
Abstract
Modern trends in the development of health care suggest its focus on the interests of the patient and its holistic nature, as well as deep penetration into all parts of health care information technology. The driving force behind the ongoing changes, of course, are scientific achievements, the importance of which in the development of new medical technologies and the creation of innovative diagnostic devices, as well as medicines, has grown significantly in recent years. These processes provide conditions for the introduction into clinical practice of a new model of medical care—personalized medicine, based on the choice of methods of diagnosis and treatment with account for the individual characteristics of the course of the disease, as well as the patient’s lifestyle. Personalized medicine technologies, which involve the creation of an appropriate, often expensive, infrastructure of omics technologies, should ultimately lead to an increase in the efficiency, quality, and, most importantly, safety of medical care. In the Russian Federation, this area is actively developing in four world-class research centers, including the Almazov National Medical Research Center. The current state and prospects of research in the field of personalized medicine are discussed in this article, prepared by the author on the basis of his scientific report at a meeting of the Presidium of the Russian Academy of Sciences.
Similar content being viewed by others


Since the beginning of the 21st century, biomedicine has developed rapidly, accumulating the achievements of basic sciences in the field of medical research and focusing on their use in real clinical practice. Life sciences have been included in the development programs of the world’s leading universities and have become their main driving force. Research in the field of mathematics, physics, chemistry, and biology has opened up the possibility of deep penetration into the intimate mechanisms of the occurrence of the most significant human diseases: oncological, cardiovascular, and many hereditary. Genetic technologies are being developed intensively, which made it possible to identify the genetic causes of almost any pathology and determine the sequence of the entire human genome. Based on these data, gene therapy began to be used in clinical practice, including genome editing technologies, which made it possible to select methods individually for the treatment of severe hereditary diseases [1].
Based on the achievements of synthetic biology, genomics, proteomics, metabolomics, bioinformatics, and other related disciplines, a new model of medical care is being formed—personalized medicine, which involves the choice of optimal diagnostic, therapeutic, and preventive approaches for a particular patient, taking into account his/her specific biomarkers (including genetic ones), which help the doctor determine which treatment method is most effective. Personalized medicine is often called precision medicine due to its focus on identifying key factors in the development of the disease (thanks to biomarkers; molecular pathways of pathology; and genomics, proteomics, and metabolomics data), as well as considering the patient’s lifestyle and environmental factors. Since it may be difficult to individualize treatment fully, including for economic reasons, precision medicine uses unique (“point”) protocols designed for stratified patient groups. It should be emphasized that these two concepts—personalized medicine and precision medicine—although not identical, are still very close in essence due to their common focus on the most important components of medical care for the patient, including:
• risk assessment (genetic testing of predisposition to diseases),
• prevention (intervention to prevent disease),
• detection (early detection of diseases at the molecular level),
• diagnostics (accurate diagnostics allows to individualize the treatment strategy),
• treatment (improvement of outcomes due to more accurate targets of exposure and prevention of the side effects of therapy),
• observation (active monitoring of response to therapy and a marker of disease progression).
This is not to say that a personalized (individual) approach is something completely new for clinicians. Earlier, certain morphofunctional parameters were used for this, reflecting the level of development of medical science and practice corresponding to the time. It is safe to say that the principle of treating the patient and not the disease has been known and widely used since ancient times. However, “an integrated, coordinated, and individualized approach to analyzing the occurrence and course of diseases for each patient,” considering environmental factors and the lifestyle of each person, including “the development of personalized treatments based on genomics, testing for disease susceptibility, prevention, combining diagnostics with treatment and treatment monitoring” [2, p. 4], began to form precisely from the beginning of the current century.
It took decades to move from the dominance of the concept of evidence-based medicine, in which the treatment of the patient was based mainly on data from randomized clinical trials calculated for the average patient to a healthcare model based on personalized care. It is this approach that makes it possible to detect quickly the targets for the effects of drugs and thereby achieve not only the best effect but also reduce the risk of developing adverse events due to the selection of the optimal drug dose. Finally, the possibility of making a more accurate and faster diagnosis, even when using expensive diagnostic technologies, will lead to significant savings in health care resources. Not to mention a significant reduction in mortality, especially among patients with oncological, neurological, cardiovascular, and other socially significant diseases. It can be assumed that personalized medicine will become a strong factor in shifting the focus from the treatment of diseases to their prevention. Faster patient access to information and better medical care will make it possible if not to prevent the disease then certainly to identify it at an early stage, and, in general, to increase the patient’s adherence to treatment and interaction with the attending physician, following his/her recommendations.
PERSONALIZED MEDICINE IN THE CONTEXT OF THE DEVELOPMENT OF MODERN HEALTH CARE
As mentioned, the penetration of personalized medicine into real clinical practice took place at the beginning of the 21st century. This was manifested not only in the acceleration of the introduction of innovative technologies due to translational research. It was during this period that the idea of a patient-centered approach was formed in the health-care system, which means that the interests of the patient are considered superior to those of medical institutions and their employees. Organizationally, an understanding of the importance of closed-loop medical care and the continuity of all its stages has taken shape. Value-based health-care technologies have begun to be applied, which involve a change in emphasis in the provision of medical care from focusing on process to results [3]. The trend of the recent decades is that trial and error medicine, moving towards medical consensus medicine, in turn, has given way to evidence-based medicine, and today evidence-based medicine is already giving way to personalized medicine. The medical profession acquires a research character, becomes closer to science than to art.
Another major factor in the breakthrough development of personalized medicine in the last two decades is the introduction of digital information technologies. Improvements in bioinformatics methods, genetic pathology registries, medical decision support systems, and artificial intelligence technologies have contributed to the emergence of “big data,” the importance of which, apparently, will increase. The greatest effect of big data should be expected in the predictive modeling of drugs. Based on the processing of gigantic amounts of genetic information, which are becoming more and more accessible, doctors will be able to prescribe unique drugs and apply new methods of treatment. Finally, the identification of disease patterns will improve the quality of prognostic estimates, identify risk profiles, offer effective treatment methods, and improve prevention.
