
Abstract
Background
Knowledge about coronary heart disease (CHD) and its risk factors is an important pre-requisite for an individual to implement behavioral changes leading towards CHD prevention. There is scant data on the status of knowledge about CHD in the general population of Pakistan. The objective of this study was to assess knowledge of CHD in a broad Pakistani population and identify the factors associated with knowledge.
Methods
Cross sectional study was carried out at four tertiary care hospitals in Pakistan using convenience sampling. Standard questionnaire was used to interview 792 patient attendants (persons accompanying patients). Knowledge was computed as a continuous variable based on correct answers to fifteen questions. Multivariable linear regression was conducted to determine the factors independently associated with knowledge.
Results
The mean age was 38.1 (±13) years. 27.1% had received no formal education. The median knowledge score was 3.0 out of a possible maximum of 15. Only 14% were able to correctly describe CHD as a condition involving limitation in blood flow to the heart. Majority of respondents could identify only up to two risk factors for CHD. Most commonly identified risk factors were stress (43.4%), dietary fat (39.1%), smoking (31.9%) and lack of exercise (17.4%). About 20% were not able to identify even a single risk factor for CHD. Factors significantly associated with knowledge included age (p = 0.023), income (p < 0.001), education level (p < 0.001), residence (p < 0.001), a family history of CHD (p < 0.001) and a past history of diabetes (p = 0.004). Preventive practices were significantly lacking; 35%, 65.3% and 84.6% had never undergone assessment of blood pressure, glucose or cholesterol respectively. Only a minority felt that they would modify their diet, stop smoking or start exercising if a family member was to develop CHD.
Conclusion
This is the first study assessing the state of CHD knowledge in a relatively diverse non-patient population in Pakistan. There are striking gaps in knowledge about CHD, its risk factors and symptoms. These translate to inadequate preventive behavior patterns. Educational programs are urgently required to improve the level of understanding of CHD in the Pakistani population.
Similar content being viewed by others

Background
Coronary heart disease (CHD) is a major public health concern and accounts for more deaths than any other disease [1] worldwide. Developing countries were once considered to be less affected by CHD. However, the burden of CHD in developing countries has increased to epidemic proportions [2]. Furthermore, it is anticipated that within the next fifteen years, CHD will be the leading cause of death in these countries [1]. The prevalence of cardiovascular risk factors in the Asian population is high [3]. According to data from the National Health Survey of Pakistan, the prevalence of hypertension and diabetes is approximately 33% and 25% respectively, in persons over the age of 45 years [4, 5] while the overall prevalence of smoking is 28% in men, going as high as 41% amongst those aged 40 to 49 years [6]. Furthermore dietary habits in Pakistan are heavily weighed towards the consumption of saturated fats as well as ghee (hydrogenated vegetable oil) [7]. Knowledge about CVD and its risk factors is an important (albeit not the only) pre-requisite for an individual to implement behavioral changes leading towards CHD prevention. Estimating the knowledge base of the community regarding CHD has important public health applications as it assists in developing targeted educational programs.
Studies in South Asians (Indians, Pakistanis and Bangladeshis) suggest a very poor degree of knowledge regarding CHD and its risk factors. In the study by Rankin [8] only a minority (approximately 20%) identified lack of exercise and obesity as a risk factor, while about 30% identified smoking as a factor related to CHD (amongst Pakistanis, this estimate was 14%) and approximately 30% considered dietary fat as a risk factor. Interestingly, only 5% of our respondents mentioned family history of CHD as a risk factor. There is scant data on the level of knowledge about CHD in the population of Pakistan. One prior study [9] has reported on the very poor awareness about risk factors for CHD in a lower middle-class urban population in Karachi, a major metropolitan city of Pakistan. In this selected population, consisting predominantly of women with a variable degree of formal education, less than 20% were aware of most risk factors for CHD. However, there is paucity of data on the status of knowledge in the broader population of the country, which consists of a much higher proportion of people with lower incomes, rural residency and no formal education. The aim of our study was to assess knowledge of CHD in a more diverse Pakistani population and identify the factors associated with knowledge in this study group. We also aimed to identify attitudes and behaviors regarding CHD prevention.
