
Abstract
Background
Antimicrobial resistance is one of the most challenging issues in modern medicine.
Methods
We evaluated the secular trends of the relative frequency of blood isolates and of the pattern of their in vitro antimicrobial susceptibility in our hospital during the last four and a half years.
Results
Overall, the data regarding the relative frequency of blood isolates in our newly founded hospital do not differ significantly from those of hospitals that are functioning for a much longer period of time. A noteworthy emerging problem is the increasing antimicrobial resistance of Gram-negative bacteria, mainly Acinetobacter baumannii and Klebsiella pneumoniae to various classes of antibiotics. Acinetobacter baumannii isolates showed an increase of resistance to amikacin (p = 0.019), ciprofloxacin (p = 0.001), imipenem (p < 0.001), and piperacillin/tazobactam (p = 0.01) between the first and second period of the study.
Conclusion
An alarming increase of the antimicrobial resistance of Acinetobacter baumannii isolates has been noted during our study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Increasing antimicrobial resistance among bloodstream isolates is considered a significant problem worldwide [1, 2]. This is especially true in some areas including the countries of Southern Europe where a considerable proportion of pathogens are resistant to antibiotics of several classes [3]. Although antimicrobial resistance is noted in all pathogens, some phenotypes of resistance such as methicillin resistant Staphylococcus aureus (MRSA), vancomycin resistant enterococci (VRE), methicillin resistant coagulase negative staphylococci (MRCNS), and carbapenem resistant enterobacteriacae, Pseudomonas aeruginosa, and Acinetobacter baumannii are of particular concern. We sought to study the secular trends of the relative frequency and antimicrobial resistance of blood isolates in a newly founded hospital in Greece.
Methods
Patient population
The patient population comprised of patients admitted to Henry Dunant Hospital, Athens, Greece in the period of 01/01/2001–30/06/2005. Henry Dunant Hospital was founded in October 2000. It is a general tertiary hospital with 450 beds covering most medical specialties with the exception of pediatrics, obstetrics, and transplant surgery. It has 3 combined medical and surgical intensive care units with a total of 38 beds.
Microbiological studies
Identification of the microorganisms to the species level was performed with the automated system Vitek 2 (Biomérieux) according to the manufacturer's instructions. Not all, but only the first blood isolate per patient was included in the study. The Bactec system (Becton-Dickinson) was used during 2001, 2002, and 2003, and the BacT Alert 3D (Biomérieux) was used during 2004 and 2005. Isolation of bacteria was followed by susceptibility testing that was performed with the Vitek 2 system, applying the criteria suggested by the Clinical and Laboratory Standards Institute (CLSI) [4, 5]. The identification and antimicrobial susceptibility of viridans Streptococci was preformed by the use of API (BioMérieux) and the use of the Kirby-Bauer method. Fungi were identified with the use of the specific card for the Vitek 2 system. Susceptibility to colistin was tested by the Vitek method and the E-test. Pulsed field gel electrophoresis and ribotyping were not performed to exclude secondary outbreak strains.
Statistical analysis
Differences in proportions were compared by x2 test or Fisher's exact test where appropriate. Statistical significance was set for p < 0.05. All statistical analyses were performed using SPSS 11.0 and S-PLUS 6.1 Professional.
