
Abstract
Background
Quality of care is under pressure due to demographic changes (shifting age of the population), epidemiological trends (more chronic diseases) and changes in the external environment (rapid development of technological innovations). Transformation in care is essential to deal with these changes. However, there is no consensus in the literature regarding the definition and factors contributing to care transformation.
Methods
This systematic review systematically searched the scientific databases Scopus, Web of Science and Pubmed until 22 January 2022. We included articles that focused on care transformation from a complex setting and multi-level perspective, with an empirical or theoretical rationale and methodology. Relevant data regarding the interconnection between contextual conditions, mechanism of change and outcomes were analysed using deductive coding. The generic contextual conditions-mechanisms outcome structure (CMO) as reported (Pawson and Tilly in Realistic Evaluation, Sage Publication Ltd, London, 1997) was used as a framework to synthesise the results.
Results
Nineteen articles were included. All related articles explain transformation from a complex systems perspective. Four of the 19 articles gave a definition of care transformation. These definitions of care transformation have the following in common: It involves radical and far-reaching change at an organisational and system-wide level, with the aim of improving performance, behaviour, efficiency, and quality of care, both at individual and population level. Relevant contextual conditions were the changing environment, organisational conditions, collaboration, direction of change and sources of funding. Relevant mechanisms for change were collaboration, leadership, interpersonal relationships, engagement, information technology and coordination. The key outcomes of care transformation are Integration of care, patient-centred care, and improvement of quality of care.
Conclusions
An important goal of care transformation is to deliver better quality of care and enable care integration. This study showed that effective collaboration among healthcare providers, supported by transformational leadership, strong interpersonal relationships, and coordination from multiple perspectives, play an important role in facilitating care transformation. Collaboration is an important mechanism for achieving the key outcomes of care transformation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
In 2015, the United Nations (UN) presented the 2030 Agenda for Sustainable Development, consisting of 17 goals, representing the transformational vision for the world [33, 38] One of the goals focused on improving the quality of care, namely "ensuring healthy lives and promoting well-being for all ages" [33, 38]. Transformation is needed because the care environment is facing demographic and epidemiological trends and developments that put pressure on the quality of care.
A first trend is a shift in the age structure of the population. The number of people over 60 years old worldwide is increasing dramatically, at a faster rate than before [4, 22, 39] Second, a shift is evident in the leading causes of death from infectious diseases in children to non-communicable diseases associated with ageing [10]. In addition, an increase in lifestyle-related diseases puts both more pressure on the health care system and asks for different approaches in providing care [22]. Fourth, due to depleted medical and nursing staff delays occur in regular care, e.g. waiting lists [3]. Fifth, explosive technological innovations and their acceptance are resulting in disruption of the healthcare system. The introduction of these technologies affects all levels of healthcare, including society, processes, structures, organisational coordination, and the way professionals do their work [29]. Finally, there is a high fragmentation of services within health care caused by various factors such as: subspecialties, data silos, market forces and competition between healthcare organisations for resources [6, 22, 31].
These trends, developments and changes require transformation of healthcare rather than an incremental change. Hence, within a complex system such as healthcare, there is a high degree of interconnectedness between the actors involved, resulting in a high degree of interdependence between them [27]. A complex system is associated with high levels of uncertainty and low levels of agreement [27]. The response of the healthcare system to this ‘wicked problem’ requires a radical change in mindset, internal and external goals, norms and values [19, 34]. Transformation is needed to enable this fundamental, irreversible change in an organisation's vision and way of working. The role of interventions to achieve this transformation is important to consciously improve care. More recent literature highlights showed that little is known about how transformation can be driven [30].
The aim of this systematic literature review is twofold namely, to provide insight (1) into care transformation and the process of transformation; (2) to change the process of care transformation. This review describes the existing definitions of care transformation and the contexts and mechanisms of care transformation. Hence, the research question was: how is care transformation conceptually explained in the existing scientific literature?
