
Abstract
Background
Expression of human Interleukin-5 receptor alpha (hIL-5Rα) is controlled by alternative splicing, which generates two different transcripts encoding a membrane-anchored and a soluble form of the receptor, respectively. Although the study of the expression and regulation of hIL-5Rα is of crucial importance in the field of immunological processing, methods and techniques until now described lack sufficient sensitivity for detection of small differences in the expression of these isoforms. The aim of this study was to develop a reliable and sensitive real-time quantitative PCR assay to analyse the expression level of each isoform.
Methods
For the quantitative real-time PCR assay, two standard curves specific for each splice variant were constructed. PCR amplifications were performed on CDNA from peripheral blood, eosinophilic chronic rhinosinusitis and normal nasal tissue using a common forward and two specific reverse primers, in combination with SYBR Green I as the detection format.
Results and conclusion
We have developed an accurate and reliable assay for quantification of interleukin-5 receptor alpha mRNA isoforms over a broad dynamic range of input molecules. Importantly, excess of one isoform did not influence accurate quantification of the other isoform. Quantification of hIL-5Rα variants in human samples demonstrated an overexpression of both membrane-anchored and soluble encoding variants in eosinophilic chronic rhinosinusitis tissue and peripheral blood in patients with eosinophilic chronic rhinosinusitis compared to healthy subjects. The implementation of this assay will allow a better understanding of the regulatory mechanisms of the hIL-5Rα gene and hence its role in the pathogenesis of chronic inflammatory diseases.
Similar content being viewed by others

Background
Immune responses are mediated by a large group of peptides known as cytokines. These molecules play an important role in promoting cell growth, differentiation, activation and regulation of human inflammatory responses. Human interleukin-5 (hIL-5), a haemopoietin that belongs to the alpha-helical group of cytokines, plays an essential role in the induction and maintenance of eosinophilic airway infiltration [1–3]. It has been shown that this cytokine is linked to the occurrence of chronic inflammatory diseases such as asthma and eosinophilic chronic rhinosinusitis [4–6]. The action of the hIL-5 is mediated by interaction with its receptor, the human IL-5 receptor. This receptor belongs to the class I cytokine receptor family together with receptors for IL-3 and GM-CSF [7, 8] and consists of a heterodimer containing a unique α-subunit required for ligand-specific binding [9], and a β-subunit involved in binding affinity and signal transduction events [9]. Expression of the α-subunit has been described, in vitro, in eosinophils and basophils, whereas the β-subunit is expressed in eosinophils, B cells, and basophils, but also in type II pneumocytes [10–12].
The gene for the human interleukin 5 receptor alpha subunit (hIL-5Rα) is present in a single copy on chromosome 3 (band 3p26) of the human genome [13] and is composed of 13 introns and 14 exons [13].
Recent studies have shown that function and expression of hIL-5Rα can be regulated through splicing events and by ligand (hIL-5) stimulation [14]. Splicing of the hIL-5Rα gene can generates two different transcripts: one encoding a membrane-anchored protein through alternative splicing, and a second one encoding a soluble form of this receptor, by normal splicing events [15].
Although both receptor isoforms bind to hIL-5 with equal affinity [15], different responses are generated. The membrane-anchored receptor interacts with the β-subunit, increasing the affinity for hIL-5 and activating specific signal transduction pathways, such as cellular proliferation, maturational responses and inhibition of cell apoptosis [16, 17]. The soluble isoform competes with the membrane-anchored receptor for hIL-5 binding [18], and therefore this variant is considered to be a potential natural negative regulator of hIL-5 function in vivo [19].
Knowledge of the regulatory mechanisms of hIL-5Rα expression is of utmost relevance for the development of future therapeutic strategies to control eosinophil activation mechanisms. However, although the groundwork for such strategies is currently being laid [16, 20, 21], regulation of hIL-5Rα gene transcription still remains largely unknown.