Results
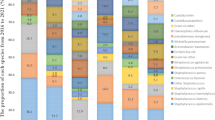
The frequency of isolation of bacteria from cultures of blood specimens was 182 per 12,593 admissions during 2001 (14.4 per 1,000 admissions), 507 per 25,865 admissions during 2002 (19.6 per 1,000 admissions), 693 per 30,597 admissions during 2003 (22.6 per 1,000 admissions), 566 per 30,599 admissions during 2004 (18.4 per 1,000 admissions) and 208 per 15,683 admissions during 2005 (13.2 per 1,000 admissions). There was a significant difference in the proportion of isolates identified over the 5year period (p < 0.001). The percentage of positive blood cultures to the total number of blood cultures was 4.84% for the year 2001, 6.46% for 2002, 7.91% for 2003, 6.71% for 2004 and 5.7% for 2005. Regarding the relative frequency of the bacteria isolated from blood specimens, Gram-positive bacteria were more common than Gram-negative bacteria throughout the study period (Table 1). Coagulase negative staphylococci were the commonest blood isolates (52.5 % of total). The relative frequency of other Gram-positive and Gram-negative microorganisms was the following, in descending order: Escherichia coli (8.9 %), Staphylococcus aureus (5.9 %), Pseudomonas aeruginosa (5.2 %), Klebsiella spp (4.8 %), Acinetobacter baumannii (4.1 %), Enterococcus faecalis (2.2 %), and Enterococcus faecium (1.8 %). In Table 2 we summarized the relative frequency of blood isolates by service, namely wards and intensive care unit.
We compared the antimicrobial resistance of blood isolates of two periods: the first period was 1/1/2002–31/12/2003 and the second period 1/1/2004–30/6/2005. The year 2001 was not included in the comparison of the antimicrobial resistance because the in vitro susceptibility data were not readily available. The antimicrobial resistance of Gram-negative bacteria isolated from blood in our hospital showed some interesting trends (Table 3). In Table 4 we present data regarding the in vitro susceptibility patterns and the respective MIC90 of the isolated bacteria. Acinetobacter baumannii isolates showed an increase of resistance to amikacin (p = 0.019), ciprofloxacin (p = 0.001), imipenem (p < 0.001), and piperacillin/tazobactam(p = 0.01) between the first and second period of the study. In addition, we noted the appearance of resistance to polymyxins in one Acinetobacter baumannii isolate. Regarding the secular changes of the antimicrobial resistance of Pseudomonas aeruginosa isolates during our study, there was only one statistically significant association, namely increased resistance to ceftazidime (p = 0.016).
The antimicrobial susceptibility pattern of Klebsiella pneumoniae isolates changed significantly during our study. Increased resistance of Klebsiella pneumoniae isolates was noted for all beta lactams tested [specifically to piperacillin/tazobactam (p < 0.001), ceftazidime (p = 0.01), cefepime (p < 0.001), cefoxitin (p < 0.001) and meropenem (p < 0.001)] between the first and second period of the study. There was also increased resistance of Klebsiella pneumoniae to ciprofloxacin (p = 0.006) and tobramycin (p < 0.001).
Regarding the antimicrobial susceptibility pattern of Gram-positive bacteria during our study there was a considerable proportion of staphylococci with resistance against oxacillin (Table 1); however, the difference of the proportions of oxacillin resistant staphylococci between the two study periods was not statistically significant (Table 2). We did not isolate any staphylococci with resistance to vancomycin. Enterococcus faecalis and Enterococcus faecium were generally susceptible to vancomycin although some strains were resistant; however the difference of the proportions of VRE between the two study periods was not statistically significant (Table 2).
Discussion
Patients with bacteremia have remained a challenge to treat. Knowledge of the hospital epidemiology and antimicrobial susceptibility pattern of blood isolates helps physicians to effectively manage blood stream infections. This is because considerable differences of the frequency of blood isolates are reported even from hospitals of similar size and mixture of patients of the same country [6].
In this study we evaluated the secular trends of the relative frequency and antimicrobial resistance of blood isolates in a newly founded Greek hospital. Gram-positive microorganisms are the most common blood isolates. Among them, coagulase negative staphylococci are the commonest blood isolates. The percentage of coagulase negative staphylococci (%) is higher in our study than that reported in large series (31.6%) [7–9]. It is possible that the proportion of coagulase negative staphylococci that were contaminants was considerable in our study. The interpretation of blood cultures that are positive for coagulase negative staphylococci has inherent difficulties and requires careful reasoning [10]. The observed relative frequency of MRSA was considerable high during the studied period. Data from the WHONET Greece (antimicrobial surveillance system) regarding the period from January 2005 through June 2005 showed that a significant proportion of S. aureus blood isolates are resistant to methicillin (MRSA strains). Specifically, 32.6%, 55.6%, and 69% of S. aureus blood isolates from medical wards, surgical wards, and ICUs respectively were MRSA.