2 Methods
2.1 Research design
A systematic literature review was conducted following the guidelines of the Grounded Theory Literature Review [40]. Hanelt et al. [17] and Coles et al. [9] adopted Pawson and Tilley's [37] generic contextual conditions-mechanisms-outcome structure (CMO) in their studies [9, 17]. This allows the data collected to be analysed without bias or prior assumptions (validity and reliability). The aim of this review is to conceptually define and identify which aspects play a role in care transformation. To identify care transformation, we focus on the theory of change, describing the context, mechanisms of change and outcomes. According to the theory of Pawson and Tilly [37] context refers to the social, political, economic, and historical circumstances or conditions that shape the emergence and impact of social programs, policies, and interventions. Context includes both the immediate circumstances in which a program or policy is implemented, as well as the broader social and historical forces that shape the context of the intervention [37]. Pawson and Tilly define a mechanism as a measure that gives a specific pattern of outcomes in each context [37]. Outcomes are defining as; "the practical effects produced by causal mechanisms, set in motion from a given context" [37].
2.2 Search strategy
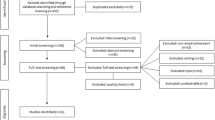
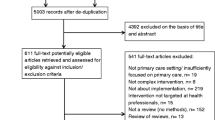
The search focused on articles describing or discussing transformations within healthcare at multiple levels and across different sectors. Multiple levels referred to the different organisational levels (macro, meso and micro). Sectors referred to first-, second- and third-line care. This choice was made to obtain a wide range of literature addressing the concept of care transformation and identifying the aspects involved. The Web of Science, Scopus and Pubmed databases were systematically searched until 22 January 2022 [2]. The search strategy is shown in Fig. 1 and Additional file 3: Appendix S3. The search was limited to the years 2000 to 2022, the English language and specific research areas (e.g., health care, social sciences, medicine, business administration and management). The limitation regarding the scope of the years was made because it is only from the year 2000 that the concept of care transformation is discussed in the scientific literature. Only Western countries were selected because they are socio-economically comparable and in terms of level of care provision [4]. Additional file 3: Appendix S3 provides an overview of the criteria for the systematic search. The PRISMA model was used [36] to summarise the study choice process (Fig. 2).

Search strategy in pubmed

Selection process of the included articles
First, a list of articles emerged from the search series was compiled. Duplicates were then filtered out based on DOI and title. Articles were then jointly reviewed by the research team (G.A.G. Garritsen, S.F.H. Hulshof, W.A. Keijser) on title and abstract. The researchers used the snowball method to search wider and deeper into the literature with the aim of finding lesser known and/or more recent literature that did not emerge directly from the search. In case of disagreement, a decision was made based on arguments by the members of the research team. Based on this review, articles were selected for inclusion in the full-text review. The inclusion and exclusion criteria were determined and refined by mutual agreement among the researchers. At this stage, inter-rater reliability was calculated, where it was agreed that there should be at least 90% overlap between reviewers [32]. Inter-rater reliability ranged from 0.84 in the first trial of 100 items to 0.93 in the fourth trial of 200 items. After four trials, reviewers agreed on the following selection criteria:
2.2.1 Inclusion criteria
-
The perspective of the included articles is multi-level; micro, meso, macro.
-
The following themes were included: transformation, transition, co-design, re-institutionalisation, re-engineering, and radical change.
-
The next settings were included: complex setting, ecosystem, region, networks involving different parties/disciplines/domains within the healthcare context.
-
The following types of literature were included: empirical and theorizing concerning research with the theoretical foundation, including SLR. Practical studies with incorporation of research methodology.
2.2.2 Exclusion criteria
-
Commentaries, opinion articles, book chapters, conference papers, narrative reviews were excluded.
-
The following themes were also excluded: improvements, innovation, implementation, small changes, tech-driven changes.
The perspective should reflect all organisational levels (macro and meso and micro) in the article to be included. Within the theme, the focus was on the disruptive nature of a change. This means that incremental innovations were not included. This also applies to technology-driven changes. A total of 63 articles were screened for their full text. The articles were randomly assigned to one of two researchers (G.A.G. Garritsen, S.F.H. Hulshof). They read the articles independently and decided on inclusion or exclusion. The third investigator (W.A. Keijser) read all the articles to confirm the decision. Of the 63 articles screened, 19 were selected by the research team for coding (see Additional file 1: Appendix S1). In an iterative process, the 19 full-text articles were analysed using deductive coding with the CMO framework as a starting point [37, 40].