Reverse transcriptase PCR (RT-PCR) is a technique that is increasingly used to quantify physiological changes in gene expression. However, this method has the limitation that accurately quantification is in most of the cases not possible [22]. To circumvent this problem, several RT-PCR techniques have been developed during the last decade with the real-time PCR being the most accurate and straightforward. This methodology consists in the continuous monitoring of a fluorescent reporter, the signal of which increases in direct proportion to the amount of PCR product formed in a reaction. Quantitative real-time PCR has the advantage of a large dynamic range of quantification, no requirement for post-PCR sample handling and extremely good sensitivity [23]. Several fluorescent detection strategies for this technique have been developed, including the SYBR Green I DNA binding dye [24, 25] and the use of specific fluorescently labelled hybridization or hydrolysis probe(s) [26, 27].
The aim of this study was to develop a reliable and accurate real-time PCR method using SYBR Green I technology that allows cost effective measurements of the expression levels of the hIL-5Rα splice variants in human tissue and peripheral blood. As a model system, we use eosinophilic chronic rhinosinusitis, a sinus disease associated with severe local and systemic eosinophilic inflammation.
 and beta-actin genes
and beta-actin genesResults and Discusion
Experimental validation
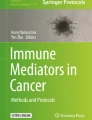
A common forward primer and two exon specific reverse primers were used for the quantification of the soluble and membrane-anchored hIL-5Rα encoding transcripts by real-time PCR amplification (Fig. 1). The forward primer is located in exon 10, whereas the reverse primer for the transcript encoding for the soluble form hybridises to exon 11, which is specific for this isoform [15]. The reverse primer for the membrane-anchored encoding variant is positioned in exon 12, which is also specific for this splice form [15]. Specific amplification was verified by agarose electrophoresis (4% in TAE), which resulted in one specific band of the expected size (membrane-anchored = 87 bp, soluble = 95 bp). These data were also confirmed in a melting curve analysis performed on the GeneAmp 5700 Sequence Detection System. Dissociation curves showed a single peak corresponding to a melting temperature of 80.2°C for the soluble and 81.6°C for the membrane-anchored hIL-5Rα encoding splice form, demonstrating specific amplification and the absence of primer dimers.

Alternative splicing of the human Interleukin 5 receptor alpha gene (hIL-5Rα) generating two transcripts encoding the soluble and membrane-anchored hIL-5Rα isoforms. Skipping of exons 12, 13 and 14 generate the soluble encoding form, whereas for the membrane-anchored encoding variant, only exon 11 is skipped. Arrows indicate the region amplified by the primer pairs 3 or 4.
To exclude the possibility of coamplification of contaminating genomic DNA during RT-PCR, we performed a PCR run with either cDNA or genomic DNA extracted from eosinophilic chronic rhinosinusitis tissue samples. The amplicons were analysed by 2% agarose electrophoresis and the absence of a specific band for the genomic DNA sample confirmed the cDNA specificity of the primers. In addition, all samples were treated with DNase during RNA purification as described by the manufacturer (Qiagen, USA).
To quantify the number of molecules of each hIL-5Rα splice form, we constructed two different standard curves. The template of these standards consisted of PCR fragments obtained from two plasmids containing the specific cDNA sequence for each splice variant as explained in Materials and Methods. Analytical sensitivity in the GeneAmp 5700 Sequence Detection System was determined by using a ten-fold serial dilution of the standards for the soluble and membrane-anchored encoding transcripts as template for amplification. Amplification with the SYBR Green I Master mix and primer pair 3 or 4, resulted in sensitive standard curves where a minimum of 5 molecules of each splice variant could be detected. A high linearity (expressed as correlation coefficient R2) was observed over a dynamic range of at least 4 orders of magnitude. The maximum amount that could be quantified to keep the standard curve's linearity was 5 × 105 molecules for the soluble and 5 × 104 molecules for the membrane-anchored encoding transcripts.
