
Abstract
Carbapenemase-producing bacteria are a growing issue worldwide. Most phenotypic detection methods are culture-based, requiring long incubation times. We present a phenotypic screening panel for detection of carbapenem non-susceptibility and differentiation of carbapenemase classes and AmpC, the MALDI-TOF MS-based direct-on-target microdroplet growth assay (DOT-MGA). It was validated on 7 reference strains and 20 challenge Enterobacterales isolates. Broth microdilution (BMD) and combination disk test (CDT) were also performed, as well as PCR as reference method. The panel based on the synergy between meropenem and carbapenemase inhibitors, determined by incubating these substances with bacterial suspension on a MALDI-TOF MS target and subsequently assessing bacterial growth on the target’s spots by MS. After 4 hours of incubation, DOT-MGA correctly identified KPC, MBL and OXA (100% agreement with PCR). Detection of AmpC coincided with BMD and CDT but agreement with PCR was low, not ruling out false negative PCR results. DOT-MGA delivered more accurate results than BMD and CDT in a significantly shorter time, allowing for detection of carbapenem non-susceptibility, MIC determination and carbapenemase differentiation in one step.
Similar content being viewed by others


Introduction
The time to availability of microbiological results plays a critical role in the medical decision-making process as it has a direct impact on the choice of antimicrobial therapy. Advanced antimicrobial susceptibility testing (AST) methods may help to accelerate the targeted antimicrobial therapy1. However, the implications of a rapid and accurate laboratory diagnosis go beyond the clinical aspects: the consumption of antimicrobial substances as well as the rate of the development of bacterial resistance have shown to be directly affected by the information provided by the microbiology laboratory2. An association has also been observed between aspects concerning hospitalisation (amount of resources invested, total length of stay) and the accuracy of the implemented therapeutic strategies, which in turn depends on the turnaround times of the diagnostic tools employed3,4,5,6. Most importantly, a prompt detection of resistance patterns leads to better clinical outcomes3,7,8.
Despite advances in phenotypic AST methodology, the time required for bacteria to replicate remained a natural obstacle, as reaching the stationary growth phase is required for the performance and interpretation of most available antibiotic susceptibility tests. This translates into incubation times exceeding 10 hours for culture-based diagnostic methods, a time lapse during which therapeutic decisions are taken empirically. Thus, developing new diagnostic methods that tackle the delay posed by the usual incubation times should be prioritised, especially in an era of increasing antimicrobial resistance1.
As resistance against antibiotics raises concern worldwide, carbapenem resistance stands out as one of the most preoccupying edges of this problem, seeing as how carbapenems constitute the most reliable treatment option for infections caused by multidrug-resistant (including ESBL-producing) Gram-negative bacteria, particularly Enterobacteriaceae and other Enterobacterales9. First described in the early 1990s10, resistance against carbapenems has reached a high incidence in various regions9,11,12.
Several rapid molecular, colourimetric and mass spectrometry-based methods have been developed and represent an alternative to the growth-based techniques, offering results in a shorter time. However, various drawbacks hampered their widespread use in the routine laboratory. Concerning PCR-based approaches, a limited number of targeted genes and the inability to detect emerging ones represent the main disadvantages of these genotypic techniques13. Colourimetric methods provide no information on the specific carbapenemase type present13 and have been reported to display a low sensitivity for the detection OXA-48 producers14,15.
The applicability of matrix-assisted laser desorption ionisation time-of-flight mass spectrometry (MALDI-TOF MS) for susceptibility testing has been demonstrated in recent years, based on: (i) monitoring the mass shifts that derived from antibiotic hydrolysis16,17,18; (ii) detecting the incorporation of isotopically labelled aminoacids by resistant bacteria growing in presence of carbapenems19; (iii) analysing the biomass present after cultivating bacteria in presence or absence of carbapenems20; or (iv) the recently described direct-on-target microdroplet growth assay (DOT-MGA)21,22,23.