2.3 Data analysis
Studying the articles, we examined which shift of change led to which type of outcome. The data analysis process involved several steps. Firstly, a thorough examination was conducted to identify if a definition of care transformation was utilized in the literature. If such a definition was found, it was documented for further analysis. Secondly, the focus shifted towards exploring the presence and content of discussions regarding contextual conditions, mechanisms, and outcomes. It was crucial to understand the meaning of each factor in the context of the study and to only include information that directly emerged from the articles, such as outcomes reported within the study rather than mentions in the introduction. Finally, all fragments labeled as context, mechanism, or outcome were systematically coded inductively into their respective categories. This iterative process allowed for a comprehensive analysis of the data, ensuring that relevant insights were captured and properly classified. First, a document analysis (see Additional file 1: Appendix S1) was prepared. This analysis provides insight and a picture of all coding used. It indicates how often and in which article the relevant coding occurs. This analysis was made using the programme Atlas.ti. In addition, a co-occurrences analysis was used as a method to gain insight into which codes occur together to a reasonable extent in the studied included articles. The programme Atlas.ti was used for this purpose.
3 Results
A total of 19 articles were included in the systematic review. The data analysis resulted in 29 code groups, which could be linked to context, mechanisms, and outcomes (i.e., CMO, see detailed description in Additional file 3: Appendix S3) [37]. Four articles give a definition of care transformation.
3.1 Definition of care transformation
Four of the 19 articles studied proposed a definition of care transformation. Kash et al. [25] described transformation from the perspective of the organisation. They defined care transformation as "a radical, sweeping change or reform of the performance and behavior of the organisation and its people" [25]. Best et al. [5] linked the definition to the whole system and defined care transformation based on “necessary interventions, affecting multiple healthcare organisations” [5]. According to Nyström et al. [35], large system transformation is defined as: "interventions aimed at coordinated, system-wide change affecting multiple organisations and healthcare providers, with the aim of significantly improving healthcare efficiency, quality of patient care and patient outcomes at the population level"[35]. Finally, Hunter et al. [22] defined care transformation as a "never-ending process in which continuous structural change takes place” [22]. Both Nyström et al. [35] and Best et al. [5] emphasised transformation from a public health approach, in which improving the quality of care for the whole population is an important outcome. Based on the 4 definitions found, it can be said that the definitions of Best et al. [5] and Hunter et al. [22] focus on process and the definitions of Kash et al. [25] and Nyström et al. [35] on interventions [5, 22, 25, 35]
3.2 Context
The changing environment (24 codes in 12 of the 19 articles) and collaboration (18 codes in 9 of the 19 articles), in addition to direction of change and funding sources (18 codes in 9 of the 19 articles), are contexts that often recur in the articles studied. The main contexts from the literature review are further explained below. Contexts that were coded but occurred less frequently in the articles studied and are not discussed further are: communication, complexity, culture, process and procedures, financial resources, and trust. Additional file 1: Appendix S1 lists all codes used and the frequency that a code was used in an article.
3.2.1 Context—changing environment
In this study, changing environment refers to external elements that cause an entity but cannot be influenced. The included studies described environment dynamics, changing demographics, frequently changing policies and changing patterns as contexts that determine the success or failure of deploying change [15, 21, 22]. Furthermore, Urtaran, [39] indicates that system-wide transformations are influenced by political dynamics and specific contexts (e.g. health insurance) [39].
3.2.2 Context—organisational conditions
Organisational conditions, in this study, refers to the ability of an organisation to provide direction and design for change initiatives. Too much demarcation between health and society and bounded thinking from an organizational perspective affect the success of change initiatives [25]. Uncertainties about the organisation’s design for change can also be limiting [11, 14, 31]. According to Kash et al. [25], sticking to the same way of working affects the 'absorptive capacity' of organisations to. Absorption refers to the ability to discover and aggregate innovations, within and across healthcare organisations; a key prerequisite for successful transformation [25].
3.2.3 Context—direction of change and availability of resources
A clear direction of public policy (politics and ideology) is an important factor for sustaining and supporting successful change initiatives [22, 31]. In addition, a clear vision to care transformation and commitment to change are key elements for achieving system-wide transformation [39]. Lack of alignment between different funding models, especially important in system-wide change, and budgetary constraints can be barrier of the initiated transformation [24].
3.2.4 Context—collaboration
The collaboration context refers to the conditions needed to connect people and organisations. Most of the included articles address forms of collaboration between entities and at the system level. Only the articles by Hutchinson [24] and Maniatopolous et al. [31] considered collaboration within an organisation (see Table 1) [24, 31]. According to Halsall et al. [16], the alignment of structures and processes between organisations and the sharing of information are important features and conditions to achieve collaboration. The competitive environment (market forces) can be a barrier that limits collaboration due to differences in incentives [16].