In all cases, PCR efficiency ranged between 0.95 and 0.97 for both splice variants. Accuracy of the standard curves was evaluated by analysing each standard dilution point as unknown as previously described [29]. Coefficients of variation (C.V.) less than 2% for CT and 25 % for calculated quantities demonstrate the accuracy of the standard in all dilutions tested (Table 2).
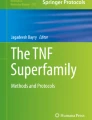
Quantification of either soluble or membrane-anchored hIL-5Rα encoding transcripts in the presence of the alternative form was tested by mixing an excess (5 × 105 molecules) of one transcript form with a dilution series of the other. As a control, we used a standard curve containing only a single splice variant. In absence of inhibition, both dilution series should give equal CT values and quantities for each dilution point. The low coefficient of variation values obtained in this experiment indicate that accurate and specific quantification of hIL-5Rα splice variants is possible up to 5 molecules (equivalent PCR product), in presence of excess of the alternative splice form (Figure 2).

PCR amplification plots of each hIL-5Rα splice variant in the presence of excess of the alternative splice form. PCR amplification plots of the membrane-anchored (A) and soluble (B) encoding splice variant in presence of the alternative splice variant (data generated on iCycler iQ Real-Time PCR Detection System, BioRad Laboratories, USA). Curves in blue indicate the standards diluted in water; curves in red represent standards diluted in 5 × 105 molecules of the alternative splice form. The table indicates the quantities for both standard curves and the coefficient of variation (C.V) between the quantities (molecule number) obtained for each dilution point.
Expression of hIL-5Rα splice variants in biological samples
Quantities of the transcripts encoding the soluble and the membrane-anchored forms of hIL-5Rα are expressed as relative number of molecules normalized to the number of molecules of internal control gene ACTB. Analysis of mRNA levels showed a significantly higher expression of both splice forms in eosinophilic chronic rhinosinusitis tissue (CRS) compared to normal nasal mucosa (Fig. 3). In addition, in peripheral blood from CRS patients compared to control subjects, both transcripts were also overexpressed, reaching statistical significance however only for the soluble variant (Fig. 3).

Relative number of molecules of the transcripts encoding the soluble and membrane anchored of hIL-5Rα after normalization to beta-actin (ACTB) gene in eosinophilic chronic rhinosinusitis and normal nasal mucosa (A) and in peripheral blood from eosinophilic chronic rhinosinusitis patients and healthy subjects (B). **: p < 0.01; *: p < 0.05; N.S.: non significant differences, CRS: eosinophilic chronic rhinosinusitis patients; Ctrol.: healthy subjects.
These data demonstrate that quantification of the hIL-5Rα splice isoforms by real-time quantitative PCR is feasible in human peripheral blood and eosinophilic chronic rhinosinusitis tissue, showing an up-regulation of both isoforms in nasal tissue and blood from eosinophilic chronic rhinosinusitis patients. In view of the crucial role of hIL-5 in the terminal differentiation of eosinophils and the involvement of these cells in severe airway and skin diseases, tools to investigate the regulation of the IL-5 receptor expression in vivo are mandatory to understand the pathomechanisms involved as well as to design future therapeutic approaches [3, 30–33]. Treatment of eosinophil-infiltrated polyp tissue with neutralizing anti-IL-5 monoclonal antibody (mAb) resulted in eosinophil apoptosis and decreased tissue eosinophilia in vitro [29], but antagonizing IL-5 activity in asthma patients with humanized anti-IL-5 mAbs was largely unsuccessful [33] [34]. A reassessment of the in vivo regulation of the soluble and membrane anchored hIL-5Rα expression may help to understand the role of the soluble variant, which has antagonistic properties in vitro, and a possible role in failures of anti-IL5 treatment.
Conclusion
We have established a fast, accurate and reliable assay for mRNA quantification of the hIL-5Rα splice isoforms over a broad range of input molecules. The assay was applied on eosinophilic chronic rhinosinusitis tissue and human peripheral blood and demonstrated an overexpression of both soluble and membrane-anchored encoding splice variants of hIL-5Rα in both tissue and peripheral blood of patients with eosinophilic chronic rhinosinusitis compared to healthy subjects. The development of this assay will greatly help in the study of the regulatory mechanisms of hIL-5Rα. It will also allow investigations of relative expression of this receptor in other eosinophil-related diseases such as asthma, atopic dermatitis and hypereosinophilic syndrome, and hence will contribute to the development of future therapeutic strategies for eosinophil inflammatory diseases.
