kupfer DJ: Medication effects in neuroimaging studies of bipolar disorder. Am J Psychiatry. 2008, 165: 313-320. 10.1176/appi.ajp.2007.07071066.
Kameyama M, Fukuda M, Yamagishi Y, Sato T, Uehara T, Ito M, Suto T, Mikuni M: Frontal lobe function in bipolar disorder: a multichannel near-infrared spectroscopy study. Neuroimage. 2006, 29: 172-184. 10.1016/j.neuroimage.2005.07.025.
Takizawa R, Fukuda M, Kawasaki S, Kasai K, Mimura M, Pu S, Noda T, Niwa S, Okazaki Y: Neuroimaging-aided differential diagnosis of the depressive state. Neuroimage. 2014, 85 (Pt 1): 498-507.
Kinou M, Takizawa R, Marumo K, Kawasaki S, Kawakubo Y, Fukuda M, Kasai K: Differential spatiotemporal characteristics of the prefrontal hemodynamic response and their association with functional impairment in schizophrenia and major depression. Schizophr Res. 2013, 150: 459-467. 10.1016/j.schres.2013.08.026.
Sakatani K, Lichty W, Xie Y, Li S, Zuo H: Effects of aging on language-activated cerebral blood oxygenation changes of the left prefrontal cortex: near infrared spectroscopy study. J Stroke Cerebrovasc Dis. 1999, 8: 398-403. 10.1016/S1052-3057(99)80047-0.
Wang SP, Shibahara N, Kuramashi D, Okawa S, Kakuta N, Okada E, Maki A, Yamada Y: Effects of spatial variation of skull and cerebrospinal fluid layers on optical mapping of brain activities. Opt Rev. 2010, 17: 410-420. 10.1007/s10043-010-0076-6.
Montorio I, Izal M: The Geriatric depression scale: a review of its development and utility. Int Psychogeriatr. 1996, 8: 103-112.
Acknowledgments
We are grateful to Naomi Kuroiwa for assisting in laboratory investigations. We would like to thank Shimadzu Corporation for providing technical guidance on the FOIRE-3000 and for providing support for data analysis. We would also like to thank all the subjects who participated in this study. This study was funded by a research grant from the Preventive Medical Center of Shinshu University Hospital, Japan.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
HK, AR, and NA conceived and designed the experiments. HK and AR performed the experiments. HK, YK, and DS analyzed the data. NS, TO, TY, TH, SI, TT, HG, HN, TH, and SW collected the data and helped with clinical diagnosis. YK, DS, and NS helped to draft the manuscript. HK wrote the paper. All authors contributed to and have approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Kito, H., Ryokawa, A., Kinoshita, Y. et al. Comparison of alterations in cerebral hemoglobin oxygenation in late life depression and Alzheimer’s disease as assessed by near-infrared spectroscopy. Behav Brain Funct 10, 8 (2014). https://doi.org/10.1186/1744-9081-10-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1744-9081-10-8