3.2.5 Co-occurrences analyse of context
A Co-occurrences analysis (Additional file 2: Appendix S2) showed that context leadership and context information technology occur together to a reasonable extent (c-coefficient = 0.3). This is further confirmed from the publications of Chrystanthaki [8] and Kash et al. [25]. Chrystanthaki [8] describes that IT systems, structures and leadership at the strategic level must be a prerequisite to achieve major systemic change [8, 25]. Kash et al. [25] confirmed that the combination of leadership and the use of information technology, are important characteristics to bring about change. In addition, they indicate that strong leadership enables everyone to seek insights and improvements in processes and the overall functioning of the organisation. Information technologies optimise essential (administrative, clinical, social, and informational) processes, structures, and objectives [25]. Care transformation involves improving the quality, accessibility, and affordability of healthcare services using innovative technologies and processes. Effective leadership is essential for driving transformational change in healthcare organisations, as described by Chrystanthaki [8]. This includes strategic planning, collaboration and developing a vision for the future of healthcare [8].
3.3 Mechanism
Key mechanisms mentioned in the articles included are collaboration (58 codes in 16 of the 19 articles), engagement (22 codes in 8 of the 19 articles), Interprofessional relationship (23 codes in 12 of the 19 articles), leadership (39 codes in 11 of the 19 articles), coordination (22 codes in 8 of the 19 articles) and Information Technology (20 codes in 11 of the 19 articles). These key mechanisms are detailed below. Mechanism that was coded but occurred less frequently in the articles studied and are not discussed further are communication, culture, education, financial structure, organisational elements process and procedures. Additional file 1: Appendix S1 gives an overview of all used codes, the frequency and mentioned articles.
3.3.1 Mechanism—collaboration
The analysis of the articles studied shows that the mechanism 'collaboration' is mentioned to a reasonable extent. The aim of collaboration is integration at all levels and improvement of quality of care. To create integrated care and improve quality of care, collaborative relationships between organisations and collaboration from people within an organisation are essential. Multiple studied articles confirm the importance of building positive relationships with external partners based on trust, personal contact, short lines of communication and appropriate available structures [15, 16, 31].
3.3.2 Mechanism—leadership
Kash et al. [25] talk about three different leadership mechanisms that can be deployed; convergent leadership (promotes cooperative effectiveness), generative leadership (creates potential for change by bringing in more alternatives) and finally unified leadership (balance between centralised and distributed leadership). Generative leadership is more transactional in nature. Convergent and unified leadership are transformational, so more suitable for care transformation. For leadership as a mechanism to work well, the type and style of leadership are important, as well as the ability to transfer such skills within an organisation (dispersed/distributed leadership) [25].
3.3.3 Mechanism—engagement
Openness and engagement are an important mechanism to mobilize communities, where healthcare organisations actively involved clients to make change sustainable [15, 21]. Maniatopoulos [31] finds that higher levels of engagement lead to better results in initiating change initiatives [31].
3.3.4 Mechanism—interprofessional relationships
Interprofessional relationships are derived from the fact that different audiences with diverse knowledge working together based on shared values. Aggarwal [1] indicates that by combining knowledge and expertise of different professions (nurse, nurse-specialist, therapists, and technologists), more comprehensive integrated and person-centred care can be deployed to improve quality care [1]. Combining knowledge and expertise thus contributes to transforming care. Greenhalgh [15] describes that the coming together of people and resources to build relationships contributes to gaining a sense of community and results in value-driven change [15].
3.3.5 Mechanism—coordination
Bussu [7], like Aggarwal [1] and Hussey et al. [23], talks about the use of care navigators as a coordination mechanism for patients with multiple care needs. Hussey et al. [23] talks about care navigators in primary care to better guide a patient through the system. Care navigators act as a central coordinating point of contact and help organise and coordinate different aspects of care. Care navigators thereby contribute to improving the quality of care and are important as a mechanism in transforming care [1, 7, 23]. Urtaran et al. [39] indicate that bottom-up interventions at the local level contribute to better coordination and therefore enable integration rather than a focus on structural or managerial integration. [39]. Nyström et al. [35] mainly emphasise that those change initiatives that are complex require more structuring and coordination [35].