In general, our results about the relative frequency of blood isolates in our newly founded hospital are not substantially different from those of hospitals that are functioning for a much longer period of time. Similar data have been reported in studies performed in hospitals elsewhere in Europe as well as in North America [7–9]. An explanation may be that it is not the microbial ecology of the structure (our newly founded tertiary urban hospital compared to hospitals that are functioning for longer time) but rather the characteristics of the admitted patients like comorbidity, medications, and other host factors that play the most important role in the relative frequency of blood isolates.
It is also noteworthy that the isolation of Candida spp from the blood was not uncommon during the study period. This is in agreement with the reports from all over the world regarding a considerable prevalence of fungemia due to extensive use of antibiotics, aggressive treatment of neoplastic disease, an expanding population of patients with AIDS with prolonged survivors, use of indwelling devices for ICU monitoring, and many other factors that predispose to fungal infections [8, 9]. Although our hospital does not have a transplant unit, the observed high frequency of Candida isolates is probably explained by the fact that oncology patients and thus neutropenic patients constitute a significant portion of our patients.
We also evaluated in our study the trends of the antimicrobial resistance of the blood bacteria isolates in our newly founded hospital. The antimicrobial resistance of Acinetobacter baumannii showed an alarming increase during the study. Acinetobacter baumannii remained susceptible to colistin during the two periods, although the recovery of one resistant strain is of note [11, 12]. Unfortunately, antimicrobial resistance increased also for Klebsiella pneumoniae for all of the 7 antibiotics it was tested for. These results are in concordance with data of the literature about the increasing antimicrobial resistance of Gram-negative bacteria [13–15]. In addition, it is noteworthy that the majority of bloodstream K. pneumoniae strains recovered in 2005 were resistant to meropenem, however this would probably reflect a nosocomial outbreak of a carbapenem-resistant K. pneumoniae clone.
We should acknowledge several limitations of our study. First, the results obtained from the Vitek II were confirmed by the E-test methodology only for colistin. Second, we did not proceed to the interpretation of the results of this study in terms of culture contamination or clinically relevant bloodstream infection. Third, pulsed-field gel electrophoresis was not performed to identify epidemic clones. Since molecular typing was not performed some of the studied isolates with antimicrobial resistance may be clonally related. Fourth, the number of patients visit the outpatient clinic of the hospital was not readily available. However, the number of positive blood cultures in the ambulatory outpatients is relatively small [16].
Conclusion
Our data suggest that the relative frequency and the antimicrobial resistance pattern of the blood isolates in a newly founded hospital is not very different from those data described in the literature from other older hospitals around the world. In addition, an alarming increase of antimicrobial resistance was noted during our study for Gram-negative bacteria, especially Acinetobacter baumannii and Klebsiella pneumoniae.
References
Biedenbach DJ, Moet GJ, Jones RN: Occurrence and antimicrobial resistance pattern comparisons among bloodstream infection isolates from the SENTRY antimicrobial surveillance program (1997–2002). Diagnostic Microbiology and Infectious Disease. 2004, 50: 59-69. 10.1016/j.diagmicrobio.2004.05.003.
Sader HS, Jones RN, Andrade-Baiocchi S, Biedenbach DJ, SENTRY Participants Group (Latin America): Four-year evaluation of frequency of occurrence and antimicrobial susceptibility patterns of bacteria from bloodstream infections in Latin America medical centers. Diagn Microbiol Infect Dis. 2002, 44: 271-280.
