
Abstract
Background
General and preventive health checks are a key feature of contemporary policies of anticipatory care. Ensuring high and equitable uptake of such general health checks is essential to ensuring health gain and preventing health inequalities. This literature review explores the socio-demographic, clinical and social cognitive characteristics of those who do and do not engage with general health checks or preventive health checks for cardiovascular disease.
Methods
An exploratory scoping study approach was employed. Databases searched included the British Nursing Index and Archive, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Database of Systematic Reviews (CDSR) and Database of Abstracts of Reviews of Effects (DARE), EMBASE, MEDLINE, PsycINFO and the Social Sciences Citation Index (SSCI). Titles and abstracts of 17463 papers were screened; 1171 papers were then independently assessed by two researchers. A review of full text was carried out by two of the authors resulting in 39 being included in the final review.
Results
Those least likely to attend health checks were men on low incomes, low socio-economic status, unemployed or less well educated. In general, attenders were older than non-attenders. An individual’s marital status was found to affect attendance rates with non-attenders more likely to be single. In general, white individuals were more likely to engage with services than individuals from other ethnic backgrounds. Non-attenders had a greater proportion of cardiovascular risk factors than attenders, and smokers were less likely to attend than non-smokers. The relationship between health beliefs and health behaviours appeared complex. Non-attenders were shown to value health less strongly, have low self-efficacy, feel less in control of their health and be less likely to believe in the efficacy of health checks.
Conclusion
Routine health check-ups appear to be taken up inequitably, with gender, age, socio-demographic status and ethnicity all associated with differential service use. Furthermore, non-attenders appeared to have greater clinical need or risk factors suggesting that differential uptake may lead to sub-optimal health gain and contribute to inequalities via the inverse care law. Appropriate service redesign and interventions to encourage increased uptake among these groups is required.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Anticipatory care [1] has increasingly been seen as a means by which the increasing demands of an aging population [2], growing numbers of people living with long term conditions, and persisting inequalities in health [3] may be addressed [4, 5]. A key feature of such approaches are general and preventive health checks, defined as interventions which include a physical examination and/or an assessment of demographic and lifestyle risk factors which assess an individual’s current health or predict their chance of developing illness in the future [6]. These may be carried out for primary and secondary preventive purposes, as part of annual routine health check-ups required among older age groups [7], or embedded opportunistically within routine clinical encounters [8].
Regular community based general health check-ups are important for the early identification of risk factors for conditions such as heart disease, diabetes and stroke [9], as evidenced in the recent introduction of Health Check within the United Kingdom (UK) National Health Service (NHS). The evidence base to support such health checks rests predominantly on the known efficacy of the individual screening components subsumed within them. For example, recent National Institute for Health and Clinical Excellence (NICE) guidance on the prevention of cardiovascular disease points to the known effectiveness of interventions within health checks in relation to risk assessment, smoking, and physical activity [10]. Such preventive health strategies may therefore also provide a cost effective way of dealing with the causes of ill health before they manifest into serious long-term conditions.
Despite the potential importance and benefit of such health checks, their uptake is known to be largely sub-optimal [11]. For example, data illustrating the implementation of the recent NHS Health Check in the UK has shown uptake rates of around 50% [12]. Furthermore, there is good reason to think that the pattern of uptake is likely to be differentially spread across socio-economic groupings and thus follow the inverse care law [13, 14]: those who have greatest to benefit from the services are least likely to engage with them. Differential uptake therefore has the potential to exacerbate health inequalities [14]. Consequently, knowledge of the socio-economic correlates of high and low uptake is important if current services are to be appropriately adapted in order to rectify such inequity.
Community based health-checks which aim to effectively and efficiently screen maximum proportions of eligible populations, are likely to be complex interventions consisting of numerous potential parameters: method of invite, location, timing, and nature (duration and content) of the screening process. Consequently, the development of new forms of health check should consider the theoretical and empirical basis to support maximal uptake [15, 16].
This exploratory scoping study aims to establish the nature and extent of current knowledge relating to the uptake and engagement with general health checks and preventative health checks for the risk factors of cardiovascular disease in particular, and thus contribute to the development of such a theoretical and empirical basis to informal future service development. In particular, it sought to address three fundamental questions:
-
1.
What are the socio-demographic characteristics of those who do and do not engage with health checks?
-
2.
What are their stated reasons for not attending health checks?
-
3.
What are the clinical needs and risk factors of these non-attenders?
