
Abstract
Atherosclerosis is the primary origin of acute coronary syndrome (ACS) diseases. Previous studies have shown that lncRNA plaque-enriched long noncoding RNA in atherosclerotic macrophage regulation (lncRNA PELATON) is a specific lncRNA in macrophage nuclei. This study aims to identify serum lncRNA PELATON as a biomarker for assessing the incidence and prognosis of ACS. Levels of serum lncRNA PELATON were detected by real-time polymerase chain reaction (RT–PCR) in patients with ACS and healthy individuals. The clinical significance of lncRNA PELATON in patients with ACS was assessed by analyzing receiver operating characteristic and survival curves. The serum levels of lncRNA PELATON in patients with ACS were significantly higher than those in healthy individuals. LncRNA PELATON expression was positively correlated with the expression levels of high sensitivity C-reactive protein (hs-CRP), cardiac troponin T (cTnT) and creatine kinase MB (CK-MB) (p < 0.05). LncRNA PELATON can be used as a potential diagnostic index with an AUC of 0.706 for unstable angina pectoris (UA), 0.782 for acute non-ST-segment elevation myocardial infarction (NSTEMI) and 0.900 for acute ST-segment elevation myocardial infarction (STEMI). The incidence of major cardiovascular events in patients with ACS with high lncRNA PELATON expression was higher than that in those with low lncRNA PELATON expression. However, the mortality between patients in the high and low lncRNA PELATON groups was not significantly different. This study showed that higher levels of lncRNA PELATON were negatively correlated with the prognosis of ACS, revealing the potential of this measurement to serve as an index to assess the incidence and prognosis of ACS.
Similar content being viewed by others

Introduction
China is one of the countries with the heaviest burden of cardiovascular diseases in the world1. In China, cardiovascular diseases are the main cause of death2,3, accounting for 40% of population deaths4. Acute coronary syndrome (ACS) is a group of clinical syndromes, including acute ST-segment elevation myocardial infarction (STEMI), acute non-ST-segment elevation myocardial infarction (NSTEMI), and unstable angina pectoris (UA), based on the rupture or invasion of coronary atherosclerotic plaque5. Coronary angiography is a common and effective method for the diagnosis of coronary atherosclerotic heart disease6. It is a relatively safe and reliable invasive diagnostic technique that has been widely used in clinical practice, and it is considered as the "gold standard" for the diagnosis of coronary heart disease7. However, some patients, such as those who are allergic to iodine or contrast agents, have severe cardiopulmonary insufficiency, have uncontrolled severe arrhythmias, have electrolyte disorders, and have severe hepatic and renal insufficiency, cannot undergo invasive operations. Moreover, complications, such as coronary artery perforation, cardiac tamponade, embolism of vital organs, and cervical and mediastinal hematoma limit its use8. Therefore, it is particularly important to find new and effective early diagnostic indicators for acute coronary syndrome.
LncRNA, which is a class of RNA molecules with sequences that lack an open reading frame, is a functional molecule existing in various species9. It has obvious cell specificity and can fold to form many second-order structures with active energy, and its recording process is regulated by dynamic states10. Based on publicly available lncRNA-related databases, novel lncRNA-disease associations have been predicted by multiple computational prediction models, such as the Improved Random Walk with Restart for LncRNA-Disease Association prediction (IRWRLDA)11 and the KATZ measure for LncRNA-Disease Association prediction (KATZLDA)12. Combining computational prediction models with experimental validation, lncRNAs are believed to be closely associated with a variety of diseases in the human body, such as cancer, heart failure and Alzheimer's disease12,13,14,15. In the state of cardiovascular disease, many lncRNAs are differentially expressed16,17.
LncRNA ANRIL has been identified as an important risk factor for coronary artery disease because of its involvement in the regulation of histone methylation18,19. In addition, lncRNA MI-related transcripts were associated with myocardial infarction (MI)20. Seven candidate lncRNA biomarkers were identified by analyzing the lncRNA expression profiles of 52 ACS patients. In addition, functional analysis of GO and KEGG suggested that these seven lncRNAs may be involved in MI-related biological processes and pathways21. Further studies found that lncRNAs were better than miRNAs or mRNA expression profiles for predicting heart failure in different pathological states, suggesting that lncRNAs have important pathophysiological functions in the cardiovascular system22.
