
Abstract
Background
Few studies have focused on the association between the sociodemographic characteristics of a patient with the change in health-related quality of life (HRQOL) following invasive coronary procedures, and the results remain inconclusive. The objective of the present study was to measure the temporal changes in HRQOL of patients with coronary heart disease, and assess how these changes are associated with invasive coronary procedures and sociodemographic characteristics.
Methods
This was a prospective study of 254 patients with angina pectoris and 90 patients with acute coronary syndrome. HRQOL was assessed with the multi-item scales and summary components of the SF-36, both 6 weeks and 2 years after baseline hospitalization in 1998. Paired t-tests and multiple regression analyses were used to assess temporal changes in HRQOL and to identify the associated factors.
Results
Physical components of HRQOL had improved most during the 2 years following invasive coronary procedures. Our findings indicated that patients with angina pectoris who were younger, male, and more educated were most likely to increase their HRQOL following invasive coronary procedures. When adjusting for baseline HRQOL scores, invasive coronary procedures and sociodemographic characteristics did not explain temporal changes in patients with acute coronary syndrome, possibly due to higher comorbidity.
Conclusion
Sociodemographic characteristics should be taken into account when comparing and interpreting changes in HRQOL scores in patients with and without invasive coronary procedures.
Similar content being viewed by others


Background
In the medical treatment of patients with coronary heart disease (CHD), invasive coronary procedures – such as percutaneous coronary intervention – are effective in reducing mortality and morbidity [1, 2]. An important supplementary outcome of medical interventions and the processes of health care is health-related quality of life (HRQOL) [3, 4]. There is a strong interest in differences in the care and outcomes between sociodemographic groups to optimize population health. Differential temporal changes in HRQOL between diverse sociodemographic groups may be of interest in secondary prevention programs to maximize the benefit from treatment for CHD.
Most studies investigating the association between sociodemographic characteristics and HRQOL in patients with CHD focus on cross-sectional group comparisons [5–11]. Longitudinal studies on the association between sociodemographic characteristics and HRQOL have indicated that being female [12–14] and lower socioeconomic status [15] are associated with less temporal improvement in HRQOL. These studies, however, lacked information on medical interventions and focused on short-term changes lasting only up to 1 year. Studies assessing the effect of invasive coronary procedures on HRQOL, have shown that HRQOL improves after intervention [16–20] to levels similar to population norms [21–23]. Some of these studies were clinical trials and involved very selective populations.
Only few studies have focused on the association of sociodemographic variables with temporal changes in HRQOL following invasive coronary procedures. A recent observational study indicated that higher income is associated with greater improvement in physical HRQOL following invasive coronary procedures [24]. Improvements in physical HRQOL appear to be unrelated to the age of patients [25], whereas elderly patients exhibit a stronger improvement in mental HRQOL after medical intervention [24, 26]. However, the association of sex and educational attainment with changes in HRQOL following invasive coronary procedures remains inconclusive.
In the present study of patients with CHD, we aimed to (i) describe the effect of invasive coronary procedures on different domains of HRQOL at both 6 weeks and 2 years after baseline hospitalization, (ii) assess the association between sociodemographic characteristics and temporal changes in HRQOL.
Methods
Baseline data in the present study were derived from the Norwegian study on outcomes research and quality improvement (RESQUA), a cross-sectional postal survey of HRQOL and the experiences of patients receiving hospital care [27]. All patients from surgical and internal medicine wards at 17 hospitals (4 teaching hospitals, 6 central hospitals, and 7 local hospitals) between October and December 1998 were sent a questionnaire 6 weeks after hospital discharge. No response within 4 weeks triggered one reminder. Patients younger than 16 years and those registered as dead at discharge were excluded from the study.
Participants with CHD discharged from internal medicine wards were selected for a follow-up postal survey approximately 2 years later, in October and November 2000. We used information on primary and secondary diagnoses from the patient-administration systems of the hospitals, and included patients with acute coronary syndrome (ICD-9 410.xx and 411.xx) and angina pectoris (ICD-9 413.xx). Patients with chronic heart failure (ICD-9 428.xx) as the primary diagnosis were classified as angina pectoris or acute coronary syndrome dependent on their secondary diagnoses.