Methods
Establishing the state of knowledge with regard to a number of important but general questions requires a broad and inclusive review type rather than a highly focussed systematic review targeting a highly specified question around effectiveness. Scoping studies as defined by Arksey and O’Malley provide a structured but less restrictive alternative to the traditional systematic review of the literature [17]. They discuss four potential uses for a scoping study:
-
1.
To examine the extent, range and nature of research activity
-
2.
To determine the value of undertaking a full systematic review
-
3.
To summarise and disseminate research findings
-
4.
To identify research gaps in the existing literature” p6 [17].
This literature review followed an iterative scoping process which incorporated these objectives. The methodology was selected over the systematic review as its purpose was to explore the broad state of knowledge regarding attendance at general health checks rather than answer a clearly defined question. The breadth of potential studies and their heterogeneous nature meant that a scoping study with a narrative synthesis providing comprehensive representation of the evidence was more appropriate.
Search strategy
A search of bibliographic databases did not identify any existing systematic review which focused specifically on this topic, and a decision was made to develop an alternative search strategy designed specifically for the project.
Types of studies
This review considered both quantitative and qualitative studies including, but not limited to: project evaluations, randomised controlled trials, cohort studies, experimental or quasi-experimental trials, uncontrolled trials, systematic reviews, meta-analyses and studies using evaluation methodology such as the theory of change. Inclusion and exclusion criteria were developed using the ‘population, intervention, comparison and outcome’ (PICO) acronym as a framework [18], and are detailed in Table 1. Differences in the delivery of health care systems may mean that findings from studies in underdeveloped countries may not be relevant to the context of this project. This resulted in the decision to restrict studies to developed countries. Similarly, studies where health insurance was not controlled for were excluded from the review. Findings were restricted to papers on general or preventive health checks for the risk factors of cardiovascular disease, as other disease specific screening programmes (for example breast screening) have their own intricacies with barriers which are better understood and findings which are not always transferable. Papers on geriatric annual health checks were excluded as these were less likely to be of a preventive nature due to the age group and focused more on functionality and ability to live independently than clinical or lifestyle risk factors. Some papers which were retrieved considered general health checks and disease specific screening within the same study. Therefore, papers were included if they contained both disease specific AND general heart health checks, but excluded if disease specific (other than heart/cardiovascular disease) screening was the main focus of the paper.
Databases used
The databases used for the review were the British Nursing Index and Archive, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Database of Systematic Reviews (CDSR) and Database of Abstracts of Reviews of Effects (DARE), EMBASE, MEDLINE, PsycINFO and the Social Science Citation Index (SSCI). A wide variety of databases were chosen to allow the complex concept of ‘uptake of services’ to be explored from a number of different disciplines. Searches were performed on each database individually to improve functionality and allow search terms and limits to be amended from the original template (Table 2) to meet each database’s specifications. Specific database search strategies and terms are available from the authors. Given that predictors of uptake are likely to change over time as cultures, values and services change, a judgement was made to exclude older studies. A subjective judgment was made to include papers published from 1996 onwards.
Selection process
The search and review procedure was conducted systematically and is outlined below with the initials of the researchers involved alongside:
-
Ran search in databases individually (RD)
-
Removed duplicates within databases (RD)
-
Removed duplicates between databases (RD)
-
Papers screened for relevance by title (RD)
-
Papers independently screened for relevance by abstract (RD and CM)
-
Meeting to discuss agreement (RD, CM, BW)
-
Remaining papers screened using full text (RD and BW)
Results
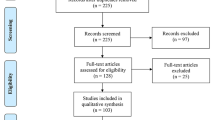
A total of 17,463 studies were returned after searching the databases and performing electronic de-duplication within and between each database; the breakdown of papers by database is shown in Table 3 and the identification and exclusion of papers throughout the process is shown in Figure 1. A total of 39 papers were included in the final review (See Table 4). The findings of the literature review are presented below using a narrative synthesis reflecting the Economic and Social Research Council guidance [19].

Flow diagram of review process.
What are the socio-demographic characteristics of those who do and do not engage with health checks?
Studies consistently indicate that males are less likely to engage with health checks or screening and to endorse periodic health examinations than females [20–28]. This difference in rates of non-attendance between males and females ranged from 8% to 19% in those invited for a health check at General Practice [21, 23, 24]. In community based drop-in sessions, women were more likely to self-present than males, with the proportion of attenders at least 60-65% female [20, 22]. Additionally, 11% of men compared to 6% of women did not endorse periodic health examinations [28]. Two other studies found no difference in attendance rates by gender [29, 30].
