
Abstract
Cardiovascular disease (CVD) and depression are common diseases that lead to adverse health outcomes. Depressive Symptoms may be a risk factor for CVD. But few studies focused on the impact of socioeconomic factors, common medical history and dietary intake about this association. This study analyzed National Health and Nutrition Examination Survey (NHANES) 2007–2016. Complex sampling-weighted logistic regression models were used to compare the odds ratios (ORs) of CVD in participants with different depressive symptoms. 11,516 NHANES participants aged ≥ 40 years were included in the final analysis, of whom 1842 had CVD. Compared with participants with no/minimal depression, participants with mild, moderate, and moderately severe/severe depression had OR values of 1.25 (95% CI 1.01–1.54), 1.98 (95% CI 1.32–2.96), and 2.41 (95% CI 1.63–3.57). The association of depressive symptoms with CVD follow a dose-dependent pattern. The interactions of depressive symptoms with gender (Interaction P = 0.009), diabetes (Interaction P = 0.010), household income level (Interaction P = 0.002), dietary cholesterol intake (Interaction P = 0.017) on CVD were observed. More severe depressive symptoms are associated with increased risk of CVD in US population. The association may be more pronounced in the female population, population with diabetes, low family income level, or high dietary cholesterol intake.
Similar content being viewed by others

Introduction
Cardiovascular disease (CVD) is a group of heart and vascular diseases, mainly represented by ischemic heart disease and stroke, that are the leading causes of death and disability globally. The Global Burden of Disease Study shows that the incidence of CVD is on the rise worldwide, with total cases reaching 523 million and deaths from CVD reaching 18.6 million in 20191. Therefore, it is crucial to recognize and manage CVD risk factors. In addition to traditional risk factors, the impact of psychological factors on CVD has been paid increasingly more attention.
Depression is a prevalent chronic medical condition that affects thought, mood, and physical health, is one of the main causes of disability worldwide2. The Global Burden of Disease Study showed depression affected approximately 280 million people and accounted for more than 47 million disability-adjusted life-years in 20193. Multiple studies have reported associations between depression and a variety of CVDs, especially coronary heart disease and stroke4,5,6,7,8,9,10,11. There are many common pathogenic mechanisms in depression and CVD, including hypothalamic–pituitary–adrenal axis, autonomic dysfunction, genetic factors, etc12,13,14,15,16,17. Some potential factors may influence the association between depression and CVD through these co-pathogenic mechanisms. However, previous studies have not paid sufficient attention to these potential factors. the association of depression and CVD may be different by these neglected factors, such as common medical history, socioeconomic factors, dietary intake, and lifestyle. It is promising to identify the potential factors influencing the association between depression and CVD for the prevention and treatment of depression and CVD.
The Patient Health Questionnaire depression module (PHQ-9) is a 9-item self-administered instrument used for detecting depression and assessing severity of depression18,19. For more than two decades, numerous studies have determined the reliability of PHQ-9 for screening for depression18,19,20,21,22. And its simplicity makes PHQ-9 a useful clinical and research tool widely used in primary health care worldwide21. This study aimed to investigate the association between depressive symptoms (assessed by PHQ-9) and CVD, paying attention to the impact of common medical history, socioeconomic factors, dietary intake and lifestyle on this association.
Methods
Study participants
NHANES is a national survey of the health and nutrition status of the US population. The US National Center for Health Statistics (NCHS) is in charge of generating critical health statistics, and accomplishes this by utilizing a stratified, multi-stage probability sampling design that makes it possible for participants to be an accurate representation of the US civilian deinstitutionalized population23. The NCHS Research Ethics Review Board approved the NHANES protocol24. Written informed consent was obtained from each participant when NHANES was conducted.
This study obtained data on participants between 2007 and 2016 from the NHANES database. We focused on participants aged 40 years or older at baseline (n = 19,344). Since there were few cases with CVD under the age of 40, the 40-year-old cutoff was used in this study. Participants with depression screener and CVD questionnaire data were retained (n = 16,798). Then, participants with incomplete covariate information were excluded (n = 5282). Finally, A total of 11,516 participants were included in the analysis (Fig. 1).