Here, we propose a rapid all-in-one MALDI-TOF MS-supported screening panel based on the DOT-MGA. The panel allows to detect carbapenem non-susceptibility as well as to make a differential identification of carbapenemase classes. A validation of the method was carried out with 20 carbapenem-non-susceptible Enterobacterales strains.
Results
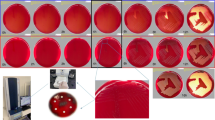
The DOT-MGA screening panel was developed as a one-step method for detection of carbapenem non-susceptibility, AmpC production and carbapenemase class differentiation. It was performed on a 96-well MALDI-TOF target (Bruker Daltonik, Bremen, Germany), following the layout depicted in Fig. 1. A total of 6 µl containing a suspension of the tested strain and meropenem in serial two-fold dilutions was pipetted onto each of the target’s spots, with each row containing antibiotic concentrations ranging from 0.03 to 64 µg/ml. In order to differentiate between carbapenemase classes, specific inhibitors were added in several rows. After incubating the target and removing the broth, the meropenem minimum inhibitory concentration (MIC) of each row could be determined by assessing the bacterial growth on the spots through a mass spectrometric analysis. High temocillin resistance, common in OXA-producing isolates, was determined by this same principle in the panel’s last row (concentrations 0.25 to 512 µg/ml). The meropenem concentration present in the first spot (in ascending order) of a given row that showed no bacterial growth was considered the MIC. A significant decrease of the meropenem MIC (8-fold or more) in rows with added carbapenemase inhibitors was interpreted as an indicator of a synergistic effect, allowing for the differential identification of carbapenemase classes.

Layout of the DOT-MGA screening panel. The mass spectrometric assessment of bacterial growth on each spot allows the MIC determination for each row. Significant MIC decrease (8-fold or more) in zones 2–5 in relation to zone 1 indicates presence of a certain carbapenemase. Temocillin MIC > 128 µg/ml (last row) is compatible with OXA production MEM: meropenem; PBA: phenylboronic acid; APBA: aminophenylboronic acid; CLX: cloxacillin; EDTA: ethylendiamintetraacetic acid; AVI: avibactam; TEM: temocillin.
The validation of the method was performed on seven reference strains recommended by EUCAST for detection of carbapenemases24 (Table 1), as well as on 20 meropenem non-susceptible Enterobacterales strains isolated from clinical samples (Table S1). The method was carried out with two different incubation times, namely 3 and 4 hours, observing a significantly higher accuracy at the second time point. The results of DOT-MGA, as well as of BMD and CDT, were evaluated considering the PCR as an imperfect standard (accepted method of comparison which may be imprecise to some extent)25, calculating the positive percent agreement (PPA) and negative percent agreement (NPA) for each method (Table 2):
DOT-MGA accurately detected carbapenem non-susceptibility
After 4 hours of incubation, DOT-MGA was able to detect carbapenemase activity in the 6 carbapenemase-producing reference strains as well as in 10 of 10 isolates with carbapenemase production confirmed by PCR. PPA and NPA values of 100% were reached, as opposed to those shown by BMD (80%/80%) and CDT (90%/10%).
DOT-MGA correctly identified KPC, MBL and OXA carbapenemases
The foreknown mechanisms of resistance present in all control strains (KPC; MBL; OXA and AmpC) were correctly identified by DOT-MGA after 4 hours of incubation (Table 1).
The identification of carbapenemase classes among the clinical isolates tested was also most accurate after 4 hours of on-target incubation. Aside from one KPC-positive control strain, KPC production was not detected by DOT-MGA in clinical isolates, in accordance with the PCR results (Table S1); this translated into an NPA of 100% (BMD: 90%; CDT: 65%). DOT-MGA displayed a PPA of 100% for the detection of MBL, in comparison to 75% reached by BMD and CDT. All three methods correctly identified MBL-negative isolates with an NPA of 100%. OXA production was detected by DOT-MGA with PPA and NPA values of 100%. BDM and CDT yielded several false positive results (2 and 6, respectively), leading to a significantly lower NPA. Strains were also analysed for AmpC production as possible additional mechanism of resistance. Here, all three methods performed similarly, identifying two (DOT-MGA) to three (BMD, CDT) isolates as AmpC-positive while they were negative by PCR.
