
Abstract
Background
Antibiotics overuse is a global public health issue influenced by several factors, of which some are parent-related psychosocial factors that can only be measured using valid and reliable psychosocial measurement instruments. The PAPA scale was developed to measure these factors and the content validity of this instrument was assessed.
Aim
This study further validated the recently developed instrument in terms of (1) face validity and (2) construct validity including: deciding the number and nature of factors, and item selection.
Methods
Questionnaires were self-administered to parents of children between the ages of 0 and 12 years old. Parents were conveniently recruited from schools’ parental meetings in the Eastern Province, Saudi Arabia. Face validity was assessed with regards to questionnaire clarity and unambiguity. Construct validity and item selection processes were conducted using Exploratory factor analysis.
Results
Parallel analysis and Exploratory factor analysis using principal axis factoring produced six factors in the developed instrument: knowledge and beliefs, behaviours, sources of information, adherence, awareness about antibiotics resistance, and parents’ perception regarding doctors’ prescribing behaviours. Reliability was assessed (Cronbach’s alpha = 0.78) which demonstrates the instrument as being reliable.
Conclusion
The ‘factors’ produced in this study coincide with the constructs contextually identified in the development phase of other instruments used to study antibiotic use. However, no other study considering perceptions of antibiotic use had gone beyond content validation of such instruments. This study is the first to constructively validate the factors underlying perceptions regarding antibiotic use in any population and in parents in particular.
Similar content being viewed by others

Introduction
Although antibiotics are targeted to kill or inhibit the growth of bacteria and have no effect on viral agents [1], they are often inappropriately used to treat viral infections such as upper respiratory tract infections (URTIs). URTIs are usually self-limiting and resolve in the same amount of time regardless of antibiotic consumption [2]. Thus, using antibiotics to treat these viral infections is considered misuse or overuse of antibiotics. This misuse/overuse is common in children [3, 4], and is currently considered to be one of the major worldwide public health issues [5–7].
Antibiotics misuse/overuse may cause several problems, for instance: development of antibacterial resistance [8, 9], increasing the burden of chronic diseases and rising costs of health services [10], and the development of side effects (e.g. adverse gastrointestinal effects) [11].These adverse effects are more significant in children according to Simasek [12].
This misuse may be due to reasons related to: patients, parents or guardians, or the medical practitioner. Several studies have discussed the reasons associated with antibiotics overuse. These include: attitudes, beliefs, knowledge of antibiotic use [13–15], behaviours (e.g. over-the-counter medication and self-medication) [5, 16, 17], patients’ perceptions regarding patient-doctor interaction, patient satisfaction, and patients’ experience with antibiotics [15, 18]. These studies have provided a framework for the development of the Parental Perception on Antibiotics Scale –‘The PAPA Scale’ [19].
The behaviours associated with the overuse of antibiotics may include antibiotics self-medication and over-the-counter medication. These behaviours specifically are considered a public health issue in many middle-east countries that are similar to Saudi Arabia, geographically and culturally [13, 16, 17, 20]. However, information regarding trends in antibiotic consumption in Saudi Arabia is very limited. Moreover, there are no reports on parents’ behaviours regarding antibiotics use among Saudi children, especially those with upper respiratory tract infections (URTIs) [21]. As a result, it is important to measure this psychosocial phenomenon in Saudi Arabia.
In order to measure such psychosocial phenomena, a valid and reliable measurement instrument needs to be available [22]. Assessing the validity of an instrument involves confirming the instrument’s capability of measuring what it is intended to measure [23]. However, an extensive literature review has not revealed any validated instrument worldwide that measures the factors influencing antibiotics overuse in children with URTIs [24]. This study aims to validate a developed and content-validated instrument [19]; further validation includes construct validity of the instrument using factor analysis, which will determine the number and nature of the underlying construct in the developed instrument.
Methods
This was a cross-sectional study design using a preliminary-validated questionnaire [19]. The required ethical approvals were obtained from Queensland University of Technology (ethical approval number: 1200000022) and the Ministry of Education in the Eastern Province in Saudi Arabia (ethical approval number: 33505889). The questionnaire was distributed to parents of children (younger than 12 years old) in primary schools in the Eastern Province of Saudi Arabia between March to April 2012. Participants’ consent was implied by the return of the completed questionnaire.
Only questionnaires completed by one of the parents or a legal guardian were included in the study. One questionnaire was excluded because it was completed by a sibling who was less than 18 years old.