Measures
Health-related quality of life
HRQOL was measured by the Norwegian version 1.2 of the Short-Form 36 (SF-36), a widely used generic health status measure that enables comparison with normative scores [28, 29]. The scales and items of the SF-36 have satisfactory reliability, validity, and responsiveness, also in patients with CHD [3, 10, 30, 31]. Single items of the SF-36 are transformed and aggregated into eight multi-item scales: Physical Functioning, Physical Role Limitations, Bodily Pain, General Health Perceptions, Vitality, Social Functioning, Emotional Role Limitations, and Mental Health. The resulting summated rating scales range from 0 to 100, with higher scores indicating better health.
To estimate the potential impact of CHD on HRQOL, we compared the SF-36 scores from the patients in our study with normative data from the Norwegian general population [32]. Norm scores for the eight multi-item scales were adjusted to reflect age and sex distributions similar to those of the patients in the present study. These adjusted norm data for the eight multi-item scales were used to calculate the standardized Physical (PCS) and Mental (MCS) Component Summary scores [33].
Procedures, sociodemographics, and comorbidity
Invasive coronary procedures referred to diagnostic and therapeutic procedures, such as coronary angiography, which contributes to diagnosis of potential coronary artery disease, and when followed by angioplasty, it can contribute to a relief from chest-pain as well as improve the prognosis in high-risk patients. Procedure codes were derived from the patient-administration systems of the hospitals in 1998 (Classification of Operations; version 3, 1995). We defined invasive coronary procedures as a dichotomous variable, differentiating between patients with and without invasive coronary procedures during baseline hospitalization in 1998. The age and sex data were also derived from the administration systems in 1998. Information about the highest level of educational attainment was obtained from self-reported data in the 1998 postal survey. This variable was heavily positively skewed, and we therefore created two groups: (1) below and equal to, and (2) above the median value in our cohort. As a crude estimate of the degree of comorbidity for each patient, we used the total number of secondary diagnoses registered in the administration databases during baseline hospitalization in 1998.
Statistical analyses
Changes in HRQOL were only assessed in patients who had valid scores on all multi-item scales both in 1998 and 2000. We used χ2-statistics or the t-test for independent samples to analyze the extent of selective attrition, and differences in the use of invasive coronary procedures across characteristics of respondents.
Temporal changes in HRQOL were analyzed with paired-samples t-tests. As a measure of the minimally important difference in intra-individual scores, we calculated the standardized response mean, a distribution-based approach that compares temporal change by the standard deviation of change [34]. Standardized response means of 0.2–0.5, 0.5–0.8, and > 0.80 are regarded as small, moderate, and large, respectively [35].
Additionally, we applied multivariate linear regression analyses to determine the association of invasive coronary procedures and sociodemographic factors with PCS and MCS scores 2 years after baseline hospitalization. By including baseline PCS and MCS scores in the regression model, the regression coefficients of invasive coronary procedures and sociodemographic factors indicate the one unit increase in 2-year PCS and MCS scores, provided that baseline scores are held constant.
All analyses were performed separately in patients with angina pectoris and acute coronary syndrome. We chose a 5% statistical significance level. The Regional Medical Research Ethics Committee, the Data Inspectorate, and the Norwegian Board of Health approved the study.
Results
A total of 1,534 patients with CHD were sent a questionnaire in 1998, and 1,059 (69%) responded. In 2000, 700 patients with valid HRQOL scores were sent a follow-up questionnaire (and, where necessary, one reminder), and 473 patients responded. After excluding 38 patients who had recently died and 9 patients with an unknown address, the adjusted response rate in the follow-up study was 72% (Figure 1).

Flow chart describing attrition in the cohort of patients with coronary heart disease
A total of 254 patients with angina pectoris and 90 patients with acute coronary syndrome had valid MCS and PCS scores both in 1998 and 2000, of which 108 patients with angina pectoris and 41 patients with acute coronary syndrome underwent an invasive coronary procedure. The majority underwent catheterization (N = 79) or percutaneous coronary intervention (N = 45). Twenty-one patients underwent coronary bypass surgery and the remaining patients (N = 4) underwent other medical procedures related to the cardiovascular system. Compared to the original cohort of patients, patients with valid HRQOL scores both in 1998 and 2000, more often had undergone invasive coronary procedures, were male, younger, and had lower comorbidity (Table 1). Compared to the cohort with valid responses in 1998, attrition was associated with age, educational attainment and comorbidity. Angina pectoris patients who responded both in 1998 and in 2000 had higher PCS scores in 1998 compared to nonrespondents to the follow-up survey (mean HRQOL score 42 versus 39; P < 0.001). Among patients with valid HRQOL scores both in 1998 and 2000, women, elderly patients, and patients with higher comorbidity had fewer invasive coronary procedures during the baseline hospitalization (Table 2). Educational attainment was not associated with invasive coronary procedures.