The status of personalized medicine in our country is enshrined in the Strategy of Scientific and Technological Development of the Russian Federation, according to which the transition to high-tech health care promoting health protection is becoming one of the main priorities of the state [4]. In accordance with the national project Science, as part of the implementation of this trend, three genomic centers were created in 2019 and four world-class research centers in 2020, the tasks of which include R&D in the field of personalized medicine.
Impressive success with the use of new approaches has been achieved in oncology and oncohematology (this concerns improving patient survival). Clinical and population studies are actively developing in cardiology, endocrinology, neurology, and psychiatry, which contributes to the creation of support systems for medical decision making, the choice of specific drugs and their doses, and the formation of individual predictive risk scales. In pediatrics, rare (orphan) and genetically determined diseases attract the greatest research interest.
The choice of a personalized treatment and prevention strategy, especially in acute cardiovascular conditions, using big data will significantly increase the accuracy of an individual prognosis. Combined analysis of big clinical data (including images and data from prospective observation) with the involvement of omics technologiesFootnote 1 and machine learning methods seems promising for real clinical practice. Note that the pandemic of the new coronavirus infection became a serious incentive for the development of personalized approaches in the treatment of patients with infectious pathology, primarily with COVID-19 [5]. The experience accumulated over the past two years in dealing with the pandemic indicates the greatest clinical effectiveness of personalization of therapeutic strategies.
The main vectors in the development of personalized medicine in Russia are concentrated in the following areas:
• personalization of approaches to diagnostics, treatment, and prevention in real clinical practice (algorithms and the medical decision support system);
• oncogenomics;
• pharmacogenetics (including the selection of doses of drugs using computer programs);
• genetic risk assessment;
• prenatal diagnosis;
• study of molecular mechanisms of diseases, search for targets for therapy, study of small regulatory molecules and microvesicles, mitochondrial DNA, etc.;
• diagnostic panels;
• test systems, including those for prenatal diagnostics, including maternal blood diagnostics.
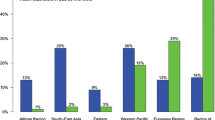
The process of introducing personalized methods of diagnostics, treatment, and prevention into practical health care will take more than one decade and will be inseparable from the development of biomedical science, expensive omics technologies, and bioinformatics. However, it is already obvious that this area has significant socioeconomic prospects [6]. Investment in personalized health care is expected to increase by more than 30% in the coming years. Today, in oncology, more than 70% of innovative drugs are targeted drugs; their number should increase by 69% in the next five years. From 2015 to 2020, the number of drugs with personalized indications for their use increased by 70%. Moreover, the likelihood that a drug will be approved for clinical use increases significantly if a specific biomarker is present in the mechanism of its action.
The benefits from the introduction of personalized medicine methods will affect all participants in the health-care system without exception: taxpayers, medical institutions, patients, and society as a whole (Table 1).
Personalized medicine: Main development tools. The accumulated experience suggests that rapid introduction of any new, especially expensive, technology requires a certain infrastructure. Personalized medicine involves an innovative ecosystem that includes universities and scientific institutions engaged in research in this area and business that creates a specific innovative product, as well as a health-care system that puts these developments into practice. Here it is necessary to emphasize once again the leading role of science and scientific institutions in building such an ecosystem. They should become a kind of academic biomedical hub, providing a comprehensive, integrative approach to the creation and promotion of medical technologies and their accessibility to the health-care system as a whole. It is in this context that the efforts of the state to form four world-class research centers in Russia should be considered; one of these centers, the Center for Personalized Medicine, was created on the basis of two research centers in St. Petersburg: the Almazov National Medical Research Center of the Ministry of Health of Russia—the initiator of the creation of the Center for Personalized Medicine—and the Institute of Experimental Medicine—a participant in the center (Fig. 1).

Ecosystem of the Almazov National Medical Research Center.
The purpose of the center under formation fully meets the current ideology of biomedical research and is aimed at building a scientific and industrial biomedical ecosystem for the development and implementation of technologies for diagnosing and treating diseases based on personalized medicine in health-care practice. This activity includes genetic risk assessment, pharmacogenetics and pharmacogenomics methods, disease biomodelling, genome modification, and the creation of drugs for gene therapy, as well as biomedical cell products using genome editing technologies to improve the quality of treatment and reduce mortality in cardiovascular diseases, concomitant metabolic disorders, oncohematological pathologies and some types of tumors, a number of infectious diseases, and pathologies of a genetic nature, including rare and poorly studied ones.
The activities of the Center for Personalized Medicine include four blocks that meet the main challenges for the health-care system.
(1) Population genetics and noncommunicable diseases of polygenic nature. Within this block, it is planned to develop algorithms for assessing the genetic risks of cardiovascular and metabolic diseases of a polygenic nature in the Russian population and to identify new predictors of the development of acute complications based on omics technologies and methods of personalized prevention. It is also necessary to develop educational programs for training specialists in the field of personalized medicine, pharmacogenetics and pharmacogenomics, and omics data processing.
Polygenic diseases are extremely diverse, but the focus is on those that have long acquired the character of noninfectious epidemics on a global scale—obesity, metabolic syndrome, type 2 diabetes mellitus, and cardiovascular pathologies. Obesity is an extremely heterogeneous condition in which some patients maintain good metabolic health and a favorable cardiovascular prognosis for many years, while others develop early dyslipidemia, arterial hypertension, hyperuricemia, and dysglycemia with accelerated formation of atherosclerotic changes and cardiovascular diseases. Many different factors, including phenotypic (anthropometric, behavioral, psychological, hormonal, etc.) and molecular genetic factors, predetermine the prognosis of the health status of obese patients.