Discussion
Carbapenem resistance among Gram-negative microorganisms is a global threat with increasing significance for human and veterinary public-health and with growing environmental concerns, e.g. as hospital wastewater contaminants26,27,28. An innovative phenotypic method is presented that offers concrete information about the carbapenem non-susceptibility Enterobacterales isolates. The DOT-MGA screening panel has been designed in an easy-to-perform format that allows testing for several mechanisms of carbapenem non-susceptibility in a single step.
Our approach detected type-specific carbapenemase production with a performance equivalent to that of the PCR and a higher accuracy than that of the other phenotypic methods evaluated, identifying specific carbapenemase types.
KPC production was successfully detected in one control strain, with no false positive results among the clinical strains, all of which tested negative for KPC by PCR. MBL was successfully detected in all 4 clinical isolates also identified by PCR, despite the additional production of AmpC in two of them. With high PPA and NPA values of 100%, the test performed satisfactorily in terms of OXA detection, a worldwide spread carbapenemase class of special relevance in Germany12,29 which often poses a diagnostic challenge30,31. The combination of two detection principles, synergy of meropenem with avibactam and high-level temocillin resistance, allowed overcoming the possible masking effect of MBL in an isolate producing both carbapenemases.
In addition to the identification of carbapenemases, the detection of AmpC production was included in the screening panel as a complementary feature, due to the decreased susceptibility to carbapenems that these enzymes may cause32,33,34. DOT-MGA coincided with the PCR in one AmpC-positive isolate. However, two further isolates negative for AmpC in the PCR showed positive DOT-MGA results, as they proved susceptible to the combination meropenem/cloxacillin. In both cases, BMD and CDT also delivered AmpC-positive results. An explanation for this, besides possible false positive results, is the presence of AmpC genes in the isolates that were not detected by the PCR microarray.
The proposed assay offers a one-step method that allows for (i) determination of carbapenem non-susceptibility; (ii) MIC quantification; and (iii) specific carbapenemase detection. Being a phenotypic approach, it allows the detection of unknown or uncommon carbapenemases encoded by uncommon or emerging genes not identified by routine DNA-based methods. While designed as proof-of-principle study delivering primary data on a new technique, a limitation is the small number of isolates tested and the low carbapenemase diversity. This is in part a result of the strictly consecutive collection of clinical strains at the routine laboratory, thus reflecting the German epidemiological situation12. Further evaluation on clinical isolates producing diverse carbapenemases, especially KPC, would be useful in order to complement the validation process carried out in the present study. Also, customised assay equipment and adapted analysis software may further enhance the standardisation, manageability and performance of this approach.
Overall, the screening panel identified the main carbapenemase classes with a higher accuracy than other phenotypic methods routinely used, yielding results comparable to those of the genotypic reference method (PCR). This assay provides detailed and reliable type-specific carbapenemase detection after 4 hours, constituting a valuable tool for the acceleration of microbiological diagnostic procedures. The method can be easily implemented in laboratories working with MALDI-TOF MS, since it does not require additional instrumentation and the testing procedure is similar to that of the regular MALDI-TOF MS identification. In future phases of development, alternative preparation of the necessary stock solutions (i.e. pre-coated targets) could facilitate the automation of the method, further reducing the turnaround time. Being performed as a routine technique, the DOT-MGA screening panel would expedite the decision-making process in the healthcare setting, contributing to a more appropriate approach to carbapenem-resistant microorganisms at both the clinical and epidemiological level. This would translate into better clinical outcomes, a more rational use of carbapenems and faster implementation of infection control measures.