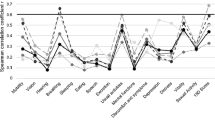
Six weeks after hospitalization, patients with angina pectoris and acute coronary syndrome had lower scores compared to the Norwegian norm data in all domains of HRQOL (Table 3 [see Additional file 1]). Patients without invasive coronary procedures exhibited the largest differences, particularly in domains referring to physical aspects of HRQOL: Physical Role Limitations, Emotional Role Limitations, and Bodily Pain; but also in General Health Perceptions. Two years after the baseline hospitalization in 1998, scores on all multi-item scales were still below the scores of the norm population.
Over the 2 years analyzed, Physical Role Limitations (P = 0.001) and Social Functioning (P = 0.003) improved in angina pectoris patients without invasive coronary procedures, corresponding to a small effect size (Table 3). Physical Functioning (P = 0.03), Physical Role Limitations (P < 0.001), and Bodily Pain (P = 0.03) improved in patients with angina pectoris undergoing invasive coronary procedures. The change in Physical Role Limitations corresponded to a moderate effect size. A significant deterioration was found in General Health Perceptions (P = 0.04).
In patients with acute coronary syndrome without invasive coronary procedures, Physical Role Limitations (P = 0.003), Social Functioning (P = 0.005), and Emotional Role Limitations (P = 0.009) significantly improved. Physical Role Limitations (P = 0.001) improved in patients with acute coronary syndrome undergoing invasive coronary procedures.
Patients with invasive coronary procedures showed a small improvement in PCS scores (P = 0.034 for angina pectoris and P = 0.015 for patients with acute coronary syndrome). MCS scores remained stable during the 2 years of follow-up; only patients with angina pectoris without an invasive coronary procedure experienced a small improvement in MCS scores (P = 0.007).
Multiple linear regression analyses revealed that, after taking baseline PCS scores into account, invasive coronary procedures and being younger, male, and more educated were significantly associated with higher PCS scores in 2000 in patients with angina pectoris (Table 4 [see Additional file 2]). For these patients, being older was significantly associated with higher MCS scores in 2000. In patients with acute coronary syndrome, PCS scores and MCS scores in 2000 were significantly associated only with baseline scores, and not with invasive coronary procedures or sociodemographic characteristics.
Discussion
In the present study, most improvement was found in the physical components of HRQOL 2 years following invasive coronary procedures. These results support the findings of Krumholz et. al. [21] that the SF-36 scale for Physical Role Limitations was most responsive after elective coronary angioplasty. Furthermore, in patients with angina pectoris, PCS scores improved more among those who were male, younger, and more educated, independently of invasive coronary procedures. One explanation for this, as suggested by some previous studies, is related to differences in disease severity: women and patients from disadvantaged socioeconomic strata may have more extensive coronary disease at the onset of symptoms [12, 13, 36]. Additionally, undesirable events and adverse experiences might have stronger negative emotional consequences in this group [37], suggesting worse adaptation to the long-lasting physical limitations of CHD and a greater risk of recurrent events [36].
When adjusting for baseline scores, invasive coronary procedures and sociodemographic characteristics did not explain any additional variation in PCS and MCS scores 2 years after hospitalization in patients with acute coronary syndrome. This may be due to the relatively small sample size. An alternative explanation is that patients with acute coronary syndrome exhibited higher comorbidity that could limit the effect of invasive coronary procedures on HRQOL, and accordingly, the sensitivity of the SF-36 in detecting differences [20].
Our results demonstrated that invasive coronary procedures and sociodemographic characteristics were weakly associated with MCS scores and indicated small deviations from the population norm, which corresponds to previous findings in patients with CHD [6, 38]. This may be attributable to health care having less impact on mental health than on physical health. An alternative explanation refers to the construction of the SF-36 MCS and PCS measures. The scores of these component scales are calculated using all eight multi-item scales with factor score coefficients derived from factor analysis with orthogonal rotation, thereby defining that PCS and MCS are uncorrelated. Mean scores on the multi-item scales that are below the population mean will contribute to component scores opposite to the direction defined by the factor score coefficient [39]. In our study, the low scores of Physical Role Limitations contributed negatively to PCS and positively to MCS. Hence, MCS scores were probably inflated by poor physical health. The RAND-36 has been suggested as an alternative method for computing PCS and MCS scores that avoids the orthogonal approach of the SF-36 [40, 41].
