
Abstract
The needs of modern surgery triggered the intensive development of transplantology, medical materials science, and tissue engineering. These directions require the use of innovative materials, among which porous polymers occupy one of the leading positions. The use of natural and synthetic polymers makes it possible to adjust the structure and combination of properties of a material to its particular application. This review generalizes and systematizes the results of recent studies describing requirements imposed on the structure and properties of synthetic (or artificial) porous polymer materials and implants on their basis and the advantages and limitations of synthesis methods. The most extensively employed, promising initial materials are considered, and the possible areas of application of polymer implants based on these materials are highlighted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
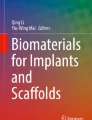
The need of society for modern implants and tissue engineering products is steadily increasing owing to an increase in operative interventions caused by diseases, injuries, and age-related changes. The huge number of transplantation operations led to a high demand for donor organs and tissues. The use of autotransplants and allotransplants is effective but suffers from a number of limitations. Medical materials science, whose task is to design functional substitutes of the damaged tissue and which lies at the intersection of sciences, such as chemistry, biology, and engineering, offers an alternative—various implants based on metals and alloys, bioceramics and bioglass, and natural and synthetic polymers. New materials and compounds are a basis for the manufacture of tissue-engineering products using scaffold technologies and cellular cultures. In the past two decades, the number of studies concerning scaffold development and tissue engineering has increased exponentially (Fig. 1).

Number of publications in the Scopus database (https://www.scopus.com/) found by search for keywords (1) “{scaffold},” (2) “{tissue engineering},” and (3) “3{D printing}” vs. the year of publication from 2000 to 2019.
The development and practical application of medical implants have revolutionized the field of public health. Orthopedic, dental, and vascular implants and heart valves and stents make it possible to considerably improve the duration and quality of life. At present, the manufacture of modern functional implants is an extremely urgent issue. The reconstruction of large or critical size bone defects resulting from injuries, osteoporosis, and surgical intervention during bone infection or bone tumor resection is a difficult task [1, 2]. The annual global demand for implants applied to fill bone defects is above a million units and to treat cardiovascular diseases is on the order of five hundred thousand units.
The key element of tissue engineering, a porous material “scaffold,” functions as an artificial extracellular matrix (ЕСМ) and provides the migration, differentiation, and proliferation of cells. Control over porosity, architecture, and biomimetic properties of engineering frameworks is of crucial importance to ensure the appropriate biological function in addition to mechanical integrity and mass transfer (diffusion and permeability).
In recent years, natural and synthetic polymers have taken leading positions among materials suitable for designing customized implants (Fig. 2). These are first of all porous biocompatible polymer materials; their properties and operating time can be varied and adjusted to a specific task [3].

Number of publications in the Scopus database (https://www.scopus.com/) found by search for keywords (1) “(scaffold *polymer*),” (2) “(scaffold *metal*),” and (3) “(scaffold *ceram*)” vs. the year of publication from 2000 to 2019.
The use of polymers allows the physicomechanical characteristics, structure, and properties of the formed material to be transformed over a wide range. A change in the nature of the synthesized (co)polymer presents an opportunity to design novel biocompatible and noncytotoxic materials with required physicomechanical characteristics for manufacturing modern functional customized implants. The application of polymer materials with a system of open interconnected pores of the specified size enables one either to reproduce the necessary structure of a tissue or to form a framework (scaffold) for further manufacture of a tissue or organ. One of the advantages of polymer materials is their reduced immunogenicity compared, for example, with commonly used xenogenic materials. Another undoubted advantage of polymer materials is that they can be functionalized with various drugs and growth factors; this widens opportunities and improves their application efficiency. The classical fabrication techniques for tissue-engineering scaffolds are solvent casting/particulate leaching, gas foaming, electrospinning, cryogelation, freeze drying, and thermally induced phase separation. Each of these techniques has its own advantages and disadvantages. The growing demand for customized implants necessitates the use of new effective approaches, especially within the framework of additive manufacturing technologies, also called “3D printing.” A rapid growth in the number of publications on 3D printing has been observed only during the past six years (Fig. 1, curve 3). This is largely associated with the technical development and improvement of personal computers as well as the expiration of 3D printing patents acquired in the 1980s. However, the creation of effective porous polymer implants under lab conditions and their successful implementation in clinical practice are a global challenge to date.
Earlier, the authors of [4] considered polymers in orthopedic surgery and tissue engineering while focusing on biofunctionalization of the surface. The main goals of this review are to generalize and systematize the most influential publications on methods for the synthesis of porous polymer materials and implants, to highlight the advantages and disadvantages of a particular technology depending on the purpose of the final product, to list the most commonly used and advanced initial materials (polymers and polymerizable systems) pertinent to the manufacture of porous polymer scaffolds, to address requirements for porous polymer implants depending on their application, and to consider promising applications of such implants.
REQUIREMENTS IMPOSED ON IMPLANTS
Physicomechanical Characteristics
The physicomechanical characteristics of implants may be estimated by measuring a number of physical parameters, such as the elastic modulus or the Young modulus, the bulk modulus, and the shear modulus [5, 6]. In the vast majority of studies, the physicomechanical characteristics of porous polymer biomaterials are assessed in terms of the Young modulus. For various tissues, this parameter varies in a very wide range. It is less than 1 kPa for the brain, ~1 MPa for cartilage, ~10 kPa for muscle, 100 kPa for calcified bone, and 2–4 GPa for bone [7, 8]. It was found that, upon cultivation in polyacrylamide gels of different stiffness (0.1–1.0, 8–17, and 25–40 kPa), human mesenchymal stem cells (hMSC) are capable of differentiating into nerve, muscle, or bone cells, respectively [9]. Hence, the elastic properties of a biomaterial used for implant fabrication strongly influence the fate of stem cells encapsulated into the gel. This provides a tool to control their differentiation. The dependence of cell migration, proliferation, and differentiation processes on the physicomechanical characteristics of implants is studied by a new branch of science, mechanobiology [10, 11].
Porosity, Size, and Randomness of Pore Distribution
The important characteristics of implant materials are porosity and pore structure. The porosity of implants is of prime importance, because it influences the formation and growth of the vasculature and the diffusion of biological compounds. It is important that pores be open and interconnected. In materials not featuring optimal porosity, the necessary processes of cell adhesion, proliferation, differentiation, and migration are suppressed. Porosity is determined as the ratio of the total volume of voids (pores) to the total volume of the implant and is closely related to the physicomechanical characteristics of the implant [12]. The experimental data on the effect of porosity of polymers (polymers based on emulsions and foamed polymers) on the elastic modulus were theoretically substantiated in a recent paper [13].
The porous structure of an osteochondral implant is considered optimal if it contains pores with sizes from 5 to 200–400 µm [14, 15]. In stereolithography and selective laser sintering methods, each element of the porous structure “is drawn” by a laser beam with the minimum diameter of the beam spot being 40 µm. Therefore, the production of polymer materials with a pore size from 5 µm by these methods is hardly possible. The nanolithography technique makes possible the manufacture of scaffolds with a minimum size of the scaffold structure element of ~100 nm. However, because of a low “printing” rate, this process is used for creating 3D objects with a size of 102–103 µm [16, 17].
Microstructure of Polymer Surface
The microstructure of polymer surface exerts a considerable effect on the adhesion and proliferation of cells [18]. Recent progress in the field of microtechnologies and nanotechnologies made it possible to achieve a breakthrough in gaining insight into the effect of material microstructure on the behavior of cells. It was shown that cells can “sense” relief up to several nanometers [19] and can envelop submicron structures [20]. For example, the nanotextured surface of poly(methyl methacrylate) exhibits an increased cell adhesion compared with the nontextured surface [21].
Biofunctionalization of Polymers
Not all polymer materials can be immediately suitable for manufacturing implants. For example, biocompatible poly(ethylene glycol) diacrylate and poly(methyl methacrylate) are bioinert and require pretreatment. The possibility to functionalize a material with biological compounds, such as laminin, fibronectin, vitronectin, RGD peptides, or growth factors, is particularly important in the manufacture of porous implants. This functionalization may be accomplished via noncovalent interactions (e.g., hydrogen bonds, ionic or hydrophobic interactions) or covalent (chemical) bonding. Noncovalent interactions are often achieved by impregnating a porous polymer implant with solution of a functionalizing compound and subsequent drying [22]. If the prolonged release of a biological compound (suppose, antibiotic, VEGF) in the body is required, then its solutions in biodegradable materials, for example, poly(ε-caprolactone) [23] or gelatin [24], may be used for treatment. The chemical bonding of functionalizing compounds is as a rule less effective, because in most cases it causes a partial loss in activity of the compound being grafted. From this point of view, the application of porous polymer materials for manufacturing functional implants is the most promising, because polymers make it possible to realize many approaches not only to the surface modification but also to the bulk chemical modification.
There are three ways of polymer surface modification to ensure a better interaction of polymer materials with cells: the first way involves a change in polymer morphology, that is, the creation of roughnessеs and porous coatings to enhance the germination of tissues; the second way consists in the noncovalent adsorption of biologically active compounds or drugs on the pore surface of the polymer material [25, 26]; and the third way includes chemical modification, that is, plasma or glow discharge treatment and grafting of biologically active compounds, macromolecules, or cellular adhesion functional groups [27–29].
Biocompatibility and Biodegradability
The most important and necessary property of materials for biomedical applications is biocompatibility, that is, the ability of materials not to cause adverse reactions upon introduction into the body [30, 31]. According to GOST [Russian State Standard] R ISO 10993-2-2009, biocompatibility implies the absence of a local inflammatory response, toxic and allergic effects, oncogenicity, and immunogenicity while maintaining functional characteristics of the implant for a specified time.
The nature of natural and synthetic polymers plays the decisive role in biocompatibility, because it defines their effect on the immune system of the host. Natural biopolymers, for example, finely dispersed suspensions of allogeneic tissues obtained by “decellularization” technologies, are frequently used in bioprinting or electrospinning methods [32]. The as-manufactured implants are composed solely of components of the extracellular matrix. However, the accuracy of the reproduction of the geometry of implants manufactured by these methods still cannot reach the accuracy of additive technologies based on UV, visible, or near infrared light initiation. The latter, in turn, suffer from limitations related to the toxicity of initial materials, because the majority of necessary light-sensitive materials are not intended for biological applications [33].
Requirements for polymers and polymer products may be different depending on their purpose. For example, for products operating in contact with blood, vessel prostheses, cardiac valves, and the whole heart, hemocompatibility, that is, the ability of a material to cause no changes in blood functions, transformation of its components, or clotting, is of vital importance. For these products the interaction of a polymer with a biological medium should be reduced to a minimum. In contrast, in the case of orthopedic applications, the intense interaction and fusion of the implant with the tissue are required [34].
Sometimes implants should be not only biocompatible but also biodegradable. Biodegradability is the ability to a material to degrade within the framework of a certain biological system at which the degradation products are nontoxic for this system (body). The formed degradation products in the body should be involved in metabolic and biochemical processes or absorbed by macrophages. Subsequently, the structures of this implant may be replaced with tissues of the body.