Instrument development
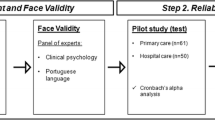
The PAPA scale was developed to assess parental perceptions regarding antibiotics. This scale aims to assess the factors influencing parents to use antibiotics for their children, especially in relation to upper respiratory tract infections. A content evaluation panel was developed to assess the content and face validity of the instrument by building a group brainstorming process [25]. The scale items were firstly derived from relevant literature in the field. This was followed by a three-round Delphi process conducted using a panel of experts knowledgeable in such areas as pediatrics, infectious diseases, epidemiology, family medicine, psychology and counseling, and social sciences. The report of this study has been published elsewhere [19].
Experts were provided with a pool of 80 questions retrieved from the relevant literature [18, 26–29]. They were asked to choose the most relevant questions to measure the study objectives; i.e. factors influencing the overuse of antibiotics in children with URTIs in Saudi Arabia for the first round. Experts were also invited to generate ideas in this round [30]. The included questions from the first round were then sent again to the same panel members with the percentage of agreement for each item [31]. In this second round, experts were asked to agree, disagree, and/or comment on the items. The third and last round was sent to the experts to obtain their final confirmation on the instrument. The development process involved face validity as well as content validation. Face validity was conducted by asking the experts to comment on the clarity and flow of the questions in the proposed questionnaire.
A 58-question content-validated survey was developed to conduct this study [19]. The first part of the questionnaire, which is not the focus of this study, dealt with parental demographics and children’s health-related history. The second part consisted of questions about the factors associated with antibiotics use, e.g. parental knowledge, behaviours, attitudes and beliefs about antibiotics use for children younger than 12 years of age. The last part was to assess the face validity of the questionnaire. All questions relating to antibiotics use were measured on a five-point Likert scale. Questions to assess the face validity of the questionnaire were on Binary scale (yes/no).
Statistical analysis
Personal characteristics were summarised using frequencies and percentages. The association of antibiotics use per year with the frequency of common cold episodes per year was assessed using cross tabulation.
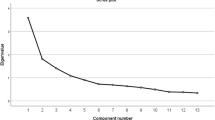
Parallel analysis based on Principal Components Analysis was conducted; scree plots and Kaiser Criteria (Eigen value > 1) were used along a theoretical basis for choosing the number of factors. As this is a multivariate analysis, missing values were excluded listwise from the list.
Following the parallel analysis, Principal axis factoring was used to determine the nature of the underlying factors [25]. Both an orthogonal (Varimax) and an oblique (Promax) rotation were performed on the factor solution to determine which type of rotation was most suitable. The internal consistency of the instrument (i.e. reliability) was measured using Cronbach’s alpha.
All data analysis was conducted using the Statistics Package for Social Sciences (SPSS v19) with the exception of the parallel analysis, which used the nFactor library (v2.3.3) within the R statistics package (v2.14.2).
Results
The questionnaires were completed by 238 parents (25% response rate). Mothers were more responsive than fathers; 70 percent of the parents in the study are mothers. Parents’ personal characteristics are summarised in Table 1. Some demographic differences were noticeable between mothers and fathers in the sample. With regard to age, the average age category of mothers in the study appears to be 31-40 years old (52%), while fathers tend to fall within the age category of 41-50 years old (44%). Most mothers and fathers are employed (56% and 79% consecutively), and third of mothers are housewives (34%). Moreover, illiteracy is more observable in mothers (2%), while all fathers in the study are literate. The majority of mothers and fathers have a diploma or a bachelor degree (76% and 55% consecutively). However, only 2 percent of mothers have higher degrees, compared to 26 percent of fathers.
Parents were asked to assess their child’s health-related history in relation to the number of common cold episodes per year and the number of antibiotic use per year (see Table 2). According to the parents, 13 (5.5%) children in the study had a serious infectious disease in the past including chicken pox and unidentified respiratory infections. Thirty-two (13.4%) children had chronic diseases such as heart disease, diabetes, asthma, and allergies.
Parallel analysis was performed to decide on the number of factors to retain in the Parental Perception on Antibiotics Scale (PAPA Scale). Based on a 10,000-permutations parallel analysis, a six-factor solution was produced (Figure 1).

Parallel Analysis derived from a principal component analysis.
