
Abstract
Diagnostic and decision-making processes in the 2019 Coronavirus treatment have combined new standards using patient chest images, clinical and laboratory data. This work presents a systematic review aimed at studying the Artificial Intelligence (AI) approaches to the patients’ diagnosis or evolution with Coronavirus 2019. Five electronic databases were searched, from December 2019 to October 2020, considering the beginning of the pandemic when there was no vaccine influencing the exploration of Artificial Intelligence-based techniques. The first search collected 839 papers. Next, the abstracts were reviewed, and 138 remained after the inclusion/exclusion criteria was performed. After thorough reading and review by a second group of reviewers, 64 met the study objectives. These papers were carefully analyzed to identify the AI techniques used to interpret the images, clinical and laboratory data, considering a distribution regarding two variables: (i) diagnosis or outcome and (ii) the type of data: clinical, laboratory, or imaging (chest computed tomography, chest X-ray, or ultrasound). The data type most used was chest CT scans, followed by chest X-ray. The chest CT scan was the only data type that was used for diagnosis, outcome, or both. A few works combine Clinical and Laboratory data, and the most used laboratory tests were C-reactive protein. AI techniques have been increasingly explored in medical image annotation to overcome the need for specialized manual work. In this context, 25 machine learning (ML) techniques with a highest frequency of usage were identified, ranging from the most classic ones, such as Logistic Regression, to the most current ones, such as those that explore Deep Learning. Most imaging works explored convolutional neural networks (CNN), such as VGG and Resnet. Then transfer learning which stands out among the techniques related to deep learning has the second highest frequency of use. In general, classification tasks adopted two or three datasets. COVID-19 related data is present in all papers, while pneumonia is the most common non-COVID-19 class among them.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
1 Introduction
In December 2019, China announced the emergence of a new coronavirus infection in humans in Wuhan (China). The disease spread rapidly worldwide and was declared as a pandemic with significant morbidity and mortality by the World Health Organization (WHO) [1, 2] in March 2020. A ribonucleic acid (RNA) virus named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes coronavirus disease 2019 (COVID-19). The current pandemic succeeds the significant occurrences of severe acute respiratory syndrome (SARS, caused by SARS-CoV-1 virus) in 2002–2004 and middle east respiratory syndrome (MERS, caused by MERS-COV virus) in 2012 [3]. According to WHO,Footnote 1 until February, 2023, morbidity had reached more than 757 million cases and almost 6.850 million deaths, characterizing itself as a principal public health problem to be tackled with the help of applied science.
After the first day of contamination, common clinical manifestations such as fever, cough, fatigue, sore throat, headache and shortness of breath may appear. There is high transmissibility of the virus. Droplets, aerosols or contact with contaminated surfaces can spread the infection. In addition, there is a possibility of transmission by asymptomatic people or even before the onset of symptoms. Some groups of patients are more likely to progress to pneumonia, respiratory failure and death. Treatment is essentially supportive for symptomatic patients [4].
According to the World Health Organization, of the more than 100 vaccines proposed for COVID-19, 10 candidate vaccines had reached the human trial phase (clinical trials), as presented in the World Report of Lacet on June 6, 2020. Various technologies and compounds are in use to produce the vaccines, such as a virus (Inactivated and Weakened), viral vector (replicating and non-replicating), nucleic acid (DNA (deoxyribonucleic acid) and RNA) and protein-based vaccine (protein subunit and virus-like particles) [5].
In addition, as a way to control the spread of the virus, personal and environmental restrictions have been implemented in several countries, such as the use of masks, social distancing, closing of commercial establishments, schools, and universities [6]. The first impacts generated many concerns due to the high rate of contamination with a high number of deaths. However, the emergence of new strains and complications after the disease are still a matter of concern. This scenario may continue until widespread adoption of the COVID-19 vaccine.
The COVID-19 pandemic has mobilized governments, universities, and research centers around the world. However, now the scenario is still worrying due to the high rate of virus variants and because the disease complications are related to increasing long term sequelae. This scenario may continue until the full adoption of the vaccine against COVID-19.