Methods
Bacterial strains
For the development of the panel, preliminary experiments were performed on 6 carbapenem-resistant strains recommended by EUCAST for the detection of carbapenemase production24 and one non-carbapenemase-producing strain used as a negative control (Table 1).
In a second phase, the panel was challenged with a total of 20 Enterobacterales strains (Table S1) consecutively isolated from clinical samples processed at the Institute of Medical Microbiology of the University Hospital Münster, Germany. These isolates were routinely identified by MALDI-TOF MS and displayed resistance against meropenem35 as determined by the Vitek 2® card AST-N214 (bioMérieux, Marcy l’Etoile, France).
Bacterial suspensions were prepared and adjusted to a density of 0.5 McFarland employing a nephelometer (Densimat, bioMérieux, Marcy l’Etoile, France). Subsequently, a dilution 1:100 was made with cation-adjusted Mueller-Hinton broth (CA-MHB).
Antimicrobial substances
Given its high sensitivity and specificity36,37, meropenem (TCI Deutschland GmbH, Eschborn, Germany) was used as indicator substance to screen for carbapenem non-susceptibility. The detection of each carbapenemase class relied on the synergy of meropenem with the following specific carbapenemase inhibitors: phenylboronic acid (PBA, TCI), aminophenylboronic acid (APBA, TCI), cloxacillin (CLX, TCI), dipicolinic acid (DPA, TCI), ethylenediaminetetraacetic acid (EDTA, TCI) and avibactam (Advanced ChemBlocks Inc., Burlingame, CA, USA). Temocillin (Eumedica Pharmaceuticals, Basel, Switzerland) was used as an indicator for OXA production. Stock solutions of each substance were prepared following the guidelines of the Clinical and Laboratory Standards Institute (CLSI)38 using deionised distilled water. Due to the physicochemical properties of PBA and APBA, a dilution in dimethyl sulfoxide (AppliChem, Darmstadt, Germany) and deionised distilled water (mixed in a 1:1 ratio) was necessary. The quality of the meropenem stock solution was tested according to the specifications of CLSI38 and EUCAST39, verifying the MIC of E. coli ATCC 25922. Seeing as how no quality standards have been established for the rest of the substances employed, the working concentrations were standardised in triplicate.
Screening panel
The panel was designed to comprise several zones distributed over a 96-spot format as shown in Fig. 1. Zone 1, a two-fold dilution series of meropenem constituted the primary carbapenem non-susceptibility screening. Zones 2, 3 and 4 contained meropenem in combination with specific inhibitors, allowing for the detection of three carbapenemase classes: KPC (PBA, APBA), AmpC (CLX), MBL (EDTA, DPA). Zone 5 included two different methods of OXA detection based on the synergy between meropenem and avibactam40, as well as on the high-level temocillin resistance (>128 µg/ml) frequently observed in OXA-producing strains24,41. The appropriate concentrations of the different inhibitors were defined in internal standardisation tests partly based on previous reports42,43.
DOT-MGA was performed as previously described23. Microdroplets (total volume 6 µl) containing 3 µl of bacterial suspension (final inoculum approximately 5 × 105 CFU/ml) and 3 µl of the different antimicrobial solutions (meropenem, meropenem/inhibitor and temocillin) were distributed on the spots of an MBT Biotarget 96 (Bruker Daltonik, Bremen, Germany). A second target was used for the sterility and growth controls.
Targets were incubated for 3 or 4 hours at 35 ± 1 °C. In order to avoid the evaporation of the microdroplets, targets were kept in plastic transport boxes (Bruker Daltonik) containing water during the incubation. Afterwards, broth was carefully removed from the spots employing filter paper (size 37 × 100 mm, GE Healthcare GmbH, Freiburg, Germany), avoiding cross contamination of the microdroplets. The spots were then overlaid with 1 µl of α-cyano-4-hydroxycinnamic acid matrix including internal standard (MBT MASTeR prototype kit, Bruker Daltonik) and MALDI-TOF MS spectra were acquired on a microflex smart instrument (Bruker Daltonik). The assay was performed in triplicate. The median of the values obtained in each measurement was used for further interpretation.