Flowchart of participants selection.
Assessment of outcome
CVD was determined using a standardized medical condition questionnaire filled out during the individual interview. The detailed questionnaire and interview procedures are available on the NHANES website25. Participants were considered CVD patients if they answered “yes” to any of the following structured questions: Has a doctor or other health professional ever told you that you had congestive heart failure, coronary heart disease, angina (also called angina pectoris), heart attack (also called myocardial infarction), or stroke?
Assessment of depressive symptoms
Depressive Symptoms was assessed using the Patient Health Questionnaire-9 (PHQ-9). This is a self-reported assessment based on the nine signs and symptoms for depression on Diagnostic and Statistical Manual of Mental Disorders fourth edition. Detailed questionnaires are available from the NHANES. When responding to the nine symptom questions, participants answered according to one of the following categories: “not at all”, “several days”, “more than half the days”, and “nearly every day”. Depression severity can be defined by several cut points from the total score that ranges from 0 to 27: No/Minimal (0–4), mild (5–9), moderate (10–14), moderately severe (15–19) and severe (20–27). Due to the small number of participants with moderately severe or severe depression, they were combined into one group in this study.
Covariates
Information on age, sex (male, female), race/ethnicity (Hispanic and Mexican American, , non-Hispanic white, non-Hispanic black, or other race), educational level (less than high school, high school graduate/ equivalent, or more than high school), marital status (married/living with partner, widowed/separated/divorced, or never married), family income-poverty ratio (< 1.30, 1.30–3.49, ≥ 3.50), smoking status (current, former, or never), alcohol consumption (< 12 or ≥ 12 alcoholic drinks/year), and disease histories (including trouble sleeping, hypertension, diabetes, dyslipidemia, and cancer) was collected through questionnaires during the survey interviews. Based on the dietary information collected from the 24-h recall interviews, total daily dietary protein, sugar, fiber, cholesterol, caffeine intakes were obtained, and the Healthy Eating Index (HEI) 2010 was used to represent the overall quality of the diet (with scores ranging from 0 to 100, where higher scores represent better dietary quality)26. Data of body mass index (BMI), blood pressure, glycohemoglobin, total cholesterol, triglycerides, low-density lipoprotein, high-density lipoprotein, and serum creatinine were measured according to standard protocols. Based on serum creatinine, the estimated glomerular filtration rate (eGFR) was determined using the Chronic Kidney Disease Epidemiology Collaboration algorithm27. Hypertension was defined as measured systolic blood pressure (SBP) ≥ 140 mmHg, or/and diastolic blood pressure (DBP) ≥ 90 mmHg, or/and previous diagnosis of hypertension, or/and taking antihypertensive medicine. Diabetes was defined as measured glycohemoglobin level ≥ 6.5%, or/and previous diagnosis of diabetes, or/and taking anti-diabetes medicine. Dyslipidemia was defined as total cholesterol ≥ 200 mg/dL, triglycerides ≥ 150 mg/dL, low-density lipoprotein ≥ 130 mg/dL or high-density lipoprotein ≤ 40 mg/dL in males and ≤ 50 mg/dL in females. Obesity was defined as BMI ≥ 30 kg/m2.