According to the parallel analysis, a six-factor solution was used. The coefficients in the pattern matrix in Table 3 show the number and nature of factors in the PAPA Scale using Exploratory factor analysis. The produced factors include: Factor 1: knowledge and beliefs (10 items), Factor 2: behaviours (6 items), Factor 3: sources of information (7 items), Factor 4: adherence (5 items), Factor 5: awareness about antibiotics resistance (5 items), and Factor 6: parents’ perception on doctors’ prescribing behaviours (3 items). In addition, the inter-factor correlation matrix shown in Table 4 suggests that at least some of the factors are moderately correlated indicating that an oblique measurement model is justified.
By assessing the Instrument’s reliability it was found that the total and sub-scales were demonstrated as being reliable with the overall Cronbach’s alpha = 0.87, and the individual subscales Cronbach’s alphas ranging from 0.771 to 0.794.
Discussion
After conducting parallel analysis and factor analysis to the newly developed and content validated measurement instrument, the following factors emerged from the analysis: knowledge and beliefs, behaviours, sources of information, adherence, awareness about antibiotics resistance, and parents’ perception on doctors’ prescribing behaviours.
The influencing factors on the overuse of antibiotics include psychosocial factors such as attitudes and beliefs; knowledge-related factors that may lead to unwanted behaviours such as parents’ pressure and inappropriate use of antibiotics; and demographic factors including education levels, socioeconomic status, and employment.
The constructs measured in the literature in the field of antibiotics use include: attitudes, beliefs, knowledge (including experience with antibiotics), and behaviours (over-the-counter medication and self-medication) [5, 13, 16, 17, 20, 32–35]. Other factors are measured within these major dimensions including: patient expectations and adherence to antibiotics, patients’ perceptions regarding patient-doctor interaction, and patient satisfaction [15, 18, 36, 37]. Demographic characteristics were also measured in the reviewed literature relating to antibiotics use including: age, gender, level of education, and socio-economic status. Figure 2 shows the frequency of the dimensions reviewed in other studies that were conducted to measure the use of antibiotics. Thus, according to the dimensions available in previous studies and the dimensions present from this study, a conceptual model was created to show the relationship between the factors underlying antibiotics use/overuse (Figure 3).

The frequency distribution of the dimensions mentioned in the literature.

Conceptual framework.
Further psychometric testing is needed to determine the construct, concurrent, discriminate, and predictive validity of the PAPA scale. Moreover, the developed instrument can now be used in future research by translating it and culturally adapting it to different communities. In psychosocial research, instruments are frequently translated and cultural adapted to fit the population at hand [38]. Most instruments are developed in English. Therefore, for non-English speaking populations that are significantly different from the population used to develop the instrument, researchers usually translate and culturally adapt the English instrument to fit the local population [38]. Translation usually is a more efficient key for the scarcity of available instruments.
The PAPA scale produces a valid and reliable measurement instrument that can be used to assess parental perceptions regarding antibiotics. Since antibiotics overuse [3, 4] and antibiotics resistance are global public health issues [8, 9], many studies are targeted to minimise this problem. The PAPA scale could be effective in cross-sectional studies that aim to reduce the overuse of antibiotics in a community, starting by understanding the reasons behind this overuse. This, in turn, could inform the development of interventions directed to minimise the overuse of antibiotics.
Limitations
The survey was distributed within primary schools in order to capture a more generalised cross-section of the community. However, since kindergartens are scarce in Saudi Arabia and not mandatory like primary, secondary, and high schools, parents of children under the age of six are not represented in such a sample unless there is more than one child in the household. Consequently, this could be considered a source of bias [39]. Also, another limitation is the low response rate which may raise concerns about selection bias.
Conclusion
This is the first paper to validate an instrument that measures the overuse of antibiotics at the patients/parents level. The study shows promising results, producing evidence of strong collection of conceptually homogenous items and clear alignment of the ‘factors’ with constructs identified in early phase. This instrument now needs further validation such as: confirming the construct validity using confirmatory factor analysis, and criterion-related validity.
References
Jetacar : The use of Antibiotics in Food-producing animals. Australia: Commonwealth Department of Health and Aged Care; 1999.