Methods
Sample Preparation
Samples from normal nasal mucosa and eosinophilic chronic rhinosinusitis biopsies were collected, frozen in liquid nitrogen and thoroughly grinded with a cooled mortar and pestle (Fisher Scientific, UK). 30 mg of tissue were then resuspended in 0.6 ml of lysis (RLT) buffer (Qiagen, USA) and stored at -20°C until RNA extraction.
Peripheral blood (5 ml) from subjects was collected in tubes containing EDTA (Terumo, Leuven, Belgium) and centrifuged at 300 g for 5 minutes. Leukocytes were collected and red blood cells were hemolysed in 25 ml (5 ml per 1 ml of leukocytes suspension) of cold isotonic NH4Cl-EDTA lysis buffer (155 mM NH4Cl, 10 mM KHCO3, 0.1 mM EDTA, pH 7.2) during 5 minutes at 15°C. Cell suspensions were then centrifuged at 300 g for 6 minutes at 4°C and washed in PBS. Finally, cells were resuspended in 0.6 ml of RLT buffer (Qiagen, USA) and stored at -20°C until RNA preparation.
RNA isolation and reverse transcription
For extraction of total RNA, peripheral blood leukocytes, eosinophilic chronic rhinosinusitis and normal nasal mucosa tissue, (all present in RLT buffer), were first homogenized with QIAshreder homogeniser (Qiagen, USA) as described by the manufacturer. RNA purification was performed with RNeasy mini Kit (Qiagen, USA). RNA was quantified using the RiboGreen kit (Molecular Probes, Leiden, The Netherlands) on a TD-360 fluorometer (Turner Design, USA) and reverse transcription was performed for 1 μg of total RNA in a 20 μl reaction volume. Briefly, 1 μl of Oligo (dT)12–18 (500 μg/ml) (Invitrogen, USA) and 200 ng of Random Primers (Invitrogen, USA) were added to each RNA sample and incubated at 70°C for 10 min. Then, the samples were incubated with 4 μl of 5 × First-Strand Buffer (Invitrogen, USA), 1 μl of 10 mM dNTP mix (Pharmacia Biotech, USA), 2 μl of 0.1 mM dithiothreitol (Invitrogen, USA) and 200 units of Superscript RNase H- Reverse Transcriptase (Invitrogen, USA), first at 25°C for 10 minutes and subsequently at 42°C during 50 minutes. The reaction was stopped by heating at 90°C for 5 minutes. Finally, RNA complementary to the cDNA was removed by adding 1 μl (2 units) of E. coli Ribonuclease H (Invitrogen, USA) and incubated for 30 minutes at 37°C. All cDNA samples were stored at -20°C until analysis.
Primer design
Different primer pairs were designed for generation of standard curve template and for the actual quantification of the hIL-5Rα splice variants (Table 1), based on published cDNA sequences (GenBank accession nos. M75914 and M96652). Primer pairs 1, 2 and 5 were designed using Primer 3 software (Rozen et al., 2000) using the following parameters: primer size between 20 and 27 base pairs, primer Tm range between 60 and 66°C, GC content between 45 and 50%, and sequences containing no runs of four or more identical nucleotides.
Primer pairs 3, 4 and 5 were designed in Primer Express Software version 1.5 (Applied BioSystems, USA) using the sequences flanked by the first set of primers 1, 2 and 5 respectively. Default TaqMan parameters were used with a restriction of amplicon length between 80 and 100 bp.