Methods
Study design
This was a multi-center cross sectional study conducted at four tertiary care hospitals in Pakistan. A convenience sample of 810 subjects consisting of attendants of patients (defined as persons accompanying patients to the hospital, usually family members or close relatives) visiting various outpatient departments of these four hospitals were invited to undergo an interview regarding their understanding of what coronary heart disease (CHD) was, risk factors, symptoms and practices related to CHD by trained medical officers. The four hospitals were chosen to enable the study population to pertain to a wide demographic spectrum of Pakistan. These hospitals were as follows: the Aga Khan University Hospital (AKUH) in Karachi is a private hospital that caters to a mixture of middle and upper class patients who (mostly) pay for their care. The Mayo Hospital in Lahore is a public hospital that caters primarily to poor patients who receive free care. The Pakistan Institute of Medical Sciences (PIMS) in a public hospital in Islamabad that caters to patients from a wide area that includes rural as well as urban areas and provides subsidized care. Finally, the Allied General Hospital (AGH) in Faisalabad is a large public hospital in Faisalabad that cares for urban as well as rural patients from central Punjab at nominal costs. The study was approved by each hospital's ethics review body.
Survey instrument
Study subjects were surveyed using a structured questionnaire that was developed to contain questions on four basic themes: (1) understanding of what CHD was; (2) knowledge of risk factors for CHD – respondents were asked what factors are related with CHD and the direction of the relationship between these factors and CHD was specified; (3) knowledge of the symptoms of CHD; and (4) preventive practices relating to CHD – whether subjects thought CHD was preventable and what preventive practices had they undertaken. The questionnaire was initially developed in English, translated into Urdu, then back-translated into English to check for consistency. The questionnaire, consisting of open-ended questions only, was pre-tested in 20 attendants and revised accordingly. All respondents were surveyed in an identical fashion. All questions were asked in Urdu. Responses to open-ended questions were recorded in English either by selection from a list of predefined answer categories or in writing if the particular response was not listed. Subjects were asked, at each question, whether they wished to add anything to their response, but were not prompted or given hints.
Study subjects
Patient attendants were selected as somewhat reflective of the general population for convenience reasons. Subjects were approached in the outpatients departments of the respective hospitals. If over the age of 18 years and able to give verbal consent, respondents underwent a standard questionnaire based survey. Subjects who were patients, under the age of 18 years, unable to communicate in Urdu (the national language of Pakistan) or were members of the hospital staff were excluded from this study. We estimated that a sample size of 371 would be required to estimate an assumed prevalence of 0.5 of various aspects knowledge about CHD at a confidence level of 95% with an error bound of 0.05.
Definitions
Knowledge was computed as a continuous variable using the cumulative score for each subject based on correct responses to 15 questions (Table 1). Each correct response was assigned one point. Urban dwelling was defined as residence within the geographical bounds of a major metropolitan city (Karachi, Islamabad, Rawalpindi, Faisalabad and Lahore). Rural dwelling was defined as residing outside the major metropolitan cities (most of Pakistan is fairly rural outside the major cities). Formal education was defined as education received in school (but did not include those going to traditional educational institutions or "madrassa").
Statistical analysis
All variables were entered into Statistical Package for Social Sciences (SPSS) version 10. Means and standard deviations were calculated for continuous variables and frequencies for categorical variables. Univariate analysis was performed by simple linear regression to determine the factors associated with knowledge. Univariate covariates with a p value of ≤0.25 were entered into the multivariable model. Multivariable regression using a stepwise technique was conducted to adjust for confounders and determine the factors independently associated with knowledge. The standardized residuals of the regression model were examined for outliers as well as for non-normality and nonlinearity using probability plots and residual plots. A significant level was defined as p < 0.05.
