
Abstract
We hypothesized that blood lactate concentration([Lac]blood) is a function of cardiopulmonary variables, exercise intensity and some anthropometric elements during aerobic exercise. This investigation aimed to establish a mathematical model to estimate [Lac]blood noninvasively during constant work rate (CWR) exercise of various intensities. 31 healthy participants were recruited and each underwent 4 cardiopulmonary exercise tests: one incremental and three CWR tests (low: 35% of peak work rate for 15 min, moderate: 60% 10 min and high: 90% 4 min). At the end of each CWR test, venous blood was sampled to determine [Lac]blood. 31 trios of CWR tests were employed to construct the mathematical model, which utilized exponential regression combined with Taylor expansion. Good fitting was achieved when the conditions of low and moderate intensity were put in one model; high-intensity in another. Standard deviation of fitting error in the former condition is 0.52; in the latter is 1.82 mmol/liter. Weighting analysis demonstrated that, besides heart rate, respiratory variables are required in the estimation of [Lac]blood in the model of low/moderate intensity. In conclusion, by measuring noninvasive cardio-respiratory parameters, [Lac]blood during CWR exercise can be determined with good accuracy. This should have application in endurance training and future exercise industry.
Similar content being viewed by others


Introduction
Blood lactate during aerobic exercise is the result of glycolytic metabolism, an anaerobic energy production pathway in muscle cells. Its concentration in muscle and blood reflect the extent of involvement of anaerobic metabolism. Blood lactate levels are also an important concern in exercise training.
Aerobic exercise intensity has been divided into three zones by ventilatory threshold 1(VT1) and ventilatory threshold 2(VT2) identified by breath-by-breath gas exchange measurement during incremental exercise testing1. In the moderate zone (between VT1 and VT2), the [Lac]blood is increased but production and elimination rates reach equilibrium. VT2 is the highest possible intensity to achieve a steady [Lac]blood, termed maximal lactate steady state2,3,4. Studies demonstrated that the intensity of endurance training between VT1 and VT2 significantly improved fitness among the untrained subjects5,6. In addition, in the high zone above VT2, the [Lac]blood accumulates rapidly and fatigue is forthcoming. VT1(also lactate threshold or anaerobic threshold) and VT2(also respiratory compensation point or onset of blood lactate accumulation) correspond to 1~2 and 4 mM/liter blood lactate concentration respectively2. Accordingly, it is valuable to noninvasively obtain the numerical value of [Lac]blood during endurance training.
The current investigation attempted to establish a novel mathematical model to estimate [Lac]blood noninvasively. During exercise, an extremely complicated relationship exists between [Lac]blood and tidal volume (VT), breathing frequency (BF), exercising heart rate(ExHR), resting HR(ReHR), and anthropometric characteristics such as body weight. Exercise intensity plays a key role in delineating the complex interaction among these physiologic variables. As intensity increases, HR, Bf, VT and [Lac]blood all increase but with different trajectories. Accordingly, we hypothesized that [Lac]blood is a function of cardiopulmonary variables, exercise intensity and anthropometric characteristics.
Methods
Thirty-one healthy male and female participants between 20 and 50 years-old were recruited by convenience sampling (Table 1). Those with cardiovascular illness were excluded. The experiment protocol was approved by the Chang Gung Memorial Hospital Institutional Review Board. All the subjects provided written informed consent after receiving an oral and printed explanation of the experimental procedures. This research was performed in accordance with the ethical standards of the Declaration of Helsinki.