LncRNA PELATON, located on chromosome 20q13.13 and containing 3 exon regions with a total length of 539 nt, is a specific lncRNA in the macrophage nucleus23. Previously, it was also known as RP11-290F20.3, GCRL1 (gastric cancer-related lncRNA 1) and SMIM-25 (small membrane integral protein 25)24. Comparing atherosclerotic carotid arteries from unstable patients to those with stable disease, LncRNA PELATON was identified as being the most significantly upregulated lncRNA among a collection of other transcripts differentially expressed in plaques25. Hung et al. found that it was specifically expressed in monocyte-macrophage cell lines and could not be detected in endothelial cells, smooth muscle cells or fibroblasts23. The lncRNA PELATON can enhance the phagocytic capacity of macrophages and increase the production of reactive oxygen species by increasing CD36 expression on the macrophage membrane23, but the mechanism has not been further explored. As a chronic disease with a large accumulation of macrophage foam cells, atherosclerosis is the primary origin of acute coronary syndrome diseases (ACS). Considering the important role of monocytes, macrophages and foam cells in the formation of atherosclerosis, we speculated that lncRNA PELATON might be an important factor for AS disease.
Thus, the clinical relevance of lncRNA PELATON for the diagnosis and prognosis of ACS was explored through RT–PCR, receiver operating characteristic (ROC) curve and survival analysis to further optimize the individualized treatment of the disease and improve the survival rate of ACS patients.
Results
Clinical characteristics of the study participants
The clinical characteristics of 98 ACS individuals and 37 healthy individuals participating in this study are shown in Table 1.
Levels of lncRNA PELATON were increased in ACS individuals
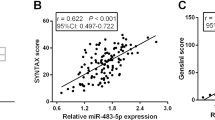
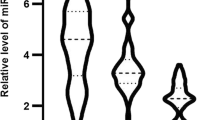
Compared with healthy individuals, the expression of lncRNA PELATON was markedly upregulated in ACS individuals (Fig. 1A). Plaque and surrounding tissue were obtained in some patients who underwent coronary artery surgery. LncRNA expression was higher in plaques than that in adjacent intimal tissues in almost all patients (n = 17) (Fig. 1B). Atherosclerotic plaques (n = 16) and healthy arteries (n = 7) were obtained from patients who underwent carotid endarterectomy. The expression of lncRNA PELATON was increased in atherosclerotic plaques (Fig. 1C). The above experiments indicated that the expression of the lncRNA PELATON was closely related to the occurrence of plaques.

Expression of lncRNA PELATON in ACS. (A) Level of lncRNA PELATON in patients with ACS and healthy individuals. (B) Level of lncRNA PELATON in atherosclerotic plaques and adjacent tissue in the coronary artery. (C) Level of lncRNA PELATON in atherosclerotic plaques and healthy arteries in the carotid artery. * indicates p < 0.05.
Correlation between lncRNA PELATON expression and clinical features of ACS individuals
To investigate whether lncRNA PELATON was related to the clinical parameters, all patients with ACS were categorized into a relatively low (n = 51)/high (n = 47) level serum lncRNA PELATON group, according to the median expression of LncRNA PELATON. Detailed information about the clinical characteristics of the 98 ACS individuals is presented in Table 2, including sex, age, BMI, diabetes mellitus, hypertension, number of diseased vessels and Grace scores. These data suggested that high expression of lncRNA PELATON in serum was significantly related to age (p = 0.005), BMI (p = 0.001), hypertension (p < 0.001), number of diseased vessels (p < 0.001) and Grace scores (p = 0.001), indicating that high serum lncRNA PELATON expression may account for the advanced stage of ACS. However, there was no apparent relationship between increased serum lncRNA PELATON expression and gender or diabetes mellitus.
Correlation of lncRNA PELATON expression in ACS individuals with hs-CRP, CK-MB, cTnT and NTpro-BNP
Pearson’s linear correlation coefficient was used to analyze the correlation of lncRNA PELATON expression in ACS individuals with hs-CRP, CK-MB, cTnT and NTpro-BNP. The results revealed that lncRNA PELATON expression was positively correlated with hs-CRP (p < 0.0001), CK-MB (p < 0.0001) and cTnT (p = 0.0029) (Fig. 2A, B and C), while no significant correlation was observed with NTpro-BNP (p = 0.6928) (Fig. 2d).