We have studied the relationship of the obesity phenotype with the biomarker profile and the response to weight-reducing interventions. The relationship between the level of inflammation markers (C-reactive protein) and the degree of obesity and the nature of the distribution of adipose tissue was revealed—in visceral obesity (body mass index ≥30 kg/m2, waist/hip ratio >0.9 for men and >0.85 for women), the median of its level was 3.48 ng/mL, while in the peripheral one (body mass index ≥30 kg/m2, waist/hip ratio ≤0.9 for men and ≤0.85 for women), it was 0.93 ng/mL (p = 0.023). A high level of fibrosis markers (type 3 procollagen, galectin-3) is associated with a high risk of the development of cardiovascular diseases. According to our data, the decrease in fibrosis markers, as well as markers of inflammation during treatment, was substrate-dependent and was observed to a greater extent in patients with initially higher levels, regardless of the body weight dynamics. This suggests the presence of an obesity phenotype with a profibrogenic status, which improves with normalization of the lifestyle, regardless of the degree of weight loss. This statement is also supported by the data of experimental studies, which have shown that a high-fat diet is associated with a worse prognosis of ischemic myocardial damage even in the absence of obesity and other metabolic disorders [7].
The approach to the study of polygenic hereditary traits and a number of pathologies (obesity, type 2 diabetes mellitus, coronary heart disease) differs to a large extent from the study of the nature of rare diseases. Polygenicity implies a small contribution of individual DNA variants to the probability of developing a particular phenotype; therefore, it requires a much larger volume of studies (in terms of the number of participants), as well as the availability of detailed clinical information about each of the participants in the study to take into account environmental effects as much as possible. Whole genome sequencing technologies have made it possible to detect a large array of biomarkers associated with various polygenic phenotypes. The search for genes associated with polygenic diseases still remains an unsolved problem. The standard method for studying the genetics of such diseases is the genome-wide association search (GWAS). However, it only points to certain regions in DNA, which can contain up to 100 genes.
To overcome this difficulty, a bioinformatic genetic risk prediction program, GPrior [8], was developed, which predicts the role of genes with an as yet unknown mechanism of action. The model is based on an ensemble of several machine learning methods and uses the functional relationship between known, on the one hand, and as yet undiscovered disease-associated genes, on the other. As initial data, the model uses an array of genes with a known functional role in the pathogenesis of coronary heart disease (CHD) (for example, regulating cholesterol secretion), as well as information on molecular processes (expression, interactions between proteins, etc.). To validate the model, 37 genes significantly associated with CHD were studied, but the molecular mechanism of their impact on the risk of the disease was not yet known. Subsequent use of the algorithm to analyze registries of patients with coronary artery disease showed that the GPrior ensemble of classifiers predicts the presence of genes, the significance of which is subsequently confirmed in large-scale studies using both GWAS and exome sequencing, which guarantees reliable gene detection.
The use of omics biomarkers, big data technologies, and machine learning will significantly increase the accuracy of an individual prognosis and personalize treatment strategies. An example is the model developed in our center to predict the development of aortic aneurysm. Atherosclerosis and other diseases of the aorta can lead to a violation of the mechanical properties of its walls and the formation of an expansion (aneurysm)—a condition that threatens to rupture the aorta with a fatal outcome. In this case, the disease is sometimes asymptomatic and the patient may not receive timely surgical treatment to prevent complications.
Often, an aortic aneurysm is found incidentally on an ultrasound of the heart for other indications. Today, based on the analysis of data from more than 78 000 echocardiographic studies, we have developed a predictive model using machine learning methods that allows us to predict the detection of an aortic aneurysm during a repeat echocardiographic study with 82% accuracy, if the results of the previous one and the main clinical characteristics of the patient (gender, age, comorbidities) are known. Thus, based on the data of an echocardiographic study performed for any reason in patients without signs of aortic aneurysm, it is possible to predict with high accuracy the risk of developing this disease in the future and plan the further follow-up accordingly.
The use of the proposed prognostic model will improve the efficiency of screening for the detection of aortic aneurysm and prevent the development of fatal complications, as well as reduce the need for expensive and high-risk emergency cardiac surgery on the aorta [9].
Such models are being developed to predict recurrent cardiovascular events and the development of diabetes mellitus and to choose the optimal therapy.
(2) Unknown, rare, and genetic diseases. The tasks of this block involve the development of a set of technologies and the creation of a world-class scientific and educational infrastructure for personalized diagnosis and treatment of diseases of a genetic nature, including rare, poorly studied, and even unknown ones, the identification of molecular mechanisms, and the determination of new targets for personalized therapy, including the creation of innovative gene therapy drugs.
The main problems of pathologies of a genetic nature, most of which are rare, are associated, first, with their low prevalence, which leads to a lack of knowledge and experience on the part of specialists, and second, with their chronic, progressive, and life-threatening nature. That is why today they require special attention. The specificity of the approach to their study lies in the need to form a single patient-oriented structure, to create and maintain registers of patients with rare and genetically determined diseases, and to implement fundamental projects aimed at identifying new specific genetic determinants of rare and unknown pathology. An indispensable attribute of these projects should be the discovery of the molecular mechanisms of diseases of a genetic nature and the use of experimental cellular and animal models both for a deeper study of pathogenetic mechanisms and for the creation and testing of new gene therapy drugs.
One of the priority areas is the creation of a registry of genetically determined cardiomyopathies. The focus of our research is on the study of atypical, rare phenotypes with the search for features of mutations that led to the formation of such unique phenotypes. We mean a group of patients with rare forms of hypertrophic cardiomyopathy (mutations in poorly studied sarcomere protein genes and mutations in nonsarcomere genes and genes of various signaling cascades) and patients with rare forms of cardiomyopathy and rhythm disturbances.