Other factors may have influenced our results, for example selective attrition. In our study, the respondents to both surveys represent a survivor cohort, and hence attrition may have reduced the temporal changes in SF-36 scores and possibly lead to underestimation of the associations with invasive coronary procedures and sociodemographic factors. Moreover, the use of self-administered and postal questionnaires may have contributed to missing SF-36 items, especially in elderly subjects who are associated with a higher frequency of missing values for items used to score physical and emotional role functioning [24]. The appropriateness of the SF-36 for use in elderly populations with expected low response rates, reduced cognitive functioning, and shifts in conceptualizations of subjective health, has been discussed previously [32]. Consequently, caution should be exercised when employing norms among people aged 70 years and older.
Another limitation of our study is the lack of HRQOL data before the baseline hospitalization in 1998, which prevented us from assessing the full impact of invasive coronary procedures on subsequent HRQOL and its association with sociodemographic characteristics. We also did not examine the influence of use of medical services after the baseline hospitalization. Finally, coronary patients and invasive procedures were defined by registry data from the patient-administration systems of hospitals, which might be inaccurate and mask some of the underlying clinical differences that could influence the HRQOL results.
Our findings indicated that patients with angina pectoris who were younger, male, and more educated were most likely to increase their HRQOL following invasive coronary procedures. In patients hospitalized for acute coronary syndrome, temporal change in HRQOL was not associated with invasive coronary procedures and sociodemographic characteristics, possibly due to higher comorbidity. In a usual care setting the occurrence of invasive coronary procedures varies with sociodemographic characteristics [42, 43]. The association of both sociodemographic variables and invasive coronary procedures with HRQOL outcomes makes it imperative to take these into account when comparing and interpreting change scores to reduce the risk of spurious findings.
References
Blumenthal RS, Cohn G, Schulman SP: Medical therapy versus coronary angioplasty in stable coronary artery disease: a critical review of the literature. J Am Coll Cardiol 2000, 36: 668–673. 10.1016/S0735-1097(00)00791-9
Parisi AF, Folland ED, Hartigan P: A comparison of angioplasty with medical therapy in the treatment of single-vessel coronary artery disease. Veterans Affairs ACME Investigators. N Engl J Med 1992, 326: 10–16.
Thompson DR, Yu CM: Quality of life in patients with coronary heart disease-I: Assessment tools. Health Qual Life Outcomes 2003, 1: 42. 10.1186/1477-7525-1-42
Testa MA, Simonson DC: Assesment of quality-of-life outcomes. N Engl J Med 1996, 334: 835–840. 10.1056/NEJM199603283341306
Heller RF, Lim L, Valenti L, Knapp J: Predictors of quality of life after hospital admission for heart attack or angina. Int J Cardiol 1997, 59: 161–166. 10.1016/S0167-5273(97)02946-X
Juenger J, Schellberg D, Kraemer S, Haunstetter A, Zugck C, Herzog W, Haass M: Health related quality of life in patients with congestive heart failure: comparison with other chronic diseases and relation to functional variables. Heart 2002, 87: 235–241. 10.1136/heart.87.3.235
Rumsfeld JS, Magid DJ, Plomondon ME, O'Brien MM, Spertus JA, Every NR, Sales AE: Predictors of quality of life following acute coronary syndromes. Am J Cardiol 2001, 88: 781–784. 10.1016/S0002-9149(01)01852-5
Beck CA, Joseph L, Belisle P, Pilote L: Predictors of quality of life 6 months and 1 year after acute myocardial infarction. Am Heart J 2001, 142: 271–279. 10.1067/mhj.2001.116758
Stavem K, Lossius MI, Kvien TK, Guldvog B: The health-related quality of life of patients with epilepsy compared with angina pectoris, rheumatoid arthritis, asthma and chronic obstructive pulmonary disease. Qual Life Res 2000, 9: 865–871. 10.1023/A:1008993821253
Brown N, Melville M, Gray D, Young T, Munro J, Skene AM, Hampton JR: Quality of life four years after acute myocardial infarction: short form 36 scores compared with a normal population. Heart 1999, 81: 352–358.