In general, each material for medical application should conform to certain biological characteristics and should be studied before clinical testing according to GOST R ISO 10993.5-99. The main parameters in terms of which each material is evaluated are cytotoxicity, chronic toxicity, immunogenicity, oncogenicity, safety, and efficiency when applied for a specific task.
MANUFACTURE OF POROUS POLYMER IMPLANTS
There are two main groups of manufacturing techniques for porous polymer implants: classical techniques and techniques based on additive technologies. Classical techniques can be easily implemented and are quite common. However, they do not allow the manufacture of customized implants with a complex of required properties and structural characteristics. These limitations can be removed using the second group of techniques, additive technologies, which have been vigorously developed in recent years. The additive technologies provide a way to manufacture implants with a high resolution and to use simultaneously several biomaterials.
Classical Techniques
Classical techniques include solvent casting/particulate leaching, gas foaming, electrospinning, cryogelation, freeze drying, and thermally induced phase separation. The production of porous polymer implants by these techniques is optimal if defects are small in size and there is no need to accurately reproduce the geometry of the lost tissue area. Owing to their purpose, these implants are as a rule bioresorbable.
Solvent сasting/particulate leaching (SCPL) is among the first techniques used for the manufacture of porous scaffolds that can be easily implemented. It is in wide use for the manufacture of scaffolds with a porous structure. According to this technique, a polymer solution containing porogenic components is loaded in a mold and the solvent is then evaporated to form a solid polymer block. Afterwards, porogenic components are removed from the block via repeated leaching with water or another solvent; as a result, a pore system appears in the material. Instead of the polymer solution, the solution of a monomer which polymerizes when the composition is loaded in the mold can be used. In most cases, the introduction of porogenic components insignificantly changes the initiation process and the resulting scaffolds are crosslinked homogeneously. Porogenic components are, for example, salts [35, 36], poly(ethylene glycol) [37], and sugar [38]. Among considerable drawbacks of the technique are the absence of accurate control over the shape and size of scaffold pores and pore size distribution as well as the difficulty of obtaning uniform pore interconnectivity. In addition, the presence of solvents, frequently toxic, does not enable the immediate loading of cells and biological compounds. The need to remove the solvent and to create the mold increases time and material expenditures. Among benefits of the SCPL method are a wide range of pore sizes, independent control of porosity and pore size, and the opportunity to produce scaffolds with the required porosity. In the case of osteochondral scaffolds, it should be at least 65%. There is a modified SCPL technique which allows the manufacture of porous polymer scaffolds with a porosity of 91% and a pore size of ~400 µm on the basis of poly(ε-caprolactone) (PCL) [39]. The potential of their use for bone tissue engineering was assessed in vitro using mouse calvaria-derived preosteoblastic cells. Strong composite porous scaffolds are manufactured from granulated calcium phosphate and polylactide (PLA) using a modified salt particulate leaching method [40]. For example, a pressure of 2.5 GPa was applied to a mixture of precompressed granules of calcium phosphate, polylactide, and sodium sulfate and the salt was then leached out. The samples produced with a porosity of 50% combined the compressive strength (4–6 MPa) and permeability typical of the trabecular bone. An elastic biodegradable implant with a pore size of 250 µm was prepared by SCPL from the copolymer of glycolide and ε‑caprolactone (PGCL) [41]. Histological and immunohistochemical analyses revealed that rat smooth muscle cells seeded on scaffolds form smooth muscle tissues. Porous implants derived from poly(3-hydroxybutyrate) and a bioactive glass powder which were produced by SCPL in the presence of sugar particles had an interconnected porosity of 85% and exhibited good adsorption and proliferation of osteoblast cells [42]. In addition, the samples demonstrated bactericidal, bioactive, electroconducting, and antioxidant properties.
Gas foaming. The gas foaming technique relies on the nucleation and growth of gas bubbles dispersed in a polymer to create the porous structure. This method makes it possible to prepare highly porous scaffolds, flexibly control porosity, and introduce bioactive compounds and drugs. Foaming can be accomplished via chemical reaction or polymer treatment with supercritical CO2. The chemical reaction is carried out using a gas-foaming agent, a compound that is added to the initial mixture and evolves gas during chemical decomposition. The most frequently used gas-foaming agents are sodium or ammonium bicarbonates. Owing to the accessibility of gas-foaming agents and easy implementation, this technique became widespread. It is important that gas-foaming agents are usually nontoxic for cells and there is no need to employ organic solvents. This makes the technique relevant for tissue engineering.
In another version, foaming is performed with the use of supercritical CO2. A high-pressure cell is filled with a polymer which is then melted and saturated with supercritical CO2 under high pressure. Next, the pressure is rapidly reduced to atmospheric; as a result, the boiling off of the melt occurs, followed by the evolution of СО2 and the formation of the porous polymer structure. The parameters of the process, such as pressure, temperature, and time of polymer saturation with gas, considerably affect the microstructure, mechanical properties, and biological activity of porous polymer materials [43]. The treatment of polymers with supercritical CO2 is an attractive strategy for producing porous implants, since this gas is inert, nontoxic, and inexpensive. A change in pressure enables one to design objects with gradient porosity. Supercritical CO2 is in wide use as a gas-foaming agent for creating porosity in PLA, PCL, and poly(lactide–co–glycolide) copolymer (PLGA).
The treatment of PLA with supercritical CO2 produced high strength scaffolds with the open cellular structure of pores having sizes from 60 to 140 µm [44]. Experiments showed that such materials maintain the adhesion, proliferation, and differentiation of mouse embryonic fibroblasts cells. Porous polymer scaffolds based on PCL and reduced graphene oxide additives which are manufactured by supercritical CO2 foaming show promise as bone implants [45].
Electrospinning is a simple and versatile technique for manufacturing porous implants from polymer fibers. The electrospinning setup usually consists of three components: a high voltage supply, a grounded metallic collector, and a solution container with a spinneret. During the electrospinning process, a strong electric field is applied between the end of the spinneret and the collector and a charged polymer solution is pushed out from the spinneret and split owing to the instability of the liquid flow. As a result, continuous ultrathin fibers are formed, which are deposited as an unwoven material on the collector. The structure, composition, morphology, diameter, and degree of interweaving of fibers in the material depend on the concentration of polymer solution, its viscosity, presence of additives, applied stress, distance between the collector and spinneret, and its diameter. Among advantages of electrospinning are a relative ease of implementation of the process and high values of porosity and ratio of surface area to volume. Using ultrathin fibers, electrospinning makes it possible to fabricate sheets, tubes, or more complex structures with the same thickness, porosity, high surface area, gradient of mechanical properties, and high ratio of surface area to volume, which is important for tissue engineering. Bifurcated vascular implants with varied diameter were produced by electrospinning from PCL [46]. A vascular implant with a small diameter (1 mm), a wall thickness of 250 µm, and a pore size of 420 nm was electrospun from a bioresorbable material, poly(ester urea) [47]. The use of these implants in mice experiments demonstrated their long-term permeability and extensive remodeling of tissues. The in situ electrospinning procedure was applied to manufacture a personalized nanofibrous dressing from PCL and silver nanoparticles [48]. The material provided the continuous release of silver ions and showed a wide-spectrum antimicrobial activity against two common types of pathogens, Staphylococcus aureus and Escherichia coli. The in vivo experiments revealed that such antibacterial dressings can reduce the inflammatory reaction and accelerate the healing of rat wounds.
Cryogelation. Cryotropic gelation involves the preparation of porous structures by cooling a solution of a precursor compound (monomer or polymer capable of crosslinking) in water or another solvent to a temperature lower than the freezing temperature in order to create conditions for phase separation of the system. As the temperature is decreased, the solvent crystallizes and crosslinking occurs in the unfrozen liquid microphase, the concentrated solution of the precursor compound. Further, water crystals present in the volume of the crosslinked polymer undergo melting during heating; as a result, the porous structure is formed. The time of the crosslinking stage exerts a direct effect on the morphology of the scaffold: the longer the time of crosslinking, the higher the porosity of the scaffold and the smaller the thickness of the wall separating pores [49]. The method makes it possible to change the porosity by varying the ratio between the solvent and the crosslinked polymer precursor solution. Moreover, the porosity and mechanical properties of a cryogel can be changed by adding composite nanofillers, fibers, and polymers [50]. Mild synthesis conditions and accessibility of various biocompatible polymers made the cryogelation method popular. The method allows the use of compositions loaded with biological objects, for example growth factors [51, 52]. Among drawbacks of the method are the absence of accurate control of pore size distribution and geometry of the final implant. A hybrid porous implant for tissue engineering which is based on covalently bound PCL and methacrylamide-functionalized gelatin was produced by the combination of 3D printing and cryogelation techniques [52]. A good colonization of osteoblast precursors and the attachment of viable cells to the cryogel part of the implant were demonstrated.
Freeze drying. In the freeze-drying technique, a polymer solution is poured in a mold of the desired geometry and kept at a low temperature to attain solidification of the solution. The frozen polymer solution is then dried in vacuum; as a result, the sublimation of the solvent occurs and voids are formed in place of the solvent. The pore size and porosity depend on the process temperature and the rates of freezing and drying of polymer solution [53]. The freeze-drying method does not require the stage of leaching and allows one to obtain the structure of uniform ordered pores. However, the method is fairly time consuming. Scaffolds with a pore size of 50–220 µm and a porosity of 55–64% promising for bone tissue regeneration were produced from a mixture of zein, chitosan, and hydroxyapatite (HA) according to this method [54]. A composite implant based on collagen and hydroxyapatite mimicking the gradient porous structure of the bone tissue was manufactured by freeze drying [55]. Owing to the seamlessly bound structure of layers, high porosity, uniform structure of pores, and high level of their interconnectivity, the implant provided optimum conditions for the adhesion and proliferation of cells. It was shown that the material possesses good biocompatibility and osteoconductivity, which contributes to secretion of the extracellular matrix and formation of the bone tissue.
Thermally induced phase separation. In this method, a change in temperature is used to create two different phases (with low and high polymer concentration) in a polymer solution [56]. A polymer is dissolved under heating, and subsequently the solution is cooled. In this case, two phase options may appear, namely, liquid–liquid and liquid–solid. In the first case, the polymer solution is cooled to a temperature lower than the freezing point of the solvent. The emerging thermodynamic instability results in phase separation. When solid and liquid phases appear, phase separation proceeds owing to solidification of the solvent. In both cases, after the induced phase separation, the solvent is removed by extraction, evaporation, or freeze drying. In this way, the porous structure is formed. HA additives are used to improve the adhesion of cells on implants [57]. When hydroxyapatite was introduced into PLA-based implants manufactured by thermally induced phase separation, the compressive modulus doubled [58]. Using the thermally induced phase separation method, an elastic PLA implant containing macropores with sizes above 300 µm was manufactured and then modified with chitosan [59]. The testing of this implant on the model of the rat calvarial bone defect of critical size demonstrated that bone regeneration improved considerably.