The final carbapenemase detection was based on the comparison and combined analysis of the minimum inhibitory concentration (MIC) detected for each substance or combination of substances tested on the panel.
By processing the spectra obtained from the MALDI-TOF MS readings with the MALDI Biotyper Software 3.1 (Bruker Daltonik), bacterial growth was identified on those spots where the tested strain was not inhibited by the antimicrobial substances used. In contrast, spots on which antibiotics achieved an inhibitory effect (i.e. because of higher concentrations or synergistic combination), no growth was identified. Based on the degree of growth detection, a score was automatically assigned to each spot, with a score ≥2.0 being considered indicative of bacterial growth. Following the principle of the classic broth microdilution method (BMD), the MIC of the antibiotics in presence or absence of inhibitors was defined as the lowest concentration at which no bacterial growth could be detected by MALDI-TOF MS, corresponding to a detection score <2.0.
The meropenem MIC in zone 1 (Fig. 1) was interpreted according to the EUCAST breakpoints and screening cut-off values defined in the guidelines for detection of resistance mechanisms24,35 in order to classify isolates in susceptible (MIC ≤ 0.125), putative carbapenemase-producers (0.125 > MIC ≤ 2), intermediate (2 > MIC ≤ 8) or resistant (MIC > 8) towards meropenem.
The identification of specific carbapenemase classes was based on the synergy between meropenem and the respective carbapenemase inhibitor, indicated by an 8-fold decrease (or more) of the initial meropenem MIC. The carbapenemase identification employing two inhibitors (KPC, MBL) was considered correct when synergy was observed in both cases. A further parameter was considered for the detection of OXA production, namely a high-level temocillin resistance (>128 µg/ml). MIC values were processed and interpreted using a computer-based algorithm in order to obtain a final result.
Complementary methods of detection of carbapenem non-susceptibility
BMD was performed on 96-well microtiter plates following the specifications of CLSI38 and the International Organization for Standardization44, following the same layout of the DOT-MGA panel. Stock solutions containing meropenem and carbapenemase inhibitors where prepared as described above. The concentrations of the different inhibitors were adapted for the recommended incubation time (18 ± 2 h), longer than that required for DOT-MGA. Bacterial suspension (30 µl) and antibiotic solutions (30 µl) were distributed in the wells and sterility and growth controls were carried out on a second plate. After incubation for 18 ± 2 h at 35 ± 1 °C, turbidity was assessed. MIC was defined as the lowest concentration showing no turbidity. Synergy between meropenem and carbapenemase inhibitors was defined by an 8-fold decrease (or more) of the initial meropenem MIC, indicating the production of a specific carbapenemase class. The method was performed in triplicate and median values were determined.
Strains were also tested with a phenotypic combination disk test (Mast Diagnostica GmbH, Reinfeld, Germany), the carbapenemase-set D70C (meropenem only and combined with MBL, KPC and AmpC inhibitors), as well as disks containing 30 µg of temocillin. Tests were performed and results interpreted according to the manufacturer’s instructions. In short, bacterial suspensions of the analysed strains (McFarland 0.5) were spread on Mueller-Hinton agar plates (BD, Heidelberg, Germany) and disks were placed onto the agar leaving enough space for inhibition zones to be seen correctly. After incubating at 35–37 °C for 18 hours, the inhibition zones were measured and interpreted accordingly.
All clinical strains tested were genotypically characterised using the PCR microarray Check-MDR CT103 XL (Check-Points, Wageningen, The Netherlands). DNA was isolated and the array was performed according to the manufacturer’s instructions. Targeted genes are summarised in Table S2.
Statistical analysis
The PCR was considered an imperfect standard25 for the evaluation of the DOT-MGA. BMD and CDT were compared with PCR as well. Positive and negative percent agreements (PPA and NPA, respectively) of all three methods were calculated according to the statistical guidance of the Food and Drug Administration45.