Kato-Maeda M, Bautista-Alavez A, Rolon-Montes-de-Oca AL, Ramos-Hinojosa A, Ponce-de-Leon A, Bobadilla-del-Valle M, Ruiz-Palacios G, Sifuentes-Osornio : Increasing trend of antimicrobial drug-resistance in organisms causing bacteremia at a tertiary-care hospital: 1995 to 2000. Rev Invest Clin. 2003, 55: 600-5.
National Committee for Clinical Laboratory Standards: Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically, sixth edition: 2003. Approved standard M7-A6. 2003, NCCLS, Wayne, PA
National Committee for Clinical Laboratory Standards: Performance standards for antimicrobial susceptibility testing : 2003. Supplemental tables, M100-S13. 2003, NCCLS, Wayne, PA
Arpi M, Victor MA, Moller JK, Jonsson V, Hansen MM, Peterslund NA, Bruun B: Changing etiology of bacteremia in patients with hematological malignancies in Denmark. Scand J Infect Dis. 1994, 26: 157-162.
Diekema DJ, Pfaller MA, Jones RN, SENTRY Participant Group: Age-related trends in pathogen frequency and antimicrobial susceptibility of bloodstream isolates in North America: SENTRY Antimicrobial Surveillance Program, 1997–2000. Int J Antimicrob Agents. 2002, 20: 412-418. 10.1016/S0924-8579(02)00204-2.
Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB: Nosocomial bloodstream infections in US hospitals: analysis of 24179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004, 39: 309-17. 10.1086/421946.
Wisplinghoff H, Seifert H, Wenzel RP, Edmond MB: Current trends in the epidemiology of nosocomial bloodstream infections in patients with hematological malignancies and solid neoplasms in hospitals in the United States. Clinical Infectious Diseases. 2003, 36: 1103-10. 10.1086/374339.
Tokars JI: Predictive value of blood cultures positive for coagulase-negative staphylococci: implications for patient care and health care quality assurance. Clinical Infectious Diseases. 2004, 39: 333-341. 10.1086/421941.
Gales AC, Jones RN, Forward KR, Linares J, Sader HS, Verhoef J: Emerging importance of multidrug-resistant Acinetobacter species and Stenotrophomonas maltophilia as pathogens in seriously ill patients: geographic patterns, epidemiological features, and trends in the SENTRY Antimicrobial Surveillance Program (1997–1999). Clin Infect Dis. 2001, 15: S104-13. 10.1086/320183.
Iinuma Y: Acinetobacter. Nippon Rinsho. 2002, 60: 2161-5.
Goosens H: European status of resistance in nosocomial infections. Chemotherapy. 2005, 51: 177-181. 10.1159/000086919.
Luzzaro F, Vigano EF, Fossati D, Grossi A, Sala A, Sturla C, Saudelli M, Toniolo A, AMCLI Lombardia Hospital Infectious study group: Prevalence and drug susceptibility of pathogens causing bloodstream infections in northern Italy: a two-year study in 16 hospitals. Eur J Clin Microbiol Infect Dis. 2002, 21: 849-55.
Chan CY, Tang JL, Hsueh PR, Yao M, Chen YC, Chen YC, Shen MC, Wang CH, Tsai W, Chang SC, et al: Trends and antimicrobial resistance of pathogens causing bloodstream infections among febrile neutropenic adults with hematological malignancy. J Formos Med Assoc. 2004, 103: 526-532.
Laupland KB, Church DL, Gregson DB: Blood cultures in ambulatory outpatients. BMC Infect Dis. 2005, 5: 35-10.1186/1471-2334-5-35.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/6/99/prepub
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
MEF conceived the idea for the study. SKK, PM, GG, DN, and PIF collected the data. MEF and PIF drafted the manuscript. All authors made revisions of the manuscript and approved its final version.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Falagas, M.E., Kasiakou, S.K., Nikita, D. et al. Secular trends of antimicrobial resistance of blood isolates in a newly founded Greek hospital. BMC Infect Dis 6, 99 (2006). https://doi.org/10.1186/1471-2334-6-99
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2334-6-99