In general, attenders at health checks are older than non-attenders [20–23, 25, 31–35], although some studies found no association between age and attendance [29, 30, 36–39]. In many cases the demographics of engagers were dependent on the targeting strategy of the intervention; for example where the service was only offered to a particular age group. Some of the included studies were targeted specifically at older adults while others were offered to an entire adult practice population. Although there was a tendency for attenders to be older than non-attenders, the heterogeneous nature of the study methodologies meant that it was difficult to define an optimum age for uptake. Indeed, the relationship between age and participation may not be linear. For example, participation in a health examination after completion of a health interview in the Netherlands followed a curve which rose with increasing age until 60 then declined significantly with any age above this [40].
Individuals were found to be less likely to attend if they had low socio-economic status [23, 33, 34, 36, 38, 40, 41]. Defining which socio-economic/demographic characteristics differentiate between attenders and non-attenders was complicated by the numerous ways social status was reported in the literature. Some studies discussed social class, employment status, occupational training and level of education or years spent in education independently; whilst others used the terms interchangeably or as proxy measures for each other. In general lower uptake was associated with low incomes [21, 30–32, 42], being unemployed [38, 41, 42] and lower educational attainment [22, 25, 27, 31–34, 41]. Although these terms may be closely related, one study found that each had an independent effect on the attendance rate [34].
An individual’s marital status was found to affect attendance rates with non-attenders more likely to be single [21, 23, 24, 35, 36, 42]. Studies suggested a possible interaction between marital status and gender in explaining uptake. For example, a number of studies reported that attendance at health checks was higher in males who were married or cohabiting, compared to single males [21, 24, 35, 42–44]. A possible explanation was proposed in a qualitative study using focus groups with participants and non-participants in community health screenings, which found that the decision to attend a screening is often made by the partner, with this initiation behaviour prevalent across a number of socio-demographic factors [45].
The tendency of women to present more than men (as evidenced earlier) persists regardless of marital status. Higher rates of attendance in women who were single, divorced or widowed (79%) were found compared to men with equivalent marital status (65%). Furthermore, the rates of attendance were 88% in married women and 84% in married men, indicating that being married appears to have a stronger effect on uptake in men [24]. Other studies have found no relationship between marital status and attendance rates [39, 41, 46].
In general, white individuals were more likely to engage with preventive health services than individuals from other ethnic backgrounds [22, 31, 38, 40, 46]. However, ethnicity was only reported in a small proportion of the studies (Seven of 39 papers). Only one of these reported no difference according to race [39]. One paper reported a higher proportion of non-attenders at registration health checks were of African origin [38]. On the other hand, a large American survey (n = 4879) found that 9.6% of white people did not believe in periodic health examinations compared to 3.4% of black people, and that black people were more likely to have been screened for cholesterol in the past 5 years than white people [28].
What are patients' reasons for not attending preventative health checks?
The relationship between social cognitive factors and attendance behaviour was not straightforward as although health beliefs were found to affect uptake [47], the factors influencing the decisions of attenders and non-attenders may not necessarily reflect “opposite motivations of beliefs” [48]. To clarify, this meant that attenders may present for screening to reduce the fear or perceived danger of a condition, while non-attenders may have used the same rationale to not present, e.g. they did not feel at risk or were too frightened of the possible outcome if they did attend.
Despite this caveat, non-attenders were shown to value health less strongly, have lower self-efficacy, feel less in control of their health and be less likely to believe in the efficacy of screening [39, 49]. Components of the health belief model were identified as significant predictors, with those who did not engage with services less likely to feel susceptible to ill health or perceive the conditions being screened for as serious as those who attended [25, 30, 48].
Individuals may present in response to symptoms, a family history of the condition [29], or to seek reassurance [50]. Others are simply interested in their health, seek confirmation of a previous reading/monitor an existing condition or are worried well [20, 22, 45]. Those who do not present may have no perceived need for a health check: they may feel healthy or have an absence of symptoms [27, 33, 51, 52], are already in contact with the health service [27, 33, 41, 51, 53], or have recently had a health check [27, 51, 54]. Alternatively, they are aware they are unhealthy and do not want to be told off and have to make lifestyle changes, or have a fear of what it might find [26, 28, 31, 47, 51].
Fear acted as a barrier to uptake of screening in a number of ways, including: a fear of what the health check might find [33, 52, 55], the belief that “what I don’t know won’t hurt me” [45] and that knowing wouldn’t make them any happier [51], or the fear of the test results [25, 45] and their consequences [51]. Concerns related to the procedure itself were also apparent in relation to a fear of needles or a general fear of doctors or medical settings, anxiety about what the tests might involve [45, 47] or the experience level of those carrying out the tests [45].