Whole-exome sequencing and sequencing of targeted cardiopanels developed by us (a panel of genes for hypertrophic cardiomyopathy and its rare phenocopies—39 genes, as well as a panel including the full sequence of the giant titin gene and titin complex genes—four genes) turned out to be highly effective in determining the genetic basis of rare forms of hereditary myocardium diseases. Thus, we have identified a new variant of the RBM20 gene as the cause of the development of isolated arrhythmias. Usually, mutations in RBM20 are associated with myocardial remodeling, in particular, leading to the development of cardiomyopathic phenotypes, which is mainly associated with impaired splicing of the titin gene (TTN) and other sarcomere proteins. We described a rare association of the pathogenic RBM20 variant with isolated arrhythmias [10].
Within this block of studies, much attention is paid to the study of arrhythmogenic cardiomyopathy/right ventricular dysplasia, a rare hereditary myocardial disease characterized by a severe form of arrhythmia, the development of progressive heart failure, and a high risk of sudden cardiac death, the genetic and molecular cellular bases of the pathogenesis of which remain poorly understood. A study was made of the spectrum of microRNA molecules in the pericardial fluid of patients with a verified diagnosis of this disease (using high-throughput sequencing of small RNAs). As a result of bioinformatic analysis, it was possible to determine the full spectrum of miRNAs in samples of the pericardial fluid of patients, as well as to identify five differentially expressed types of miRNAs in patients with arrhythmogenic cardiomyopathy compared with the control group (hsa-miR-1-3p, hsa-miR-21-5p, hsa-miR-122-5p, hsa-miR-206, and hsa-miR-3679-5p). Analyzing the enrichment of a set of differentially expressed miRNAs made it possible to prove their association with other cardiovascular diseases and myopathies (including chronic atrial fibrillation, coronary artery disease, arrhythmia, hypertension), as well as to determine the main affected signaling pathways and biological processes (including the cell cycle, the development and differentiation of heart and skeletal muscle cells, and cell proliferation and apoptosis). Identification of specific extracellular miRNAs makes it possible to better understand the processes underlying pathogenesis and, in the long term, to identify biomarkers for more accurate and timely diagnosis and prognosis of the course of the disease [11].
Considering the specifics of many rare and little-studied diseases, the identification of their pathogenetic, including molecular, mechanisms, as well as the development of platforms for the creation and testing of drugs, is impossible without the use of biomodeling technologies for pathological processes. All leading medical centers in the world use this kind of genetic technology. Preclinical models of selected human diseases in vitro, ex vivo, and in vivo have already been created and described for further analysis. The most widely used are genetically modified model systems (rodents and zebrafish). An increase in the number of lines of transgenic animals that would have unique characteristics in terms of solving the problems of cardiology, neurology, oncology, and other research areas is a necessity dictated by the high level of medical research in the world and the personalized approach to treating patients.
As part of the work in this area, the Center for Biomodeling of Pathological Processes, has developed a biotechnological platform at our center to create new organoid and transgenic (mice, rats, fish) models that mimic various pathological processes—atherosclerotic, neurodegenerative, cardiological, endocrine, etc. The project uses the latest technologies of transgenesis (introduction of artificial genetic information into animal embryos by various methods). We get animals with desired properties (this can be a Cre/Lox system for genetic tracing, the introduction of mutations that turn off a gene or cause the replacement of one gene by another, and, finally, Crispr-Cas9,Footnote 2 which makes it possible to obtain zebrafish and rodent mutants already in the first generation). Unique lines of transgenic animals were created, in particular new transgenic lines of mice (Sox10, PLP, CHAT, DTA, ASCL, WNT) and lines of zebrafish (Sox10Cre: Zebrabow-S), which were used to study the mechanisms of formation of the nervous system and molecular genetic basics of the pathogenesis of neurodegenerative diseases [12].
We have shown that embryonic glial precursor cells in the early development of embryos of transgenic lines of mice and fish perform important functions associated with the correct development of individual organs and animals as a whole. These cells have properties reminiscent of the pluripotent properties of the neural crest and, depending on their location in the body, can transform into various cell types in peripheral tissues, including neurons. In addition, using the method of genetic tracing of a transgenic zebrafish line, it has been shown that neurons of the autonomic nervous system, as well as some populations of neurons of the central nervous system, originate not only from neural crest cells but also from Schwann progenitor cells, which can be considered as a new cellular material for regenerative medicine and a cellular source of mature neurons in case of their loss in neurodegenerative diseases accompanied by a catastrophic loss of neurons in the human central nervous system [12].
Diseases associated with excess calcification are widespread, especially in aging populations. Vascular calcification worsens the course and prognosis of diseases of the cardiovascular system, and calcification of the aortic valve leads to disruption of the heart. However, there are still no therapeutic approaches for the medical treatment of these diseases in the world, and, for example, about half a million expensive operations to replace a calcified valve are performed annually for the treatment of aortic stenosis alone. One of the most important limitations for the development of appropriate therapies is the lack of adequate platforms for testing promising compounds. To solve this problem, our world-class research center has developed a unique technological platform, on the basis of which potential compounds and genetically engineered constructs capable of suppressing excessive calcification can be tested [13]. When creating the platform, a collection of more than 100 samples of primary cell cultures from patients with aortic valve calcification was used. A technology for growing and testing the calcification potential (osteogenic potential) of these cells is proposed. Using the platform during cell cultivation, the expression of a number of genes associated with calcification was checked, and to obtain a more complete characterization of the pathological process, an analysis of the proteome of differentiating cells was carried out.
The platform allows testing substances and genetic constructs with potential anticalcification effects, as well as studying the molecular and cellular basis of pathological calcification, which, in turn, serves as an integral step in the search for therapy. During the approbation of the technological platform, we managed to identify the compound krenigacetate, which has an anticalcifying effect. Further, for all promising compounds, we study the mechanism of action using proteomics and the analysis of these data in the context of information about the patient.
Another striking example of the implementation of the principles of personalized medicine is the scientific project Creating a Register of Unknown, Rare, and Genetically Caused Diseases, which includes patients with pathologies the development mechanisms of which are not known or little studied, and diagnostics and therapy are not supported by standard protocols. Today, the register covers more than 200 children with 68 extremely rare nosologies. Using the sufficiently large clinical experience in managing patients with hereditary and rare diseases, the formed multidisciplinary teams of medical specialists, the possibility of applying the most state-of-the-art laboratory and genetic diagnostic equipment, and the means for implementing scientific projects using experimental studies, the foundation was prepared for the creation of a competence center Hereditary, Rare, and Little-Studied Diseases, which opened in 2021.