Additive Technologies
Large or critical size defects are difficult to restore completely in clinical practice. The additive technologies attract considerable attention as an alternative to classical procedures since they allow the manufacture of customized implants with preset characteristics. The use of additive technologies for the development of porous polymer implants makes it possible to produce a 3D object with the targeted distribution in its structure of biomaterial, cells, growth factors, drugs, and other components needed for the recovery of living tissues. There are two main types of additive technologies. The first type is bioprinting, where a 3D object having the desired geometry and containing the necessary cells and biological components is “printed” via one step. The second type is multistage and consists in the manufacture of an acellular 3D structure followed by its functionalization with signal molecules and seeding with bio-objects [60].
The creation of a customized three-dimensional porous polymer implant always begins with collecting magnetic resonance imaging or computed tomography data on the damaged tissue or organ. The data obtained provide information on the macrostructure of tissues and organs and are used to construct a mathematical model of the future implant. In fact, the “printing” of the customized implant according to the mathematical model may be conducted within the framework of several technologies that have been developed in the past decades and have become widely used. The examples of such technologies are 3D powder binding, selective laser sintering, stereolithography, digital light processing, fused deposition modeling, extrusion bioprinting, and inkjet printing. The principle of each of the above-mentioned methods is schematically shown in Fig. 3. It should be emphasized that each additive technology method has its own advantages and disadvantages related to the choice of polymers, printing resolution, possibility to encapsulate biological objects, cost, and need for subsequent treatment. The influence of additive technologies on the environment was analyzed in a recent paper [61]. In what follows, we will address additive technology methods as applied to the manufacture of porous polymer implants, as well as several recent reviews addressing them in general [62–64].

Principle of manufacturing 3D porous materials by (a) stereolithography, (b) selective laser sintering, (c) digital light processing, (d) fused deposition modeling, (e) 3D powder binding, (f) inkjet printing, and (g) extrusion bioprinting.
3D powder binding/binder jetting (3DP). The binder jetting technology, which has a great potential for use in tissue engineering applications, was advanced in 1995 for the manufacture of 3D objects from aluminum oxide powder [65]. At present, the binder jetting process is extensively used for fabricating products from ceramics, metals, polymers, and composite materials. The manufacture of a 3D object from a powder occurs through the layer-by-layer joining of particles by a binder which is fed from a nozzle. When the binder is deposited directly, the initial powder for producing the porous polymer implant of the desired geometry may be poly(glycolic acid) (PGA), poly(lactic acid), poly(ε-caprolactone), or poly(ethylene oxide) (PEO), and an appropriate solvent usually serves as a binder. The advantage of this method is the accurate control of the microarchitecture and macroarchitecture of the final implant. The introduction of a porogenic agent into the powder enables one to reach a high degree of pore interconnectivity as well as uniform porosity and desired pore size upon leaching of the porogenic agent. At the same time, the need to use organic solvents able to dissolve the components of printheads of industrial 3D printers as porogenic agents and also a low resolution related to spreading of the binder deposited on the powder impose substantial restrictions on the use of this technology in practice.
The above limitations were overcome using a mixture of poly(lactic-co-glycolic acid) and sucrose particles as a printing powder [66]. After printing with a liquid binder, polymer particles were bound together to produce a 3D object and fixed by the solvent vapor. The sucrose was then removed from the object, and the resulting scaffold was placed in a plasticizer (methanol) which was a nonsolvent to reach the rearrangement and effective packing of polymer chains. Here, it is of interest to consider an alternative technology, one which involves the indirect deposition of the binder. Initially the positive replica of the desired shape is printed and the polymer solution is then poured in the printing plate cavity. At the next stage, the replica is removed. Using the indirect binder jetting technology, customized implants mimicking human mandibular condyle were successfully manufactured [67]. A gelatin powder was used as a material for 3D printing of the replica, and PCL and chitosan played the role of a polymer. It was shown that the created implants can be modified with a bioactive apatite coating which activates the spreading and proliferation of bone marrow stromal cells. Nevertheless, because of the complexity of removal of the replica material from the inner pores of the implant, this approach does not allow the manufacture of objects with a complex internal architecture.
Selective laser sintering (SLS). This technology is similar to 3DP. However, instead of gluing particles by the binder in SLS, particles are sintered under exposure to laser radiation [68]. Grains are sintered under high-intensity laser irradiation, and a radiation source is positioned with the aid of a computer according to the specified model. After treatment of one layer, a platform with the implant is lowered, the next powder layer is applied on the top, and the sintering process is repeated. The fabrication of porous polymer implants by SLS is limited to the use of the powders of thermoplastics, for example, PCL [69] or polyetheretherketone. As in the 3DP technology, the mechanical properties, roughness, and porosity can be adjusted by changing the size of powder grains [70]. The accuracy of reproduction and the mechanical strength of implants depend on laser power, particle size, and printing temperature [71]. The main benefits of SLS are a high accuracy of reproduction, the absence of potentially toxic additives (e.g., photoinitiators), and a higher mechanical strength of the product compared with other additive technologies. Moreover, the SLS process makes it possible to manufacture 3D objects with rigidity and porosity gradients [35]. This predetermines the wide use of SLS in bone tissue engineering. [69, 72–74]. A serious disadvantage of SLS is a high local sintering temperature which may destroy cells, proteins, and other bioactive components encapsulated into the polymer. This drawback may be eliminated by adding carbon particles to absorb IR radiation used for sintering [75]. Among other factors restraining the development and implementation of the SLS technology are the complexity of the manufacturing technique and its high cost.
Stereolithography (SLА). The concept of the stereolithographic manufacturing of 3D objects was developed by Н. Kodama at the onset of the 1980s, and in 1986, C.W. Hull received a patent on layer-by-layer lithographic synthesis [76, 77]. The process is based on the layer-by-layer formation of a 3D polymer object of arbitrary shape from the photopolymerizing composition. For this purpose, a mathematical model of the object sliced into layers of preset thickness is built. At the next step, in a reservoir filled with a composition, a platform is placed over which a layer of the composition corresponding to the thickness of the first layer of the mathematical model remains. Next, the image of the first layer is scanned by the laser beam over the surface of the photopolymerizing composition layer; as a result, curing of the irradiated regions of the composition layer occurs through the entire layer thickness. Afterwards, the platform is lowered in the composition by the thickness of the second layer and irradiated with the scanning beam in accordance with the profile of the second layer of the model and so on. When applying a new layer of the photopolymerizing composition, its viscosity plays an important role. In most cases, the introduction of inert additives or solvents is needed to reduce the viscosity. The time of manufacturing one layer depends on the rate of beam scanning and the size of the printable region. In the classical SLA technology, polymerization is initiated by UV laser radiation. An alternative may be initiation by visible light [78, 79]. When ultraviolet is replaced with visible light, polymerization can be implemented in thicker layers [80] and decomposition of the components of the composition may be prevented [81]. Moreover, the use of visible light makes it possible to avoid damage of encapsulated cells by UV light. The search for less cytotoxic photoinitiators in combination with more biocompatible materials for SLA is still a topical problem [82, 83]. The mechanical properties of the resulting implants can be tuned through a change in the degree of polymerization by varying the irradiation dose or photoinitiator concentration or by varying the nature of the initial light-sensitive material (monomer, oligomer, or polymer). The vertical resolution (the layer thickness) depends on the irradiation dose and the depth of light penetration, which can be controlled by introducing various kinds of absorbers of initiating radiation into a light-sensitive material. The SLA technology provides the highest resolution (10–50 µm along the z coordinate) among all the additive technologies. To create small objects with resolution on the order of one micron, nanolithography should be used [84]. The practical application of SLA is limited to light-sensitive materials and owing to the fact that solvents and photoinitiators may leave cytotoxic residues. Nevertheless, the technology is well developed and very popular because of a high productivity of the process and a relatively low manufacturing cost.
Digital light processing (DLP) is similar to SLA in that, in both processes, 3D implants are produced using light for the layer-by-layer selective curing of the photopolymerizing composition. However, here the entire layer of the composition is exposed to light passing through a computer mask (a projection apparatus is used) rather than to laser beam scanning, as in SLA. Information on each layer of the object being formed is presented as a set of digital black and white images which are projected with the aid of a digital micromirror device (DMD) [85]. This enables one to reach a horizontal resolution of ~50 µm depending on the projection system and the number of DMD pixels and a vertical resolution of up to 25 µm. Light sources may be both classical lamps and light-emitting diodes (LED). This makes it possible to cover the wavelength range from UV to visible. The main advantage of DLP (along with reduction in the apparatus cost) is a high rate of manufacturing implants (during each exposure, a new layer is produced).
Using visible light, the DLP technology allows the manufacture of porous polymer scaffolds from composition poly(ε-caprolactone diacrylate)–poly(ethylene glycol) diacrylate with chitosan additives [86]. The cultivation of cells in vitro demonstrated the ability of chitosan to control the hydrophobic properties and thus to improve the adhesion and differentiation of cells. In a recent study [87], customized porous scaffolds with tunable mechanical properties and degradability were printed with a high resolution by the DLP technology from compositions based on various poly(urethane acrylates). The authors managed to choose the composition which upon curing made it possible to produce implants with properties similar to the properties of a cartilage. Porous 3D scaffolds with an average pore size of 600 µm and a porosity of 70% were manufactured from methacrylated polylactide using the DLP method [88]. The sample had the highest compressive strength (2.2 MPa) and showed no cytotoxicity and bicompatibility according to the MTT assay (colorimetric assay for assessing cell metabolic activity).
Fused deposition modeling (FDM). The fused deposition modeling method patented by S.S. Crump in 1992 [89] is one of the first additive technologies. Three-dimensional objects are created with the use of a thermoplastic polymer thread which is fused, extruded through a heated nozzle, and deposited on a working platform according to the specified computer model. The nozzle, chamber, and working platform may be heated independently. The process makes it possible to produce a 3D structure of arbitrary shape without overhangs. Objects with overhangs are manufactured with the aid of support structures that are removed later. The resolution of FDM is ~100 µm and depends on the nozzle diameter, which is chosen according to the rheological properties of the thread used. The characteristics of the final 3D object are affected not only by the nozzle diameter but also by the extrusion rate [90]. The direction and angle of deposition, the layer thickness, and the technology of thread preparation have a strong impact on the mechanical properties of the resulting 3D structure [91]. Various initial materials may be combined into a common structure when a system with several nozzles is employed. In the manufacture of medical products by FDM, biodegradable polymers, such as PCL [91] and PLGA, and nondegradable polymers, for example, impact-resistant polystyrene [92], are most commonly used as a thermoplastic. In a recent paper [93], poly(ethylene-2,5-furandicarboxylate) was synthesized from materials isolated from the biomass (5-hydroxymethylfurfural and ethylene glycol). It was shown that, owing to the optimum adhesion, thermal plasticity, absence of separation, and low thermal shrinkage, this polymer has promise for FDM printing. The FDM method suffers from a low surface roughness of the final object and the need for heating to fuse the polymer, which may destroy the introduced bioactive materials. There are two approaches to the FDM manufacture of porous polymer implants encapsulated by bioactive molecules: either an object is covered by a bioactive material or the treatment temperature and/or extrusion pressure are reduced to acceptable values. However, the FDM procedure is in common use for the manufacture of 3D scaffolds, because a wide variety of relatively inexpensive 3D printers of this type is available on the market.