Statistical analysis
Complex survey designs needed be considered because the NHANES samples were not straightforward random samples. Following the recommendations of the US Centers for Disease Control and Prevention28, we utilized appropriate weights for each analysis based on the selected variables. Continuous variables are expressed as mean ± standard error (SE), and comparisons between groups were made using Student's t-test. Categorical variables are expressed as percentages, and comparisons between groups were made using the chi-squared test. Complex sampling-weighted univariate logistic regression analysis was used to screen for covariables included in subsequent analyses. Complex sampling-weighted multivariate logistic regression models were established for the odds ratios (ORs) and 95% confidence intervals (95% CIs) between depressive symptoms and CVD. Variance inflation factor is used to evaluate the multicollinearity in multivariate logistic regression models. Likelihood ratio tests were used to assess the statistical efficacy of the model. Model 1 was adjusted for age, sex, race/ethnicity, education level, marital status, PIR. Model 2 was further adjusted for smoking status, alcohol consumption, BMI and HEI. Model 3 was further adjusted for disease histories (trouble sleeping, hypertension, diabetes, dyslipidemia, and cancer), blood pressure, glycohemoglobin, low-density lipoprotein, and eGFR. We developed regression models using not only depression severity, but also PHQ-9 score as a continuous variable. Thereafter, subgroup analyses stratified by sex, age, BMI, race/ethnicity, educational level, marital status, smoking status, alcohol consumption, trouble sleeping, hypertension, diabetes, dyslipidemia, cancer, eGFR, PIR, HEI, serum cotinine and dietary protein, sugar, fiber, cholesterol, caffeine intakes were conducted based on model 3. Meanwhile, interactions between PHQ-9 score and the above stratification variables were assessed. Furthermore, restricted cubic spline regressions were used to explore the dose–response association of PHQ-9 score and CVD in subgroups with significant interactions. All statistical analyses were performed using R version 4.1.2 (R Project for Statistical Computing), and P < 0.05 was regarded as statistically significant for all tests.
Ethics approval and consent to participate
The NCHS Research Ethics Review Board approved the NHANES protocol (https://www.cdc.gov/nchs/nhanes/irba98.htm). The NHANES has obtained written informed consent from each participant.
Results
Baseline characteristics
In this study, 11516 NHANES participants aged 40 years or older were included in the final analysis, of whom 1842 had CVD. Figure 2 shows the incidence of CVD in different depressive states (including the unweighted and weighted data). Baseline characteristics of patients grouped according to depressive states were listed in Table 1. Participants with more severe depressive symptoms were more likely to be younger, female, non-Hispanic black, Hispanic, non-married, and current smokers, had lower education levels, lower family income level, lower high-density lipoprotein, lower HEI, lower dietary protein, fiber, cholesterol intakes and higher BMI, higher glycohemoglobin, higher triglyceride, higher dietary caffeine intake. In addition, participants with more severe depressive symptoms had higher prevalence of CVD (heart failure, coronary heart disease, stroke, angina, myocardial infarction), trouble sleeping, hypertension, and diabetes.

Incidence of CVD in different depressive states. CVD: cardiovascular disease.
Association of depressive symptoms with CVD
Table 2 presented survey-weighted multivariate logistic regression results. Univariate logistic regression analysis was used to screen for covariables included in multivariate logistic regression (Supplementary Table 1). And variance inflation factor is used to evaluate the multicollinearity in the regression model, and variance inflation factor is all less than 5, indicating that the collinearity between variables is reasonable (Supplementary Table 2). Likelihood ratio tests indicated that model 3 had the best statistical performance (Supplementary Table 3). Multivariate adjusted model 3 showed that depressive Symptoms was positively associated with CVD in participants (Supplementary Table 4). Compared with participants with no/minimal depression, participants with mild, moderate, and moderately severe/severe depression had OR values of 1.25 (95% CI, 1.01–1.54), 1.98 (95% CI, 1.32–2.96), and 2.41 (95% CI, 1.63–3.57), respectively. Moreover, the association of depressive symptoms with CVD may be in a dose-dependent manner. When the PHQ-9 depression score was used as a continuous variable, the OR value for CVD was 1.06 (95% CI, 1.04–1.08). In addition, the associations of depressive symptoms with heart failure, coronary heart disease, stroke, angina, and myocardial infarction was similarly significant when assessed separately (Table 2).