Wutzke S, Artist M, Kehoe L, Fletcher M, Mackson J, Weekes L: Evaluation of a national programme to reduce inappropriate use of antibiotics for upper respiratory tract infections: effects on consumer awareness, beliefs, attitudes and behaviour in Australia. Health Promot Int 2007, 22: 53–64. 10.1093/heapro/dal034
Cebotarenco N, Bush P: Reducing antibiotics for colds and flu: a student-taught program. Heal Educ Res 2008, 23: 146–157.
Huang S, Rifas-Shiman S, Kleinman K, Kotch J, Schiff N, Stille C, Steingard R, Finkelstein J: Parental knowledge about antibiotic Use: results of a cluster-randomized, multicommunity intervention. Pediatrics 2007, 119: 698–706. 10.1542/peds.2006-2600
Grigoryan L, Burgerhof J, Haaijer-Ruskamp F, Degener J, Deschepper R, Monnet D, Di Matteo A, Scicluna E, Bara A, Lundborg C, Birkin J: Is self-medication with antibiotics in Europe driven by prescribed use? J Antimicrob Chemother 2007, 59: 152–156.
Flora K, Scott W, Jason B, Jonathan Z: Improving antibiotic utilization among hospitalists: A pilot academic detailing project with a public health approach. J Hosp Med 2008, 3: 64–70. 10.1002/jhm.278
Tenover F: Mechanisms of antimicrobial resistance in bacteria. Am J Med 2006, 119: 3–10.
Sorkhou I, Al-Qallaf B, Hajiah A, Al-Sheibani H, Bayoomi A, Mustafa A: Perceptions of patients attending primary care in kuwait regarding upper respiratory tract infections. Kuwait medical Journal 2002, 34: 272–275.
Green R: Symptomatic treatment of upper respiratory tract symptoms in children. South African Family Practice 2006, 48: 14–19.
Mora Y, Avila-Agtiero M, Umafia M, Jimenez A, Paris M, Faingezicht I: Epidemiologic observations of the judicious use of antibiotics in a pediatric teaching hospital. Int J Infect Dis 2002, 6: 74–77. 10.1016/S1201-9712(02)90141-4
Irshaid Y, Al-Homrany M, Hamdi A, Adjepon-Yamoah K, Mahfouz A: A pharmacoepidemiological study of prescription pattern in outpatient clinics in Southwestern Saudi Arabia. Saudi Med J 2004, 25: 1864–1870.
Simasek M, Blandino D: Treatment of the common cold. Am Fam Physician 2007, 75: 515–520.
Awad A, Eltayeb I, Matowe L, Thalib L: Self-medication with antibiotics and antimalarials in the community of khartoum state. Sudan J Pharm Pharmaceut Sci 2005, 8: 326–331.
Chan G, Tang S: Parental knowledge, attitudes and antibiotic use for acute upper respiratory tract infection in children attending a primary healthcare clinic in Malaysia. Singapore Med J 2006, 47: 266–270.
Mitsi G, Jelastopulu E, Basiaris H, Skoutelis A, Gogos C: Patterns of antibiotic use among adults and parents in the community: A questionnaire-based survey in a Greek urban population. Int J Antimicrob Agents 2005, 25: 439–443. 10.1016/j.ijantimicag.2005.02.009
Al-Azzam S, Al-Husein B, Alzoubi F, Masadeh M, Al-Horani M: Self-medication with antibiotics in jordanian population. IJOMEH 2007, 20: 373–380.
Sarahroodi S, Arzi A, Sawalha A, Ashtarinezhad A: Antibiotics self-medication among southern iranian university students. Int J Pharmacol 2010, 6: 48–52.
Crossley J, Eiser C, Davies H: Children and their parents assessing the doctor–patient interaction: a rating system for doctors’ communication skills. Medical Education 2005, 39: 820–828. 10.1111/j.1365-2929.2005.02230.x
Alumran A, Hou X-Y, Hurst C: Assessing the overuse of antibiotics in children with URTIs in Saudi Arabia: Development of the parental perception on antibiotics scale (PAPA scale). Global Health: Journal of Epidemiology and; 2013.
Bawazir S: Prescribing pattern at Community Pharmacies in Saudi Arabia. Int Pharm J 1992, 6: 222–224.
Alumran A, Hurst C, Hou X-Y: Antibiotics Overuse in Children with Upper Respiratory Tract Infections in Saudi Arabia: Risk Factors and Potential Interventions. Clinical Medicine and Diagnostics 2011, 1: 8–16.