The data were presented in part on ECCMID 2018, Madrid, 21–24 April (#5622) and IDWeek 2018, San Francisco, 03–07 October (#2066).
Data availability
All data generated or analysed during this study are included in this published article (and its Supplementary Information Files).
References
van Belkum, A. et al. Developmental roadmap for antimicrobial susceptibility testing systems. Nat. Rev. Microbiol. 17, 51–62 (2018).
Roca, I. et al. The global threat of antimicrobial resistance: science for intervention. N. Microbes N. Infect. 6, 22–29 (2015).
Barenfanger, J., Drake, C. & Kacich, G. Clinical and financial benefits of rapid bacterial identification and antimicrobial susceptibility testing. J. Clin. Microbiol. 37, 1415–1418 (1999).
Galar, A. et al. Clinical and economic impact of rapid reporting of bacterial identification and antimicrobial susceptibility results of the most frequently processed specimen types. Eur. J. Clin. Microbiol. Infect. Dis. 31, 2445–2452 (2012).
Shorr, A. F. et al. Inappropriate antibiotic therapy in Gram-negative sepsis increases hospital length of stay. Crit. Care Med. 39, 46–51 (2011).
Pliakos, E. E., Andreatos, N., Shehadeh, F., Ziakas, P. D. & Mylonakis, E. The Cost-Effectiveness of Rapid Diagnostic Testing for the Diagnosis of Bloodstream Infections with or without Antimicrobial Stewardship. Clin. Microbiol. Rev. 31, https://doi.org/10.1128/CMR.00095-17 (2018).
Doern, G. V., Vautour, R., Gaudet, M. & Levy, B. Clinical impact of rapid in vitro susceptibility testing and bacterial identification. J. Clin. Microbiol. 32, 1757–1762 (1994).
Kumar, A. et al. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest 136, 1237–1248 (2009).
ECDC. Rapid risk assessment: Carbapenem-resistant Enterobacteriaceae. First update. European Centre for Disease Prevention and Control, https://ecdc.europa.eu/en/publications-data/rapid-risk-assessment-carbapenem-resistant-enterobacteriaceae-first-update (2018).
Watanabe, M., Iyobe, S., Inoue, M. & Mitsuhashi, S. Transferable imipenem resistance in Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 35, 147–151 (1991).
Livorsi, D. J. et al. A systematic review of the epidemiology of carbapenem-resistant Enterobacteriaceae in the United States. Antimicrobial Resistance & Infection Control 7, 55 (2018).
Pfennigwerth, N. Bericht des Nationalen Referenzzentrums (NRZ) für gramnegative Krankenhauserreger, https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2018/Ausgaben/28_18.pdf?__blob=publicationFile (2018).
Lutgring, J. D. & Limbago, B. M. The Problem of Carbapenemase-Producing-Carbapenem-Resistant-Enterobacteriaceae Detection. J. Clin. Microbiol. 54, 529–534 (2016).
de Lima-Morales, D. et al. Rapid detection of carbapenemase production directly from blood culture by colorimetric methods: evaluation in a routine microbiology laboratory. J. Clin. Microbiol. 56, https://doi.org/10.1128/JCM.00325-18 (2018).
Pasteran, F. et al. Evaluation of the Blue-Carba test for rapid detection of carbapenemases in gram-negative bacilli. J. Clin. Microbiol. 53, 1996–1998 (2015).
Sparbier, K., Schubert, S., Weller, U., Boogen, C. & Kostrzewa, M. Matrix-assisted laser desorption ionization-time of flight mass spectrometry-based functional assay for rapid detection of resistance against beta-lactam antibiotics. J. Clin. Microbiol. 50, 927–937 (2012).
Hooff, G. P. et al. Characterization of beta-lactamase enzyme activity in bacterial lysates using MALDI-mass spectrometry. J. Proteome Res. 11, 79–84 (2012).