Generation of gene-specific real-time PCR standards
Two plasmids containing the cDNA sequences for the soluble or membrane-anchored encoding transcripts of hIL-5Rα, kindly provided by Prof. Dr. Jan Tavernier, were used to prepare the template for the standards. A cDNA fragment from each isoform was amplified by mixing 1 × Taq Polymerase Master mix (Invitrogen, USA) with 200 nM of primer pair 1 or 2, 20 ng of plasmid DNA and nuclease-free water to a final volume of 50 μL. The PCR conditions were: 95°C for 10 minutes followed by 35 cycles at 95°C for 30 seconds and 64°C for 1 minute and a final cycle at 72°C for 5 minutes in an ICycler thermal cycler (BioRad Laboratories, USA). The PCR products consisted of a DNA fragment of 294 bp for the soluble and 347 bp for the membrane-anchored encoding transcripts. PCR fragments were run on a 2% agarose gel, excised and eluted using the QIAquick PCR purification kit (Qiagen, USA).
PCR fragments were quantified using the PicoGreen kit (Molecular Probes, The Netherlands) on a TD-360 fluorometer (Turner Design) and the molar concentration of each PCR product was calculated on the basis of the mass concentration and the length in base pairs of each fragment as previously described [29]. Equimolar quantities of both standards were 10-fold serially diluted and used to generate standard curves. The generation of a standard curve, based on serial dilutions of fluorometrically quantified PCR products has been shown to be very reliable [29]. Template for the standard curve for the internal control gene ACTB was prepared following the same procedure described above, using primer pair 5 (Table 1).
Real-time quantitative PCR using SYBR Green I
Real-time PCR was performed on a GeneAmp 5700 Sequence Detection System (Applied BioSystems, USA). In each experiment, duplicates of a standard dilution series of specific PCR fragments for each hIL-5Rα transcript variant and 25ng cDNA (total RNA equivalent) of unknown samples were amplified in a 25 μl reaction containing 1x SYBR Green I Master mix (Qiagen, USA) and 300 nM of primer pair 2, 3 or 4 for the membrane-anchored or soluble receptor encoding transcripts, respectively, and nuclease-free water. The thermal profile consisted of 1 cycle at 95°C for 10 minutes followed by 40 cycles at 95°C for 30 seconds and at 60°C for 1 minute. Real-time PCR efficiencies for each reaction were calculated using the formula:Efficiency (E) = [10(1/slope)] - 1, from the slope values given in the GeneAmp 5700 Sequence Detection System.
Quantification and data analysis
For each run, data acquisition and analysis was done by the 5700 Sequence Detection System software (version 1.3, Applied Biosystems, USA). The relative number of molecules of each transcript was determined by interpolating the C T values of the unknown samples to each standard curve and the obtained values were normalized with respect to the ACTB number of molecules. Statistical tests were performed using the MedCalc program version 6. The Mann Whitney U-test (unpaired) was used for comparison between the groups and p values < 0.05 were considered statistically significant.
References
Kaminuma O, Mori A, Suko M, Kikkawa H, Naito K, Okudaira H: Development of lung eosinophilic inflammation by the infusion of IL-5-producing T cell clones. International Archives of Allergy and Immunology. 1997, 114: 10-13.
Hamelmann E, Cieslewicz G, Schwarze J, Ishizuka T, Joetham A, Heusser C, et al: Anti-interleukin 5 but not Anti-IgE prevents airway inflammation and airway hyperresponsiveness. American Journal of Respiratory and Critical Care Medicine. 1999, 160: 934-941.
Blumchen K, Kallinich T, Hamelmann E: Interleukin-5: a novel target for asthma therapy. Expert Opinion on Biological Therapy. 2001, 1: 433-453.
Bachert C, Wagenmann M, Hauser U, Rudack C: IL-5 synthesis is upregulated in human nasal polyp tissue. Journal of Allergy and Clinical Immunology. 1997, 99: 837-842.
Denburg JA: Haemopoietic mechanisms in nasal polyposis and asthma. Thorax. 2000, 55: S24-S25. 10.1136/thorax.55.suppl_2.S24.