What are the clinical needs and risk factors of those who present for health checks?
Non-attenders had a greater proportion of cardiovascular risk factors than attenders. Smokers were less likely to attend than non-smokers [21, 23, 25, 27, 32, 33, 36, 38, 42, 46, 56]. Unhealthy lifestyle factors were important predictors of non-attendance, with odds ratios higher for smokers, heavy drinkers, and those with unhealthy diets and the obese [36]. However, one paper showed occasional smokers and ex-smokers were more likely to receive a check-up than non-smokers [21] and smokers with the intention of giving up were more likely to attend than those who did not want to [23].
A personal history but not family history of coronary heart disease (CHD) was significantly more common in non-attenders, as was a higher body mass index (BMI) [34], high cholesterol, systolic and diastolic blood pressure values [33].
Follow up of non-participants in a prospective study of cardiovascular disease found that this group were more likely to have died than participants in the three years following the health checks. The difference in the mortality rates between participants and non-participants was biggest in the youngest age group (40–44 year olds), indicating premature death. However, the mortality rates were not significantly different between these groups for cardiovascular disease or cancer [35].
The vast majority of studies supported the higher risk profile of non-attenders; however, non-attenders were found to have lower levels of cholesterol than those who did attend in a post-study follow up [32]. In another study initial responders had higher total cholesterol but lower diastolic blood pressure than those who had to be re-contacted [24].
In general, frequent or recent consulters at General Practice were found to be more likely to present for a health check [23, 32, 36, 40, 41, 44] but for some people this recent or on-going contact can be a reason not to attend [27, 42, 51, 57]. Consequently, this inconsistent relationship between frequency of attendance at GP practice and the likelihood of participation in preventive health screening has been described as ‘complex’ [40], and the two areas are inherently related. Some studies have shown that frequent or recent GP consulters are more likely to attend for a health check [23, 32, 36, 40, 41, 44]; for example, over 90% of patients who attended a health check at a shopping centre reported having a regular source of medical care [22]. Conversely, other patients cited recent or ongoing contact with their GP as reasons for not attending a health check [27, 42, 51, 57]. A survey of attenders and non-attenders at General Practice in the past year showed that attenders were more likely to indicate that they would make an appointment for a health check compared to non-attenders (83% v 66%) [58].
Discussion
This review identified a substantial number of primary empirical studies contributing data to questions of uptake. Although the heterogeneous nature of interventions and populations precluded formal statistical meta-analysis, there appeared sufficient commonality across studies to inform a number of key conclusions. Routine health check-ups appear to be taken up inequitably with gender, age, socio-demographic status and ethnicity all associated with differential service use. Furthermore, non-attenders appeared to have greater clinical need or risk factors suggesting that differential uptake may lead to sub-optimal health gain and contribute to inequalities via the inverse care law. Our findings provide an initial contribution to the development of programme theories or conceptual frameworks to underpin future strategies, as suggested by NICE and others [59, 60].
Limitations of the review
Established and appropriate search strings were not available thus necessitating the development of new strategies. Like all reviews we cannot guarantee that studies have not been missed. However, our emphasis was on sensitivity over specificity resulting in almost 18,000 papers being examined by members of the team. We therefore believe that it is likely that few papers were missed. The purpose of the review was to identify sufficient studies across diverse contexts to inform the theoretical and practical development of future interventions to improve uptake of health checks. This necessary focus on diversity also meant that formal statistical meta-analysis or meta-regression of predictors of uptake would have been inappropriate.
The majority of studies came from North America (n = 13) and Europe (n = 24), and the remaining two papers were from Israel and Taiwan. There may have been benefits from loosening inclusion criteria to include both geriatric health checks and non-developed countries. Such diversity could potentially lead to sufficient numbers of papers with common interventions or populations as to justify a number of meta-analyses of effectiveness or meta-regression of predictors of uptake. While the scoping nature of this study precluded such an approach for pragmatic reasons we have demonstrated that such a review may be feasible and desirable in the future.
The inverse care law in operation
In his original description of the inverse care law Julian Tudor Hart’s argued that “the availability of good medical care tends to vary inversely with the need for the population served” [14]. The validity of his law was demonstrated in a number of studies and in a number of ways in our review. Men from lower socio-economic backgrounds and on low incomes were consistently found to be less likely to engage with check-ups than women or people from a higher socio-economic status. Both of these variables are well established risk factors for a range of clinical conditions, perhaps most importantly in the context of this study, cardiovascular disease. This, again, was reinforced through this review since non-attenders were consistently found to have a range of poor lifestyle behaviours including smoking, alcohol consumption and diet. These findings suggest that without adaptation or increased efforts to increase uptake from these more “needy” populations there is the possibility that health checks, like other contemporary public health policies, risk exacerbating rather than narrowing health inequalities [61].