Extrusion bioprinting. The extrusion bioprinting technology is similar to FDM; however, it includes deposition of not the finished polymer but а flowable matrix (bioink) containing desired biomolecules and cells, which is subsequently cured under heating or irradiation [94]. An extrusion bioprinter prints in accordance with the computer-aided (CAD) model, and the material is extruded continuously. Therefore, the bioactive 3D structure of the desired geometry can be produced at once. Shortening the time interval between extrusion and curing under heating or irradiation leads to a higher accuracy of printing and an increase in the strength of the final object. For the extrusion bioprinting method, it is important to optimize the viscoelastic properties of a bioink during extrusion and the mechanical stability of the resulting structure after extrusion. In this case, it should be taken into account that, when the implant is manufactured, encapsulated biological compounds may differ appreciably in activity depending on the extrusion pressure, shear stress, and nozzle size. The most prominent benefit of extrusion bioprinting is that implants containing biologically active compounds, including growth factors, proteins, drugs, and even cells, can be printed At present, the technology is well developed and offers a wide range of commercially available extrusion bioprinters and bioinks that may be adapted to various tasks [95–97]. However, a low accuracy of printing limits the application of extrusion bioprinting in tissue engineering.
Inkjet рrinting. In this process, bioink droplets are sprayed under heating [98] or the piezoelectric effect [99] according to the specified algorithm. The deposited materials are then cured by UV [100], chemical, or ionic crosslinking. The advantages of inkjet thermal printers are a high printing rate, low cost, and wide availability. However, there is the risk of thermal and mechanical impact on cells during printing. Other significant limitations of thermal printers in 3D bioprinting are the nonuniform size of droplets and often nozzle clogging. The benefits of inkjet printers with a piezoelectric crystal are the opportunity to eject identical droplets of the required size and the absence of heat and pressure impacts on cells. Inkjet printing makes it possible to apply inks with a very high rate (104 droplets per second) [101] and has a wide range of spatial resolution (50 µm) [94]. Even though the inkjet printing method makes it possible to introduce cells, their concentration should be carefully chosen. A low concentration of cells facilitates the formation of droplets and prevents nozzle clogging, while their high concentration may inhibit the process of crosslinking. The feasible modification of commercial inkjet printers for 3D bioprinting makes this process attractive. A wide set of (meth)acrylic materials can be used as bioinks for inkjet printing [100]. A porous implant was created from poly(ethylene glycol) dimethacrylate with encapsulated human chondrocytes using this method [100]. The compressive modulus of the printed implant was close to that of the native human articular cartilage. Three-dimensional porous materials promising for the regeneration of soft tissues were produced by inkjet printing using gelatin methacrylate–chitosan–glyceryl phytate ink [102]. The UV curing of the ink allowed the achievement of a resolution of 150 µm. Experiments in vitro with fibroblasts featured good adhesion, differentiation, and proliferation of cells on these matrices.
POLYMERS FOR MANUFACTURING POROUS IMPLANTS
The choice of a polymer material depends on the target characteristics of porous implants selected for a specific task as well as the synthesis methods. The advancement of synthetic approaches led to the creation of biocomposites and hybrid biomaterials. This makes it possible to precisely tune a wide set of properties, such as biocompatibility, biodegradability, mechanical rigidity, structural strength, cytotoxicity, and bioactivity. All polymers used for manufacturing porous implants may be divided into natural and synthetic biomaterials. The first group encompasses collagen, alginate, chitosan, silk, and hyaluronic acid, which were described in detail in [103]. These materials are obtained from the natural extracellular matrix; therefore, their properties are very close to the properties of natural tissues. The second group consists of poly(lactic acid), polyetheretherketone, poly(ε-caprolactone), poly(propylene fumarate), polylactide-со-polyglycolide, and the ternary copolymer of acrylonitrile, butadiene, and styrene (ABS); some of them will be considered below in more detail. Photosensitive materials applied in SLA and DLP technologies will be considered separately.
Poly(lactic acid)
Poly(lactic acid) (PLA) is a biodegradable, biocompatible, and nontoxic polyester, which is in common use in the manufacture of porous polymer scaffolds by SLS [104, 105] and FDM methods [106–109] and under exposure to light [110–113]. In the latter case, PLA is subjected to preliminary methacrylation. Among benefits of PLA are the renewability of raw materials and the ease of processing as well as a low expansion coefficient. The latter allows excellent shape control in FDM. Depending on the method, scaffolds with different pore sizes from 20 µm for two-photon photopolymerization [110] to 100 µm and 1 mm for FDM [106] and SLA [111], respectively, can be produced. Poly(lactic acid) is applicable in bone tissue engineering [114], because it has the highest mechanical strength among all biodegradable polymers (the elastic modulus, 3–4 GPa; the tensile strength, 50–70 MPa) [104]. However, a high brittleness and lower compressive strength compared with the natural bone remain severe restrictions on the use of this material. The influence of the mentioned drawbacks may be reduced to a minimum by mixing PLA with other materials (PCL, PGA) [115]. The mechanical properties and adhesion and proliferation of cells on these samples may be improved by introducing particles of another material, for example, silk [116], HA, or graphene oxide [107–109].
Polyetheretherketone
Polyetheretherketone (PEEK) is a bioinert thermoplastic [117] with a high chemical resistance and a long biodegradation time [118]. Owing to a fairly high melting temperature of PEEK (343°C), porous polymer implants on it basis are manufactured by SLS [119] and FDM technologies [117, 120]. Extrusion methods require the precise control of nozzle, chamber, and working platform temperatures, which strongly affect the properties of the final object [121]. Owing to a complex of properties (biocompatibility, low thermal conductivity, elasticity, strength) [122] close to those of bone tissue, PEEK is used for its substitution [123]. The main drawbacks of PEEK are its high production cost compared with other thermoplastics and a low bioactivity. The bioactivity of PEEK can be enhanced by introducing various additives. Implants produced from PEEK with tricalcium phosphate and PLA by the SLS technology have improved the parameters of adhesion, proliferation, and differentiation of osteoblasts [119]. Sulfonated porous PEEK loaded with the system chlorogenic acid–grafted peptide has an increased level of proliferation and differentiation of osteoblasts and features a high antibacterial activity against gram-negative and gram-positive bacteria [124]. The FDM method provides a way to optimize mechanical properties (tensile, compressive, bending strength) [125] of implants owing to the thermal gradient during printing [121] or through a change in the thickness of the layer being formed [126].
Poly(ε-caprolactone)
Poly(ε-caprolactone) is a biodegradable, biocompatible, and noncytotoxic polymer approved by the United States Food and Drug Administration (FDA) [127]. Owing to the excellent rheological properties of melt suitable for extrusion methods (important for FDM), low melting temperature (60°С), and a relatively low cost, PCL is in common use for creating porous polymer implants by SLS [73], FDM [128], extrusion bioprinting [129], SLA [130], and DLP methods [131] and, after preliminary methacrylation, by two-photon photopolymerization [127]. Poly(ε-caprolactone) implants manufactured by SLS possess mechanical properties appropriate for bone and cartilage tissue engineering [70, 73]. The introduction of tricalcium phosphate [132, 133] and HA [134] enables a flexible change in the properties of the object. In the FDM method, various additives can be used to improve the properties of porous implants, namely, PLA [135], cellulose [136], and polyurethanes [137]. The SLS technique provides an opportunity to manufacture porous PCL implants with properties analogous to the properties of human bone [74]. The use of PCL mixture with alginate within the framework of the FDM technology makes it possible to improve wetting and water absorption and to increase the efficiency of seeding and the adhesion of cells and viability of osteoblasts [138, 139]. Using methacrylated PCL, 3D objects with a pore size on the order of 500 µm were manufactured by SLA [140].
Poly(propylene fumarate)
Poly(propylene fumarate) (PPF) is a unsaturated linear polyester satisfying a number of medical needs, including biocompatibility, mechanical strength, osteoconductivity, and sterilizability [141, 142].
PPF may be crosslinked by free-radical polymerization via main-chain double bonds with (meth)acrylate monomers [142, 143], N-vinylpyrrolidone [144], and diethyl fumarate [141]. The latter is employed most often to decrease the viscosity of the polymerizing mixture. The advantage of PPF-based compositions is a low crosslinking temperature (40–55°C) [145]. Porous polymer implants based on PPF are manufactured both by classical methods (salt leaching [146, 147] and electrospinning [148]) and using additive technologies (FDM [149], SLA [150–154], and DLP [155, 156]). The additive technologies opened new opportunities for the therapeutic application of PPF-based materials [157]. In the FDM method, the diameter of the fiber obtained and the pore size of the implant depend on the PPF concentration and the pressure and rate of printing [149]. The hydrolysis of ester bonds of PPF in the body leads to decomposition of the polymer into fumaric acid (the Krebs cycle component) and propylene glycol (food additive) [158]. The time of degradation depends on the molecular weight of the main chain, the type of crosslinking agent, and the crosslink density [141, 143]. In contrast to other materials, which degrade too rapidly or too slowly, the degradation of PPF occurs over a period of time comparable with the times of bone recovery and remodeling [159]. High strength characteristics of this polymer make materials based on PPF promising for bone tissue engineering [160]. The mechanical properties of PPF implants may be improved through the introduction of HA [161], tricalcium phosphate [145], and TiO2 nanowires [162] and via a change in molecular weight [159] or crosslink density. A three-dimensional scaffold with a pore size of 150 µm was produced from PPF by microstereolithography (μ-SLA) [163]. The immobilization of the RGD peptide on the surface of pores made it possible to effectively maintain the initial adhesion and proliferation of human chondrocytes, which may contribute to cartilage tissue regeneration. The bioactivity of implants based on PPF may be increased through copolymerization with poly(ethylene glycol) [164], surface functionalization with peptides [150, 165], filling of pores with collagen, and coating with neurotrophin-3 [166].