Norris CM, Ghali WA, Galbraith PD, Graham MM, Jensen LA, Knudtson ML: Women with coronary artery disease report worse health-related quality of life outcomes compared to men. Health Qual Life Outcomes 2004, 2: 21. 10.1186/1477-7525-2-21
Brezinka V, Kittel F: Psychosocial factors of coronary heart disease in women: a review. Soc Sci Med 1996, 42: 1351–1365. 10.1016/0277-9536(95)00284-7
van Jaarsveld CH, Sanderman R, Ranchor AV, Ormel J, van Veldhuisen DJ, Kempen GI: Gender-specific changes in quality of life following cardiovascular disease: a prospective study. J Clin Epidemiol 2002, 55: 1105–1112. 10.1016/S0895-4356(02)00506-1
Chin MH, Goldman L: Gender differences in 1-year survival and quality of life among patients admitted with congestive heart failure. Med Care 1998, 36: 1033–1046. 10.1097/00005650-199807000-00010
Lacey EA, Walters SJ: Continuing inequality: gender and social class influences on self perceived health after a heart attack. J Epidemiol Community Health 2003, 57: 622–627. 10.1136/jech.57.8.622
Nash IS, Curtis LH, Rubin H: Predictors of patient-reported physical and mental health 6 months after percutaneous coronary revascularization. Am Heart J 1999, 138: 422–429.
Cleary PD, Epstein AM, Oster G, Morrissey GS, Stason WB, Debussey S, Plachetka J, Zimmerman M: Health-related quality of life among patients undergoing percutaneous transluminal coronary angioplasty. Med Care 1991, 29: 939–950.
Five-year clinical and functional outcome comparing bypass surgery and angioplasty in patients with multivessel coronary disease. A multicenter randomized trial. Writing Group for the Bypass Angioplasty Revascularization Investigation (BARI) Investigators JAMA 1997, 277: 715–721.
Pocock Stuart J., Henderson Robert A., Seed Paul, Treasure Tom, Hampton John R.: Quality of Life, Employment Status, and Anginal Symptoms After Coronary Angioplasty or Bypass Surgery: 3-Year Follow-up in the Randomized Intervention Treatment of Angina (RITA) Trial. Circulation 1996, 94: 135–142.
Spertus JA, Winder JA, Dewhurst TA, Deyo RA, Fihn SD: Monitoring the quality of life in patients with coronary artery disease. Am J Cardiol 1994, 74: 1240–1244. 10.1016/0002-9149(94)90555-X
Krumholz HM, McHorney CA, Clark L, Levesque M, Baim DS, Goldman L: Changes in health after elective percutaneous coronary revascularization. A comparison of generic and specific measures. Med Care 1996, 34: 754–759. 10.1097/00005650-199608000-00003
Brorsson B, Bernstein SJ, Brook RH, Werko L: Quality of life of patients with chronic stable angina before and four years after coronary revascularisation compared with a normal population. Heart 2002, 87: 140–145. 10.1136/heart.87.2.140
Wahrborg P: Quality of life after coronary angioplasty or bypass surgery. 1-year follow-up in the Coronary Angioplasty versus Bypass Revascularization investigation (CABRI) trial. Eur Heart J 1999, 20: 653–658. 10.1053/euhj.1998.1237
Müller-Nordhorn J, Kulig M, Binting S, Völler H, Gohlke H, Linde K, Willich SN: Change in quality of life in the year following cardiac rehabilitation. Quality of Life Research 2004, 13: 399–410. 10.1023/B:QURE.0000018473.55508.6a
Seto TB, Taira DA, Berezin R, Chauhan MS, Cutlip DE, Ho KK, Kuntz RE, Cohen DJ: Percutaneous coronary revascularization in elderly patients: impact on functional status and quality of life. Ann Intern Med 2000, 132: 955–958.
Pasquali SK, Alexander KP, Peterson ED: Cardiac rehabilitation in the elderly. Am Heart J 2001, 142: 748–755. 10.1067/mhj.2001.119134
Pettersen KI: Assessing outcomes in Norwegian Hospitals - the Norwegian Outcomes study. Quality of Life Newsletter 1997, 2–2.
Keller SD, Ware J.E.,Jr, Bentler PM, Aaronson NK, Alonso J, Apolone G, Bjorner JB, Brazier J, Bullinger M, Kaasa S, Leplege A, Sullivan M, Gandek B: Use of structural equation modeling to test the construct validity of the SF-36 Health Survey in ten countries: results from the IQOLA Project. International Quality of Life Assessment. J Clin Epidemiol 1998, 51: 1179–1188. 10.1016/S0895-4356(98)00110-3
Loge JH, Kaasa S, Hjermstad MJ, Kvien TK: Translation and performance of the Norwegian SF-36 Health Survey in patients with rheumatoid arthritis. I. Data quality, scaling assumptions, reliability, and construct validity. J Clin Epidemiol 1998, 51: 1069–1076. 10.1016/S0895-4356(98)00098-5
McHorney CA, Ware J.E.,Jr., Lu JF, Sherbourne CD: The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care 1994, 32: 40–66.