Implications for future service design
Given the diversity of populations, clinical needs and motives not to attend health checks, a “one size fits all” solution consisting of promoting attendance at health checks and subsequent support for behaviour change is simplistic and flawed, particularly in the interaction with patients with complex needs [62]. Indeed, the current focus on a limited number of delivery types, and a failure to tailor services may at least in part contribute to the problem. However, while it would appear sensible to assume that complex problems require complex solutions, there may be exceptions. The increasing role of both social marketing and financial incentives as drivers of behaviour change both focus on increasing perceived value while not essentially changing the service itself or addressing many of the pre-stated barriers. Incentive based schemes are gaining significant attention as a means of promoting behaviour change through extrinsic motivations [63–65]. However, such schemes have led to a number of questions with regard to political acceptability, ethical justification and effectiveness. In addition, questions over their ability to sustain behaviour modification, once an incentive is withdrawn, were raised [64]. Given the preponderance of people on lower incomes among non-attenders, incentive schemes, whether based on finance or benefits in kind, may prove particularly effective and could be considered.
If tailoring of health check-ups is to take place then consideration would need to be given to the varied demands that this would place on health professionals charged with delivering the service. Among the challenges surrounding service delivery are clinician’s frequently low adherence to protocols on prevention within consultations [66–68]. This may be related to a lack of awareness of, and agreement with, guidelines, or a belief that many practices and outcomes would be difficult to change due to time pressure and other issues [69, 70].
Moreover, clinicians in deprived communities are faced with higher rates of ill health and multi-morbidities, poor patient access, and high stress levels among clinicians, which in turn lead to higher demands on the service and service provider [71]. Diversifying the provision of health checks to multiple tailored forms may well exacerbate these pressures and reduce service compliance to such new protocols unless tailoring is largely cost and time neutral. Certainly, increasing intervention complexity may be associated with reduced levels of implementation. An alternative approach may be to provide increased emphasis on opportunistic health checks at routine consultations; although even this has still been found to be time consuming [8]. However, it has recently been suggested from a substantive evaluation of a complex outreach prevention service that the complexity of reasons for non-engagement among some people may not be predictable or “read in advance” [59]; this would suggest that whatever tailoring to services is made there will always be an imperative on the skill of the clinician to judge and respond to unique opportunities within the opportunistic consultation as well as wider systems approaches [59].
Conclusion
All of these challenges and complexities indicate that a diverse range of approaches may be required if the full benefit of health checks are to be realised. While tailoring and targeting the form of delivery may have a role to play, it is likely that their implementation would require increased investment to ensure adoption and sustainability, particularly if narrowing health inequalities is a serious and central goal of such health checks. The Marmot report “Fairer Society Fairer Lives”, recently argued for a policy of “proportionate universalism”:
“Focusing solely on the most disadvantaged will not reduce health inequalities sufficiently. To reduce the steepness of the social gradient in health, actions must be universal, but with a scale and intensity that is proportionate to the level of disadvantage. We call this proportionate universalism.” p15 [72].
Such proportionate universalism would define “tailoring” as much in terms of the scale and intensity of action required for those most in need, as much as any changes in objective intervention form. Whatever approach is adopted, it is important that a clear theoretical underpinning that acknowledges both the complexity of the diverse population needs/attitudes and the challenges currently facing primary care and associated public health services is required. This synthesis of current findings has attempted to make a contribution to such a development.
References
Van den Dool C: Allgemeinmedizin. International. 1973, 3: 100-
Riley JC: Rising life expectancy: A global history. 2001, Cambridge: Cambridge University Press
Hanlon P, Walsh D, Buchanan D, Redpath A, Bain M, Brewster D, Chalmers J, Muir R, Smalls M, Willis J, et al: Chasing the Scottish effect: Why Scotland needs a step-change in health if it is to catch up with the rest of Europe. 2001, Glasgow: Public Health Institute of Scotland/Information and Statistics Division
Scottish Executive Health Department: Building a health service fit for the future - A national framework for service change in the NHS in Scotland. 2005, Edinburgh: The Scottish Executive
The Scottish Government: Better health, better care: Action plan. 2007, Edinburgh: The Scottish Government
The Scottish Government: Equally well: Report of the ministerial task force on health inequalities. 2008, Edinburgh: The Scottish Government
Delivering the NHS health check: A practical guide to implementation. http://www.healthcheck.nhs.uk/Library/F26E1C01d01.pdf,
Watt G, O’Donnell C, Sridharan S: Building on Julian Tudor Hart’s example of anticipatory care. Primary Health Care Research and Development. 2011, 12 (1): 3-10. 10.1017/S1463423610000216.