(3) Oncology. For this block, the task was to develop technologies and create a set of centers of competence for personalized diagnosis and therapy of cancer, including oncohematological diseases, tumors of the brain and gastrointestinal tract, and neuroendocrine tumors and to propose theranosticFootnote 3 approaches and a set of personalized drugs for the treatment of oncological diseases based on genetically modified cells of the immune system.
The scientific significance of fundamental developments in the field of oncology is determined by the use of the latest expression analysis technologies, including single cell genomic analysis in combination with epigenetic profiling and high throughput sequencing. In addition, data on the genomic structure of solid tumors and tumors of the hematopoietic system, obtained using the material of existing and future bioresource collections, combined with the possibility of detailed phenotyping of patients, will allow the development of new criteria that determine the chemo- and radiosensitivity of tumors, the creation of genetic diagnostic systems, and new genetically engineered drugs for the treatment of cancer and to determine new genetic markers for personalized targeted therapy for a number of tumors.
From the point of view of oncology, it is equally important to study the fundamental mechanisms of action of drugs based on the creation of chimeric antigen receptors, to use genetically modified immune cells, and to search for methods for obtaining biomedical cellular products of this kind.
Embryonic tumors are a common morphological form of malignant neoplasms of the central nervous system, with the number of high-risk patients being about 70%. The unsatisfactory survival rates of patients in high-risk groups, determined by the refractoriness of the tumor to the therapy and its high toxicity, necessitate the development of other strategies for antitumor treatment. Within this vector, using whole-exome sequencing of the new generation in embryonic tumors of the central nervous system, the effectiveness of therapy with drugs with a targeted mechanism of action is being studied based on the detection of identical molecular disorders. Carrying out a comparative analysis of DNA sequences in tumor cells and normal tissue of each patient makes it possible to isolate pathogenic mutations that are significant for the prognosis of the disease and serve as a potential therapeutic target.
As an additional option for patients of the studied prospective cohort with an unsatisfactory response to treatment after the completion of an intensive program or the development of a relapse of the disease, we use a metronomic chemotherapy regimen in combination with targeted therapy. In contrast to the standard, the proposed method is based on low-dose combination chemotherapy (etoposide + cyclophosphamide) in combination with antiangiogenic (sirolimus) and anti-inflammatory therapy (celecoxib) in a continuous mode. Our approach eliminates the need for long-term inpatient treatment. Reducing the intensity of therapy makes it possible to avoid the development of side effects, usually those associated with severe hematological toxicity and infectious complications. This reduces the cost of treatment.
The study of neuroendocrine tumors (NETs), which cause severe metabolic disorders, is aimed at solving the problem of diagnosing and predicting the recurrence of NETs of the pituitary and adrenal and parathyroid glands after surgical treatment. We are searching for new germinal (congenital) and somatic mutations responsible for the development of NETs of the adrenal and parathyroid glands and determining the recurrent or malignant course of these diseases. Optimal diagnostic approaches are being developed to predict the clinical course, response to therapy, and malignant nature before the development of metastases, including omics technologies, as well as modern imaging methods, such as PET/CT with various innovative radiopharmaceuticals. The search for targets for antitumor therapy is underway. As a result of study, markers of the prognosis of the course and response to therapy will be identified and a program will be formulated to assist in making decisions in the diagnosis and treatment of these diseases, which will reduce the time for diagnosis and improve prognosis—increase survival and reduce mortality.
Within the framework of the project, a target panel for sequencing genes responsible for the development of NETs was created using a next generation sequencing method. In patients with malignant pheochromocytoma, a germline mutation in the ZNRF3 gene, previously associated with the development of adrenocortical cancer, was detected for the first time. New methods of topical diagnostics of neoroendocrine tumors of the pituitary and parathyroid glands have been developed and tested. Data have been obtained that PET/CT with 11-C methionine can detect parathyroid adenoma in cases where traditional methods do not give a positive result. A technique for detecting MRI-negative adrenocorticotropic hormone-secreting pituitary adenomas has been developed and tested. According to the data obtained, 18F-FDG PET (radiopharmaceutical 18F-fluorodeoxyglucose) can be used to localize MRI-negative adrenocorticotropic hormone-secreting pituitary adenomas. According to our data, its use made it possible to increase the number of patients who achieved remission of hypercortisolism after transsphenoidal adenomectomy [14].
One of the new promising tools for cell therapy of malignant diseases is the technology of using CAR NK cells. Unlike CAR T cells, these effectors provide not only specific CAR-dependent destruction of tumor cells expressing target surface proteins but also anticancer activity due to a wide range of activating receptors characteristic of NK cells. On the way to creating an optimal platform for CAR NK cell therapy (Fig. 2), we performed a systematic analysis of feeder cells expressing combinations of activating-receptor ligands, in particular, CD40L, CD27, 4-1BBL, mbIL15, mbIL21, mbIL18, and mbIL12. In order to chart the direction of genetic modification of NK cells, an in-depth analysis of the transcriptome of single NK cells was carried out in comparison with T cells [15]. Unlike T cells, in which the dominant activation mechanism is controlled by the T cell receptor, NK cells do not have such a “nodal” receptor, so overexpression of activating receptors or their combinations in NK cells to stimulate their antitumor activity seems very promising.

Creation of a unified technological and scientific platform for the development of cellular immunotherapy for oncological diseases.