Subgroup analysis
Subgroup analyses were conducted to investigate the association of depressive symptoms with CVD in different populations. Table 3 shows that the association between depressive symptoms and CVD remains significant in most subgroups. Interestingly, we observed interactions of depressive symptoms with multiple stratification factors (gender, diabetes, Family income-poverty ratio) on CVD. Compared with participants without depression/mild depression, participants with moderate severe/severe depression had an OR value of 2.98 (95% CI, 1.81–4.91) in the female population, whereas the OR value was 1.32 (95% CI, 0.74–2.37) in the male population. Compared with participants without depression/mild depression, participants with moderate severe/severe depression had an OR value of 4.41 (95% CI, 2.19–8.88) in the population with diabetes, whereas the OR value was 1.87 (95% CI, 1.11–3.17) in the population without diabetes. Compared with participants without depression/mild depression, participants with moderate severe/severe depression had an OR value of 2.66 (95% CI, 1.75–4.03) in the population with low family income level, whereas the OR value was 0.93 (95% CI, 0.20–4.39) in the population with high family income level. To further assess the impact of various important nutrients on the association between depression symptoms and CVD, subgroup analyses were performed with dietary protein, sugar, fiber, cholesterol, and caffeine intakes as stratification factors (Supplementary Table 5). Compared with participants without depression/mild depression, participants with moderate severe/severe depression had an OR value of 5.21 (95% CI, 3.06–8.85) in the population with high dietary cholesterol intake, whereas the OR value was 1.36 (95% CI, 0.82–2.26) in the population with low dietary cholesterol intake.
Restricted cubic spline analysis
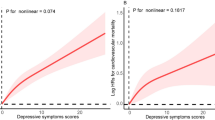
The results of restricted cubic spline analysis showed the dose–response association of PHQ-9 score and CVD in subgroups with significant interactions. Figure 3A shows that the dose–response association of PHQ-9 score and CVD were more pronounced in the female population than in the male population. Figure 3B shows that the dose–response association of PHQ-9 score and CVD were more pronounced in the population with diabetes than in the population without diabetes. Figure 3C shows that the dose–response association of PHQ-9 score and CVD were more pronounced in the population with low family income level than in the population with high family income level. Figure 3D shows that the dose–response association of PHQ-9 score and CVD were more pronounced in the population with high dietary cholesterol intake than in the population with low dietary cholesterol intake.

The OR of CVD with PHQ-9 score stratified by gender, diabetes, family income level, and dietary cholesterol intake. OR: Odds ratio; CI: Confidence interval. CVD: cardiovascular disease; PHQ-9: Patient Health Questionnaire-9 (depression score).
Sensitivity analysis
Sensitivity analyses were performed to test the robustness of the results, including removing some NHANES data and modifying several covariates. The association between depressive symptoms and CVD was significantly positive in multiple sensitivity analysis results (Supplementary Table 6).
Discussion
Our study found a significant positive association between depressive symptoms and CVD, even after adjusting for socioeconomic factors, common medical history, and dietary intake. Compared to participants with No/Minimal depressive symptoms, participants with Moderate depressive symptoms had a 98% increased risk of CVD, Participants with Moderately severe/Severe depressive symptoms had a 141% increased risk of CVD. When compared with other risk factors in regression models, the effect of even Moderate depressive symptoms on CVD risk exceeded that of hypertension, diabetes, or dyslipidemia. And there may be a positive dose–response curve between depressive symptoms and CVD. Moreover, the association of depressive symptoms and CVD may be more pronounced in the female population, population with diabetes, population with low family income level, or population with high dietary cholesterol intake.
Some previous studies have investigated the association of depression with CVDs. Multiple meta-analyses have shown a substantial increase (60–80%) in the risk of coronary heart disease associated with depression5. In addition, Meijer et al. conducted a meta-analysis of over 25 years of research into the relationship between post-myocardial infarction depression and cardiac prognosis and found that depression was consistently associated with worse prognosis after myocardial infarction29. In a pooled analysis of 563 255 participants in 22 cohorts, Harshfield et al. found that baseline depressive symptoms were associated with CVD incidence, including at symptom levels lower than the threshold indicative of a depressive disorder4. Similarly, a recent meta-analysis suggests that depression has a significant negative impact on CVD development and CVD outcomes30. Several other studies based on the NHANES database have suggested an association between depressive symptoms and cardiovascular mortality31,32,33. However, the current findings suggest that the association between depressive symptoms and CVD risk cannot be explained primarily by established cardiovascular risk factors, including blood pressure, serum lipids, obesity, and diabetes. And few studies have further explored the factors that influence the association between depressive symptoms and CVD. Xu et al. found that Moderate recreational activity modified and mediated the associations between depressive symptoms and CVD based on NHANES 2007–201634. Lu et al. discovered an interaction effect of depressive symptoms and inflammation on the occurrence of CVDs based on NHANES 2007–201635. The factors that influence the association between depression and CVD are not well investigated. Therefore, our study further included some potential influencing factors such as sleep problems, socioeconomic status, multiple dietary intakes, etc., which were not fully considered in previous studies. And our study investigated the influence of these factors on the association between depressive symptoms and CVD. Notably, in addition to gender and diabetes, family income level and dietary cholesterol intake were found to possibly influence the association between depression and CVD. This suggests that the population with low family income level or high dietary cholesterol intake may pay more attention to screening for depression and CVD. This is a promising direction worthy of further research.