LIGHT-SENSITIVE MATERIALS (RESINS) IN THE MANUFACTURE OF POROUS POLYMER IMPLANTS
Compounds (monomers, oligomers, polymers) capable of crosslinking under exposure to light are called light-sensitive materials or resins. The class of light-sensitive biomaterials which being cured give a wide range of compounds (from solid thermoreactive materials to soft hydrogels) actively used for the manufacture of porous polymer implants by SLA [167–169], DLP [170, 171], and μ-SLA [172]. The exposure of resins to light induces photopolymerization which yields a three-dimensional polymer network. The most commonly used compounds are (meth)acrylate resins (mono-, di-, tri-, tetra-, penta(meth)acrylates) [167] or (meth)acrylated polymers, such as (meth)acrylated poly(ethylene glycol) di(meth)acrylates (PEGDMA) [173], methacrylated gelatin (GelMA) [174], and poly(ester urethane acrylates) [170], as well as thiolenes [171] and poly(propylene fumarates) [156]. In recent studies, porous polymer scaffolds possessing good adhesion, proliferation, and differentiation of mesenchymal stem cells were produced from commercial oligomeric dimethacrylates MDP-2 [175] and OCM-2 [78]. Owing to the possibility to optimize the composition formulation, the monomer and photoinitiator nature, and the density of the resulting network, porous implants with desired properties can be manufactured from light-sensitive biomaterials. Recently, the approach relying on the curing of light-sensitive materials under exposure to visible light has emerged and is being developed. Photoinitiators are Eosin Y [79], a mixture of ruthenium and sodium persulfate [176] as well as quinones, for example, carboxylated camphoroquinone [177] and substituted ortho-quinone [78, 175]. Compared with UV radiation, visible light possesses a lower energy. This makes it possible to introduce cells and biological compounds into resins even at the stage of production of porous polymer implants.
APPLICATION AREAS OF POROUS POLYMER IMPLANTS
Bone Tissue Replacement
A bone is a hierarchically structured connective tissue composed of an inorganic material (65%), an organic material (25%), and water (10%). Inorganic and organic components form a well-oriented hierarchical structure. The bone is capable of self-healing upon fracture or when small defects are to be bridged [178]. Stem cells from skeletal and vascular tissues form a cartilaginous callus that further vascularizes. However, the bone is incapable of self-healing of critical size defects, and surgical treatment with autologous bone transplants is employed for their reconstruction. At the same time, autotransplants are of the limited accessibility and their use requires additional operations and increases the possibility of complications and infection. Bone tissue regeneration with porous polymer implants is an attractive alternative to solve this problem. It is necessary that the implant material have good mechanical properties and a complex hierarchical pore structure and be capable of vascularization.
Porous implants containing pores with sizes from 70 to 200 µm and a porosity from 85 to 96% which were electrospun from PLA showed good results in bone replacement on the rabbit skull defect model [179]. The conducting porous polymer scaffolds are of interest as potential candidates for improving the piezoelectric properties of the bone tissue and inducing enhanced osteogenesis in implantation. Upon freeze drying of a poly(3,4-ethylenedioxythiophene)-polystyrene sulfonate dispersion, a highly porous electrically conducting material with a high degree of pore interconnectivity and an average diameter of above 50 µm was produced; this material provided the infiltration of cells and the deposition of the matrix in voids [180]. The differentiation of precursor cells of osteogenic cells into positively colored osteocalcin osteoblasts was observed, which makes this material promising for bone tissue engineering. A new strategy of creating biomaterials for induction of the osteogenic differentiation of bone marrow stem cells (BMSC) was proposed in [181]. Three-dimensional porous conducting composite scaffolds based on polylactide–polyaniline nanofibers had good cytocompatibility with BMSC and enhanced their osteogenic differentiation. As a consequence, the levels of expression of alkaline phosphatase and osteocalcin as well as the mineralization of BMSC increased. Н.Т. Liao et al. obtained macroporous cryogels on the basis of gelatin [182]. The effective formation of the bone tissue was revealed for the model of rabbit calvarial defect reconstruction. For several patients, customized craniofacial porous implants were developed from a composition bisphenol-А-glycidyl methacrylate–triethylene glycol dimethacrylate and a bioactive glass additive which was cured by visible light (wavelength, 468 nm) [183]. Over four years in a group of 12 patients, none of the implants were removed and no skin or infection problems were revealed.
Cardiology
Myocardial infarction (blockage of one or several blood vessels) decreases the supply of nutrients and oxygen to heart muscle and causes abnormalities of the electrical function of the cardiovascular system (arrhythmia). As a result of myocardial infarction, the efficiency of the contractile muscle function of the heart worsens. Note that the myocardium of the adult human is incapable of effective regeneration. To address this problem, tissue engineering offers polymer implants with cultivated cardiomyocytes called a heart patch, which can be implanted in the damaged area. The electromechanical coupling of myocytes for their synchronous response to electrical pacing signals is crucial for the effective work of this implant.
Electroactive polymer scaffolds with the system of open and interconnected pores with sizes from several microns to 150 µm were produced from a blend of PCL and aniline-pentamer-modified polyurethane [184]. The compressive modulus and the tensile strength of the samples were 4.1 and 1.3 MPa, respectively. The material was manufactured by the leaching of porogens: poly(ethylene glycol) and sodium chloride. It was shown that its mechanical and chemical properties facilitate the adhesion and growth of neonatal cardiomyocytes, affecting the expression of cardiogenes involved in muscle contraction and relaxation (troponin-Т) and cytoskeleton alignment (actinin-4). These results highlight the potential of this material as an electroactive component for the induction of cardiomyocyte proliferation and repair of damaged heart tissue. For example, L.R. Madden et al. [185] synthesized the hydrogel of 2-hydroxyethyl methacrylate-methacrylic acid copolymer with the pore structure providing integration of the heart tissue. The implant contained parallel channels for the placement of cardiomyocytes and spherical micron pores which enhanced angiogenesis and decreased cicatrization. Scaffolds with the modified surface were seeded with cardiomyocytes of human ES cells and cultivated in vitro. The seeded cardiomyocytes survived and proliferated for two weeks. The cardiac implantation of acellular scaffolds with a pore size of 30–40 µm caused angiogenesis and reduction in the fibrotic response.
Recovery of Nerve Tissues
It is customary to anatomically divide the human nervous system into the central nervous system (CNS), peripheral nervous system (PNS), and two neural networks which function in a coherent manner and are responsible for sensations and response to external stimuli. The CNS is composed of the brain and spinal cord, and the PNS includes nervous roots and endings and immediately nerves distributed in all parts of the body. The regeneration ability of nerve cells is very insignificant [186, 187]. The random interfacial polymerization of 3,4-ethylenedioxythiophene on the pore surface of the chitosan–gelatin polymer yielded conducting porous polymer scaffolds [188]. The presence of poly(3,4-ethylenedioxythiophene) nanoparticles increased the electrical conductivity, hydrophilicity, mechanical characteristics, and thermal stability of the material, decreased its water absorption and biodegradation, and enhanced the growth of cellular neurites. This is the first example of preparing conducting porous scaffold poly(3,4-ethylenedioxythiophene–chitosan–gelatin) by interfacial polymerization in situ. This approach may be promising for neural tissue engineering. It is shown that conducting porous polymer materials show promise for the recovery of neurons or other tissues in tissue engineering [189].
Vascular Implants
The human circulatory system consisting of arteries, veins, and capillaries ensures gas exchange and delivery of nutrients as well as removal of waste products excreted by all cells of the body. The formation of new blood vessels formed in an organ or tissue, angiogenesis, occurs in the calm state in the body with a moderate intensity and is activated when damaged. In the body, blood vessels are united into vasculature and their diameter varies from 2 cm for large arteries to several microns for capillaries. The optimal manufacturing technology of vascular implants depends on the targeted vessel size. L. Shao et al. [190] developed a novel coaxial bioprinting method for producing porous methacrylated gelatin microfibers encapsulated in calcium alginate. It was shown that a tissue containing human umbilical cord vein endothelial cells may be built from these microfibers. In the structure of this tissue, cells gradually migrate and combine to form blood vessel semblance. A promising tubular implant with a length of 40.0 mm, an inner diameter of 4.5 mm, a porosity of 82%, and a tensile strength of 2.2 MPa was electrospun from two types of fibers (PLA outside layer and silk fibroin inner layer) [191]. It was found that, upon culturing on the material, mouse fibroblasts and human umbilical vein endothelial cells feature good adhesion and proliferation and form a continuous monolayer over time. Three months after subcutaneous implantation, these scaffolds could facilitate the production of vasculature. Three-dimensional tubular small-diameter scaffolds with the controlled orientation of nanofibers manufactured by electrospinning are candidates for use as vascular implants.
Cartilage Tissue Replacement
A cartilage is an elastic connective tissue which is formed at the early stages of embryonic development and which is preserved in some parts of the mature skeleton. It exists in the body in three forms, elastic, fibrous, and articular, and each form has different properties and functions. Owing to the absence of vessels and a low concentration of cells, all three types of cartilage are incapable of self-healing or regeneration to functional tissue. J. Kundu et al. [192] FDM printed a porous PCL structure with chondrocyte cell-encapsulated alginate and showed in vivo that a cartilage was formed in it. The auricle model with a pore size on the order of 200 µm was FDM printed from PCL [193]. Using a cell-loaded hydrogel, effective chondrogenesis was induced. The aqueous dispersion of elastic and biodegradable polyurethane nanoparticles was used to print the cartilage implant by the FDM method [194, 195]. These materials had mechanical properties close to those of the native cartilage and facilitated chondrogenesis both in vitro and in vivo. The authors of [196] managed to print the auricular cartilage implant on a 3D printer of original design which allowed the simultaneous deposition of several different materials using chondrocyte-loaded hydrogel, thermoplastic PCL, and Pluronic F-127 [196]. It was revealed that, upon cultivation for five weeks in a growth medium, a new cartilage matrix was formed. This process occurred owing to the presence of microchannels (pores) through the diffusion of nutrients and oxygen. Histological tests conducted after experiments in vivo also demonstrated formation of the new cartilage tissue.
CONCLUSIONS
The demand of modern society for improving the quality of life and increasing life expectancy encourages researchers to upgrade existing and search for new approaches to tailor effective customized implants. In the past decades, methods of manufacturing porous, including polymer, materials for medicine have experienced a very rapid growth, which is largely associated with the extensive development of additive technologies. Owing to the use of computer technologies providing a high resolution of printing and the creation of modern polymer materials and new biofunctionalization methods, it is possible to approach the creation of customized implants approximating native tissues in properties. At the same time, the potential of the existing methods of manufacturing porous polymer implants is not fully realized. Realization of this potential requires solution of many issues, such as increase in the mechanical strength, creation of porous structure gradient, enhancement of biological activity, achievement of the active microcirculation of tissue fluid over the system of interconnected pores, and improvement of the efficiency of immobilization of signal molecules on the pore surface of polymer implants. In addition, it is necessary to find ways to accelerate the production process and to reduce its cost. With the advancement of technologies, porous polymers may become key materials in the manufacture of effective implants for clinical application.
Change history
17 November 2021
An Erratum to this paper has been published: https://doi.org/10.1134/S1811238221330018
REFERENCES
M. Tarchala, V. Engel, J. Barralet, and E. J. Harvey, Injury 49, 523 (2018).
Y. Yan, H. Chen, H. Zhang, C. Guo, K. Yang, K. Chen, R. Cheng, N. Qian, N. Sandler, Y. S. Zhang, H. Shen, J. Qi, W. Cui, and L. Deng, Biomaterials 190–191, 97 (2019).