Results
Approximately 1000 potential respondents were approached. Eight hundred and ten subjects consented to participate in the study. Complete data were available for 792 subjects. The demographic and clinical characteristics of the study group are shown in Table 2.
Subjects were asked about what they thought CHD meant. Only 14% were able to correctly describe the latter as a condition involving limitation in blood flow to the heart. A variety of other descriptions were offered including a "malfunction of the heart" by 35%. Table 3 displays the distribution of responses to this question.
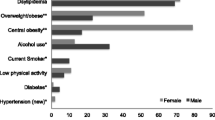
Participants were questioned about risk factors for CHD. As seen in Table 3, the most commonly identified risk factors were stress (43.4%), dietary fat (39.1%), smoking (31.9%) and lack of exercise (17.4%). However about 20% were not able to identify even a single risk factor for CHD (Figure 1). When questioned about the symptoms of CHD, only a minority were able to correctly identify symptoms of chest pain, dyspnea and diaphoresis (Table 3).

Risk factors for coronary heart disease identified by study subjects.
Subjects were questioned regarding preventive practices against CHD. Although nearly three quarters of the study group felt that CHD was preventable (Table 4), preventive practices in this study group were largely lacking.
Knowledge was assessed in this study as a continuous variable. Responses to 15 questions were scored as correct or incorrect and each respondent received one point for each correct answer (Table 1). The median knowledge score of the study group was 3.0 (range 0–11) out of a possible maximum of 15. Figure 2 shows the distribution of knowledge scores in the study group. No participant was able to achieve a score above 11.

Knowledge score for coronary heart disease.
Table 5 shows the results of the univariate and multivariable analyses for factors associated with knowledge of CHD, with the respective coefficients (slope of the regression line). In the univariate analysis, factors significantly associated with knowledge included age, gender, education (formal vs. no formal), monthly income (<3000 vs. >3000 Rupees), residence (rural vs. urban), smoking status, family history of CHD and a prior history of diabetes, hypertension or CHD (Table 5). Interestingly, there were also significant differences in the knowledge scores of subjects recruited from different hospitals. In the multivariable analysis factors independently associated with knowledge included age, education, residence, monthly income, family history of CHD, prior history of diabetes and hospital attended. Not unexpectedly, education had the most robust association with knowledge. In the adjusted analysis, gender, smoking and prior history of CHD and hypertension were not associated with knowledge.
Discussion
Our study demonstrates a striking lack of knowledge about CHD amongst patient attendants at four hospitals catering to patients belonging to a wide demographic spectrum. Only 14% of the study group could correctly identify what coronary heart disease was. The majority of subjects were only able to identify up to 2 risk factors, the most commonly identified factors being stress, obesity, dietary fat and smoking. The median knowledge score of the study group was 3.0 out of a possible 15, suggesting a severe lack of awareness about CHD.
Our findings are consistent with the study by Rankin et al. [8]. The gaps in knowledge are considerably high compared to what has been reported in Western countries [10].
The relatively poor knowledge about modifiable risk factors for CHD, including smoking (31.9%), obesity (14.1%), lack of exercise (17.4%) and dietary fat (39.1%) in our study population has been seen in other studies on South Asians [8]. It is possible that the very poor awareness about obesity and lack of exercise are related to their under representation in mass media campaigns as opposed to smoking and dietary fat. Our study highlights a significant lack of knowledge about modifiable risk factors and suggests the need for urgent emphasis on education amongst Pakistanis.
Respondents in our study appeared to lack sufficient knowledge about the symptoms of CHD. Only 36% knew that chest pain was a symptom of heart disease and a substantial number of subjects gave vague descriptions about possible symptoms of CHD (Table 3). Failure to recognize the symptoms of acute myocardial infarction is associated with delay in seeking medical care [11] and leads to worse clinical outcomes. Our study suggests a need for educating the public about symptoms of CHD.