Only a few coreceptors, such as CD5, CD27, and CD28, are expressed by T cells, and they are practically absent in NK cells. Interestingly, despite the lack of CD28 expression in NK cells, second-generation CD28-based CARs show stronger activity in NK cells than first-generation CARs. This may be due to the fact that the main elements of the signaling apparatus are present in NK cells at levels comparable to those of T cells. Surprisingly, NK cells express more CD3zeta (CD247) than T cells, so a side-by-side comparison of cytotoxic activity induced by first-generation CARs in T and NK cells would be interesting [15].
Malignant brain tumors, both primary neuroepithelial tumors (Grade III and Grade IV) and secondary intracerebral tumors (brain metastases), are one of the main causes of death from oncological pathology in adult and pediatric populations. A promising method for their treatment is the use of targeted drugs directed to the membrane-bound form of the heat shock protein Hsp70 to visualize the neoplasm and target delivery of antitumor agents (including radioisotopes).
According to the data we obtained, using the method of inverted confocal microscopy, the expression of the membrane-associated heat shock protein Hsp70 on tumor cells of the central nervous system in adult patients (including astrocytoma, glioblastoma, ependymoma) was demonstrated for the first time. This result provides a scientific rationale for the development of anticancer theranostic drugs that recognize mHsp70-positive cancer cells. It was shown that expression of the Hsp70 protein is observed in viable cells of glioblastoma multiforme of adult patients but not in cells of the necrotic zone (Fig. 3). A positive correlation was noted between the level of Hsp70 expression and the invasive potential of tumor cells. The data obtained indicate the possibility of targeting anticancer drugs specifically to the population of viable mHsp70-positive tumor cells.

Development of the peptide drug RAS70 against membrane-bound Hsp70 on cancer cells for targeted intraoperative diagnosis of malignant neoplasms.
To date, the development of a protocol for assessing the expression of membrane-bound Hsp70 on tumor cells obtained from biopsy material has been completed and Hsp70 has been analyzed on cancer cells obtained from neurooncological patients. In the course of a separate stage of research, in order to increase the theranostic properties of agents (antibodies, RAS70 peptide), the latter were conjugated with nanosized gold preparations (AuNPs) or superparamagnetic iron oxide nanoparticles (SPIONs), which permit, on the one hand, a diagnostic effect and, on the other, suppress tumor growth [16]. High-Z gold nanoparticles (AuNPs) conjugated to a target antibody can help improve tumor control in radiation therapy while minimizing radiotoxicity to adjacent healthy tissue. To evaluate the behavior of nanoparticles in vivo, we developed a pharmacokinetic model that mimics the uptake and distribution of AuNPs in mice. Multiscale Monte Carlo simulations were performed for AuNPs and SPIONs in tumor cells at the cellular and molecular levels to determine the increase in radiation dose and the formation of chemical radicals in the vicinity of AuNPs [17]. A biologically based mathematical model has been developed to predict the biological response of AuNPs to radiation amplification. Although simulations of AuNPs showed a clear increase in dose, simulations associated with the formation of chemical radicals and the induction of DNA strand breaks caused by aggregates of AuNPs showed only a slight increase in dose. Differences in the modeled changes at the molecular and cellular levels indicate that further research is needed to understand better the impact of physical, chemical, and biological parameters in preclinical experimental settings prior to the transition of these AuNPs models into cancer radiotherapy.
In more than 80% of cases, after radical treatment of breast cancer, regardless of the chosen methods of antitumor treatment, postmastectomy syndrome inevitably occurs and develops progressively. We have created a database “Data of Anamnesis, Complaints, Neuropsychological Examination, Neurological Status, and the Value of Biomarkers (ICAM1, PECAM1) in Patients with Postmastectomy Syndrome,” which allows us to analyze the state of the central and peripheral nervous system and endothelium depending on the method of treatment and to develop a personalized treatment rehabilitation approach.
With the help of functional MRI, we obtained new data on changes in the working networks of the resting brain in patients with postmastectomy syndrome, which correlate with clinical manifestations in the form of lymphedema, chronic pain syndrome, vertebrobasilar insufficiency, and depression, which is necessary for a more accurate diagnosis of the severity neurological disorders, as well as a personalized comprehensive treatment and rehabilitation approach [18].
We also found for the first time a significant increase in the expression of adhesion molecules ICAM-1, PECAM-1 and the content of neuron-specific enolase, a decrease in antibodies to NMDA receptors (in comparison with a group of healthy volunteers) and did not differ from groups of patients with chronic cerebral ischemia, which indicates a violation of the functions of the blood–brain barrier, suffering of brain tissue, and disruption of autoregulation processes in it and reflects a subclinical pathological process and the presence of endothelial dysfunction [19].
(4) Infectious diseases, microbial and antimicrobial therapy. The task that we solved in this block together with the Institute of Experimental Medicine was to develop personalized technologies for determining the risks of infectious diseases, including COVID-19, a set of vaccines and approaches to personalized infection prevention, and also the creation of a line of autoprobiotic preparations for modifying the microbiota in autoinflammatory, cardiovascular, and oncological diseases.
Several vaccine candidates are being developed under this project, in particular, innovative vaccines for the prevention of infectious complications in patients with chronic obstructive pulmonary disease (COPD). The goal is to obtain live vaccines based on beneficial strains of probiotic bacteria that carry proteins of pathogenic microorganisms on their surface. During the project, two new probiotic vaccine candidates against the influenza virus were developed, in which the antigens of the virus were exposed on the surface of the bacterium Enterococcus faecium L3. Vaccination of mice with them stimulated the formation of humoral and cellular immune responses. A protective efficacy study showed that mice with antibodies against viral antigens were best protected against lethal doses of the influenza virus, particularly pandemic influenza A/South Africa/3626/13(H1N1) pdm09 [20].
The goal of the other project we are implementing is the development of oral live bacterial vector vaccines based on the probiotic Enterococcus faecium L3 strain, the genome of which is modified with inserts of DNA fragments encoding SARS-Cov-2 proteins. In the course of this work, two vaccine candidates were created that demonstrated safety and immunogenicity in experiments on laboratory animals. Currently, preclinical studies on protection are being completed. Vaccine candidates under development have a number of competitive advantages over the existing SARS-Cov-2 vaccines: they can be administered orally as a fermented milk product and stored at +4°C; the manufacturing process is extremely simple; and the finished product does not require purification. In addition, vaccine technology can be quickly adapted to new pathogen variants [21].