D. Kuznetsova, P. Timashev, V. Bagratashvili, and E. Zagaynova, Mod. Technol. Med. 6 (4), 201 (2014).
V. Korzhikov, E. Vlakh, and T. Tennikova, Polym. Sci., Ser. A 54, 585 (2012).
K. Phani and D. Sanyal, Mater. Sci. Eng., A 490, 305 (2008).
N. Ramakrishnan and V. Arunachalam, J. Mater. Sci. 25, 3930 (1990).
T. R. Cox and J. T. Erler, Dis. Models Mech.4, 165 (2011).
D. E. Discher, D. J. Mooney, and P. W. Zandstra, Science 324 (5935), 1673 (2009).
D. Discher, APS 2010, Q7.003 (2010).
L. Li, J. Eyckmans, and C. S. Chen, Nat. Mater. 16, 1164 (2017).
K. A. Jansen, D. M. Donato, H. E. Balcioglu, T. Schmidt, E. H. Danen, and G. H. Koenderink, Biochim. Biophys. Acta, Mol. Cell Res. 1853, 3043 (2015).
V. Guarino, F. Causa, and L. Ambrosio, J. Appl. Biomater. Biomech. 5, 149 (2007).
A. D. Drozdov and J. de Claville Christiansen, J. Appl. Polym. Sci. 137, 48449 (2020).
L. Huang, J. Huang, H. Shao, X. Hu, C. Cao, S. Fan, L. Song, and Y. Zhang, Mater. Sci. Eng., C 94, 179 (2019).
S. M. Bittner, B. T. Smith, L. Diaz-Gomez, C. D. Hudgins, A. J. Melchiorri, D. W. Scott, J. P. Fisher, and A. G. Mikos, Acta Biomater. 90, 37 (2019).
C. Liao, A. Wuethrich, and M. Trau, Appl. Mater. Today 19, 100635 (2020).
G. Liu, S. H. Petrosko, Z. Zheng, and C. A. Mirkin, Chem. Rev. 120, 6009 (2020).
F. Gentile, L. Tirinato, E. Battista, F. Causa, C. Liberale, E. M. di Fabrizio, and P. Decuzzi, Biomaterials 31, 7205 (2010).
W. Chen, Y. Sun, and J. Fu, Small 9, 81 (2013).
L. E. McNamara, T. Sjöström, K. Seunarine, R. D. Meek, B. Su, and M. J. Dalby, J. Tissue Eng. 5, 2041731414536177 (2014).
A. Accardo, V. Shalabaeva, and R. La Rocca, MRS Commun. 8, 35 (2017).
X. Liu, Y. Won, and P. X. Ma, J. Biomed. Mater. Res., Part A 74A, 84 (2005).
O. Guillaume, X. Garric, J.-P. Lavigne, H. Van Den Berghe, and J. Coudane, J. Controlled Release 162, 492 (2012).
S. Eğri and N. Eczacıoğlu, Artif. Cells., Nanomed., Biotechnol. 45, 321 (2017).
L. E. Visscher, H. P. Dang, M. A. Knackstedt, D. W. Hutmacher, and P. A. Tran, Mater. Sci. Eng., C 87, 78 (2018).
J. Zhang, J. Li, G. Jia, Y. Jiang, Q. Liu, X. Yang, and S. Pan, RSC Adv. 7, 56732 (2017).
I. V. Averianov, V. A. Korzhikov, and T. B. Tennikova, Polym. Sci., Ser. B 57, 336 (2015).
V. Korzhikov-Vlakh, I. Averianov, E. Sinitsyna, Y. Nashchekina, D. Polyakov, I. Guryanov, A. Lavrentieva, L. Raddatz, E. Korzhikova-Vlakh, and T. Scheper, Polymers 10, 1299 (2018).
S. Hu, X. Cai, X. Qu, B. Yu, C. Yan, J. Yang, F. Li, Y. Zheng, and X. Shi, Int. J. Biol. Macromol. 123, 1320 (2019).
M. I. Shtil’man, A. V. Podkorytova, S. V. Nemtsev, and V. N. Kryazhev, Technology of Polymers for Medical and Biological Use. Polymers of Natural Origin (BINOM. Laboratoriya Znanii, Moscow, 2015) [in Russian].
“VI—Regenerative Medicine,” in Definitions of Biomaterials for the Twenty-First Century, Ed. by D. Williams and X. Zhang (Elsevier, 2019).
E. Garreta, R. Oria, C. Tarantino, M. Pla-Roca, P. Prado, F. Fernández-Avilés, J. M. Campistol, J. Samitier, and N. Montserrat, Mater. Today 20, 166 (2017).
A. K. Nguyen and R. J. Narayan, Mater. Today 20, 314 (2017).
V. I. Sevast’yanov, S. L. Vasilets, and N. V. Perova, Biocompatible Materials (Med. Inf. Agentstvo, Moscow, 2016) [in Russian].
R. Huang, X. Zhu, T. Zhao, and A. Wan, Mater. Res. Express 1, 045403 (2014).
F. Intranuovo, R. Gristina, F. Brun, S. Mohammadi, G. Ceccone, E. Sardella, F. Rossi, G. Tromba, and P. Favia, Plasma Processes Polym. 11, 184 (2014).
K. Sum Chow, E. Khor, and A. Chwee Aun Wan, J. Polym. Res. 8, 27 (2001).
C. Hu, C. Tercero, S. Ikeda, M. Nakajima, H. Tajima, Y. Shen, T. Fukuda, and F. Arai, J. Biosci. Bioeng. 116, 126 (2013).
N. Thadavirul, P. Pavasant, and P. Supaphol, J. Biomed. Mater. Res., Part A 102, 3379 (2014).
A. Rakovsky, I. Gotman, E. Rabkin, and E. Y. Gutmanas, J. Mech. Behav. Biomed. Mater. 32, 89 (2014).
S. H. Lee, B. S. Kim, S. H. Kim, S. W. Choi, S. I. Jeong, I. K. Kwon, S. W. Kang, J. Nikolovski, D. J. Mooney, and Y. K. Han, J. Biomed. Mater. Res., Part A 66, 29 (2003).
S. K. Misra, T. I. Ansari, S. P. Valappil, D. Mohn, S. E. Philip, W. J. Stark, I. Roy, J. C. Knowles, V. Salih, and A. R. Boccaccini, Biomaterials 31, 2806 (2010).
K. Kosowska and M. Henczka, Chem. Process. Eng. 38 (4), 1 (2017).
T. Kuang, F. Chen, L. Chang, Y. Zhao, D. Fu, X. Gong, and X. Peng, Chem. Eng. J. 307, 1017 (2017).
S. Evlashin, P. Dyakonov, M. Tarkhov, S. Dagesyan, S. Rodionov, A. Shpichka, M. Kostenko, S. Konev, I. Sergeichev, and P. Timashev, Materials 12, 2991 (2019).
R. Tejeda-Alejandre, H. Lara-Padilla, C. Mendoza-Buenrostro, C. A. Rodriguez, and D. Dean, Procedia CIRP 65, 207 (2017).
Y. Gao, T. Yi, T. Shinoka, Y. U. Lee, D. H. Reneker, C. K. Breuer, and M. L. Becker, Adv. Healthcare Mater. 5, 2427 (2016).
R.-H. Dong, Y.-X. Jia, C.-C. Qin, L. Zhan, X. Yan, L. Cui, Y. Zhou, X. Jiang, and Y.-Z. Long, Nanoscale 8, 3482 (2016).
A. Kumar, R. Mishra, Y. Reinwald, and S. Bhat, Mater. Today 13 (11), 42 (2010).
J. Hendriks, J. Riesle, and C. A. van Blitterswijk, J. Tissue. Eng. Regener. Med. 1, 170 (2007).
N. Bölgen, P. Korkusuz, İ. Vargel, E. Kılıç, E. Güzel E., T. Çavuşoğlu, D. Uçkan, and E. Pişkin, Artif. Cells., Nanomed., Biotechnol. 42, 70 (2014).
J. Van Rie, H. Declercq, J. Van Hoorick, M. Dierick, L. Van Hoorebeke, R. Cornelissen, H. Thienpont, P. Dubruel, and S. Van Vlierberghe, J. Mater. Sci.: Mater. Med. 26, 123 (2015).
J. Grenier, H. Duval, F. Barou, P. Lv, B. David, and D. Letourneur, Acta Biomater. 94, 195 (2019).
Z. Shahbazarab, A. Teimouri, A. N. Chermahini, and M. Azadi, Int. J. Biol. Macromol. 108, 1017 (2018).
L. Chen, Z. Wu, Y. Zhou, L. Li, Y. Wang, Z. Wang, Y. Chen, and P. Zhang, J. Appl. Polym. Sci. 134, 45271 (2017).
M. Boffito, S. Sartori, and G. Ciardelli, Polym. Int. 63, 2 (2014).
K. S. Jack, S. Velayudhan, P. Luckman, M. Trau, L. Grøndahl, and J. Cooper-White, Acta Biomater. 5, 2657 (2009).
G. Wei and P. X. Ma, Biomaterials 25, 4749 (2004).
S. Chen, X. Zhao, and C. Du, Eur. Polym. J. 109, 303 (2018).
J. Groll, T. Boland, T. Blunk, J. A. Burdick, D.‑W. Cho, P. D. Dalton, B. Derby, G. Forgacs, Q. Li, V. A. Mironov, L. Moroni, M. Nakamura, W. Shu, S. Takeuchi, G. Vozzi, T. B. F. Woodfield, T. Xu, J. J. Yoo, and J. Malda, Biofabrication 8, 013001 (2016).
M. R. Khosravani and T. Reinicke, Appl. Mater. Today 20, 100689 (2020).
C. Mota, D. Puppi, F. Chiellini, and E. Chiellini, J. Tissue Eng. Regener. Med. 9, 174 (2015).
S. C. Ligon, R. Liska, J. Stampfl, M. Gurr, and R. Mülhaupt, Chem. Rev. 117, 10212 (2017).
C. Mandrycky, Z. Wang, K. Kim, and D.-H. Kim, Biotechnol. Adv. 34, 422 (2016).
S. J. J. Lee, E. Sachs, and M. Cima, Rapid Prototyping J. 1 (4), 24 (1995).
H. N. Chia and B. M. Wu, Biofabrication 7, 015002 (2014).
J.-Y. Lee, B. Choi, B. Wu, and M. Lee, Biofabrication 5, 045003 (2013).
A. Youssef, S. J. Hollister, and P. D. Dalton, Biofabrication 9, 012002 (2017).
K.-Y. Tsai, H.-Y. Lin, Y.-W. Chen, C.-Y. Lin, T.‑T. Hsu, and C.-T. Kao, Materials 10, 65 (2017).
G. Salmoria, D. Hotza, P. Klauss, L. Kanis, and C. Roesler, Adv. Mech. Eng. 6, 640496 (2014).
S. F. S. Shirazi, S. Gharehkhani, M. Mehrali, H. Yarmand, H. S. C. Metselaar, N. A. Kadri, and N. A. A. Osman, Sci. Technol. Adv. Mater. 16, 033502 (2015).