Rizzo CA, Yang R, Greenfeder S, Egan RW, Pauwels RA, Hey JA: The IL-5 receptor on human bronchus selectively primes for hyperresponsiveness. Journal of Allergy and Clinical Immunology. 2002, 109: 404-409. 10.1067/mai.2002.122459.
Bazan JF: Structural Design and Molecular Evolution of A Cytokine Receptor Superfamily. Proceedings of the National Academy of Sciences of the United States of America. 1990, 87: 6934-6938.
Boulay JL, Paul WE: The Interleukin-4 Family of Lymphokines. Current Opinion in Immunology. 1992, 4: 294-298. 10.1016/0952-7915(92)90079-T.
Takagi M, Hara T, Ichihara M, Takatsu K, Miyajima A: Multi-Colony Stimulating Activity of Interleukin-5 (Il-5) on Hematopoietic Progenitors from Transgenic Mice That Express Il-5 Receptor Ex Subunit Constitutively. Journal of Experimental Medicine. 1995, 181: 889-899.
Denburg JA, Silver JE, Abrams JS: Interleukin-5 Is A Human Basophilopoietin – Induction of Histamine Content and Basophilic Differentiation of Hl-60 Cells and of Peripheral-Blood Basophil-Eosinophil Progenitors. Blood. 1991, 77: 1462-1468.
Migita M, Yamaguchi N, Mita S, Higuchi S, Hitoshi Y, Yoshida Y, et al: Characterization of the Human Il-5 Receptors on Eosinophils. Cellular Immunology. 1991, 133: 484-497.
Miyajima A, Mui ALF, Ogorochi T, Sakamaki K: Receptors for Granulocyte-Macrophage Colony-Stimulating Factor, Interleukin-3, and Interleukin-5. Blood. 1993, 82: 1960-1974.
Tuypens T, Tavernier J: Genomic Organization of the hIL-5R Gene. Faseb Journal. 1992, 6: A1896-
Tavernier J, Van der Heyden J, Verhee A, Brusselle G, Van Ostade X, Vandekerckhove J, et al: Interleukin 5 regulates the isoform expression of its own receptor alpha-subunit. Blood. 2000, 95: 1600-1607.
Tavernier J, Tuypens T, Plaetinck G, Verhee A, Fiers W, Devos R: Molecular-Basis of the Membrane-Anchored and 2 Soluble Isoforms of the Human Interleukin-5 Receptor Alpha-Subunit. Proceedings of the National Academy of Sciences of the United States of America. 1992, 89: 7041-7045.
Yasruel Z, Humbert M, Kotsimbos TC, Ploysongsang Y, Minshall E, Durham SR, et al: Membrane-bound and soluble alpha IL-5 receptor mRNA in the bronchial mucosa of atopic and nonatopic asthmatics. American Journal of Respiratory and Critical Care Medicine. 1997, 155: 1413-1418.
Koike M, Takatsu K: Il-5 and Its Receptor – Which Role do they play in the Immune-Response. International Archives of Allergy and Immunology. 1994, 104: 1-9.
Tavernier J, Devos R, Cornelis S, Tuypens T, Vanderheyden J, Fiers W, et al: A Human High-Affinity Interleukin-5 Receptor (IL5R) Is Composed of An IL5-Specific Alpha-Chain and a Beta-Chain Shared with the Receptor for Gm-Csf. Cell. 1991, 66: 1175-1184.
Monahan J, Siegel N, Keith R, Caparon M, Christine L, Compton R, et al: Attenuation of IL-5-mediated signal transduction, eosinophil survival, and inflammatory mediator release by a soluble human IL-5 receptor. Journal of Immunology. 1997, 159: 4024-4034.