Age appears to have a linear relationship with knowledge in our study. When age was analyzed as a categorical variable, mean knowledge scores progressively increased from the ≤30 year age group (3.06) to the >60 year group (3.93; coefficient 0.76; p = 0.03). This is different to the findings of Potvin [10] in Canadians where, compared to the age group 18–24 years, the odds ratios for knowledge about risk factors decreased as aged increased, particularly in those aged 65–74 years. One possible explanation could be a very limited emphasis on health education in schools in Pakistan, as a result of which individuals finishing school do so with very little knowledge about CHD. As the years go by, they are likely to accrue knowledge (albeit in small increments). On the other hand, modern school education in the west may involve substantially more time spent on health education; as a consequence younger individuals are likely to be more knowledgeable than the elderly who may not have received such instruction during their schooling years. The finding that knowledge increases with the acquisition of formal education is consistent with other data [10, 12]. Likewise, the association of income with knowledge has been reported in other studies [10]. In our study this association was independent of the level of education.
There were interesting differences in knowledge score between subjects recruited from the four different hospitals. The mean knowledge score was significantly higher in patients presenting to AGH, a hospital that caters to a substantially poorer, uneducated and rural population compared to AKU and PIMS (Table 6). AGH conducts a large number of public awareness seminars and it is possible that this may be contributing to the higher knowledge scores in patients recruited from that hospital. This potential association between educational seminars for the public and knowledge deserves further investigation.
Consistent with the overall poor state of knowledge in our study group, preventive practices were found to be significantly lacking. Although nearly three-fourths of the study group felt that CHD was preventable, over two-thirds had never had their blood pressure checked, and an overwhelming majority had never undergone an assessment of their blood glucose or cholesterol levels. Furthermore, only a minority felt that they would modify their diet, stop smoking or start exercising if a family member was to develop CHD (table 4), consistent with the fact that the vast majority of our study subjects did not identify a family history of CHD as a risk factor for developing CHD in the future.
Our study is not without limitations. First, the non-probability convenience sampling method introduces selection bias. As samples were taken from four different hospitals in Pakistan representing a wide demographic spectrum, we feel that our study population may be somewhat reflective of the knowledge state of the general population of Pakistan. However, patient attendants may be either less knowledgeable or more informed than the general population. On the one hand, due to more exposure to a medical environment patient attendants may know more about CHD than the general public and therefore, the true knowledge state of the public may be lower. On the other hand, diseased individuals may, in part, be in that state due to the poor knowledge of their household members. Hence, selection of subjects from households of patients risks bias whereby the study subjects may be less knowledgeable than population controls. Second, the use of an open-ended questionnaire introduces the potential of recall bias on the part of the respondents and may underestimate the knowledge state of the study group. Third, computation of a knowledge score based on correct answers to a set of questions is somewhat arbitrary, does not incorporate differential weightage that may be placed on different questions and has not been widely validated. Nevertheless, we feel that this score provides a fair estimate of the degree of knowledge of an individual. Fourth, the majority of study subjects consisted of men. This is partly related to the fact that women in Pakistan are less likely to accompany patients to the hospital; furthermore, when women were approached, if they were accompanied by other male members of the family, the latter would take the lead in answering questions. Thus women are under-represented in this study. Finally, the specialty of the specific outpatient clinic from where respondents were recruited was not recorded and, therefore, not adjusted for in the analysis.
Conclusion
In conclusion, this is the first study that has attempted to assess the state of CHD knowledge in a relatively diverse non-patient population in Pakistan. We found striking gaps in knowledge, particularly about the understanding of the nature CHD and its risk factors (physiologic factors like high blood pressure and elevated blood cholesterol in particular). In addition there was an equally significant lack of knowledge about common symptoms of CHD. These deficiencies in knowledge appear to translate into inadequate preventive behavior patterns. Factors significantly associated with knowledge included age, income, education level, residence, a family history of CHD and a past history of diabetes. An interesting association between knowledge and site of recruitment was noted in this study group which may be related to the number of public awareness seminars conducted by the site. This association deserves further investigation. Our study, despite some limitations, should raise strong concerns about the lack of knowledge and awareness about CHD amongst lay persons in Pakistan and should serve as a stimulus for establishing health education programs in the country.