Y. Du, H. Liu, Q. Yang, S. Wang, J. Wang, J. Ma, I. Noh, A. G. Mikos, and S. Zhang, Biomaterials 137, 37 (2017).
A. Mazzoli, C. Ferretti, A. Gigante, E. Salvolini, and M. Mattioli-Belmonte, Rapid Prototyping J. 21, 386 (2015).
J. M. Williams, A. Adewunmi, R. M. Schek, C. L. Flanagan, P. H. Krebsbach, S. E. Feinberg, S. J. Hollister, and S. Das, Biomaterials 26, 4817 (2005).
J. M. Kanczler, S.-H. Mirmalek-Sani, N. A. Hanley, A. L. Ivanov, J. J. Barry, C. Upton, K. M. Shakesheff, S. M. Howdle, E. N. Antonov, and V. N. Bagratashvili, Acta Biomater. 5, 2063 (2009).
H. Kodama, Rev. Sci. Instrum. 52, 1770 (1981).
C. W. Hull, US Patent No. 4575330 (1986).
V. V. Yudin, R. S. Kovylin, M. A. Baten’kin, T. I. Kulikova, D. Y. Aleynik, M. N. Egorikhina, Y. P. Rubtsova, I. N. Charykova, S. G. Mlyavykh, S. A. Chesnokov, and I. L. Fedushkin, Polymer 192, 122302 (2020).
Z. Wang, R. Abdulla, B. Parker, R. Samanipour, S. Ghosh, and K. Kim, Biofabrication 7, 045009 (2015).
M. P. Shurygina, M. Y. Zakharina, M. A. Baten’kin, A. N. Konev, A. S. Shavyrin, E. A. Chelnokov, N. Y. Shushunova, M. V. Arsenyev, S. A. Chesnokov, and G. A. Abakumov, Eur. Polym. J. 127, 109573 (2020).
S. A. Chesnokov, R. S. Kovylin, O. G. N. Mamysheva, G. K. Fukin, V. K. Cherkasov, and K. A. Lyssenko, J. Polym. Res. 21, 441 (2014).
B. Thavornyutikarn, N. Chantarapanich, K. Sitthiseripratip, G. A. Thouas, and Q. Chen, Prog. Biomater. 3 (2), 61 (2014).
N. A. Chartrain, C. B. Williams, and A. R. Whittington, Acta Biomater. 74, 90 (2018).
M. Vaezi, H. Seitz, and S. Yang, Int. J. Adv. Des. Manuf. Technol. 67, 1721 (2013).
C. Sun, N. Fang, D. Wu, and X. Zhang, Sens. Actuators, A 121, 113 (2005).
Y.-L. Cheng and F. Chen, Mater. Sci. Eng., C 81, 66 (2017).
H. Chen, S.-Y. Lee, and Y.-M. Lin, Polymers 12, 1500 (2020).
A. B. Saed, A. H. Behravesh, S. Hasannia, S. A. A. Ardebili, B. Akhoundi, and M. Pourghayoumi, J. Manuf. Process. 56, 550 (2020).
S. S. Crump, US Patent No. 5121329 (1992).
A. P. M. Madrid, S. M. Vrech, M. A. Sanchez, and A. P. Rodriguez, Mater. Sci. Eng., C 100, 631 (2019).
T. Patrício, M. Domingos, A. Gloria, U. D’Amora, J. Coelho, and P. Bártolo, Rapid Prototyping J. 20, 145 (2014).
N. Vargas-Alfredo, A. Dorronsoro, A. L. Cortajarena, and J. Rodríguez-Hernández, ACS Appl. Mater. Interfaces 9, 37454 (2017).
F. A. Kucherov, E. G. Gordeev, A. S. Kashin, and V. P. Ananikov, Angew. Chem. 129, 16147 (2017).
S. V. Murphy and A. Atala, Nat. Biotechnol. 32, 773 (2014).
S.-H. Park, C. S. Jung, and B.-H. Min, Tissue Eng. Regener. Med. 13, 622 (2016).
J. Liu, L. Sun, W. Xu, Q. Wang, S. Yu, and J. Sun, Carbohydr. Polym. 207, 297 (2019).
S. Derakhshanfar, R. Mbeleck, K. Xu, X. Zhang, W. Zhong, and M. Xing, Bioact. Mater. 3, 144 (2018).
E. A. Roth, T. Xu, M. Das, C. Gregory, J. J. Hickman, and T. Boland, Biomaterials 25, 3707 (2004).
K. Markstedt, A. Mantas, I. Tournier, H. C. Martínez Ávila, D. Hagg, and P. Gatenholm, Biomacromolecules 16, 1489 (2015).
X. Cui, K. Breitenkamp, M. Finn, M. Lotz, and D. D. D’Lima, Tissue Eng., Part A 18, 1304 (2012).
U. Demirci and G. Montesano, Lab-on-a-Chip 7, 1139 (2007).
A. Mora-Boza, M. K. Wlodarczyk-Biegun, A. del Campo, B. Vázquez-Lasa, and J. San Román, Biomater. Sci. 8, 506 (2020).
M. Mobaraki, M. Ghaffari, A. Yazdanpanah, Y. Luo, and D. Mills, Bioprinting 18, e00080 (2020).
C. Gayer, J. Ritter, M. Bullemer, S. Grom, L. Jauer, W. Meiners, A. Pfister, F. Reinauer, M. Vučak, K. Wissenbach, H. Fischer, R. Poprawe, and J. H. Schleifenbaum, Mater. Sci. Eng., C 101, 660 (2019).
A. E. Woźna, A. F. Junka, and A. Szymczyk, Acta Bioeng. Biomech. 20 (3), 1 (2018).
A. Grémare, V. Guduric, R. Bareille, V. Heroguez, S. Latour, N. L’Heureux, J.-C. Fricain, S. Catros, and D. Le Nihouannen, J. Biomed. Mater. Res., Part A 106, 887 (2018).
Y. Li, C. Liao, and S. C. Tjong, Nanomaterials 9, 590 (2019).
J. Wu, N. Chen, F. Bai, and Q. Wang, Polym. Comopos. 39, E508 (2018).
Q. Chen, J. D. Mangadlao, J. Wallat, A. De Leon, J. K. Pokorski, and R. C. Advincula, ACS Appl. Mater. Interfaces 9, 4015 (2017).
A. Koroleva, A. Gill, I. Ortega, J. Haycock, S. Schlie, S. Gittard, B. Chichkov, and F. Claeyssens, Biofabrication 4, 025005 (2012).
S. Tanodekaew, S. Channasanon, P. Kaewkong, and P. Uppanan, Procedia Eng. 59, 144 (2013).
F. P. W. Melchels, J. Feijen, and D. W. Grijpma, Biomaterials 30, 3801 (2009).
J. Jansen, F. P. W. Melchels, D. W. Grijpma, and J. Feijen, Biomacromolecules 10, 214 (2009).
P. R. Pawar, U. S. Tekale, U. S. Shisodia, T. J. Totre, and J. A. Domb, Recent Pat. Regener. Med 4, 40 (2014).
P. Saini, M. Arora, and M. N. V. R. Kumar, Adv. Drug Delivery Rev. 107, 47 (2016).
Y. K. Yeon, H. S. Park, J. M. Lee, J. S. Lee, Y. J. Lee, M. T. Sultan, Y. B. Seo, O. J. Lee, S. H. Kim, and C. H. Park, J. Biomater. Sci., Polym. Ed. 29, 894 (2018).
M. Vaezi and S. Yang, Virtual Phys. Prototyping 10, 123 (2015).
S. M. Kurtz and J. N. Devine, Biomaterials 28, 4845 (2007).
P. Feng, P. Wu, C. Gao, Y. Yang, W. Guo, W. Yang, and C. Shuai, Adv. Sci. 5, 1700817 (2018).
X. Deng, Z. Zeng, B. Peng, S. Yan, and W. Ke, Materials 11, 216 (2018).
C. Yang, X. Tian, D. Li, Y. Cao, F. Zhao, and C. Shi, J. Mater. Process. Technol. 248, 1 (2017).
H. Wang, M. Xu, W. Zhang, D. T. Kwok, J. Jiang, Z. Wu, and P. K. Chu, Biomaterials 31, 8181 (2010).
S. Singh, C. Prakash, and S. Ramakrishna, Eur. Polym. J. 114, 234 (2019).
X. He, Y. Deng, Y. Yu, H. Lyu, and L. Liao, Colloids Surf., B 181, 767 (2019).
M. F. Arif, S. Kumar, K. M. Varadarajan, and W. J. Cantwell, Mater. Des. 146, 249 (2018).
W. Wu, P. Geng, G. Li, D. Zhao, H. Zhang, and J. Zhao, Materials 8, 5834 (2015).
J. R. Thompson, K. S. Worthington, B. J. Green, N. K. Mullin, C. Jiao, E. E. Kaalberg, L. A. Wiley, I. C. Han, S. R. Russell, E. H. Sohn, C. A. Guymon, R. F. Mullins, E. M. Stone, and B. A. Tucker, Acta Biomater. 94, 204 (2019).
I. Zein, D. W. Hutmacher, K. C. Tan, and S. H. Teoh, Biomaterials 23, 1169 (2002).
M. Domingos, F. Chiellini, A. Gloria, L. Ambrosio, P. Bartolo, and E. Chiellini, Rapid Prototyping J. 18, 56 (2012).
L. Elomaa, S. Teixeira, R. Hakala, H. Korhonen, D. W. Grijpma, and J. V. Seppälä, Acta Biomater. 7, 3850 (2011).
B. J. Green, K. S. Worthington, J. R. Thompson, S. J. Bunn, M. Rethwisch, E. E. Kaalberg, C. Jiao, L. A. Wiley, R. F. Mullins, E. M. Stone, E. H. Sohn, B. A. Tucker, and C. A. Guymon, Biomacromolecules 19, 3682 (2018).
H. Doyle, S. Lohfeld, and P. McHugh, Med. Eng. Phys. 37, 767 (2015).
H.-T. Liao, M.-Y. Lee, W.-W. Tsai, H.-C. Wang, and W.-C. Lu, J. Tissue Eng. Regener. Med. 10, E337 (2016).
S. Buyuksungur, T. Endogan Tanir, A. Buyuksungur, E. I. Bektas, G. Torun Kose, D. Yucel, T. Beyzadeoglu, E. Cetinkaya, C. Yenigun, E. Tönük, V. Hasirci, and N. Hasirci, Biomater. Sci. 5, 2144 (2017).
L. D. Albrecht, S. W. Sawyer, and P. Soman, 3D Print. Addit. Manuf. 3, 106 (2016).
M. E. Alemán-Domínguez, E. Giusto, Z. Ortega, M. Tamaddon, A. N. Benítez, and C. Liu, J. Biomed. Mater. Res., Part B 107, 521 (2019).