U.S. Preventive Services Task Force: Guide to clinical preventive services. 2004, Rockville: Agency for Healthcare Research and Quality
National Institute for Health and Clinical Excellence: Prevention of cardiovascular disease (PH25). 2010, London: National Institute for Health and Clinical Excellence
Over-40s health check provision in England ‘patchy. http://www.bbc.co.uk/news/health-16137013,
NHS health check national learning network 13th workshop. http://www.healthcheck.nhs.uk/Library/DHupdateonlyMarch2012v12.ppt,
Dalton ARH, Bottle RA, Okoro C, Majeed FA, Millett C: Uptake of the NHS health checks programme in a deprived, culturally diverse setting: cross sectional study. J Epidemiol Community Health. 2011, 65: A21-
Tudor Hart J: The inverse care law. Lancet. 1971, 297 (7696): 405-412. 10.1016/S0140-6736(71)92410-X.
Medical Research Council: A framework for development and evaluation of RCTs for complex interventions to improve health. 2000, London: Medical Research Council
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M: Developing and evaluating complex interventions: the new medical research council guidance. BMJ. 2008, 337: 1655-10.1136/bmj.a1655.
Arksey H, O’Malley L: Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. 2005, 8 (1): 19-32. 10.1080/1364557032000119616.
Richardson WS, Wilson MC, Nishikawa J, Hayward RS: The well-built clinical question: a key to evidence-based decisions. ACP J Club. 1995, 123 (3): A12-A13.
Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, Britten N, Roen K, Duffy S: Guidance on the conduct of narrative synthesis in systematic reviews. A product from the esrc methods programme. 2006, Lancaster; Institute of Health Research: ESRC Methods Program
Bletzer KV: Review of a health fair screening program in Mid-Michigan. J Community Health. 1989, 14 (3): 149-157. 10.1007/BF01324364.
Culica D, Rohrer J, Ward M, Hilsenrath P, Pomrehn P: Medical checkups: who does not get them?. Am J Public Health. 2002, 92 (1): 88-91. 10.2105/AJPH.92.1.88.
Greenland P, Hildreth NG, Maiman LA: Attendance patterns and characteristics of participants in public cholesterol screening. Am J Prev Med. 1992, 8 (3): 159-164.
Waller D, Agass M, Mant D, Coulter A, Fuller A, Jones L: Health checks in general practice: another example of inverse care?. BMJ. 1990, 300 (6732): 1115-1118. 10.1136/bmj.300.6732.1115.
Jacobsen BK, Stensvold I, Fylkesnes K, Kristiansen IS, Thelle DS: The Nordland health study - design of the study, description of the population, attendance and questionnaire response. Scand J Soc Med. 1992, 20 (3): 184-187.
Simpson WM, Johnston M, McEwan SR: Screening for risk factors for cardiovascular disease: a psychological perspective. Scott Med J. 1997, 42 (6): 178-181.
Thomas KJ, Nicholl JP, Fall M, Lowy A, Williams BT: Case against targeting long term non-attenders in general practice for a health check. Br J Gen Pract. 1993, 43 (372): 285-289.
Wall M, Teeland L: Non-participants in a preventive health examination for cardiovascular disease: characteristics, reasons for non-participation, and willingness to participate in the future. Scand J Prim Health Care. 2004, 22 (4): 248-251. 10.1080/02813430410006611.
Cherrington A, Corbie-Smith G, Pathman DE: Do adults who believe in periodic health examinations receive more clinical preventive services?. Prev Med. 2007, 45 (4): 282-289. 10.1016/j.ypmed.2007.05.016.
Karwalajtys T, Kaczorowski J, Chambers LW, Levitt C, Dolovich L, McDonough B, Patterson C, Williams JE: A randomized trial of mail vs. telephone invitation to a community-based cardiovascular health awareness program for older family practice patients [ISRCTN61739603]. BMC Fam Pract. 2005, 6: 35-10.1186/1471-2296-6-35.