3.3.6 Mechanism—information technology
Aggarwal [1] indicates that well-designed information management systems are supportive across the continuum of care and generate performance measures that contribute to improved quality of care. Performance monitoring is an important support mechanism. It enables healthcare organisations to set goals, measure performance and monitor progress to work towards improving quality of care. A well-functioning information management system thus contributes to transforming care [1]. Kash et al. [25] argue that technology increases absorptive capacity within organisations and thus is an important mechanism to facilitate transformation initiatives [25]. Macleod et al. [30] and Urtaran et al. [39] indicate that information management systems help integrate care [30, 39].
3.3.7 Co-occurrences analysis of mechanisms
A co-occurrences analysis (Additional file 2: Appendix S2) was prepared where the coherence within the different mechanisms was investigated. This analysis shows that the mechanism collaboration goes together to a reasonable extent with the mechanism’s leadership, interpersonal relations, and coordination (c-coefficient is between 0.07 and 0.15). This seems to imply that care transformation requires a collaborative effort among stakeholders. Transformational leadership, interpersonal relationships, using the deployment interdisciplinary teams, and coordination of care to promote transfer and collaboration contribute to achieving an improvement in care quality [13, 15, 25, 31].
3.4 Outcomes
Based on the coding, it is possible to identify the main outcomes pursued with transformation of care. These are respectively, improving quality of care and integration of care.
3.4.1 Outcome—improving quality of care
In 9 of the 19 articles studied, the item 'improving quality of care' was mentioned. In these studied articles, an important role was played by the mechanisms of coordination and collaboration in improving care processes. Information technology and transformational leadership were mentioned as important facilitators to achieve improvement in quality of care [13, 15].
3.4.2 Outcome—integration of care
In 11 of the 19 articles studied, the item 'integration of care' was mentioned.
Collaboration, coordination, and interpersonal relationships are important mechanisms in integrating care. Urtaran et al. [39] and Nystrom et al. [35] indicate that bottom-up interventions at the local level contribute to better coordination and enable integration rather than a focus on structural or managerial integration. Bottom-up initiatives lead to different professional roles to ensure better coordination between primary care and hospital care. Transformational leadership as a type is supportive and information technology should be facilitative in integrating care [35, 39].
4 Discussion
Based on the results and more specifically the definition of care transformation, we have seen that it involves collaboration at the system level and within and between organizations and takes place together with the mechanisms of leadership, interpersonal relations, and coordination. Figure 3 shows the most common codes in the perspective of Pawson and Tilly's theory [37].

Most frequently mentioned codes divided by context, mechanism and outcomes
From the results of this SLR, the researchers note that the term collaboration should receive more attention when defining the concept of care transformation. In none of the articles studied does the term collaboration appear in the definition of care transformation. This review shows that collaboration is an essential element in the definition of care transformation.
The central question is: “How is care transformation conceptually explained in the existing literature?” Based on the aim of the present study, the PICO(TS)-strategy was applied to formulate the research question and search strategy (Fig. 1) to gain insights into the concept of care transformation, the process of care transformation and changing the process. In this study, the population (P) comprises healthcare organisations, examined from a multilevel perspective, and the outcomes (O) are related to care transformation. The existing literature approaches the concept of care transformation from different perspectives, leading to different definitions. This lack of a single universally accepted definition is probably due to the fact that care transformation occurs at multiple levels and to the diverse research contexts in which it has been studied.
Care transformation is a broad concept that encompasses the reconfiguration and improvement of healthcare systems, processes, and practices to achieve better patient outcomes and experiences. Researchers have chosen to look at care transformation from different perspectives, such as the patient-centred perspective or the organisational perspective. These different perspectives result in differences in emphasis on specific aspects of the concept, leading to different definitions.
It is notable that in the publications reviewed, 15 out of 19 do not provide a stand-alone definition of care transformation. Instead, they present care transformation within the context of their research focus or framework.
To gain a clearer understanding of care transformation, it is important to explore the different perspectives and aspects associated with care transformation. By considering different dimensions, such as patient-centeredness, organisational change, process improvement and system-wide impact, a more comprehensive understanding of care transformation can be developed.
The second sub-question is about “what are the main contexts of care transformation?” Contexts identified in the literature review support the need for healthcare transformation. The changing environment, organisational conditions, resource availability and collaboration all contribute to addressing healthcare challenges and opportunities. Care transformation is a means of improving the overall quality, efficiency and patient experiences within healthcare systems and ensuring that these systems remain adaptive and adjust to the changing needs of individuals and populations. This review shows that integration and quality improvement are important outcomes of care transformation. None of the articles address the how question or are vague and not very concrete on this, apart from identifying possible high-level mechanisms.