Correlation analysis of the expression of lncRNA PELATON with the concentration of myocardial indicators. (A) Correlation between lncRNA PELATON and hs-CRP; (B) Correlation between lncRNA PELATON and CK-MB; C. Correlation between lncRNA PELATON and cTnT; (D) Correlation between lncRNA PELATON and NTpro-BNP.
Diagnostic value of serum lncRNA PELATON for ACS
We evaluated the diagnostic value of serum lncRNA PELATON levels for UA, NSTEMI or STEMI. The ROC curve results showed that the expression of lncRNA PELATON could distinguish UA individuals from healthy individuals, and the AUC was 0.7056. Moreover, the sensitivity was 86.96%, and the specificity was 62.16% (Fig. 3A and Supplementary Table 1). The ROC curve results showed that the expression of lncRNA PELATON could distinguish NSTEMI individuals from healthy individuals, and the AUC was 0.782. Moreover, the sensitivity was 71.79%, and the specificity was 75.68% (Fig. 3B and Supplementary Table 1). The ROC curve results showed that the expression of lncRNA PELATON could distinguish STEMI individuals from healthy individuals, and the AUC was 0.900. Moreover, the sensitivity was 88.90%, and the specificity was 81.10% (Fig. 3C and Supplementary Table 1).

Receiver operating characteristic curve for evaluating UA, NSTEMI or STEMI by lncRNA PELATON. (A) ROC curve for evaluating UA; (B) ROC curve for evaluating NSTEMI; (C) ROC curve for evaluating STEMI.
Combination of lncRNA PELATON and CK-MB as diagnostic biomarkers of NSTEMI or STEMI
We evaluated the diagnostic value of serum lncRNA PELATON combined with CK-MB for NSTEMI or STEMI. A ROC curve (Fig. 4A) showed that the lncRNA PELATON combined with CK-MB could distinguish NSTEMI individuals from healthy individuals, and the AUC was 0.966. Moreover, the sensitivity was 84.62%, and the specificity was 97.3% (Supplementary Table 2). The lncRNA PELATON combined with CK-MB could distinguish STEMI individuals from healthy individuals, and the AUC was 0.973 (Fig. 4B). Moreover, the sensitivity was 97.44%, and the specificity was 89.19% (Supplementary Table 2).

Evaluating ACS by lncRNA PELATON and CK-MB. (A) ROC curve for evaluating NSTEMI; (B) ROC curve for evaluating STEMI.
Survival analysis of ACS individuals
Serum lncRNA PELATON levels were remeasured in 68 patients at 1 year after admission (1 patient died within 1 year, and 29 patients were diagnosed less than a year after their last diagnosis). The results showed that the level of serum lncRNA PELATON after treatment in patients was significantly decreased (Fig. 5A). Next, we determined whether lncRNA PELATON expression correlates with future adverse cardiovascular events (MCE). The major cardiovascular events included cardiovascular death, myocardial infarction and stroke. We found that high lncRNA PELATON expression levels in serum were associated with a higher incidence of MCE (p < 0.05) (Fig. 5B). However, the probability of survival between high and low lncRNA PELATON had no significant difference (p = 0.3357) (Fig. 5C).

Survival analysis of ACS individuals. (A) The expression of lncRNA PELATON in patients with treatment. (B) The incidence of MCE in ACS patients between high and low lncRNA PELATON expression. (C) The probability of survival between high and low lncRNA PELATON.
Discussion
The pathological process of AS begins when circulating low-density lipoproteins (LDL) stimulate endothelial cell damage, causing endothelial cell dysfunction, activating endothelial secretory cell adhesion factors and chemokines that promote leukocyte recruitment, and inducing inflammatory cell infiltration26. Increased vascular permeability and infiltration of monocytes that differentiate into macrophages promote the formation of foam cells27. Simultaneously, local hypoxic stimulation of the vascular intima induces angiogenesis, which extends to the vascular intima and promotes the development of AS28. LncRNAs can act on pathological processes at different stages, such as endothelial dysfunction, angiogenesis, and immune response, to play an important role in the process of AS 29,30. Based on the important role of lncRNAs in gene transcription, we believe that there are still many unknown lncRNAs waiting to be discovered. However, it is inefficient to find the association between new lncRNAs and diseases through traditional experimental methods. Fortunately, after various biological experiments and RNA sequencing, a large amount of biological data on the association between noncoding RNAs (lncRNAs, circRNAs and miRNAs) and diseases have been accumulated. Based on RNA sequencing, RNA expression profiling, disease-directed acyclic graphs, RNA-gene interactions, disease-gene associations and RNA-disease associations, Chen et al. developed several effective computer prediction models to clarify the link between RNA and disease and further verified the validity of the above models through biological methods15,31,32. Undoubtedly, this is one of the effective ways to elucidate the important role of noncoding RNA in the future.