Thus, this COVID-19 scenario has brought together specialists and researchers from different areas in initiatives that can help combat the disease. Above all, artificial intelligence (AI) has directed efforts to develop solutions to the crisis. In different contexts, similar resources have been used such as diagnosis and treatment, prediction of the disease spreading, development of new drugs and vaccines, management of hospital beds and supplies, identification of crowds of people, in addition to economic analysis due to social isolation and fighting fake news [7].
In the efforts against COVID-19, AI can play an essential role in the diagnosis and outcome of the disease. When addressing AI in this context, machine learning (ML) methods stand out and have been applied to classify different medical image modalities, using a variety of attributes, for several diseases and tools, such as computer-aided diagnosis/detection and radiomics [8,9,10]. The development of a ML method involves creating a training function for a dataset, making use of a logical inference mechanism [11]. Indeed, such an approach can be used in different ways in the analysis of medical images or clinical data of the patient, for example, in the area of radiology and diagnostic imaging, they have been mainly applied in computer-aided diagnosis/detection, content-based image retrieval and radiomics/radiogenomics [10, 11]. The trained algorithms can make predictions with adequate speed and accuracy. The purpose is to identify non-visible patterns, indications, among other events, with the probability of the disease’s progression or complication [12].
This systematic review aimed to study the approaches of AI applied to the diagnosis or outcome of patients with COVID-19 published until the beginning of the pandemic when there was no vaccine. This period aimed at identifying patterns that mapped relationships between clinical data and images with diagnoses and outcomes, with a high volume of works involving diagnosis. Furthermore, AI classification methodologies and models were identified.
The Covid-19 epidemic and the spread of AI/ML have increased studies on the exploration of AI/ML techniques applied to various dimensions of the epidemic: drugs and vaccines development [13], models of disease advance [14], use of images [15] and clinical data [16] for disease diagnosis and outcome.
In this context, some literature reviews were carried out and identified the use of AI/ML techniques to model, simulate and project COVID-19. The review described by Dogan et al. [17] pointed out that the convolutional neural network (CNN) was the most used network model to diagnose COVID-19 from X-ray exams. ResNet was the most used network for classification. Logistic regression was the most used model for prediction purposes. However, this work does not accurately determine the time window in which the works were published. Abd-Alrazaq et al. [18] carried out a review considering works published from Dec 2019 to April 2020. The limitation of this paper is that as the pandemic was at the beginning, the review considered many preprints that have not yet been evaluated by experts. This paper identified works carried out with clinical, laboratory and image databases, in which the most used model was CNN, followed by support vector machines (SVM) and recurrent neural networks (RNN). In the review developed by Islam et al. [19], 49 studies were identified. They explored AI techniques to diagnose, analyze and predict risks and project the progress of the epidemic, among other less frequent ones. Among these works, 10 used images to mostly apply the CNN model. Their work presented some still incipient papers which analyzed the possibilities of AI in the identification, dissemination, and control of the disease via vaccination.
Our proposal complements some of these works, which considered reviews carried out at the beginning of the pandemic, when there was not much knowledge about the use of AI/ML techniques with the COVID-19. Abd-Alrazaq et al. [18] considered works until April 2020; the paper by Goel [14] was published in July 2020 and Islam et al. [19], whose research was up to August 2020, considered early work on the use of AI techniques on COVID-19 data.
The main contributions of this systematic review are: (i) identification of studies that explored AI techniques considering imaging, laboratory, and clinical data to generate diagnoses or outcomes related to COVID-19 when the vaccine had not yet been distributed; (ii) present results, with several data crossings, carried out by a large team that was able to perform three rounds of reviews to identify the most used AI and ML techniques in the context of the pandemic; (iii) describes all datasets associated with each work; (iv) an analysis of the adoption of AI methods related to the attributes of data used in the studies; and (v) a discussion of the most used AI/ML techniques associated with each data type.
This review is organized as follows: Sect. 2 presents the adopted methodology considering PRISMA [20] criteria, describing the search strings, databases, and studies selection strategies. It describes the collection phase, presents a flowchart that summarizes results from the application of PRISMA steps, a summary of an analysis of the selected studies, a Sankey diagram with the distribution of papers concerning their data types and purpose, and a discussion about the terms that appeared in the studies. In Sect. 3, we analyze the major AI approaches adopted in the studies relating them to the data type: images, laboratory and clinical. Section 4 discusses the results, presenting the frequency of the machine learning techniques used in the papers. Section 5 describes some limitations of this study. Finally, Sect. 6 concludes, stressing some perceptions about the adoption of AI techniques and some challengers.