A key question still is how care transformation can lead to the implementation of initiatives that measurably improve quality of care? Examination of the articles included shows that no position has yet been determined in this and this requires further research. To arrive at practical insights on how to change, Kotter's [28] theory, described in book "Leading Change", is relevant. In this book, Kotter describes concrete steps to deal effectively with change. Kotter highlights crucial actions, such as forming a change team, creating a vision and action plan, mobilising supporters, removing barriers, achieving quick successes, maintaining the rhythm of change, and embedding results in the organisational culture [28]. Future research should focus on whether these steps will lead to the desired care transformation and combining insights from science and practice into evidence-based guidelines for the health care sector.
What the review has shown, is that multi-level collaboration is an important mechanism for care transformation. However, care transformation requires more than just collaboration. It requires adapting the way care is delivered. Important tools contributing to this come from the domain of e-Health. From the literature, we know that e-Health technologies can create changes in the ecosystem [12]. The use of e-Health applications can lead to new work processes, restructuring of tasks and responsibilities. In addition, it can affect communication and collaboration at different levels within an organisation. This seems to make e-Health technologies a good fit with the aims and mechanisms of care transformation and warrant further research into how insights and technologies from the field of e-Health can be applied within the domain of care transformation.
Moreover, it seems relevant and useful to use institutional theory to learn how healthcare should deal with care transformation from an organisational perspective in relation to joint digital ecosystems [18]. Joint digital ecosystems refer to collaborative networks or platforms where multiple healthcare organisations and stakeholders come together to share information, coordinate care, and leverage digital technologies for transformative purposes as integrated care and improve quality of care.
Change processes need to interact with the underlying digital underpinning ecosystem. One of the directions for future research could therefore be to study the E-health Readiness of organisations, to assess how prepared healthcare organisations are to adequately deal with a changing organisational ecosystem [17], and how to improve that.
Some limitations can be identified in this research. First, care transformation is described in different ways in the literature and is a relatively new topic. Therefore, a broad search query was used, which followed in lower search effectiveness. However, as much has been published on this topic and it is becoming increasingly popular, it may be that, even with a broad search, we have still missed relevant studies. This review only included studies that looked at care transformation from a muli-level perspective. This was done to form a broad picture of care transformation. Not all perspectives (such as economic) were included in the selection, creating a certain focus or picture of care transformation that does not reflect all aspects.
A strength of this study is the high inter-rater reliability between the researchers, which is an indication of this study’s reliability. The strict application of inclusion and exclusion criteria and open, axial, and selective coding further contributed to increasing the reliability of the study.
Due to the exploratory nature of this study, a broad search was conducted. This made it possible to paint a comprehensive and multifaceted picture of what is currently known about care transformation. We have assessed the quality of the include studies using several measures. First a summary was prepared for all included studies. Next, the citation score of the first-named author of the article and the H-index and impact factor of the Journal in which it was published were assessed. The overview of the quality assessment was attached to the manuscript as supplementary material (Additional file 4: Appendix S4). The study used co-occurrence analysis to discover possible links and relationships between the terms used in the study. This analysis does not offer causal explanations but provides possible indications of links and relationships.
5 Conclusion
Global trends such as the ageing population, an increasing number of chronic diseases, a shrinking workforce, and an accelerating availability of technological innovations call on healthcare to rapidly adapt and adjust via healthcare transformations [26]. However, to date it is still largely unknown what contributes to the chances of success of such transitions.
The current literature review investigated key factors that contribute to successful care transformation. It is concluded that even though there is no universally accepted definition of care transformation, collaboration is seen as important factor for achieving key goals of transformation, such as better-quality care. Achieving care transformation requires mechanisms that combine contexts with the intended goals of care transformation.
Interdisciplinary collaboration, coordination regarding the transfer of care between healthcare professionals and healthcare institutions and transformational leadership are crucial mechanisms for driving healthcare transformation. Deploying the right mechanisms to transform healthcare leads outcomes such as integration of care and improved quality of care. Deploying the right mechanisms depends on the context and expected outcome of the final transformation.
6 Contribution to the literature
-
This systematic review showed that there is no clear definition of care transformation in the literature. Hence, the Context-Mechanism-Outcome (CMO) framework was introduced to identify important factors of care transformation.