For the association between depression and CVD, some possible mechanisms have been proposed. There are data on depression affecting the autonomic nervous system, endothelial function, neurohormonal changes, platelet receptors and function, clotting factors, and pro-inflammatory cytokines, etc36,37,38,39. The association between depression and CVD may be potentially gender-differentiated in this study, and several previous studies have reported similar results40,41,42. This may be related to sex hormone secretion (e.g., estrogen and progesterone) and related neurotransmitters43,44. Current studies have shown that abnormal stress of depression activates the hypothalamic–pituitary–adrenal (HPA) by increasing the concentration of glucocorticoids, which promotes the occurrence and development of cardiovascular diseases45. Sex hormones play an important role in the regulation of the HPA axis46, which may be the underlying physiological mechanism of the sex difference between depression and cardiovascular diseases. In addition, specific environmental exposures and social processes specifically influence gender differences, involving nutrition in daily life, cultural behaviors, stress responses, and disease prevention47,48. Further studies are necessary to explore the underlying specific mechanisms. We also found that diabetes may have affected the association between depression and CVD, which is consistent with previous studies49. However, the exact role of diabetes in this process remains unclear. There is evidence that depression and type 2 diabetes share biological origins, particularly overactivation of innate immunity leading to a cytokine-mediated inflammatory response, and potentially through dysregulation of the HPA axis50. This may lead to a potential interaction between depression and diabetes on CVD. Our study also found that low family income level and high dietary cholesterol intake may be enhanced the association between depression and CVD. Inoue et al. have suggested that the HPA axis, which is essential for regulating glucocorticoid production by the adrenal glands, may be prone to dysregulation with low socioeconomic status and poor health behaviors49. Sullivan et al. proposed that socioeconomic disadvantage can lead to disparities in access, treatment, and care, which may also increase cardiovascular risk through shared stress pathophysiology with depression51. Further direct evidence is needed to confirm the effect of socioeconomic status and dietary intake on the association between depression and CVD.
This study focuses on the impact of socioeconomic factors, common medical history, and dietary intake on the association between depressive symptoms and CVD, which provides a reference for the prevention and treatment of depression and CVD in susceptible population. But we also recognize several shortcomings. Depressive symptoms were assessed by a single PHQ-9 depression score and may not fully reflect participants' depressive status. And PhQ-9 does not represent clinical diagnosis. Next, CVD was determined based on the participants' self-reported history of disease, which may have some bias. Finally, this study is cross-sectional. The cross-sectional analysis does not show directionality and we cannot infer if depression leads to CVD or vice versa. Further carefully designed prospective studies are needed to confirm the results of this study.
Conclusion
More severe depressive symptoms are associated with increased risk of CVD in the US population. The association of depressive symptoms and CVD may be more pronounced in the female population, population with diabetes, population with low family income level, or population with high dietary cholesterol intake.
Data availability
The data used in this study are openly available in the NHANES website: NHANES Questionnaires, Datasets, and Related Documentation (https://wwwn.cdc.gov/nchs/nhanes/Default.aspx).
References
Roth, G. A. et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 76, 2982–3021. https://doi.org/10.1016/j.jacc.2020.11.010 (2020).
Malhi, G. S. & Mann, J. J. Depression. Lancet Lond. Engl. 392, 2299–2312. https://doi.org/10.1016/s0140-6736(18)31948-2 (2018).
Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England) 396, 1204–1222, (2020).
Harshfield, E. L. et al. Association between depressive symptoms and incident cardiovascular diseases. Jama 324, 2396–2405. https://doi.org/10.1001/jama.2020.23068 (2020).
Carney, R. M. & Freedland, K. E. Depression and coronary heart disease. Nat. Rev. Cardiol. 14, 145–155. https://doi.org/10.1038/nrcardio.2016.181 (2017).
Wu, Q. & Kling, J. M. Depression and the risk of myocardial infarction and coronary death: A meta-analysis of prospective cohort studies. Medicine 95, e2815. https://doi.org/10.1097/md.0000000000002815 (2016).
Li, M., Zhang, X. W., Hou, W. S. & Tang, Z. Y. Impact of depression on incident stroke: A meta-analysis. Int. J. Cardiol. 180, 103–110. https://doi.org/10.1016/j.ijcard.2014.11.198 (2015).
Daskalopoulou, M. et al. Depression as a risk factor for the initial presentation of twelve cardiac, cerebrovascular, and peripheral arterial diseases: Data linkage study of 1.9 million women and men. PloS one 11, e0153838. https://doi.org/10.1371/journal.pone.0153838 (2016).
Liu, N. et al. Association of major depression with risk of ischemic heart disease in a mega-cohort of Chinese adults: The China Kadoorie biobank study. J. Am. Heart Assoc. https://doi.org/10.1161/jaha.116.004687 (2016).
Zhang, Y. et al. Depression duration and risk of incident cardiovascular disease: A population-based six-year cohort study. J. Affect. Disord. 305, 188–195. https://doi.org/10.1016/j.jad.2022.03.005 (2022).
Dhingra, R. et al. Cardiovascular disease burden is associated with worsened depression symptoms in the U.S. general population. J. Affect. Disord. 323, 866–874. https://doi.org/10.1016/j.jad.2022.12.038 (2023).
Pandi-Perumal, S. R. et al. Clarifying the role of sleep in depression: A narrative review. Psychiatry Res. 291, 113239. https://doi.org/10.1016/j.psychres.2020.113239 (2020).
Petersen, K. S. & Kris-Etherton, P. M. Diet quality assessment and the relationship between diet quality and cardiovascular disease risk. Nutrients https://doi.org/10.3390/nu13124305 (2021).
Opie, R. S. et al. Dietary recommendations for the prevention of depression. Nutr. Neurosci. 20, 161–171. https://doi.org/10.1179/1476830515y.0000000043 (2017).
Rojas-García, A. et al. Healthcare interventions for depression in low socioeconomic status populations: A systematic review and meta-analysis. Clin. Psychol. Rev. 38, 65–78. https://doi.org/10.1016/j.cpr.2015.03.001 (2015).
Schultz, W. M. et al. Socioeconomic status and cardiovascular outcomes: Challenges and interventions. Circulation 137, 2166–2178. https://doi.org/10.1161/circulationaha.117.029652 (2018).
Li, X., Zhou, J., Wang, M., Yang, C. & Sun, G. Cardiovascular disease and depression: A narrative review. Front. Cardiovasc. Med. 10, 1274595. https://doi.org/10.3389/fcvm.2023.1274595 (2023).
Levis, B. et al. Accuracy of the PHQ-2 alone and in combination with the PHQ-9 for screening to detect major depression: Systematic review and meta-analysis. Jama 323, 2290–2300. https://doi.org/10.1001/jama.2020.6504 (2020).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ-9: Validity of a brief depression severity measure. J. General Int. Med. 16, 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x (2001).
Boothroyd, L., Dagnan, D. & Muncer, S. PHQ-9: One factor or two?. Psychiatry Res. 271, 532–534. https://doi.org/10.1016/j.psychres.2018.12.048 (2019).
Costantini, L. et al. Screening for depression in primary care with patient health questionnaire-9 (PHQ-9): A systematic review. J. Affect. Disord. 279, 473–483. https://doi.org/10.1016/j.jad.2020.09.131 (2021).