In modern medical practice, the concept of therapy for an infectious disease, aimed at the destruction of the pathogen, must be replaced by a set of therapeutic measures aimed at restoring the natural microbiocenosis characteristic of a particular individual. The first step towards achieving this goal should be an accurate diagnosis of the causative agent of the disease and its genetic characteristics, including the study of the presence of antibiotic resistance genes, virulence genes, and the nature of their expression. Only after that, in order to achieve an effective result, can one proceed to personalized therapy, aimed either at reducing the percentage of the pathogen in the microbiocenosis or replacing it with a bacterial variant of the same species with a low pathogenicity potential.
Today, we are implementing two projects related to personalized therapy, which uses probiotic and autoprobiotic (that is, isolated from a particular patient) bacteria. As part of one of them, an approach is being developed to improve the long-term results of treatment of cancer patients. In the course of our research, the features of the intestinal microbiota in patients with different tumor locations were revealed, and the effectiveness of the use of autoprobiotic and probiotic support in the perioperative and early postoperative periods of treatment for colorectal cancer and gastric cancer was evaluated. As a result of studies of the feces of patients with colorectal cancer, it was shown that in 100% of cases there is dysbiosis, which is aggravated after surgical treatment. The use of autoprobiotics or the probiotic Enterococcus faecium L3 led to a decrease in the content of opportunistic bacteria, including bacterial tumor markers. With this maintenance therapy, a rapid recovery of the functions of the gastrointestinal tract was observed and the patients showed compliance (adherence to treatment).
In another project, personalized microbial therapy was used to correct somatic pathologies (metabolic syndrome and type 2 diabetes). The technology we have used in applying the components of our own microbiota (autoprobiotics), which has world priority, has undeniable advantages due to the adaptation of indigenous bacteria to the host organism, immunological tolerance to our own microbiota, and mutually beneficial conditions for the existence of components. In the course of study, already after the first course of autoprobiotics, against the background of the disappearance or reduction of opportunistic pathogenic bacteria, there was a tendency to increase the number of enterococci, lactobacilli, and fecalibacteria, a decrease in fasting glucose and glycated hemoglobin, a steady tendency towards normalization of the lipidogram, and a decrease in the weight of patients [22].
It should be noted that for therapeutic purposes we use not only probiotic and autoprobiotic strains of bacteria but also conditionally pathogenic microorganisms. Thus, one of the projects is devoted to the development of oncolytic bacterial strains, and on their basis, recombinant proteins for the treatment of neoplasms of the intestine, pancreatobiliary zone, and brain tumors.
In the course of research, the in vitro cytotoxic effect of various bacterial strains of Streptococcus pyogenes was evaluated in relation to PANC02 pancreatic cancer cell lines, C6 glioma, human astroglioma U251, and hepatoma 22a. Two strains of the S. pyogenes M49 serotype with pronounced oncolytic properties were found. The cytotoxic efficacy of S. pyogenes was compared with the effect of standard chemotherapy drugs, nerve growth factor (NGF), and cathelicidins LL37, PG-1 on the brain tumor cell culture. The absence of a cytotoxic effect of oncolytic S. pyogenes on normal cells was shown.
* * *
An analysis of even the first results of the work of a world-class Scientific Center suggests that the presence of significant state support with a high degree of readiness of scientific teams can become a decisive factor in accelerating the generation of new scientific data and creating innovative technologies in the field of personalized medicine. However, it would be naive to believe that this will happen quickly. It is likely that the process of bringing more and more diseases into the orbit of personalized treatment will turn out to be gradual and, as already mentioned, will require more than a dozen years. Here, apparently, the most difficult thing will be the formation of infrastructure and training of highly qualified personnel for the introduction of personalized medicine technologies into healthcare practice. The list of such proposals is not limited to those presented in Table 2, and with further work in this direction—the development of biomedicine and artificial intelligence technologies—it will be significantly adjusted. First of all, this will apply to the technologies of regenerative medicine and adaptive immunotherapy, the use of personal vaccines, neurointerfaces, and bioprosthetics made from autologous materials. However, even today one can see how big the gap is between innovations and the willingness of the professional community to accept them.
To reduce this gap, it is important to develop professional education, in which more than university training is important, where most programs already contain courses in personalized medicine, pharmacogenetics, and digital technologies in medicine. It is necessary to implement the teaching of new technologies as part of the retraining of doctors and their advanced training in areas such as oncology, cardiology, endocrinology, pediatrics, neurology, and psychiatry, in which the demand for knowledge in pharmacogenetics and the use of genetic testing results is extremely high.
The future of personalized healthcare lies in quality education, collaboration between scientists and practitioners, and a patient-centered approach, which assumes that the medical problems of our citizens will be solved effectively using the most modern technologies.
Notes
Omics technologies are a set of modern molecular technologies that are used to study the body at different levels, from reading genetic information (genomics), identifying factors regulating gene expression (epigenomics), and determining the activity of genes (transcriptomics) and their protein products (proteomics) to determining the composition and concentration of end decay products (metabolomics). (Hereinafter, Ed.)
CRISPR/Cas is a system of adaptive acquired immunity of bacteria and archaea, aimed at destroying foreign DNA that has entered the cell, for example, phages or plasmids.
Theranostics is an approach to the creation of pharmaceutical compositions, which consists in a comprehensive solution of therapeutic and diagnostic problems by creating drugs that are both an early diagnostic tool and a therapeutic agent.
REFERENCES
I. S. Chan and G. S. Ginsburg, “Personalized medicine: Progress and promise,” Annu. Rev. Genomics Hum. Genet. 12, 217–244 (2011).