Cardiopulmonary Exercise test and blood lactate measurement
Every participant underwent four cardiopulmonary exercise tests on a cycle ergometer (Ergoselect 150 P, Germany) on different days: one incremental and three constant work rate (CWR) tests. CWR tests were of mild, moderate and high intensity. Each subject was instructed to refrain from exercise for 12 hours before each test. The incremental exercise test comprised 1 minute of unloaded pedaling followed by an incremental increase in work rate of 15 watts per minute until exhaustion; thereby the peak work rate was determined. The VO2peak was defined by the following criteria: (i) VO2 increased by less than 2 mL/kg/min over at least 2 min, (ii) HR exceeded 85% of its predicted maximum, (iii) the respiratory exchange ratio exceeded 1.15, or (iv) some other symptom/sign limitations7. Subsequently, each subject performed three CWR exercise tests: 15-minute low-constant load at 35% peak work rate, 10-minute moderate-constant load at 60% peak work rate and 4-minute high constant-load at 90% peak work rate. The CWR intensity of low (35%), moderate (60%) and high (90%) were chosen based on three zones: below VT1, between VT1 and VT2, and above VT21,2. In the majority of healthy people, VT occurs at 40–60% of VO2max8. RCP has been reported to be 61.3 to 85.4% of VO2max in healthy subjects3,9. Minute ventilation (VE), oxygen uptake (\(\dot{{\rm{V}}}{{\rm{O}}}_{2}\)), and carbon dioxide production (\(\dot{{\rm{V}}}{{\rm{C}}{\rm{O}}}_{2}\)) were measured breath-by-breath using a computer-based system (MasterScreen CPX, Cardinal-health Germany). Heart rate (HR) was determined from the R-R interval of a 12-lead electrocardiogram (CardioSoft, GE, Wilwaukee, USA). Arterial blood pressure was measured every two minutes using an automatic blood pressure system (Tango, SunTech Medical, UK), and arterial O2 saturation was monitored continuously by a finger pulse oximetry (model 9500, Nonin Onyx, Plymouth, Minnesota). End-exercise values were determined as the average of the final 30 seconds of exercise. In the CWR tests, venous blood was sampled mostly from an antecubital vein or in a few cases from a dorsal interosseous metacarpal vein for [Lac]blood assay 30–60 seconds after the end of constant work rate exercise tests. The sample was collected in NaF/K3EDTA tubes and then placed on ice. The whole blood was centrifuged within 90 minutes to obtain plasma, which was stored at 4 °C. [Lac]blood was measured by the enzymatic method within 14 days after sampling (DXC880i).
Mathematical model for lactate estimation
We propose a novel model to estimate [Lac]blood by noninvasively-measured physiologic signals including VT, BF, ReHR, ExHR, age, body mass index (BMI) and sex at the end of the CWR testing. The model is based on an exponential regression method combined with Taylor expansion10 to find the best predictors of [Lac]blood.
Exponential function and Taylor expansion
An exponential regression model between [Lac]blood and the physiologic signals at CWR testing was examined, including BF, VT, BMI, age, ReHR and ExHR. We asserted that the connection between [Lac]blood and various physiologic signals can be formulated into a poly-exponential function11,12 and defined by equation 1.
where x is a matrix of the independent variables, A is the weighting matrix corresponding to each independent variable, and f(x) is [Lac]blood. A supervising gradient descent was adopted to equation 1 to solve the model A with a full-rank matrix by x and f(x)13. In order to solve the equation 1 efficiently, Taylor expansion was applied to transfer equation 1 into polynomial form for linear solution. Taylor expansion can be expressed in equation 2 for x = a.
Equation 1 can be transformed into equation 3 for cubic approximation polynomials by Taylor expansion.
Equation 3 is rewritten in matrix form as follows14.
where \({\rm{A}}=[{a}_{0}-{a}_{1}\,\frac{{a}_{2}}{2!}\,\frac{-{a}_{3}}{3!}]\) and \({\rm{X}}={[1x{x}^{2}{x}^{3}]}^{T}\).
Linear regression
Equation 4 is the relationship between the multiple independent variables X and [Lac]blood; the model A can be solved by linear regression analysis15 Additionally, leave-one-out cross validation was applied to avoid overfitting8–10 as follows:
In the training step, physiologic, anthropometric variables and [Lac]blood from the database involving CWR testing at low, moderate and high intensity were employed to construct the A matrix and solve for regression coefficients. In the testing step, estimated blood lactate concentration ([Lac]estimate), \(\hat{Y}=AX\), was used to verify the difference between true and the estimated lactate value by error and variance.
The error distance d is
and the sum of squares D of all data is
Where σ2 is the variance. The solution matrix A in equation 5 is satisfied with the minimum D in order to get the minimum error variance.
Leave-one-out cross validation
Additionally, leave-one-out cross validation was applied to avoid overfitting16,17,18, which is briefly described as follows:
-
If k observations are recorded, one is used for testing and the other k-1 observations are for training.
-
The above procedure is repeated k times in the k observations for testing and training.
-
Mean square error is used for justification in order to get the best model. The mean square error of the leave-one-out cross validation models was determined at about 0.27 in the low & moderate intensity model and 0.25 in the high intensity model.
Weighting factor
In the linear regression, the selected 8 independent variables were used to build the model for lactate estimation. The 8 weightings directly acquired from the model A in equation 5 corresponding to the 8 factors are the absolute positive or negative weighting. Additionally, normalized weighting was computed, which was defined by each absolute positive or negative weighting divided by sum of all the absolute positive or negative weighting. These two kinds of weighting were applied to quantify the impact of the 8 independent variables in lactate estimation.