Kimberlin CL, Winterstein AG: Validity and reliability of measurement instruments used in research. Am J Health Syst Pharm 2008, 65: 2276–2284. 10.2146/ajhp070364
Ramaker C, Marinus J, Stiggelbout A, Van Hilten B: Systematic evaluation of rating scales for impairment and disability in Parkinson’s disease. Mov Disord 2002, 17: 867–876. 10.1002/mds.10248
Alumran A, Hou X-Y, Hurst C: Validity and reliability of instruments designed to measure factors influencing the overuse of antibiotics. J Infect Public Health 2012, 5: 221–232. 10.1016/j.jiph.2012.03.003
Colton D, Covert R: Designing and constructing instruments for social research and evaluation. San Francisco, CA: Jossey-Bass; 2007.
Corbett K, Gonzales R, Leeman-Castillo B, Flores E, Maselli J, Kafadar K: Appropriate antibiotic use: variation in knowledge and awareness by Hispanic ethnicity and language. Prev Med 2005, 40: 162–169. 10.1016/j.ypmed.2004.05.016
Britten N, Ukoumunne O: The influence of patients’ hopes of receiving a prescription on doctors’ perceptions and the decision to prescribe: a questionnaire survey. BMJ 1997, 315: 1506–1510. 10.1136/bmj.315.7121.1506
Akici A, Kalaca S, Ugurlu U, Oktay S: Prescribing habits of general practitioners in the treatment of childhood respiratory-tract infections. Eur J Clin Pharmacol 2004, 60: 211–216. 10.1007/s00228-004-0749-9
Larson E, Dilone J, Garcia M, Smolowitz J: Factors which influence latino community members to self-prescribe antibiotics. Nurs Res 2006, 55: 94–102. 10.1097/00006199-200603000-00004
Hasson F, Keeney S, McKenna H: Research guidelines for the Delphi survey technique. J Adv Nurs 2000, 32: 1008–1015.
Lawshe C: A Quantitative approach to content validity. Pers Psychol 1975, 28: 563–575. 10.1111/j.1744-6570.1975.tb01393.x
Kogan M, Pappas G, Yu S, Kotelchuck M: Over-the-counter medication Use among US preschool-age children. JAMA 1994, 272: 1025–1030. 10.1001/jama.1994.03520130063034
Bi P, Tong S, Partonc K: Family self-medication and antibiotics abuse for children and juveniles in a Chinese city. Soc Sci Med 2000, 50: 1445–1450. 10.1016/S0277-9536(99)00304-4
Borg M, Scicluna E: Over-the-counter acquisition of antibiotics in the Maltese general population. Int J Antimicrob Agents 2002, 20: 253–257. 10.1016/S0924-8579(02)00194-2
Svensson E, Haaijer-ruskamp F, Lundborg C: Self-medication with antibiotics in a swedish general population. Scand J Infect Dis 2004, 36: 450–452. 10.1080/00365540410020721
Linstone HA, Turoff M: The Delphi method: techniques and applications. Addison-Wesley Pub. Co.: Advanced Book Program; 1975.
Ray D, Rohren C: Characteristics of patients with upper respiratory tract infection presenting to a walk-in clinic. Mayo Clin Proc 2001, 76: 169–173.
Van Widenfelt BM, Treffers PDA, de Beurs E, Siebelink BM, Koudijs E: Translation and Cross-Cultural Adaptation of Assessment Instruments Used in Psychological Research With Children and Families. Clinical Child and Family Psychology Review 2005, 8: 135–147. 10.1007/s10567-005-4752-1
UNESCO IBoE: World Data on Education. 7th edition. Saudi Arabia; 2010/11
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
There is no competing interest related to this study. Funding was received from University of Dammam, Saudi Arabia.
Authors’ contributions
AA carried out the main intellectual contribution to the conception and design of the study, data collection, and made substantial contribution in the analysis and interpretation of the data. XH participated in the design of the study, and has been involved in revising the manuscript critically for important intellectual content. CH participated in the design of the study, made substantial contribution in the analysis and interpretation of the data, was involved in the revising the manuscript critically for important intellectual content, and has given the final approval of the version to be published. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Alumran, A., Hou, XY. & Hurst, C. Assessing the overuse of antibiotics in children in Saudi Arabia: validation of the parental perception on antibiotics scale (PAPA scale). Health Qual Life Outcomes 11, 39 (2013). https://doi.org/10.1186/1477-7525-11-39
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7525-11-39