Hsu HY, Gallinagh R: The relationships between health beliefs and utilization of free health examinations in older people living in a community setting in Taiwan. J Adv Nurs. 2001, 35 (6): 864-873. 10.1046/j.1365-2648.2001.01924.x.
Bowden RG: Comparisons of cholesterol screening participants and non-participants in a university setting. International Electronic Journal of Health Education. 2001, 4: 100-104.
Franks P, Gold MR, Bell BP, Naumburg EH, Engerman J: Barriers to cholesterol testing in a rural-community. J Fam Pract. 1991, 32 (6): 614-618.
Jones A, Cronin PA, Bowen M: Comparison of risk factors for coronary heart disease among attenders and non-attenders at a screening programme. Br J Gen Pract. 1993, 43 (374): 375-377.
Sonne-Holm S, Sorensen TIA, Jensen G, Schnohr P: Influence of fatness, intelligence, education and sociodemographic factors on response rate in a health survey. J Epidemiol Community Health. 1989, 43 (4): 369-374. 10.1136/jech.43.4.369.
Walker M, Shaper AG, Cook DG: Non-participation and mortality in a prospective study of cardiovascular disease. J Epidemiol Community Health. 1987, 41 (4): 295-299. 10.1136/jech.41.4.295.
Thorogood M, Coulter A, Jones L, Yudkin P, Muir J, Mant D: Factors affecting response to an invitation to attend for a health check. Journal of Epidemioogy and Community Health. 1993, 47 (3): 224-228. 10.1136/jech.47.3.224.
Dignan MB, Young LD, Crouse JR, King JM: Factors associated with participation in a preventive cardiology service by patients with coronary heart disease. South Med J. 1995, 88 (10): 1057-1061. 10.1097/00007611-199510000-00011.
Griffiths C, Cooke S, Toon P: Registration health checks: inverse care in the inner city?. Br J Gen Pract. 1994, 44 (382): 201-204.
Wilson S, Sisk RJ, Baldwin KA: Health beliefs of blue collar workers: increasing self efficacy and removing barriers. AAOHN J. 1997, 45 (5): 254-257.
Boshuizen HC, Viet AL, Picavet HSJ, Botterweck A, Van Loon AJM: Non-response in a survey of cardiovascular risk factors in the Dutch population: determinants and resulting biases. Public Health. 2006, 120 (4): 297-308. 10.1016/j.puhe.2005.09.008.
Pill R, French J, Harding K, Stott N: Invitation to attend a health check in a general practice setting: comparison of attenders and non-attenders. J R Coll Gen Pract. 1988, 38 (307): 53-56.
Persson LG, Lindstrom K, Lingfors H, Bengtsson C: A study of men aged 33–42 in Habo, Sweden with special reference to cardiovascular risk-factors. Scand J Soc Med. 1994, 22 (4): 264-272.
Christensen B: Characteristics of attenders and non-attenders at health examinations for ischaemic heart disease in general practice. Scand J Prim Health Care. 1995, 13 (1): 26-31. 10.3109/02813439508996731.
Difford F, Telling JP, Davies KR: Continuous opportunistic and systematic screening for hypertension with computer help: analysis of non-responders. BMJ. 1987, 294 (6580): 1130-1132. 10.1136/bmj.294.6580.1130.
Engebretson J, Mahoney JS, Walker G: Participation in community health screenings: a qualitative evaluation. J Community Health Nurs. 2005, 22 (2): 77-92. 10.1207/s15327655jchn2202_2.
Harpole LH, McBride C, Strigo TS, Lobach D: Feasibility of a tailored intervention to improve preventive care use in women. Preventive Medicine: An International Journal Devoted to Practice and Theory. 2000, 31 (4): 440-446.
Norman P, Fitter M: Predicting attendance at health screening: organizational factors and patients’ health beliefs. Counselling Psychology Quarterly. 1991, 4 (2–3): 143-155.
Shiloh S, Vinter M, Barak Z: Correlates of health screening utilization: the roles of health beliefs and self-regulation motivation. Psychol Health. 1997, 12 (3): 301-317. 10.1080/08870449708406709.
Norman P, Conner M: The role of social cognition models in predicting attendance at health checks. Psychol Health. 1993, 8 (6): 447-462. 10.1080/08870449308400448.
Norman P, Fitter M: Patients’ views on health screening in general practice. Fam Pract. 1991, 8 (2): 129-132. 10.1093/fampra/8.2.129.
Nielsen KDB, Dyhr L, Lauritzen T, Malterud K: “You can’t prevent everything anyway”: a qualitative study of beliefs and attitudes about refusing health screening in general practice. Fam Pract. 2004, 21 (1): 28-32. 10.1093/fampra/cmh107.