Implementation
Modeling was performed in MATLAB 2014b (MathWorks®, Natick, Massachusetts, United States).
Statistics
Linear correlation and Bland-Altman plots19 were employed to show the validity of estimated blood lactate level. Descriptive statistics were also used. Data are presented as mean ± standard deviation.
Results
The average work rate corresponding to low, moderate and high CWR was 66 ± 29, 107 ± 46 and 146 ± 66 watts. The mean [Lac]blood was 3.7 ± 2.3, 6.9 ± 4.2 and 10.4 ± 4.1 mM/liter for the three intensities (Table 2).
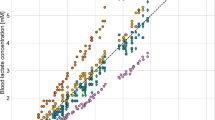
The mathematical analysis showed that, if low, moderate and high intensity are processed together, the fitting error was large (Fig. 1G–I). However, if we fit the data in low- and moderate- intensity CWR (Fig. 1A–C) together, and fit the high-intensity data (Fig. 1D–F) separately, the fitting error becomes much smaller. In these two conditions, both models fit the data quite well, especially low and moderate intensity, in which the standard deviation of fitting error is 0.52 mmol/liter (Fig. 1B). This indicates that a very different relationship exists between [Lac]blood and these measured variables under the two conditions: low/moderate, and high intensity.

Model estimates of blood lactate concentration compared with the measured value. (A–C) are low combined with moderate intensity CWR tests. (D–F) are those for high-intensity exercise. (G–I) is the model obtained when the data of three different intensities are combined. Scatter plot are demonstrated in (A,D,G). Agreement using Bland-Altman plot are shown in (B,C,E,F,H) and (B,E,H,I) show the difference between estimated and measured value. (C,F,I) are the percentage of estimation error. The dark solid horizontal lines in each Bland-Altman plot represent average bias whereas the dotted lines stand for average bias ± 1.96 standard deviation (95% upper and lower limit). The standard deviation in (B,E,H) are 0.52, 1.83 and 2.51 mmol/liter. The standard deviation in (C,F,I) are 0.1, 0.2 and 0.53.
Figure 2A presents the absolute weighting of each variable in determining [Lac]blood. In low & moderate constant-load intensity, ReHR, BF and age have the greatest positive influence. On the other hand, during high-intensity condition, ExHR alone has a significant impact (Fig. 2B).

Absolute positive or negative weighting of each variable in determining blood level of lactate. BMI: body mass index; ExHR: exercising heart rate; BF: breathing frequency; VT: tidal volume
Discussion
In the present investigation, responses to 31 trios of CWR exercise tests in 31 subjects were employed to construct a mathematical model to estimate [Lac]blood from noninvasive measurement. The database is comprised of low, moderate and high intensity exercise tests. The model is based on exponential regression method combined with Taylor expansion. The independent variables included ExHR, ReHR, Bf, VT, BMI, age and sex. Excellent fitting was achieved in the conditions of low and moderate intensity in one model, and high-intensity in another model. The standard deviations of fitting error in the former condition is 0.52 mmol/liter; and is 1.82 in the latter condition, which are acceptable for the purposes of specifying exercise training targets.
This result implies that exercise intensity is a significant determinant in the complex relationship between [Lac]blood and cardiopulmonary variables. Poor fitting was obtained when we attempted to construct a single mathematical model including of three exercise intensities. Three intensity zones divided by VT1 and VT2 has been reported to have distinct differences in sympathetic stress load, motor unit involvement, and duration to fatigue2. The difference could be too large to be mathematically processed in a single model. Additionally, regarding to the model construction, the accuracy of [Lac]blood was also affected by the amount and consistency of the training data. The database in the present study is small compared to the sample size commonly employed in deep learning. The consistency of our data, as revealed by the leave-one-out validation, is good. Therefore, increase of the sample size will improve the precision of the estimation, especially in the high-intensity database. It is also worth mentioning that multiple linear regression was attempted at first. Little or low correlation was found between almost all the independent variables versus [Lac]blood (the highest correlation coefficient is 0.54). Accordingly, a more complicated mathematical method is adopted in the analysis.
Modeling weight distribution analysis showed that BF is indispensible and even more important than heart rate as an independent variable in the conditions of low/moderate intensity. The advancement of wearing device is progressing rapidly, exercising BF may be acquired conveniently soon though we are unaware of any wearable devices that measures currently. The mathematical model is constructed with a view to applying it in the exercise industry. Therefore, \(\dot{{\rm{V}}}{{\rm{O}}}_{2}\) and \(\dot{{\rm{V}}}{{\rm{C}}{\rm{O}}}_{2}\) are not included because they are quite impossible to obtain without a gas analysis system.