2 Methodology
A systematic literature review (SLR) identifies, analyses, and interprets available evidence related to specific research. The methodology of this systematic review was conducted according to preferred reporting items for systematic reviews and meta-analyses (PRISMA) criteria [20]. The process defined an eligibility criterion that identifies the review goals, the inclusion, and the exclusion criteria applied. This section also identifies the databases used, the search strategy, the selection steps, and the study characteristics that show the papers selected in this SLR.
2.1 Eligibility Criteria
This systematic review included: (1) studies regarding the use of the AI approach for the diagnosis or outcome of patients with COVID-19, either by imaging (chest X-Ray, chest Computed Tomography (CT) or ultrasound) or clinical/laboratory data; (2) studies that validate or evaluate methodologies and classification models for the diagnosis or outcome of patients with COVID-19. In addition, as inclusion criteria, studies published from 2019 to October 2020, in English, written in scientific format and available in full format, were established.
The following exclusion criteria were used: (1) studies related to diseases other than COVID-19; (2) studies that consider other types of information that are not images and clinical data, such as meteorological and regional data; (3) studies with a different focus of diagnosis and outcome and; (4) reviews, letters, conference abstracts, book chapters or studies that described only the application of the classification model, without its evaluation.
In addition, significant criteria regarding the application of classification methodologies and performance analysis were considered as exclusion criteria: (5) studies that did not satisfactorily describe the adopted AI method or data treatments; (6) studies that did not present sufficient description regarding the database and; (7) studies that describe results considering an unbalanced database.
2.2 Databases and Search Strategy
The works were identified through an individual search strategy for each of the following electronic databases: ACM Digital Library, IEEE Xplore, PubMed, SCOPUS and Springer. Reference lists of selected studies were manually analyzed to search for potentially relevant studies that could have been missed in electronic searches in the databases.
For the selection and analysis, the collection of information was carried out according to keywords and their synonyms, which were used to elaborate a search string: (i) artificial intelligence; (ii) machine learning; (iii) deep learning; (iv) COVID-19; (v) 2019-nCoV; (vi) coronavirus; (vii) coronavirus infections and; (viii) new coronavirus. The selection of the most relevant articles, in accordance with the objectives of this work, from the selected keywords, Boolean operators were used to formulate the search expression, as shown in Table 1. It is worth mentioning that the search string was used for the Title/Summary fields to specify and limit the studies found for the analysis.
Duplicate references were removed using Mendeley® software.Footnote 2 All searches in the electronic databases occurred on October 23, 2020. The collection process searched for documents from the beginning of the pandemic.
2.3 Selection Steps
The selection of studies was carried out in two phases. In Phase 1, all studies identified in the electronic databases were divided among 6 researchers that analyzed the titles and abstracts independently and selected those that seemed to meet the inclusion criteria. In Phase 2, these selected studies were divided among the same researchers proceeding with the complete reading independently and excluding those who did not meet the inclusion criteria. Any disagreements in the first or second phase were resolved by discussion and consensus with all researchers. In some cases, it was necessary to involve a third researcher evaluating the article to make a final decision.
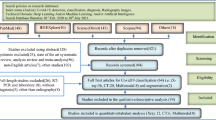
The first search collected 839 papers. Next, the abstracts were reviewed, and 138 remained after performing the inclusion/exclusion criteria. After thorough reading and review by a second group of reviewers, 64 met the study objectives. Figure 1 presents a flowchart with the steps and results of the PRISMA application [20].

Flowchart of the study search and selection process (adapted from preferred reporting items for systematic reviews and meta-analyses—PRISMA) [20])
2.4 Study Characteristics
This section will briefly evaluate the papers that were assessed. A summary of the studies included in this systematic literature review is presented in Table 2. The Ref. column indicates the bibliographic reference, the data type column describes the type of data used in the research, the AI method column highlights the base methods used and the performance column points out the results achieved [considering the adopted metric: accuracy (A), area under the ROC curve (AUC), precision (P), sensibility(S)]. The third column indicates whether the work context was focused on diagnosis (D) or outcome (O), and finally the last column indicates the databases used in the references.