Bélanger, E., Thomas, K. S., Jones, R. N., Epstein-Lubow, G. & Mor, V. Measurement validity of the patient-health questionnaire-9 in US nursing home residents. Int. J. Geriatr. Psychiatry 34, 700–708. https://doi.org/10.1002/gps.5074 (2019).
Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey, <https://www.cdc.gov/nchs/nhanes/index.htm> (2022)
Centers for Disease Control and Prevention. NCHS Research Ethics Review Board Approval, <https://www.cdc.gov/nchs/nhanes/irba98.htm> (2022).
Centers for Disease Control and Prevention. Medical Conditions, <https://wwwn.cdc.gov/Nchs/Nhanes/2015-2016/MCQ_I.htm> (2017).
Guenther, P. M. et al. Update of the healthy eating index: HEI-2010. J. Acad. Nutr. Diet. 113, 569–580. https://doi.org/10.1016/j.jand.2012.12.016 (2013).
Levey, A. S. et al. A new equation to estimate glomerular filtration rate. Ann. Int. Med. 150, 604–612. https://doi.org/10.7326/0003-4819-150-9-200905050-00006 (2009).
Centers for Disease Control and Prevention. NHANES Survey Methods and Analytic Guidelines, <https://wwwn.cdc.gov/nchs/nhanes/AnalyticGuidelines.aspx> (2022).
Meijer, A. et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: A meta-analysis of 25 years of research. General Hospital Psychiatry 33, 203–216. https://doi.org/10.1016/j.genhosppsych.2011.02.007 (2011).
Krittanawong, C. et al. Association of depression and cardiovascular disease. Am. J. Med. https://doi.org/10.1016/j.amjmed.2023.04.036 (2023).
Wei, J., Lu, Y., Li, K., Goodman, M. & Xu, H. The associations of late-life depression with all-cause and cardiovascular mortality: The NHANES 2005–2014. J. Affect. Disord. 300, 189–194. https://doi.org/10.1016/j.jad.2021.12.104 (2022).
Shen, W., Su, Y., Guo, T., Ding, N. & Chai, X. The relationship between depression based on patient health questionaire-9 and cardiovascular mortality in patients with hypertension. J. Affect. Disord. 345, 78–84. https://doi.org/10.1016/j.jad.2023.10.059 (2024).
Lee, S. Y., Lee, J. P., Lee, J., Park, J. Y. & Kim, E. Y. Association between depressive symptoms and the risk of all-cause and cardiovascular mortality among US adults. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 125, 110755. https://doi.org/10.1016/j.pnpbp.2023.110755 (2023).
Xu, H. et al. The effects of physical activity and sedentary behavior in the associations between cardiovascular diseases and depression: A four-way decomposition. J. Affect. Disord. 275, 194–201. https://doi.org/10.1016/j.jad.2020.07.017 (2020).
Lu, Y. et al. The interaction effect of depressive symptoms and inflammation on the occurrence of cardiovascular diseases. J. Affect. Disord. 350, 946–954. https://doi.org/10.1016/j.jad.2024.01.024 (2024).
Hare, D. L. Depression and cardiovascular disease. Curr. Opin. Lipidol. 32, 167–174. https://doi.org/10.1097/mol.0000000000000749 (2021).
Hare, D. L., Toukhsati, S. R., Johansson, P. & Jaarsma, T. Depression and cardiovascular disease: A clinical review. Eur. Heart J. 35, 1365–1372. https://doi.org/10.1093/eurheartj/eht462 (2014).
de Jonge, P., Mangano, D. & Whooley, M. A. Differential association of cognitive and somatic depressive symptoms with heart rate variability in patients with stable coronary heart disease: Findings from the heart and soul study. Psychosom. Med. 69, 735–739. https://doi.org/10.1097/PSY.0b013e31815743ca (2007).
de Jonge, P. et al. Psychophysiological biomarkers explaining the association between depression and prognosis in coronary artery patients: A critical review of the literature. Neurosci. Biobehav. Rev. 35, 84–90. https://doi.org/10.1016/j.neubiorev.2009.11.025 (2010).