I. I. Dedov, A. N. Tyul’pakov, I. P. Chekhonin, et al., “Personalized medicine: Current state and prospects,” Vestn. Ross. Akad. Med. Nauk, No. 12, 4–12 (2012).
E. V. Shlyakhto, A. O. Konradi, N. E. Zvartau, and L. G. Ratova, Value Medicine, or Value-Based Medicine (OOO Info-ra, St. Petersburg, 2019) [in Russian].
Strategy for Scientific and Technological Development of the Russian Federation (Approved by Decree of the President of the Russian Federation of December 1, 2016, No. 642). https://online.mai.ru/StrategySTD% 20RF.pdf?referer=https%3A%2F%2Fwww.google.com%2F
J. J. Monsuez, “Editors network of the National Societies of Cardiology Journals (NSCJ): COVID-19 and the heart: Insights from the National Society of Cardiology Journals,” Eur. Heart J. 42 (39), 4003–4005 (2021). https://doi.org/10.1093/eurheartj/ehab262
K. K. Jain, Personalized Medicine: Scientific and Commercial Aspects (Jain PharmaBiotech, Basel, 2015).
A. Simanenkova, S. Minasian, T. Karonova, et al., “Comparative evaluation of metformin and liraglutide cardioprotective effect in rats with impaired glucose tolerance,” Sci. Rep. 11, 6700 (2021). https://doi.org/10.1038/s41598-021-86132-2
N. Kolosov, M. J. Daly, and M. Artomov, “Prioritization of disease genes from GWAS using ensemble-based positive-unlabeled learning,” Eur. J. Hum. Genet. 29, 1527–1535 (2021). https://doi.org/10.1038/s41431-021-00930-w
O. Metsker, D. Kopanitsa, O. Irtyuga, and V. Uspenskiy, “Dynamic aortic aneurism risk factors,” Stud. Health Technol. Inform. 285, 130–135 (2021).
Y. Vakhrushev, A. Kozyreva, A. Semenov, et al., “RBM20-associated ventricular arrhythmias in a patient with structurally normal heart,” Genes (Basel) 12 (1), 94 (2021). https://doi.org/10.3390/genes12010094
A. A. Khudiakov, D. D. Panshin, Y. V. Fomicheva, et al., “Different expressions of pericardial fluid microRNAs in patients with arrhythmogenic right ventricular cardiomyopathy and ischemic heart disease undergoing ventricular tachycardi, ablation,” Front Cardiovasc. Med. 19 (8), 647812 (2021). https://doi.org/10.3389/fcvm.2021.647812
D. Kamenev, K. Sunadome, M. Shirokov, et al., “Schwann cell precursors generate sympathoadrenal system during zebrafish development,” J. Neurosci. Res. 99 (10), 2540–2557 (2021).
A. Rutkovskiy, A. Malashicheva, G. Sullivan, et al., “Valve interstitial cells: The key to understanding the pathophysiology of heart valve calcification,” J. Am. Heart Assoc. 6 (9), e006339 (2017). https://doi.org/10.1161/JAHA.117.006339
L. G. Yanevskaya, T. Karonova, I. V. Sleptsov, et al., “Clinical phenotypes of primary hyperparathyroidism in hospitalized patients who underwent parathyroidectomy,” Endocr. Connect. 10 (2), 248–255 (2021). https://doi.org/10.1530/EC-20-0515
S. Kulemzin, I. Evsyukov, T. Belovezhets, et al., “Horses for courses in the era of CARs: Advancing CAR T and CAR NK cell therapies,” J. Pers. Med. 11, 1182 (2021). https://doi.org/10.3390/jpm11111182
M. Shevtsov, S. Kaesler, C. Posch, et al., “Magnetic nanoparticles in theranostics of malignant melanoma,” EJNMMI Res. 11 (1), 127 (2021). https://doi.org/10.1186/s13550-021-00868-6
W. B. Li, S. Stangl, A. Klapproth, et al., “Application of high-Z gold nanoparticles in targeted cancer radiotherapy-pharmacokinetic modeling, Monte Carlo simulation and radiobiological effect modeling,” Cancers (Basel) 13 (21), 5370 (2021). .https://doi.org/10.3390/cancers13215370
M. L. Pospelova, T. A. Bukkieva, A. Yu. Efimtsev, et al., RF Patent 2754059, Byull. Izobret., No. 24 (2021).
T. A. Bukkieva, M. L. Pospelova, A. Yu. Efimtsev, et al., “Functional reorganization of brain networks in patients with postmastectomy syndrome,” Sovr. Probl. Nauk. Obraz., No. 6, 183 (2020). https://science-education.ru/ru/article/view?id=30448
Y. Desheva, G. Leontieva, T. Kramskaya, et al., “Developing a live probiotic vaccine based on the Enterococcus faecium L3 strain expressing influenza neuraminidase,” Microorganisms 9 (12), 2446 (2021). https://doi.org/10.3390/microorganisms9122446
A. Suvorov, T. Gupalova, Y. Desheva, et al., “Construction of the enterococcal strain expressing immunogenic fragment of SARS-Cov-2 virus,” Front. Pharmacol., No. 12, 3753 (2022). https://doi.org/10.3389/fphar.2021.807256
L. V. Gromova, E. I. Ermolenko, A. L. Sepp, et al., “Gut digestive function and microbiome after correction of experimental dysbiosis in rats by indigenous bifidobacteria,” Microorganisms 9 (3), 522 (2021). https://doi.org/10.3390/microorganisms9030522
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The author declares that he has no conflicts of interest.
Additional information
Translated by B. Alekseev
RAS Academician Evgenii Vladimirovich Shlyakhto is Director General of the Almazov National Medical Research Center of the Ministry of Health of the Russian Federation.
Rights and permissions
About this article

Cite this article
Shlyakhto, E.V. Scientific Basics of Personalized Medicine: Realities and Opportunities. Her. Russ. Acad. Sci. 92, 671–682 (2022). https://doi.org/10.1134/S1019331622060041
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S1019331622060041