Some works pointed out in Table 2 as AI Method, used a generic nomenclature of deep learning (DL) algorithms, such as recurrent neural networks (RNN) and convolution neural networks (CNN) as indicated in references [21,22,23,24,25,26,27,28]. CNNs is the generic name of the DL-based algorithm that introduced the convolution process in the neural network area [85], inspired by the animal visual cortex, which is most applied to in image analysis. CNNs learn to extract features from data while learning to correlate these features with the labels to minimize the losses between model and label output.
On the other hand, RNNs were created as a class of artificial neural networks that allow connections between neurons of the same layer or between non-adjacent layers generating links that form oriented or non-oriented graphs over a temporal sequence. More recently, model-based DL architectures have been inserted into this class of algorithms that aim to extract information from data that are related to longer temporal chains of information [86].
Other works used models based on hybrid architectures, combining more than one architecture of deep neural networks, such as CNNRNN (combination of CNN and RNN) or CNNLSTM (combination of CNN and LSTM (long-short time memory) indicated in reference [51]. The papers [26, 28] are essential to highlight that used eleven and five, respectively, different types of CNN-architectures such as VGG (classical CNN), residual neural network (Resnet), Inception, etc., to build a framework involving these models. As can be seen in Table 2, most of the papers aim at diagnosis because the first test for COVID-19 diagnosis was released in February 2020, distributed by the Centers for Disease Control and Prevention. However, many countries with limited resources prevented testing all patients with suspected COVID-19, which stimulated the search for alternative methods for diagnosis, either with imaging or laboratory tests.Footnote 3 Thus, only about 20% of the studies involved the evaluation of the outcome.
The Sankey diagram represented in Fig. 2 presents the frequency distribution of the papers concerning the data types (clinical, laboratory, chest X-ray, chest CT, ultrasound) and their purpose (diagnosis, outcome and diagnosis/outcome). The majority of the selected papers reached the diagnosis purpose (51 papers) while 12 worked on the Outcome problem and only one considered both situations.

Distribution of papers concerning their data types and purpose
The most used data type was chest CT scans, 29 papers, followed by chest X-Ray in 20 works and then a combination of Clinical and Laboratory data in six articles. Two studies applied Clinical or Laboratory data. The combination of Clinical, Laboratory and chest CT scans data are found in two works, and the combination of chest CT and chest X-Ray data are also found in another two works, respectively. Only one work used Ultrasound data.
Another point to be highlighted in the Fig. 2 is that while most of the data types were used to approach one or two kinds of purpose (diagnosis, outcome or both), only the chest CT scan was used on all of them. Fig. 2, when obtaining the relationship between the types of data and purposes, two thicker lines are identified, the data from CT and X-ray images, which led to the diagnosis (70.31%). Although CT is more accurate, X-ray is widely used due to its avail- ability and ease of access, especially in bedridden patients. In the beginning of COVID-19, the disease was considered to be strongly related to lung problems.
Figure 3 presents a word cloud generated with several AI-based techniques and algorithms used in the analyzed selected studies.

Word cloud generated by AI terms that appeared in the selected studies
Words written in larger size indicate their expressiveness in relation to their distribution of frequency in the selected studies. Thus, we can conclude that most of the works involve image examinations because CNN [21,22,23,24,25,26,27,28, 51] and Resnet [26, 28, 33, 53, 54, 62, 65, 66, 76, 78] (which are associated with CNN) are the largest size words. In following, the largest words are transfer learning [55, 62, 66, 69, 70, 76, 77] and VGG [26, 28, 40, 55, 57, 70, 72]. There is an emphasis on the use of Transfer Learning because many researchers have had to reduce the time to produce results for COVID-19 diagnosis (reducing training time and the amount of labeled data needed for training) and VGG was another highlighted technique mainly for being a CNN used in image classification.