The algorithm of the current study could be applied in the threshold training model2 of cycling endurance training. The suitable intensity is to keep [Lac]blood in the range of VT1 and VT2, especially for the untrained people. The corresponding [Lac]blood are 1~2 and 4 mM/liter2. SD of fitting error in the low/moderate model is 0.52 mM/liter. Considering the width of the middle zone, the fitting error should be acceptable. Increase the sample size will further minimize the fitting error. Another possible application could be in the CWR testing. Estimated [Lac]blood may be used as a criterion to judge whether the subject approaches maximal effort when gas analysis to measure \(\dot{{\rm{V}}}{{\rm{O}}}_{2}\) plateau is not available. A variety of [Lac]blood cut-off values have been proposed. Most of the criteria are around 8 mM/liter20,21. Further study is needed to prove this idea.
The mathematical methodology employed in this study should apply to other CWR conditions during exercise. The most common scenario is in treadmill exercise in which speed and slope are fixed. Further, some steppers are provided with constant-power modes. Additionally, wearable device that measure physiological responses are being developed. Our model to estimate [Lac]blood would be relevant to a free ambulation constant work rate task in which cardiac and respiratory responses are measured.
There are several study limitations. First, the sample size is relatively small. However, good validity is still attainable, which suggests that the mathematical model employed in the present study works. A large database should be acquired to increase the accuracy, especially in the model of high intensity. Secondly, equation (regression coefficient or A value) obtained in this study may only be relevant to CWR cycle ergometer exercise. Studies should be undertaken to test its validity during other exercise modalities (e.g., treadmill, walking). Third, prospective validation procedures were not performed in this study. Nonetheless, if we do prospective validation, those data can be pulled into the learning model to generate a new regression coefficient. Leave-one-out cross validation8 was already applied to our model to determine the overfitting statistical learning.
Conclusion
This is the first study to establish a mathematical model in predicting the numerical values of [Lac]blood during exercise. By measuring noninvasive cardio-respiratory parameters and including some anthropometric factors, [Lac]blood during constant work rate exercise can be determined with good validity by exponential regression combined with Taylor expansion. These experimental finding should have application in designing intensities during endurance training and future exercise industry.
Data Availability
The datasets generated during and/or analysed during the current study are not publicly available due to its potential commercial interest but are available from the corresponding author on reasonable request.
References
Esteve-Lanao, J., San Juan, A. F., Earnest, C. P., Foster, C. & Lucia, A. How do endurance runners actually train? Relationship with competition performance. Med Sci Sports Exerc 37, 496–504 (2005).
Seiler, K. S. & Kjerland, G. O. Quantifying training intensity distribution in elite endurance athletes: is there evidence for an “optimal” distribution? Scand J Med Sci Sports 16, 49–56, https://doi.org/10.1111/j.1600-0838.2004.00418.x (2006).
Dekerle, J., Baron, B., Dupont, L., Vanvelcenaher, J. & Pelayo, P. Maximal lactate steady state, respiratory compensation threshold and critical power. Eur J Appl Physiol 89, 281–288, https://doi.org/10.1007/s00421-002-0786-y (2003).
Garcia-Tabar, I. & Gorostiaga, E. M. A. “Blood Relationship” Between the Overlooked Minimum Lactate Equivalent and Maximal Lactate Steady State in Trained Runners. Back to the Old Days? Front Physiol 9, 1034, https://doi.org/10.3389/fphys.2018.01034 (2018).
Londeree, B. R. Effect of training on lactate/ventilatory thresholds: a meta-analysis. Med Sci Sports Exerc 29, 837–843 (1997).
Gaskill, S. E. et al. Changes in ventilatory threshold with exercise training in a sedentary population: the HERITAGE Family Study. Int J Sports Med 22, 586–592, https://doi.org/10.1055/s-2001-18522 (2001).
Balady, G. J. et al. Clinician’s Guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Circulation 122, 191–225, https://doi.org/10.1161/CIR.0b013e3181e52e69 (2010).
Mezzani, A. et al. Standards for the use of cardiopulmonary exercise testing for the functional evaluation of cardiac patients: a report from the Exercise Physiology Section of the European Association for Cardiovascular Prevention and Rehabilitation. Eur J Cardiovasc Prev Rehabil 16, 249–267, https://doi.org/10.1097/HJR.0b013e32832914c8 (2009).