Failde I, Ramos I: Validity and reliability of the SF-36 Health Survey Questionnaire in patients with coronary artery disease. J Clin Epidemiol 2000, 53: 359–365. 10.1016/S0895-4356(99)00175-4
Loge JH, Kaasa S: Short Form 36 (SF-36) health survey: normative data from the general Norwegian population. Scand J Soc Med 1998, 26: 250–258.
Ware J.E.,Jr, Kosinski M, Keller SD: SF-36 Physical & Mental Health Summary Scales: A user's manual. Boston, Massachusetts; 1994.
Staquet MJ, Hays RD, Fayers PM: Quality of Life Assessment in Clinical Trials: Methods and Practice. Oxford, Oxford University Press; 1998.
Cohen J: Statistical power analysis for the behavioral sciences. 2nd edition. New York, Academic Press; 1988.
Alter DA, Naylor CD, Austin P, Tu JV: Effects of socioeconomic status on access to invasive cardiac procedures and on mortality after acute myocardial infarction. N Engl J Med 1999, 341: 1359–1367. 10.1056/NEJM199910283411806
McLeod JD, Kessler RC: Socioeconomic status differences in vulnerability to undesirable life events. J Health Soc Behav 1990, 31: 162–172.
Sprangers MA, de Regt EB, Andries F, van Agt HM, Bijl RV, de Boer JB, Foets M, Hoeymans N, Jacobs AE, Kempen GI, Miedema HS, Tijhuis MA, de Haes HC: Which chronic conditions are associated with better or poorer quality of life? J Clin Epidemiol 2000, 53: 895–907. 10.1016/S0895-4356(00)00204-3
Taft C, Karlsson J, Sullivan M: Do SF-36 summary component scores accurately summarize subscale scores? Qual Life Res 2001, 10: 395–404. 10.1023/A:1012552211996
Hays RD, Morales LS: The RAND-36 measure of health-related quality of life. Ann Med 2001, 33: 350–357.
Cunningham WE, Nakazono TT, Tsai KL, Hays RD: Do differences in methods for constructing SF-36 physical and mental health summary measures change their associations with chronic medical conditions and utilization? Qual Life Res 2003, 12: 1029–1035. 10.1023/A:1026191016380
Bond M, Bowling A, McKee D, Kennelly M, Banning AP, Dudley N, Elder A, Martin A: Does ageism affect the management of ischaemic heart disease? J Health Serv Res Policy 2003, 8: 40–47. 10.1258/13558190360468218
Roger VL, Farkouh ME, Weston SA, Reeder GS, Jacobsen SJ, Zinsmeister AR, Yawn BP, Kopecky SL, Gabriel SE: Sex differences in evaluation and outcome of unstable angina. JAMA 2000, 283: 646–652. 10.1001/jama.283.5.646
Acknowledgement
This study was supported by grants from the Ministry of Health and the Research Council of Norway. We thank Tomislav Dimoski for developing software for quality assurance and patient selection.
Author information
Authors and Affiliations
Corresponding author
Additional information
Authors' contributions
MV carried out the follow-up study, analyzed the data, and drafted the manuscript. KIP performed the baseline survey. AR participated in the design of the study. KS participated in the design and coordination of the study. All authors read and approved the final manuscript.
Electronic supplementary material
12955_2004_137_MOESM1_ESM.xls
Additional File 1: Table 3: SF-36 multi-item and summary scales 6 weeks and 2 years after baseline hospitalization in patients with angina pectoris and acute coronary syndrome according to invasive coronary procedures (ICP). Norwegian norm data and 2-year change scores (XLS 20 KB)
12955_2004_137_MOESM2_ESM.xls
Additional File 2: Table 4 Predictors of Physical Component Summary (PCS) and Mental Component Summary (MCS) scores 2 years following the baseline hospitalization in patients with angina pectoris and acute coronary syndrome. Multivariate linear regression analysis; unstandardized regression coefficients (B) and 95% Confidence Intervals (CI) (XLS 16 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Veenstra, M., Pettersen, K.I., Rollag, A. et al. Association of changes in health-related quality of life in coronary heart disease with coronary procedures and sociodemographic characteristics. Health Qual Life Outcomes 2, 56 (2004). https://doi.org/10.1186/1477-7525-2-56
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7525-2-56