There is one point worth discussing when reviewing the literature. From the literature, it has been emphasized that lncRNA PELATON is specifically expressed in monocyte-macrophage cell lines, and its expression in multiple cell lines (monocytes, macrophages, endothelial cells, fibroblasts, smooth muscle cells) has also been tested in the article23. Our experiment also confirmed its specific expression. However, known as RP11-290F20.3, GCRL1 (gastric cancer-related lncRNA 1)24 is still expressed in gastric cancer tissues, gastric cancer cell lines and nude mice. However, when we conducted bioinformatics to query the miRNA related to lncRNA PELATON, it was found that it was only expressed in human species and could not be queried in mice. Although the specificity of its cell and tissue expression does not affect its important role in ACS, this problem is still worthy of further discussion.
The incidence of important cardiovascular events is a factor affecting the prognosis of patients. Our study found that the incidence of important cardiovascular events in ACS patients with high expression of lncRNA PELATON was significantly higher than that of ACS patients with low expression of lncRNA PELATON. However, during the follow-up period, we did not observe a difference in mortality between the two groups of patients. We speculate that this may be related to the lack of follow-up time, which is different from the common 1-year, 5-year or even 10-year survival rate of cancer patients. Generally, ACS patients have a long survival time with right diagnosis and proper treatment. However, some patients have poor medication compliance in clinical practice. For follow-up experiments, we need to strengthen patient compliance education to eliminate it. At the same time, we hope to extend the follow-up time to observe the impact of lncRNA PELATON on long-term mortality and major cardiovascular events in patients with ACS.
Previous studies have shown that the lncRNA PELATON is highly expressed in AS plaque23. The lncRNA PELATON can enhance the phagocytic capacity of macrophages and increase the production of reactive oxygen species by increasing CD36 expression on the macrophage membrane23. Our study found that lncRNA PELATON was significantly increased in the serum and plaques of ACS patients, and it was aggravated with the degree of blood vessel blockage. Taking into account the pathological basis of ACS disease, lncRNA PELATON has a significant effect of promoting plaque formation, and the content of lncRNA PELATON will increase significantly when macrophages are formed into foam cells. Therefore, we speculate that lncRNA PELATON and plaque block formation promote each other. Foam cell formation and foam cell mobility are important processes of AS formation when plaques are retained33. LncRNA PELATON can upregulate the expression of CD36 to promote foam cell formation. The significance of this study lies in the discussion of the clinical significance of lncRNA PELATON, including its diagnostic significance for ACS disease and its influence on subsequent ACE and death of ACS disease. This method could also be implemented to reveal the function of other LncRNAs in ACS. However, the lncRNA PELATON was chosen for the experiments based on the following two points: lncRNA PELATON is specifically expressed in the monocyte-macrophage cell line, which are two important cells involved in atherosclerosis; the expression level of lncRNA PELATON is gradually increased during monocyte-macrophage-foam cell transformation, indicating that it may be closely related to the progression of atherosclerosis. We believe that the clinical importance of lncRNAs should be paid more attention first. However, the specific mechanism of lncRNA PELATON affecting AS formation was not further discussed in this paper. Compared with the current traditional experimental methods, computer models based on bioinformatics databases may be more efficient and effective in predicting lncRNA action networks (such as lncRNA-miRNA interactions). For example, Zhang et al. explored and predicted potential interactions between lncRNAs and miRNAs based on a semisupervised interaction group network, demonstrating superiority and good generalization34. Additionally, a network distance analysis model for lncRNA-miRNA association prediction (NDALMA) obtained satisfactory results in fivefold cross-validation. All this work will be used in combination with cell and animal experiments in our next study35.