-
This article identified that effective collaboration among health care providers, supported by transformational leadership, strong interpersonal relationships, and coordination from multiple perspectives, play an important role in facilitating care transformation.
-
This knowledge can guide both scientists and healthcare organizations in successful care transformation and the implementation of technology.
Data availability
Not applicable.
Abbreviations
- PRISMA:
-
Prevention recovery information system for monitoring analysis
- CMO:
-
Context-mechanism-outcome
- DOI:
-
Digital object identifier
- SLR:
-
Systematic literature review
References
Aggarwal M, Williams A. Tinkering at the margins: evaluating the pace and direction of primary care reform in Ontario, Canada. BMC Fam Pract. 2019. https://doi.org/10.1186/s12875-019-1014-8.
Alryalat S, Malkawi L, Momani S. Comparing bibliometric analysis using Pubmed, Scopus an Web of Sciences databases. J Vis Exp. 2019. https://doi.org/10.3791/58494.
Barello S, Palamenghi L, Graffigna G. Burnout and somatic symptoms among frontline healthcare professionals at the peak fo the Italian Covid-19 Pandemic. Psychiatry Res. 2020;290:113129.
Beard J, Officer A, Cassels A. World report on Ageing and Health - Chapter 3: Health in older age. 2015. https://www.who.int/publications/i/item/9789241565042. Accessed on 8 July 2022
Best A, Berland A, Herbert C, Bitz J, van Dijk M, Krause C, Millar J. Using systems thinking to support clinical system transformation. J Health Organ Manag. 2016;30(3):302–23.
Bolmer B, Taverne M, Scherer M. Exploring the added value of blockchain technology for the healthcare domain: lessons learned from two cases by a universital hospital. Cornell University. 2019.
Bussu S, Marshall M. (Dis)Integrated Care? Lessons from East London. Int J Integr Care. 2020;20:2.
Chrysanthaki T, Hendy J, Barlow J. Stimulating whole system redesign: lessons from an organizational analysis of the Whole System Demonstrator programme. J Health Serv Res Policy. 2013;18:47–55.
Coles E, Anderson J, Maxwell M, Harris F, Gray N, Milner G, MacGillivray S. The influence of contextual factors on healthcare quality improvement initiatives: a realist review. Syst Rev. 2020;9:1–22.
Corbett S, Courtiol A, Lummaa V, Moorad J, Stearns S. The transition to modernity and cronic disease: Mismatch and natural selection. Nat Rev Genet. 2018;19(7):419–30.
Embuldeniya G, Gutberg J, Sibbald S, Wodchis W. The beginning of health system transformation: How Ontario Health Teams are implementing change in the context of uncertainty. Health Policy. 2021;125(12):1543–9.
Eysenbach G. What is e-health? J Med Internet Res. 2001;3(2):20.
Farmanova E, Baker G, Cohen D. Combining integration of care and a population health approach: a scoping review of redesign strategies and interventions and their impact. Int J Integr Care. 2019. https://doi.org/10.5334/ijic.4197.
Fitzgerald K, Biddle L. Creating the conditions for change: an NHS perspective. J Health Organ Manag. 2020;34(3):345–61.
Greenhalgh T, Macfarlane F, Barton-Sweeney C, Woodard F. “If We Build It, Will It Stay?” A case study of the sustainability of whole-system change in London. Milbank Q. 2012;90(3):516–47.
Halsall T, Manion I, Mathias S, Robeson P, Benlamri M, Helfrich W, Henderson J. Frayme: Building the structure to support the International spread of integrated youth services. Early Interv Psychiatry. 2020;14(4):495–502.
Hanelt A, Bohnsack R, Marz D, Marante C. A systematic review of the literature on digital transformation: insights and implications for strategy and organizational change. J Manag Stud. 2020. https://doi.org/10.1111/joms.12639.
Hargrave T, van Ven A. A collective action model of institutional innovation. Acad Manag Rev. 2006;31(4):864.
Head B, Alford J. Wicked problems: implications for public policy and management. Adm Soc. 2015;47(6):711–39.
Hewison A, Hodges E, Balasubramanian S, Swani T. System transformation in palliative and end of life care: developing a model fo excellence. J Health Organ Manag. 2021;35(8):1008–24.
Holton J. Social movements thinking for managing change in large-scale systems. J Organ Chang Manag. 2020;33(5):697–714.