Zanders E: Interleukin-5 Receptor-Alpha Chain Messenger-RNA Is Down-Regulated by Transforming Growth-Factor-Beta-1. European Cytokine Network. 1994, 5: 422-
Devos R, Plaetinck G, Cornelis S, Guisez Y, Van der Heyden J, Tavernier J: Interleukin-5 and its receptor: a drug target for eosinophilia associated with chronic allergic disease. Journal of Leukocyte Biology. 1995, 57: 813-
Yin JL, Shackel NA, Zekry A, McGuinness PH, Richards C, Van der Putten K, et al: Real-time reverse transcriptase-polymerase chain reaction (RT-PCR) for measurement of cytokine and growth factor mRNA expression with fluorogenic probes or SYBR Green I. Immunology and Cell Biology. 2001, 79: 213-221. 10.1046/j.1440-1711.2001.01002.x.
Bustin SA: Absolute quantification of mRNA using real-time reverse transcription polymerase chain reaction assays. Journal of Molecular Endocrinology. 2000, 25: 169-193.
Higuchi R, Fockler C, Dollinger G, Watson R: Kinetic Pcr Analysis – Real-Time Monitoring of DNA Amplification Reactions. Bio-Technology. 1993, 11: 1026-1030.
Morrison TB, Weis JJ, Wittwer CT: Quantification of low-copy transcripts by continuous SYBR (R) green I monitoring during amplification. Biotechniques. 1998, 24: 954-
Livak KJ, Flood SJA, Marmaro J, Giusti W, Deetz K: Oligonucleotides with Fluorescent Dyes at Opposite Ends Provide A Quenched Probe System Useful for Detecting PCR Product and Nucleic-Acid Hybridization. Pcr-Methods and Applications. 1995, 4: 357-362.
Wittwer CT, Herrmann MG, Moss AA, Rasmussen RP: Continuous fluorescence monitoring of rapid cycle DNA amplification. Biotechniques. 1997, 22: 130-
Vandesompele J, De Preter K, Pattyn F, Poppe B, Van Roy N, De Paepe A, et al: Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol. 2002, 3: RESEARCH0034.1-0034.11. 10.1186/gb-2002-3-7-research0034.
Vandenbroucke II, Vandesompele J, Paepe AD, Messiaen L: Quantification of splice variants using real-time PCR. Nucleic Acids Res. 2001, 29: E68-10.1093/nar/29.13.e68.
Simon HU, Yousefi S, Schranz C, Schapowal A, Bachert C, Blaser K: Direct demonstration of delayed eosinophil apoptosis as a mechanism causing tissue eosinophilia. J Immunol. 1997, 158: 3902-3908.
Liu LY, Sedgwick JB, Bates ME, Vrtis RF, Gern JE, Kita H, et al: Decreased expression of membrane IL-5 receptor alpha on human eosinophils: I. Loss of membrane IL-5 receptor alpha on airway eosinophils and increased soluble IL-5 receptor alpha in the airway after allergen challenge. J Immunol. 2002, 169: 6452-6458.
Gevaert P, Bachert C, Holtappels G, Novo CP, Van Der HJ, Fransen L, et al: Enhanced soluble interleukin-5 receptor alpha expression in chronic rhinosinusitis. Allergy. 2003, 58: 371-379.
Leckie MJ, ten Brinke A, Khan J, Diamant Z, O'Connor BJ, Walls CM, et al: Effects of an interleukin-5 blocking monoclonal antibody on eosinophils, airway hyper-responsiveness, and the late asthmatic response. Lancet. 2000, 356: 2144-2148. 10.1016/S0140-6736(00)03496-6.
Acknowledgments
We wish to thank Prof. Dr. Jan Tavernier and Jose Van der Heyden for their help in providing plasmids, cDNA sequences and helpful discussions. This work was also partially supported by the GOA-grant 12051203 and VEO-grant 011V1302.
Author information
Authors and Affiliations
Corresponding author
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Pérez, C., Vandesompele, J., Vandenbroucke, I. et al. Quantitative Real Time Polymerase Chain Reaction for measurement of human Interleukin – 5 receptor alpha spliced isoforms mRNA. BMC Biotechnol 3, 17 (2003). https://doi.org/10.1186/1472-6750-3-17
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6750-3-17