3 Discussions
3.1 Images Papers
The Fig. 2 shows all selected articles divided in groups by their data where 52 are based only on different types of chest images. Among all, 20 studies examined chest X-Ray scans [21, 23, 25,26,27, 29, 37, 47, 55, 57, 58, 66, 67, 70,71,72, 76, 77, 79, 82], 29 studies focused in chest CT [22, 32, 33, 35, 39,40,41,42,43,44, 46, 48, 50, 53, 54, 56, 59, 60, 62,63,64,65, 69, 73,74,75, 78, 81, 84], two studies considered both chest X-ray and chest CT [24, 34] and one study focused in ultrasound [36].
In order to compare the different data preprocessing techniques, present in the articles, we named three main characteristics: resize is related to the scale (in px) of the input images; synthetic means the use of GAN’s to create synthetic data and; Increase indicates the image number increase by data-augmentation techniques, which consists of making small changes to the original images, such as color and brightness changes, shift, flip and image rotations, as well as cropping. Table 3 relates the articles to their respective data preprocessing characteristics. Among the 52 selected articles, 45 perform classification tasks with the number of output classes ranging from two to nine. Most of the articles adopted two or three classes, as one can see in Fig. 4, which shows the histogram of the distribution of frequency of articles versus number of output classes. COVID-19 is the only class shared by the 45 articles, Pneumonia and Healthy are the most common Non-COVID-19 classes among them.

Frequency of articles versus number of output classes evaluated
However, some authors consider other illnesses, like bacterial pneumonia [26], H1N1 [62], influenza [65] and tuberculosis [82], as well as some authors consider illness stages, as in [27] and [66]. [64] evaluate the proposed model by distinguishing two classes (COVID-19 and non-COVID-19) and then three classes (COVID-19, common pneumonia, and no pneumonia). So, this article is considered in the two respective columns in Fig. 4.
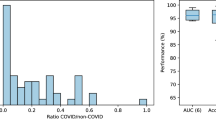
Tables 4 and 5 present the number of COVID-19 and Non-COVID-19 images for each of the 45 articles. These numbers are the articles’ original data quantities before data preprocessing, which means that the data imbalance present in some rows of Tables 4 and 5 do not represent the number of images used to train the proposed models. For instance, [81] does not employ non-COVID- 19 images, as shown in Table 5, because the authors use chest CT images for the assessment of the illness severity in COVID-19 infected patients. The non-COVID-19 images refer to healthy, pneumonia or any other illness or class considered by the different authors. It is important to consider that [34] and [24] employ both chest X-ray and CT images on their work. So, they are mentioned in both Tables 4 and 5.
Through the 52 selected articles, five achieve segmentation tasks, one performs predictions of hospitalization stay and one predicts the disease severity score. Reference [63] presents a net architecture that executes lung segmentation and illness classification. The segmentation dataset consists of 60 3D CT lung scans with manual delineations of the lung anatomy. The classification dataset included 150 3D volumetric chest CT exams of COVID-19, Community Acquired Pneumonia and non-pneumonia patients. However, the authors do not specify each class ‘selected slice number for training/validation and testing.
In order to propose COVID-19 segmentation models, [35, 74] employ datasets that consist of only infected patients chest CT scans, but they do not specify the number of images per CT scan. Reference [60] include non-infected CT scans to guarantee that the proposed model deals with non-infected slices well. Reference [59] employ COVID- 19 infected patients and patients with different medical histories other than COVID-19 to perform lung segmentation and quantification of lung opacities in chest CT scans of COVID-19 patients.
Yu et al. [81] include 31 patients with 72 lesion segments for predicting hospital stay in infected patients using chest CT scans. But it is not clear if the number of lesion segments is the number of images or slices.
An approach that uses DL techniques for the analysis of lung ultrasonography images is proposed by [36]. The authors propose a model that employs 277 lung ultrasound videos from 35 patients, corresponding to 58,924 frames. This model is a deep network that simultaneously predicts the disease severity score associated to a input frame and provides localization of pathological artefacts in a weakly-supervised way.
A relevant point about works [53, 67, 84], despite having included images as part of the data used in the research, unlike the other works, they did not use CNN to extract information from the images. Instead, the authors of these works used specific filters to extract the spatial distribution of signal intensities and pixel interrelationships [87]. The radiomics, which quantifies textural in formation, is a method that extracts, in general, a large number of features from medical images using data-characterization algorithms. [84] also used radiomics method to collect 34 statistical texture features of COVID- 19 and general pneumonia ROI images, aiming to differentiate COVID-19. The authors used ensemble of bagged trees and compared their results with other ML algorithms (K-nearest neighbor (kNN), decision tree, support vector machine (SVM), logist regression (LR)).