In conclusion, our experiments demonstrated that higher levels of lncRNA PELATON were negatively correlated with the prognosis of ACS, which could be used as a potential index to assess the incidence and prognosis of ACS.
Materials and methods
Subjects
The ACS individuals diagnosed at the Sun Yat-sen University affiliated Zhongshan Hospital from July 2018 to September 2021 were enrolled retrospectively. This was in line with the following inclusion criteria: (1) patients diagnosed with ACS for the first time and (2) patients satisfying the diagnostic criteria of ACS in accordance with the Diagnostic and Therapeutic Criteria of the Cardiovascular system and diagnosed by coronary angiography. Exclusion criteria: (1) patients with hepatic and renal insufficiency; (2) patients allergic to iodine or contrast agents; (3) patients with severe cardiopulmonary insufficiency; (4) patients with uncontrolled severe arrhythmias; (5) patients with severe electrolyte disorder; and (6) patients with severe infection. Serum samples and laboratory results from 37 healthy patients during the same period were collected. All patients agreed to participate in the experiment and signed an informed consent form. These study results had no influence on the subsequent management of patients. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Board of the Sun Yat-sen University affiliated Zhongshan Hospital.
Clinical data collection and follow-up
We obtained the clinical characteristics and laboratory test results of all enrolled subjects through our hospital’s computerized test system (Nanfang Huiqiao). Patients were followed from July 2018 to September 2021. The follow-up information of patients was obtained through systematic case data in our hospital and telephone conversations.
Real-Time Polymerase Chain Reaction (RT–PCR)
Total RNA was isolated from human tissue, serum and cell lines using the miRNEasy kit (Qiagen). It was reverse transcribed using the TaqMan microRNA reverse Transcription Kit (Thermo Fisher, Waltham, MA, USA). Next, RT–PCR was performed using 2 × SYBR Green PCR Master Mix. Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) was the internal reference. LncRNA PELATON: Forward: 5’-CCTTCCTTCTGCCTCCACTG-3’ and Reverse: 5’-CCTTCCT TCTGCCTCCACTG-3’, and GAPDH: Forward: 5’-GCTCTCTGCTCCTCCTGTTC-3’ and Reverse: 5’-ACGACCAAATCCGTTGACTC-3’.
Statistical methods
GraphPad 8.0 and SPSS 26.0 software were used for statistical analysis of the data. The chi-square test was used for nonparametric data, and the mean ± standard deviation (SD) was used for descriptive continuous variables. The independent samples or paired samples t test was used for data analysis if the data followed a normal distribution. If the data did not obey the normal distribution, the Mann–Whitney U test was used for data analysis. The Kaplan–Meier method was used for the analysis of survival curves, and the log-rank method was used for inspection. The flowchart of the whole analysis process is shown in Supplementary Fig. 1. A p value < 0.05 indicated that the difference was statistically significant.
Data availability
All data generated or analyzed during this study are included in this published article (and its Supplementary Information files).
References
Disease, G. B. D., Injury, I. & Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 390, 1211–1259. https://doi.org/10.1016/S0140-6736(17)32154-2 (2017).
Zhou, M. et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet 387, 251–272. https://doi.org/10.1016/S0140-6736(15)00551-6 (2016).
Yang, G. et al. Rapid health transition in China, 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet 381, 1987–2015. https://doi.org/10.1016/S0140-6736(13)61097-1 (2013).
Zhao, D., Liu, J., Wang, M., Zhang, X. & Zhou, M. Epidemiology of cardiovascular disease in China: Current features and implications. Nat. Rev. Cardiol. 16, 203–212. https://doi.org/10.1038/s41569-018-0119-4 (2019).
Guttman, M. et al. Chromatin signature reveals over a thousand highly conserved large non-coding RNAs in mammals. Nature 458, 223–227. https://doi.org/10.1038/nature07672 (2009).
Lun, Z. et al. Association of early and late contrast-associated acute kidney injury and long-term mortality in patients undergoing coronary angiography. J. Interv. Cardiol. 2021, 6641887. https://doi.org/10.1155/2021/6641887 (2021).
Scanlon, P. J. et al. ACC/AHA guidelines for coronary angiography. A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Coronary Angiography). Developed in collaboration with the Society for Cardiac Angiography and Interventions. J. Am. Coll. Cardiol. 33, 1756–1824, https://doi.org/10.1016/s0735-1097(99)00126-6 (1999).