Abbreviations
- AKU:
-
Aga Khan University Hospital
- PIMS:
-
Pakistan Institute of Medical Sciences
- Mayo:
-
Mayo Hospital
- AGH:
-
Allied General Hospital
- SD:
-
standard deviation.
- CHD:
-
coronary heart disease.
References
Lenfant C: Can we prevent cardiovascular diseases in low- and middle-income countries?. Bull World Health Organ. 2001, 79: 980-2; discussion 983-7.
Reddy KS, Yusuf S: Emerging epidemic of cardiovascular disease in developing countries. Circulation. 1998, 97: 596-601.
Pinto RJ: Risk factors for coronary heart disease in Asian Indians: clinical implications for prevention of coronary heart disease. Indian Journal of Medical Sciences. 1998, 52: 49-54.
Jafar TH, Levey AS, Jafary FH, White F, Gul A, Rahbar MH, Khan AQ, Hattersley A, Schmid CH, Chaturvedi N: Ethnic subgroup differences in hypertension in Pakistan. J Hypertens. 2003, 21: 905-912. 10.1097/00004872-200305000-00014.
Jafar TH, Jafary FH, S. J, Chaturvedi N: Heart Disease Epidemic in Pakistan: Women and men at equal risk. Am Heart J. 2005, 150.: 221-226. 10.1016/j.ahj.2004.09.025.
Ahmad K, Jafary FH, Jehan I, Hatcher J, Qayum A, Chaturvedi N, Jafar TH: Prevalence and predictors of smoking in Pakistan: Results of the National Health Survey of Pakistan. Eur J Cardiovasc Prev Rehabil. 2005, 12: 203-208. 10.1097/00149831-200506000-00003.
Ismail J, Jafar TH, Jafary FH, White F, Faruqui AM, Chaturvedi N: Risk factors for non-fatal myocardial infarction in young South Asian adults. Heart. 2004, 90: 259-263. 10.1136/hrt.2003.013631.
Rankin J, Bhopal R: Understanding of heart disease and diabetes in a South Asian community: cross-sectional study testing the 'snowball' sample method. Public Health. 2001, 115: 253-260.
Dodani S, Mistry R, Farooqi M, Khwaja A, Qureshi R, Kazmi K: Prevalence and awareness of risk factors and behaviours of coronary heart disease in an urban population of Karachi, the largest city of Pakistan: a community survey. J Public Health (Oxf). 2004, 26: 245-249. 10.1093/pubmed/fdh154.
Potvin L, Richard L, Edwards AC: Knowledge of cardiovascular disease risk factors among the Canadian population: relationships with indicators of socioeconomic status. Cmaj. 2000, 162: S5-11.
McKinley S, Dracup K, Moser DK, Ball K, Yamasaki K, Kim CJ, Barnett M: International comparison of factors associated with delay in presentation for AMI treatment. Eur J Cardiovasc Nurs. 2004, 3: 225-230. 10.1016/j.ejcnurse.2004.06.004.
Shea S, Stein AD, Basch CE, Lantigua R, Maylahn C, Strogatz DS, Novick L: Independent associations of educational attainment and ethnicity with behavioral risk factors for cardiovascular disease. Am J Epidemiol. 1991, 134: 567-582.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/5/124/prepub
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
FHJ, FA, HM, AW, MS, AA conceptualized this study and participated in the study design and manuscript writing and review. FA, HM, AW, MS, AA, MAQ were involved in the data collection process. FHJ performed the statistical analysis. JA, ISK and IH supervised the data collection process and also participated in manuscript review. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Jafary, F.H., Aslam, F., Mahmud, H. et al. Cardiovascular health knowledge and behavior in patient attendants at four tertiary care hospitals in Pakistan – a cause for concern. BMC Public Health 5, 124 (2005). https://doi.org/10.1186/1471-2458-5-124
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-5-124