Knox, J. et al. Phenotypic detection of carbapenemase-producing Enterobacteriaceae by use of matrix-assisted laser desorption ionization-time of flight mass spectrometry and the Carba NP test. J. Clin. Microbiol. 52, 4075–4077 (2014).
Jung, J. S. et al. Rapid detection of antibiotic resistance based on mass spectrometry and stable isotopes. Eur. J. Clin. Microbiol. Infect. Dis. 33, 949–955 (2014).
Lange, C., Schubert, S., Jung, J., Kostrzewa, M. & Sparbier, K. Quantitative matrix-assisted laser desorption ionization-time of flight mass spectrometry for rapid resistance detection. J. Clin. Microbiol. 52, 4155–4162 (2014).
Idelevich, E. A., Sparbier, K., Kostrzewa, M. & Becker, K. Rapid detection of antibiotic resistance by MALDI-TOF mass spectrometry using a novel direct-on-target microdroplet growth assay. Clin. Microbiol. Infect. 24, 738–743 (2018).
Idelevich, E. A. et al. Rapid Direct Susceptibility Testing from Positive Blood Cultures by the Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry-Based Direct-on-Target Microdroplet Growth Assay. J. Clin. Microbiol. 56, https://doi.org/10.1128/jcm.00913-18 (2018).
Correa-Martinez, C. L., Idelevich, E. A., Sparbier, K., Kostrzewa, M. & Becker, K. Rapid Detection of Extended-Spectrum beta-Lactamases (ESBL) and AmpC beta-Lactamases in Enterobacterales: Development of a Screening Panel Using the MALDI-TOF MS-Based Direct-on-Target Microdroplet Growth Assay. Front. Microbiol. 10, 13 (2019).
EUCAST. Guidelines for detection of resistance mechanisms and specific resistances of clinical and/or epidemiological importance. The European Committee on Antimicrobial Susceptibility Testing. Version 2.0, http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Resistance_mechanisms/EUCAST_detection_of_resistance_mechanisms_170711.pdf (2017).
Valenstein, P. N. Evaluating diagnostic tests with imperfect standards. Am. J. Clin. Pathol. 93, 252–258 (1990).
Köck, R. et al. Carbapenem-resistant Enterobacteriaceae in wildlife, food-producing, and companion animals: a systematic review. Clin. Microbiol. Infect. 24, 1241–1250 (2018).
Daoud, Z. et al. Multidrug-Resistant Enterobacteriaceae in Lebanese Hospital Wastewater: Implication in the One Health Concept. Microb. Drug. Resist. 24, 166–174 (2018).
Logan, L. K. & Weinstein, R. A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 215, 28–36 (2017).
Ma, L. et al. Emergence of OXA-48-Producing Klebsiella pneumoniae in Taiwan. PLoS One. 10, https://doi.org/10.1371/journal.pone.0139152 (2015).
Poirel, L., Potron, A. & Nordmann, P. OXA-48-like carbapenemases: the phantom menace. J. Antimicrob. Chemother. 67, 1597–1606 (2012).
Banerjee, R. & Humphries, R. Clinical and laboratory considerations for the rapid detection of carbapenem-resistant Enterobacteriaceae. Virulence 8, 427–439 (2017).
Philippon, A., Arlet, G. & Jacoby, G. A. Plasmid-determined AmpC-type beta-lactamases. Antimicrob. Agents Chemother. 46, 1–11 (2002).
Woodford, N. et al. Ertapenem resistance among Klebsiella and Enterobacter submitted in the UK to a reference laboratory. Int. J. Antimicrob. Agents 29, 456–459 (2007).
Nepal, S. et al. An ancient family of mobile genomic islands introducing cephalosporinase and carbapenemase genes in Enterobacteriaceae. 9, 1377–1389 (2018).
EUCAST. Breakpoint tables for interpretation of MICs and zone diameters. The European Committee on Antimicrobial Susceptibility Testing. Version 8.1, http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_8.1_Breakpoint_Tables.pdf (2018).