Mhanna, M. et al. Outcomes of distal versus conventional transradial access for coronary angiography and intervention: An updated systematic review and meta-analysis. Int. J. Cardiol. 344, 47–53. https://doi.org/10.1016/j.ijcard.2021.10.003 (2021).
Sharma, H. & Carninci, P. The Secret Life of lncRNAs: Conserved, yet Not Conserved. Cell 181, 512–514. https://doi.org/10.1016/j.cell.2020.04.012 (2020).
Senmatsu, S. & Hirota, K. Roles of lncRNA transcription as a novel regulator of chromosomal function. Genes Genet. Syst. 95, 213–223. https://doi.org/10.1266/ggs.20-00024 (2021).
Chen, X., You, Z. H., Yan, G. Y. & Gong, D. W. IRWRLDA: Improved random walk with restart for lncRNA-disease association prediction. Oncotarget 7, 57919–57931. https://doi.org/10.18632/oncotarget.11141 (2016).
Chen, X. KATZLDA: KATZ measure for the lncRNA-disease association prediction. Sci. Rep. 5, 16840. https://doi.org/10.1038/srep16840 (2015).
Chen, X. et al. Computational models for lncRNA function prediction and functional similarity calculation. Brief Funct. Genomics 18, 58–82. https://doi.org/10.1093/bfgp/ely031 (2019).
Chen, X., Yan, C. C., Zhang, X. & You, Z. H. Long non-coding RNAs and complex diseases: from experimental results to computational models. Brief Bioinform. 18, 558–576. https://doi.org/10.1093/bib/bbw060 (2017).
Chen, X. & Yan, G. Y. Novel human lncRNA-disease association inference based on lncRNA expression profiles. Bioinformatics 29, 2617–2624. https://doi.org/10.1093/bioinformatics/btt426 (2013).
Ou, M., Li, X., Zhao, S., Cui, S. & Tu, J. Long non-coding RNA CDKN2B-AS1 contributes to atherosclerotic plaque formation by forming RNA-DNA triplex in the CDKN2B promoter. EBioMedicine 55, 102694. https://doi.org/10.1016/j.ebiom.2020.102694 (2020).
Jiang, X., Liu, Z. & Qi, X. LncRNA BANCR induced vascular smooth muscle cell proliferation by downregulating miR-34c methylation in atherosclerosis. J. Thromb. Thrombol. 51, 924–932. https://doi.org/10.1007/s11239-020-02314-1 (2021).
Broadbent, H. M. et al. Susceptibility to coronary artery disease and diabetes is encoded by distinct, tightly linked SNPs in the ANRIL locus on chromosome 9p. Hum. Mol. Genet. 17, 806–814. https://doi.org/10.1093/hmg/ddm352 (2008).
Yap, K. L. et al. Molecular interplay of the noncoding RNA ANRIL and methylated histone H3 lysine 27 by polycomb CBX7 in transcriptional silencing of INK4a. Mol. Cell. 38, 662–674. https://doi.org/10.1016/j.molcel.2010.03.021 (2010).
Ishii, N. et al. Identification of a novel non-coding RNA, MIAT, that confers risk of myocardial infarction. J. Hum. Genet. 51, 1087–1099. https://doi.org/10.1007/s10038-006-0070-9 (2006).
Lu, Y., Meng, X., Wang, L. & Wang, X. Analysis of long non-coding RNA expression profiles identifies functional lncRNAs associated with the progression of acute coronary syndromes. Exp. Ther. Med. 15, 1376–1384. https://doi.org/10.3892/etm.2017.5573 (2018).
Zhang, C., Han, B., Xu, T. & Li, D. The biological function and potential mechanism of long non-coding RNAs in cardiovascular disease. J. Cell. Mol Med. 24, 12900–12909. https://doi.org/10.1111/jcmm.15968 (2020).
Hung, J. et al. Novel plaque enriched long noncoding RNA in atherosclerotic macrophage regulation (PELATON). Arterioscler. Thromb. Vasc. Biol. 40, 697–713. https://doi.org/10.1161/ATVBAHA.119.313430 (2020).