Hunter D, Erskine J, Small A, Mc Govern T, Hicks C, Whitty P, Lugsden E. Doing transformational change in english NHS in the context of “big bang” redisorganisation findings from the north east transformation system. J Health Organ Manag. 2015;29(1):10–24.
Hussey A, Sibbald S, Ferrone M, Hergott A, McKelvie R, Faulds C, Licskai C. Confronting complexity and supporting transfromation through health system mapping: a case study. BMC Health Serv Res. 2021. https://doi.org/10.1186/s12913-021-07168-8.
Hutchinson K. An exploration of the integration of health ans social care within Scotland. J Integr Care. 2015;23(3):129–42.
Kash B, Spaulding A, Gamm L, Johnson C. Leadership, culture and organizational technologies as absorptive capacity for innovation and transformation in the healthcare sector: a framework for research. Change Management. 2014;13(1):1–13.
Keijser W, van Montfort G. Zorgtransformatie: trendy innoveren of nieuw vertrekpunt? Skipr. 2020. https://doi.org/10.1007/s12654-020-0220-2.
Khan S, Vandermorris A, Shepherd J, Begun J, Lanham H, Uhl-Bien M, Berta W. Embracing uncertainty, managing complexity: applying complexity thinking principles to transformation efforts in healthcare systems. BMC Health Serv Res. 2018. https://doi.org/10.1186/s12913-018-2994-0.
Kotter J. Leading change. Boston: Harvard Business School Press; 2012.
Kraus S, Schiavone F, Pluzhnikova A, Invernizzi A. Digital Transformation in Healthcare; Analyzing the current state of research in health care and other industries. J Bus Res. 2021;123:557–67.
MacLeod M, Hanlon N, Reay T, Snadden D, Ulrich C. Partnering for change: how a health authority, physicians, and communities work together to transform primary healthcare services. J Health Organ Manag. 2020;34(3):255–72.
Maniatopoulos G, Hunter D, Erskine J, Hudson B. Large-scale health system transformation in the United Kingdom: implementing the new care models in the NHS. J Health Organ Manag. 2020;34(3):325–44.
McHugh M. Interrater_reliability_The_Kappa_Static. 2012. https://pubmed.ncbi.nlm.nih.gov/23092060. Accessed on 13 july 2022
Meeteren NN, Mecgchelen P. Kennis en Innovatieagenda 2020–2023 (Maatschappelijk thema Gezondheid en Zorg. Den Haag: Health Holland; 2019.
Nalau J, Handmer J. When is transformation a viable policy alternative? Environ Sci Policy. 2015;54:349–56.
Nyström M, Strehlenert H, Hansson J, Hasson H. Strategies to facilitate implementation and sustainability of large system transformations: a case study of a national program for improving quality of care for eldery people. BMC Health Serv Res. 2014. https://doi.org/10.1186/1472-6963-14-401.
Page M, McKenzie J, Bossuyt P, Boutron I, Hoffman T, Mulrow C, McDonald. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021. https://doi.org/10.1186/s13643-021-01626-4.
Pawson R, Tilly N. Realistic evaluation. London: Sage Publication Ltd; 1997.
United Nations. Resolution 70/1. Transforming our world: the 2030 Agenda for Sustainable Development Transforming our world: the 2030 Agenda for Sustainable Development Preamble. 2015. https://sdg.un.org/2030agenda. Accessed on 2 November 2022
Urtaran-Laresgoiti M, Alvarez-Rosete A, Nuño-Solinís R. A system-wide transformation towards integrated care in de Basque Country: a realist evaluation. Int J Care Coord. 2018;21(3):98–108.
Wolfswinkel J, Furtmueller E, Wilderom C. Using grounded theory as a method for rigorously reviewing literature. Eur J Inf Syst. 2013;22–1:45–55.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
GAGG and WAK initiated the study. GAGG, SFHH, MEMO included the studies and analyzed the data. GAGG, MEMO, NBJ and SMK were a major contributor to writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Additional file 1: Appendix S1.
Document analyses of Alas.ti.
Additional file 2: Appendix S2.
Co Occurrence analyses of Atlas.ti.
Additional file 3: Appendix S3.
Search strings.
Additional file 4: Appendix S4.
Quality assessment included articles.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Garritsen, G.A.G., den Ouden, M.E.M., Keijser, W.A. et al. Care transformation defined by conditions, mechanisms, and outcomes: a systematic literature review. Discov Health Systems 3, 11 (2024). https://doi.org/10.1007/s44250-024-00073-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44250-024-00073-x