Four different algorithms were evaluated (decision tree, kNN, Naïve Bayes, SVM) by [46] and ensemble-based algorithms involved the tree-based algorithms: AdaBoost, RUSBoost, LogitBoost, GentleBoost and bag. In this work, the features of the images were also not extracted by filters or CNNs algorithms. The radiological features were extracted by radiologists during the visual inspection process.
In the paper by [56] the lung volume, lesion volume, nonlesion lung volume (lung volume—lesion volume) and the fraction of nonlesion lung volume were quantified by U-Nets. In addition, models based on Random Forest (RF) and LR were developed to classify and assess disease severity and predict the length of ICU stay, the duration of oxygen inhalation, hospitalization, and patient prognosis using clinical data.
In turn, the paper by [73] used several CNN architectures (VGG16, InceptionV3, ResNet50, DenseNet121 and DenseNet201) keeping the original convolutional parts as in the standard models and changed the fully connected parts of the models, fixed as tree fully connected layers to evaluate the diagnosis of COVID-19 patients. The individual results of these models were merged via a majority voting approach.
3.2 Clinical and Laboratorial Papers
Of the papers selected in this review, ten works address clinical data, and ten have laboratory data. The patients’ demographic data, symptoms and history of diseases were considered clinical data. Figure 2 shows the distribution of articles regarding two variables: (i) diagnosis or outcome and (ii) the type of data: clinical, laboratory or imaging data (chest CT, chest X-ray or ultrasound). In the clinical data, there were one paper discussing diagnosis [45] and one concerning outcome [30]. In the laboratory data, there were only one work for the diagnosis [51] and another for outcome [80]. One paper that bring together clinical and laboratory data deal with diagnosis [68] and four with outcomes [31, 38, 49, 61, 83].
Figure 5 presents the clinical data word cloud. Age is included in 90% of the works [29,30,31, 38, 45, 49, 52, 61, 68]. Gender in 60% [31, 38, 49, 52, 61, 68]and cough [29, 38, 68], fever [31, 38, 68], diabetes [31, 49, 52], diarrhea [29, 31, 38], cardiovascular diseases [31, 49, 52] and pulmonary diseases [31, 38, 52] in 30%. Two works corresponding 20% of the clinical data papers mentioned smoking and kidney diseases [31, 52], oxygen saturation [29, 61] and myalgia symptoms [31, 38]. The other data are used only in one work.

Clinical data word cloud
The most used laboratory tests were C-reactive protein [29, 31, 38, 49, 51, 52, 61, 83] and white blood cells [29, 49, 52, 68, 80] with means respectively 80% and 50%. Then the D-Dimer exam with three articles (30%) [38, 49, 80]. The lactate dehydrogenase [31, 83], pro-calcitonin [38, 52] and urea [44, 73] exams had 20% of the articles (two of ten). Hemogram was used in only one work [51]. Figure 6 presents the laboratory word cloud.

Laboratorial data word cloud
We observed that the works [30, 38, 45, 51, 61, 68] did not mention any kind of variable selection technique. Whereas the works [29, 52, 80, 83] adopted different strategies to identify more promising attributes among the variables that compose the collected dataset: the minimum redundancy maximum correlation algorithm [88], least absolute shrinkage and selection operator algorithm [89], Spearman’s correlation and chi-square test or Fisher exact test [90], Principal Component Analysis [91]. The papers [31, 49] used tree-based algorithms to select the most important attributes and in the case of paper [31], it adopted these selected attributes in other classification algorithms.
3.3 Clinical, Laboratorial and Images Papers
Of the 64 selected papers, only two addressed clinical, laboratory and imaging data [29, 52]. They were related to the outcome, with data on age, pro-reactive protein, white blood series, and chest CT. [52] use U-Net and data of oxygen saturation, surgeries historical, gasometry and electrolytes, and pro-calcitonin. The different clinical data of [29] are gender, chest pain, cough, diarrhea, and laboratory data are aminotransferase and myocardial enzymes.