Norman P, Fitter M: Intention to attend a health screening appointment: some implications for general practice. Counselling Psychology Quarterly. 1989, 2 (3): 261-272. 10.1080/09515078908256682.
Williams A, Mason A, Wold J: Cultural sensitivity and day care workers: examination of a worksite based cardiovascular disease prevention project. AAOHN J. 2001, 49 (1): 35-43.
Ornstein SM, Musham C, Reid A, Jenkins RG, Zemp LD, Garr DR: Barriers to adherence to preventive services reminder letters: the patient’s perspective. J Fam Pract. 1993, 36 (2): 195-200.
Pill R, Stott N: Invitation to attend a health check in a general practice setting: the views of a cohort of non-attenders. J R Coll Gen Pract. 1988, 38 (307): 57-60.
Thompson NF: Inviting infrequent attenders to attend for a health check: costs and benefits. Br J Gen Pract. 1990, 40 (330): 16-18.
Hegarty V, Donovan MC, Pye M, Khaw KT: Reasons for nonresponse among older adults. J Am Geriatr Soc. 1995, 43 (9): 1066-1067.
Levine JA: Are patients in favour of general health screening?. J R Soc Med. 1991, 84 (5): 280-283.
Mackenzie M, Turner F, Platt S, Reid M, Wang Y, Clark J, Sridharan S, O’Donnell CA: What is the ‘problem’ that outreach work seeks to address and how might it be tackled? Seeking theory in a primary health prevention programme. BMC Health Serv Res. 2011, 11 (350):
Pawson R: Evidence based policy: the promise of ‘realist synthesis’. Evaluation. 2002, 8 (3): 340-358. 10.1177/135638902401462448.
Watt G: The inverse care law today. Lancet. 2002, 9328: 252-254.
Watt G: Anticipatory care in very deprived areas. Br J Gen Pract. 2011, 61 (584): 228-10.3399/bjgp11X561401.
Marteau TM, Ashcroft RE: Using financial incentives to achieve healthy behaviour. BMJ. 2009, 338: 983-985. 10.1136/bmj.b983.
Wilkinson E: Can you pay people to be healthy?. Lancet. 2008, 371 (9621): 1325-1326. 10.1016/S0140-6736(08)60578-4.
Wilkinson RG, Pickett KE: The spirit level: why more equal societies almost always do better. 2009, London: Penguin
Backer EL, Geske JA, McIlvain HE, Dodendorf DM, Minier WC: Improving female preventive health care delivery through practice change: an every woman matters study. J Am Board Fam Med. 2005, 18: 401-108. 10.3122/jabfm.18.5.401.
Hunt WA, Matarazzo JD, Weiss SM, Gentry WD: Associative learning, habit, and health behavior. Journal Of Behavioral Medicine. 1979, 2 (2): 111-124. 10.1007/BF00846661.
Dubey V, Mathew R, Iglar K, Moineddin R, Glazier R: Improving preventive service delivery at adult complete health check-ups: the preventive health evidence-based recommendation form (PERFORM) cluster randomized controlled trial. BMC Fam Pract. 2006, 7 (44):
Hudon E, Beaulieu MD, Roberge D: Integration of the recommendations of the Canadian task force on preventive health care. Fam Pract. 2004, 21: 11-17. 10.1093/fampra/cmh104.
Yarnall KS, Pollak KI, Ostbye T, Krause KM, Michener JL: Primary care: is there enough time for prevention?. Am J Public Health. 2003, 93 (4): 635-641. 10.2105/AJPH.93.4.635.
Mercer SW, Watt GC: The inverse care law: clinical primary care encounters in deprived and affluent areas of Scotland. Ann Fam Med. 2007, 5 (6): 503-510. 10.1370/afm.778.
Marmot M, Allen J, Goldblatt P, Boyce T, McNeish D, Grady M, Geddes I: Fair society, Healthy Lives: Strategic Review of Health Inequalities in England post-2010. 2010, London: The Marmot Review
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/12/723/prepub
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
RD designed the study, conducted the review and contributed to the writing of the paper. BW was involved in the design of the study and wrote the paper. CMC contributed to the review and the paper. MTH contributed to the review and the paper. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Dryden, R., Williams, B., McCowan, C. et al. What do we know about who does and does not attend general health checks? Findings from a narrative scoping review. BMC Public Health 12, 723 (2012). https://doi.org/10.1186/1471-2458-12-723
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-12-723