Yamamoto, Y. et al. The ventilatory threshold gives maximal lactate steady state. Eur J Appl Physiol Occup Physiol 63, 55–59 (1991).
Greenberg, M. Advanced Engineering Mathematics (2nd Edition). (Prentice Hall, 1998).
Pearl, M. L., Yashar, C. M., Johnston, C. M., Reynolds, R. K. & Roberts, J. A. Exponential regression of CA 125 during salvage treatment of ovarian cancer with taxol. Gynecol Oncol 53, 339–343, https://doi.org/10.1006/gyno.1994.1144 (1994).
Luque-Fernandez, M. A. et al. Adjusting for overdispersion in piecewise exponential regression models to estimate excess mortality rate in population-based research. BMC Med Res Methodol 16, 129, https://doi.org/10.1186/s12874-016-0234-z (2016).
Patel, V. Kalman-Based Stochastic Gradient Method with Stop Condition and Insensitivity to Conditioning. Siam J Optimiz 26, 2620–2648, https://doi.org/10.1137/15m1048239 (2016).
Alexopoulos, E. C. Introduction to multivariate regression analysis. Hippokratia 14, 23–28 (2010).
Cohen, J. & Patricia, C. Applied multiple regression/correlation analysis for the behavioral sciences. (2nd Edition). (NJ: Lawrence Erlbaum Associates, 2003).
Bermingham, M. L. et al. Application of high-dimensional feature selection: evaluation for genomic prediction in man. Sci Rep 5, 10312, https://doi.org/10.1038/srep10312 (2015).
Kohavi, R. A study of cross-validation and bootstrap for accuracy estimation and model selection. Proceedings of the Fourteenth International Joint Conference on Artificial Intelligence 2, 1137–1143 (1995).
Arlot, S. & Celisse, A. A survey of cross-validation procedures for model selection. Statistics Surveys, Institute of Mathematical Statistics (IMS) 4, 40–79 (2010).
Carkeet, A. Exact parametric confidence intervals for Bland-Altman limits of agreement. Optom Vis Sci 92, e71–80, https://doi.org/10.1097/OPX.0000000000000513 (2015).
Van Remoortel, H. et al. Validity of six activity monitors in chronic obstructive pulmonary disease: a comparison with indirect calorimetry. PLoS One 7, e39198, https://doi.org/10.1371/journal.pone.0039198 (2012).
Astrand, P.-O. Experimental Studies of Physical Working Capacity in Relation to Sex and Age. 23–27, 92–102 (Copenhagen: Ejnar Munksgaard, 1952).
Acknowledgements
This research was supported by Chang Gung Memorial Hospital [grant No. CMRPG3E1561/2], ECHOWELL ELECTRONIC CO., LTD. [XMRPG3C0941] and Healthy Aging Research Center, Chang Gung University and the Taiwan Ministry of Education’s Higher Education Deep Plowing Program (Grant Numbers EMRPD1H0351 and EMRPD1H0551).
Author information
Authors and Affiliations
Contributions
Conceptualization: Shu-Chun Huang, Richard Casaburi, Ming-Feng Liao, Hong-Ren Su. Data curation: Shu-Chun Huang, Hong-Ren Su, Kuo-Cheng Liu, Yu-Jen Chen. Formal analysis: Shu-Chun Huang, Richard Casaburi, Hong-Ren Su. Funding acquisition: Shu-Chun Huang. Investigation: Shu-Chun Huang, Hong-Ren Su. Methodology: Shu-Chun Huang, Richard Casaburi, Hong-Ren Su. Project administration: Shu-Chun Huang, Hong-Ren Su. Resources: Shu-Chun Huang, Hong-Ren Su. Software: Hong-Ren Su. Supervision: Shu-Chun Huang, Richard Casaburi, Hong-Ren Su. Validation: Shu-Chun Huang, Richard Casaburi, Hong-Ren Su. Visualization: Shu-Chun Huang, Richard Casaburi, Hong-Ren Su, Kuo-Cheng Liu Writing ± original draft: Shu-Chun Huang, Richard Casaburi, Hong-Ren Su, Kuo-Cheng Liu Writing ± review & editing: Shu-Chun Huang, Kuo-Cheng Liu, Yu-Jen Chen, Tieh-Cheng Fu, Hong-Ren Su.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, SC., Casaburi, R., Liao, MF. et al. Noninvasive prediction of Blood Lactate through a machine learning-based approach. Sci Rep 9, 2180 (2019). https://doi.org/10.1038/s41598-019-38698-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-38698-1
- Springer Nature Limited