Lin, Z. et al. Long noncoding RNA gastric cancer-related lncRNA1 mediates gastric malignancy through miRNA-885-3p and cyclin-dependent kinase 4. Cell Death Dis. 9, 607. https://doi.org/10.1038/s41419-018-0643-5 (2018).
Rayner, K. J. Leading the long noncoding RNA Pack: PELATON in human atherosclerosis. Arterioscler. Thromb. Vasc. Biol 40, 495–497. https://doi.org/10.1161/ATVBAHA.119.313762 (2020).
Tabas, I., Garcia-Cardena, G. & Owens, G. K. Recent insights into the cellular biology of atherosclerosis. J. Cell Biol. 209, 13–22. https://doi.org/10.1083/jcb.201412052 (2015).
Chen, L. et al. Lysophosphatidic acid directly induces macrophage-derived foam cell formation by blocking the expression of SRBI. Biochem. Biophys. Res. Commun. 491, 587–594. https://doi.org/10.1016/j.bbrc.2017.07.159 (2017).
Aryal, B. & Suarez, Y. Non-coding RNA regulation of endothelial and macrophage functions during atherosclerosis. Vascul. Pharmacol. 114, 64–75. https://doi.org/10.1016/j.vph.2018.03.001 (2019).
Hu, N., Zeng, X., Tang, F. & Xiong, S. Exosomal long non-coding RNA LIPCAR derived from oxLDL-treated THP-1 cells regulates the proliferation of human umbilical vein endothelial cells and human vascular smooth muscle cells. Biochem. Biophys. Res. Commun. 575, 65–72. https://doi.org/10.1016/j.bbrc.2021.08.053 (2021).
Wang, L., Xia, J. W., Ke, Z. P. & Zhang, B. H. Blockade of NEAT1 represses inflammation response and lipid uptake via modulating miR-342-3p in human macrophages THP-1 cells. J. Cell Physiol. 234, 5319–5326. https://doi.org/10.1002/jcp.27340 (2019).
Chen, X., Wang, L., Qu, J., Guan, N. N. & Li, J. Q. Predicting miRNA-disease association based on inductive matrix completion. Bioinformatics 34, 4256–4265. https://doi.org/10.1093/bioinformatics/bty503 (2018).
Wang, C. C., Han, C. D., Zhao, Q. & Chen, X. Circular RNAs and complex diseases: from experimental results to computational models. Brief Bioinform., https://doi.org/10.1093/bib/bbab286 (2021).
Chen, L. et al. Lysophosphatidic acid decreased macrophage foam cell migration correlated with downregulation of fucosyltransferase 8 via HNF1alpha. Atherosclerosis 290, 19–30. https://doi.org/10.1016/j.atherosclerosis.2019.09.001 (2019).
Zhang, L., Liu, T., Chen, H., Zhao, Q. & Liu, H. Predicting lncRNA-miRNA interactions based on interactome network and graphlet interaction. Genomics 113, 874–880. https://doi.org/10.1016/j.ygeno.2021.02.002 (2021).
Zhang, L., Yang, P., Feng, H., Zhao, Q. & Liu, H. Using network distance analysis to predict lncRNA-miRNA interactions. Interdiscip. Sci. 13, 535–545. https://doi.org/10.1007/s12539-021-00458-z (2021).
Acknowledgements
We would like to thank all the patients and healthy individuals who participated in this study.
Funding
This study was supported by the Zhongshan Social Welfare and Foundation Special Project (Grant number: K2020B3004).
Author information
Authors and Affiliations
Contributions
L. C and Y. H designed the research; Y. H collected the samples. L. C performed the tests and statistics. L. C and Y. H wrote and edited the paper. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, L., Huang, Y. High expression of lncRNA PELATON serves as a risk factor for the incidence and prognosis of acute coronary syndrome. Sci Rep 12, 8030 (2022). https://doi.org/10.1038/s41598-022-11260-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-11260-2
- Springer Nature Limited
This article is cited by
-
Long non-coding RNA SNHG7 serves as a diagnostic biomarker for acute coronary syndrome and its predictive value for the clinical outcome after percutaneous coronary intervention
Journal of Cardiothoracic Surgery (2024)
-
HAND2-AS1 associates with outcomes of acute coronary syndrome and regulates cell viability of vascular endothelial cells
Irish Journal of Medical Science (1971 -) (2024)