Nordmann, P. et al. Identification and screening of carbapenemase-producing Enterobacteriaceae. Clin. Microbiol. Infect. 18, 432–438 (2012).
Tato, M. et al. Complex clonal and plasmid epidemiology in the first outbreak of Enterobacteriaceae infection involving VIM-1 metallo-beta-lactamase in Spain: toward endemicity? Clin. Infect. Dis. 45, 1171–1178 (2007).
CLSI. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically—Eleventh Edition: Approved Standard M7-A11. Clinical Laboratory Standards Institute, Wayne, PA, USA; (2018).
EUCAST. Routine and extended internal quality control for MIC determination and disk diffusion as recommended by EUCAST. The European Committee on Antimicrobial Susceptibility Testing. Version 8.0, http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/QC/v_8.0_EUCAST_QC_tables_routine_and_extended_QC.pdf (2018).
Huang, T. D., Berhin, C., Bogaerts, P. & Glupczynski, Y. Evaluation of avibactam-supplemented combination disk tests for the detection of OXA-48 carbapenemase-producing Enterobacteriaceae. Diagn. Microbiol. Infect. Dis. 79, 252–254 (2014).
Woodford, N. et al. In vitro activity of temocillin against multidrug-resistant clinical isolates of Escherichia coli, Klebsiella spp. and Enterobacter spp., and evaluation of high-level temocillin resistance as a diagnostic marker for OXA-48 carbapenemase. J. Antimicrob. Chemother. 69, 564–567 (2014).
Jeong, S. H., Song, W., Kim, J. S., Kim, H. S. & Lee, K. M. Broth microdilution method to detect extended-spectrum beta-lactamases and AmpC beta-lactamases in enterobacteriaceae isolates by use of clavulanic acid and boronic acid as inhibitors. J. Clin. Microbiol. 47, 3409–3412 (2009).
Migliavacca, R. et al. Simple microdilution test for detection of metallo-beta-lactamase production in Pseudomonas aeruginosa. J. Clin. Microbiol. 40, 4388–4390 (2002).
ISO. 20776-1. Clinical laboratory testing and in vitro diagnostic test systems–Susceptibility testing of infectious agents and evaluation of performance of antimicrobial susceptibility test devices-Part 1: Reference method for testing the in vitro activity of antimicrobial agents against rapidly growing aerobic bacteria involved in infectious diseases. International Organization for Standardization, Geneva, Switzerland; (2006).
FDA. Guidance for industry and FDA staff–statistical guidance on reporting results from studies evaluating diagnostic tests. Food and Drug Administration, US Department of Health and Human Services, Rockville, MD; (2007).
Acknowledgements
We thank Annkatrin Bibo and Damayanti Kaiser for the excellent technical assistance. This study was funded in part by grants from the German Federal Ministry of Education and Research (BMBF) to EAI and KB (16GW0150) and MK (16GW0149K) and from the European Regional Development Fund within the “MEDUWA Vecht(e)” project (EU/INTERREG VA-1421187 to K.B. and T.K.).
Author information
Authors and Affiliations
Contributions
C.C.-M., E.I. and K.B. designed the experiments. C.C.-M. and E.I. performed the experiments. C.C.-M., E.I., K.S. and M.K. designed and analysed specific MALDI-TOF MS instrument settings for experiments. C.C.-M., E.I., K.S. and K.B. analysed the data. C.C.-M. and E.I. wrote the manuscript with input from K.S., M.K. and K.B. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
E.A.I and K.B. are inventors of a pending patent, which is owned by the University of Münster and licensed to Bruker. K.S. and M.K are employees of Bruker Daltonik GmbH.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Correa-Martínez, C.L., Idelevich, E.A., Sparbier, K. et al. Development of a MALDI-TOF MS-based screening panel for accelerated differential detection of carbapenemases in Enterobacterales using the direct-on-target microdroplet growth assay. Sci Rep 10, 4988 (2020). https://doi.org/10.1038/s41598-020-61890-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-61890-7
- Springer Nature Limited