A. Haryńska, J. Kucinska-Lipka, A. Sulowska, I. Gubanska, M. Kostrzewa, and H. Janik, Materials 12, 887 (2019).
Y. B. Kim and G. H. Kim, ACS Comb. Sci. 17, 87 (2015).
M. S. Kim and G. Kim, Carbohydr. Polym. 114, 213 (2014).
L. Elomaa, S. Teixeira, R. Hakala, H. Korhonen, D. W. Grijpma, and J. V. Seppälä, Acta Biomater. 7, 3850 (2011).
M. J. Yaszemski, R. G. Payne, W. C. Hayes, R. Langer, and A. G. Mikos, Biomaterials 17, 2127 (1996).
J. S. Temenoff and A. G. Mikos, Biomaterials 21, 2405 (2000).
S. He, M. D. Timmer, M. J. Yaszemski, A. W. Yasko, P. S. Engel, and A. G. Mikos, Polymer 42, 1251 (2001).
S. J. Peter, P. Kim, A. W. Yasko, M. J. Yaszemski, and A. G. Mikos, J. Biomed. Mater. Res. 44, 314 (1999).
C. Ma, Z. Ma, F. Yang, J. Wang, and C. Liu, Biomed. Mater. 14, 045002 (2019).
J. P. Fisher, J. W. M. Vehof, D. Dean, J. P. C. M. van der Waerden, T. A. Holland, A. G. Mikos, and J. A. Jansen, J. Biomed. Mater. Res. 59, 547 (2002).
P. J. Fisher, T. A. Holland, D. Dean, P. S. Engel, and A. G. Mikos, J. Biomater. Sci., Polym. Ed. 12, 673 (2001).
K. N. Cicotte, E. L. Hedberg-Dirk, and S. M. Dirk, J. Appl. Polym. Sci. 117, 1984 (2010).
J. E. Trachtenberg, J. K. Placone, B. T. Smith, C. M. Piard, M. Santoro, D. W. Scott, J. P. Fisher, and A. G. Mikos, ACS Biomater. Sci. Eng. 2, 1771 (2016).
P. X. Lan, J. W. Lee, Y.-J. Seol, and D.-W. Cho, J. Mater. Sci., Mater. Med. 20, 271 (2009).
J. W. Lee, K. S. Kang, S. H. Lee, J.-Y. Kim, B.‑K. Lee, and D.-W. Cho, Biomaterials 32, 744 (2011).
K. Kim, D. Dean, J. Wallace, R. Breithaupt, A. G. Mikos, and J. P. Fisher, Biomaterials 32, 3750 (2011).
K.-W. Lee, S. Wang, B. C. Fox, E. L. Ritman, M. J. Yaszemski, and L. Lu, Biomacromolecules 8, 1077 (2007).
M. Dadsetan, T. Guda, M. B. Runge, D. Mijares, R. Z. LeGeros, J. P. LeGeros, D. T. Silliman, L. Lu, J. C. Wenke, P. R. Brown Baer, and M. J. Yaszemski, Acta Biomater. 18, 9 (2015).
M. O. Wang, C. E. Vorwald, M. L. Dreher, E. J. Mott, M.-H. Cheng, A. Cinar, H. Mehdizadeh, S. Somo, D. Dean, E. M. Brey, and J. P. Fisher, Adv. Mater. 27, 138 (2015).
Y. Luo, C. K. Dolder, J. M. Walker, R. Mishra, D. Dean, and M. L. Becker, Biomacromolecules 17, 690 (2016).
H. N. Chia and B. M. Wu, J. Biol. Eng. 9, 1 (2015).
K. Rezwan, Q. Z. Chen, J. J. Blaker, and A. R. Boccaccini, Biomaterials 27, 3413 (2006).
J. M. Walker, E. Bodamer, O. Krebs, Y. Luo, A. Kleinfehn, M. L. Becker, and D. Dean, Biomacromolecules 18, 1419 (2017).
B. D. Ulery, L. S. Nair, and C. T. Laurencin, J. Polym. Sci., Part B: Polym. Phys. 49, 832 (2011).
J. E. Trachtenberg, J. K. Placone, B. T. Smith, J. P. Fisher, and A. G. Mikos, J. Biomater. Sci., Polym. Ed. 28, 532 (2017).
M. Salarian, W. Z. Xu, M. C. Biesinger, and P. A. Charpentier, J. Mater. Chem. B 2, 5145 (2014).
C. B. Ahn, Y. Kim, S. J. Park, Y. Hwang, and J. W. Lee, J. Biomater. Sci., Polym. Ed. 29, 917 (2018).
R. A. Dilla, C. M. M. Motta, S. R. Snyder, J. A. Wilson, C. Wesdemiotis, and M. L. Becker, ACS Macro Lett. 7, 1254 (2018).
Z. Cai, Y. Wan, M. L. Becker, Y.-Z. Long, and D. Dean, Biomaterials 208, 45 (2019).
X. Chen, Y. Zhao, X. Li, Z. Xiao, Y. Yao, Y. Chu, B. Farkas, I. Romano, F. Brandi, and J. Dai, Adv. Healthcare Mater. 7, 1800315 (2018).
V. S. Voet, T. Strating, G. H. Schnelting, P. Dijkstra, M. Tietema, J. Xu, A. J. Woortman, K. Loos, J. Jager, and R. Folkersma, ACS Omega 3, 1403 (2018).
S. Schüller-Ravoo, S. M. Teixeira, J. Feijen, D. W. Grijpma, and A. A. Poot, Macromol. Biosci. 13, 1711 (2013).
K. N. Bardakova, E. A. Grebenik, N. V. Minaev, S. N. Churbanov, Z. Moldagazyeva, G. E. Krupinov, S. V. Kostjuk, and P. S. Timashev, Mater. Sci. Eng., C 107, 110300 (2020).
T. Kuhnt, R. Marroquín García, S. Camarero-Espinosa, A. Dias, A. T. ten Cate, C. A. van Blitterswijk, L. Moroni, and M. B. Baker, Biomater. Sci. 7, 4984 (2019).
S. Bertlein, G. Brown, K. S. Lim, T. Jungst, T. Boeck, T. Blunk, J. Tessmar, G. J. Hooper, T. B. F. Woodfield, and J. Groll, Adv. Mater. 29, 1703404 (2017).
P. Timashev, D. Kuznetsova, A. Koroleva, N. Prodanets, A. Deiwick, Y. Piskun, K. Bardakova, N. Dzhoyashvili, S. Kostjuk, and E. Zagaynova, Nanomedicine 11, 1041 (2016).
D. C. Aduba, Jr., E. D. Margaretta, A. E. Marnot, K. V. Heifferon, W. R. Surbey, N. A. Chartrain, A. R. Whittington, T. E. Long, and C. B. Williams, Mater. Today Commun. 19, 204 (2019).
T. Billiet, E. Gevaert, T. De Schryver, M. Cornelissen, and P. Dubruel, Biomaterials 35, 49 (2014).
R. S. Kovylin, M. A. Baten’kin, T. I. Kulikova, M. N. Egorikhina, I. N. Charikova, S. A. Gusev, Y. P. Rubtsova, S. G. Mlyavykh, D. Y. Aleynik, S. A. Chesnokov, and I. L. Fedushkin, ChemistrySelect 4, 4147 (2019).
K. S. Lim, B. S. Schon, N. V. Mekhileri, G. C. J. Brown, C. M. Chia, S. Prabakar, G. J. Hooper, and T. B. F. Woodfield, ACS Biomater. Sci. Eng. 2, 1752 (2016).
E. A. Kamoun, A. Winkel, M. Eisenburger, and H. Menzel, Arabian J. Chem. 9, 745 (2016).
Z. Gugala, R. W. Lindsey, and S. Gogolewski, Macromol. Symp. 253, 147 (2007).
I. K. Shim, M. R. Jung, K. H. Kim, Y. J. Seol, Y. J. Park, W. H. Park, and S. J. Lee, J. Biomed. Mater. Res., Part B 95B, 150 (2010).
A. G. Guex, J. L. Puetzer, A. Armgarth, E. Littmann, E. Stavrinidou, E. P. Giannelis, G. G. Malliaras, and M. M. Stevens, Acta Biomater. 62, 91 (2017).
J. Chen, M. Yu, B. Guo, P. X. Ma, and Z. Yin, J. Colloid Interface Sci. 514, 517 (2018).
H.-T. Liao, K. Shalumon, K.-H. Chang, C. Sheu, and J.-P. Chen, J. Mater. Chem. B 4, 1827 (2016).
K. M. J. Aitasalo, J. M. Piitulainen, J. Rekola, and P. K. Vallittu, Head Neck 36, 722 (2014).
N. Baheiraei, H. Yeganeh, J. Ai, R. Gharibi, S. Ebrahimi-Barough, M. Azami, S. Vahdat, and H. Baharvand, J. Biomed. Mater. Res., Part A 103, 3179 (2015).
L. R. Madden, D. J. Mortisen, E. M. Sussman, S. K. Dupras, J. A. Fugate, J. L. Cuy, K. D. Hauch, M. A. Laflamme, C. E. Murry, and B. D. Ratner, Proc. Natl. Acad. Sci. U. S. A. 107, 15211 (2010).
E. Moeendarbary, I. P. Weber, G. K. Sheridan, D. E. Koser, S. Soleman, B. Haenzi, E. J. Bradbury, J. Fawcett, and K. Franze, Nat. Commun. 8, 1 (2017).
J. E. Burda and M. V. Sofroniew, Neuron 81, 229 (2014).
S. Wang, C. Sun, S. Guan, W. Li, J. Xu, D. Ge, M. Zhuang, T. Liu, and X. Ma, J. Mater. Chem. B 5, 4774 (2017).
H. Baniasadi, A. R. Sa, and S. Mashayekhan, Int. J. Biol. Macromol. 74, 360 (2015).
L. Shao, Q. Gao, H. Zhao, C. Xie, J. Fu, Z. Liu, M. Xiang, and Y. He, Small 14, 1802187 (2018).
S. Wang, Y. Zhang, H. Wang, G. Yin, and Z. Dong, Biomacromolecules 10, 2240 (2009).
J. Kundu, J. H. Shim, J. Jang, S. W. Kim, and D. W. Cho, J. Tissue Eng. Regener. Med. 9, 1286 (2015).
J.-S. Lee, J. M. Hong, J. W. Jung, J.-H. Shim, J.‑H. Oh, and D.-W. Cho, Biofabrication 6, 024103 (2014).
K.-C. Hung, C.-S. Tseng, L.-G. Dai, and S.-h. Hsu, Biomaterials 83, 156 (2016).
K.-C. Hung, C.-S. Tseng, and S.-h. Hsu, Adv. Healthcare Mater. 3, 1578 (2014).
H.-W. Kang, S. J. Lee, I. K. Ko, C. Kengla, J. J. Yoo, and A. Atala, Nat. Biotechnol. 34, 312 (2016).
Funding
This work was supported by the Russian Foundation for Basic Research (project no. 19-13-50489).
Author information
Authors and Affiliations
Corresponding author
Additional information
Translated by T. Soboleva
The original online version of this article was revised due to a retrospective Open Access order.
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kovylin, R.S., Aleynik, D.Y. & Fedushkin, I.L. Modern Porous Polymer Implants: Synthesis, Properties, and Application. Polym. Sci. Ser. C 63, 29–46 (2021). https://doi.org/10.1134/S1811238221010033
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S1811238221010033