Guimarães, P. O. et al. Sex differences in clinical characteristics, psychosocial factors, and outcomes among patients with stable coronary heart disease: Insights from the STABILITY (stabilization of atherosclerotic plaque by initiation of darapladib therapy) trial. J. Am. Heart Assoc. https://doi.org/10.1161/jaha.117.006695 (2017).
Wassertheil-Smoller, S. et al. Depression and cardiovascular sequelae in postmenopausal women The Women’s Health Initiative (WHI). Arch. Int. Med. 164, 289–298. https://doi.org/10.1001/archinte.164.3.289 (2004).
Smolderen, K. G. et al. Depressive symptoms in younger women and men with acute myocardial infarction: Insights from the VIRGO study. J. Am. Heart Assoc. https://doi.org/10.1161/jaha.114.001424 (2015).
Garcia, M., Mulvagh, S. L., Merz, C. N., Buring, J. E. & Manson, J. E. Cardiovascular disease in women: Clinical perspectives. Circ. Res. 118, 1273–1293. https://doi.org/10.1161/circresaha.116.307547 (2016).
Bucciarelli, V. et al. Depression and cardiovascular disease: The deep blue sea of women’s heart. Trends Cardiovasc. Med. 30, 170–176. https://doi.org/10.1016/j.tcm.2019.05.001 (2020).
Slavich, G. M. & Sacher, J. Stress, sex hormones, inflammation, and major depressive disorder: Extending Social Signal Transduction Theory of Depression to account for sex differences in mood disorders. Psychopharmacology 236, 3063–3079. https://doi.org/10.1007/s00213-019-05326-9 (2019).
Miller, W. L. The hypothalamic-pituitary-adrenal axis: A brief history. Hormone Res. Paediatr. 89, 212–223. https://doi.org/10.1159/000487755 (2018).
Stramba-Badiale, M. et al. Cardiovascular diseases in women: A statement from the policy conference of the European society of cardiology. Eur. Heart J. 27, 994–1005. https://doi.org/10.1093/eurheartj/ehi819 (2006).
Shah, A. J. et al. Sex and age differences in the association of depression with obstructive coronary artery disease and adverse cardiovascular events. J. Am. Heart Assoc. 3, e000741. https://doi.org/10.1161/jaha.113.000741 (2014).
Inoue, K., Beekley, J., Goto, A., Jeon, C. Y. & Ritz, B. R. Depression and cardiovascular disease events among patients with type 2 diabetes: A systematic review and meta-analysis with bias analysis. J. Diabetes Complicat. 34, 107710. https://doi.org/10.1016/j.jdiacomp.2020.107710 (2020).
Moulton, C. D., Pickup, J. C. & Ismail, K. The link between depression and diabetes: The search for shared mechanisms. Lancet. Diabetes Endocrinol. 3, 461–471. https://doi.org/10.1016/s2213-8587(15)00134-5 (2015).
Sullivan, S. & Vaccarino, V. Low socioeconomic status and depression: A double jeopardy for cardiovascular disease?. J. Psychosom. Res. 121, 6–7. https://doi.org/10.1016/j.jpsychores.2019.04.011 (2019).
Acknowledgements
We thank all participants for their supports.
Funding
This work was supported by grants from the National Natural Science Foundation of China (82070408, 82270262), the Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (2021RC014), the Traditional Chinese Medicine Science and Technology Project of Zhejiang Province (2021ZB172).
Author information
Authors and Affiliations
Contributions
W.B.Z. conceived and designed the study. K.M.R. organized these data and drafted the manuscript with the help of P.W., Z.Z.C., W.H.Z., Y.F.C., T.P.Z., and Q.Q.B. Y.M. analyzed the data. K.M.R. and S.J.C. drew the pictures. W.B.Z. detected any errors in the whole process. All authors have read and approved the manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ren, K., Ma, Y., Chen, S. et al. Factors influencing the association between depressive symptoms and cardiovascular disease in US population. Sci Rep 14, 13622 (2024). https://doi.org/10.1038/s41598-024-64274-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-64274-3
- Springer Nature Limited