Since AlexNet’s publication in 2012, CNN have become ubiquitous in the world of Computer Vision [92]. Resnet [93], CNN, VGG, U-Net, and EfficientNet [94] are architectures DL and use the convolutional process to extract information from the images [95] in 56% of the papers of this study.
4 Results
This Systematic review identified at first 839 papers but 24% were eligible and in the final selection there were 64 papers that represent 8% of the total papers found. The major of the papers (79.7%) has the purpose of Diagnosis, and only 12 papers (18.8%) address Outcome and only one (1.5%) both.
The ML techniques used by papers selected in this systematic review is summarized in Table 6. The Fig. 7 presented the machine learning techniques comparative survey, that we can highlight the following techniques: Resnet (15,6%), CNN (14,1%), VGG (10,9%), LR (9,4%), U-Net (9,4%), DenseNet (6,3%), and EfficientNet (6,3%). Since AlexNet’s publication in 2012, CNN have become ubiquitous in the world of Computer Vision [92]. Resnet, CNN, VGG, U-Net and EfficientNet are architectures DL and use the convolutional process to extract information from the images [95] in 56% of the papers of this study.

ML techniques in COVID-19
Very deep convolutional networks (VGG) is a family of architecture based on pattern recognition models. Developed as a deep neural network, it is one of the most popular image recognition architectures. The number of convolutional layers with VGG-16 or VGG-19 are 16 and 19, respectively. They are based on convolution and pooling operations along the layers, finishing with fully connected layers. The VGG-16 is composed of 13 convolutional layers, and VGG-19 has 16 convolution layers, both having three fully connected layers at the end. Specifically, the VGG architecture has increased the convolutional layers and uses a too-small filter (3x3 with a stride of 1), following the revolution caused by AlexNet with the introduction of ReLu (activation function), which won the ImageNet 2012 contest.
The “fully convolutional network” U-Net [96] have initially been developed for biomedical image segmentation at the Department of Computer Science of the University of Freiburg. The U-shape of this architecture consists of a sequence of convolutional contracting layers (the spatial information is reduced while feature information is increased) followed by another sequence in symmetric opposite with expansive character (the feature and spatial information are combined through a sequence of up-convolutions), which gives it a U-shaped architecture. The U-shape of this architecture consists of a sequence of convolutional contracting layers (the spatial information is reduced while feature information is increased). Another series of layers, which is almost symmetrical concerning the first sequence, has an expansive character (the feature and spatial information are combined through a sequence of up-convolutions), which gives it a U-shaped design. Thus, without exception, all DL networks used in image data are therefore used in work with image data, either for classification of these images for diagnosis or the outcome or semantic segmentation, which aims to identify regions affected by COVID-19 in lung images.
Only 7,8% of the papers use more than one ML techniques: paper [26] uses Resnet, CNN, VGG and DenseNet; (ii) paper [28] uses Resnet, CNN and VGG. The works [21, 24] and [51] uses CNN and LSTM.
Table 7 presents a summary of the data type and purpose (diagnosis or outcome) of the ML methods.
Logistic regression (LR) is a statistical model that uses a logistic function to model a binary dependent variable that has two levels. In general, LR and other algorithms such as SVM [97] and multi-layer perceptron (MLP)[98], decision tree-based algorithms [99] and XGboost [100]) were applied to structured data.
LR was used in 6 papers that correspond of 9% of the total, and only one (1.5%) is CT Image, other is only laboratory data, 3 (5%) are clinical and laboratory data, and 1 (1.5%) is clinical, laboratory and CT image. SVM was used in 2 works (3%), with Clinical data and other with clinical, laboratory and CT image data. Moreover, as can be seen, deep learning algorithms involving architectures for images are the most frequent.
Figure 8 shows an overview of the data type and the seven most used ML techniques (> 5%) according to Fig. 7: Resnet, CNN, VGG, LR, U-Net, DenseNet, and EfficientNet. We can conclude that CNN and VGG are the most applied techniques in X-ray (9,4%) and Resnet in CT (9,4%) image data. The CT is also used in U-Net (7,8%) and the X-ray in Resnet (6,3%). LR is the most used technique of structure data.

Data Types and ML techniques most used in COVID-19
All works using Resnet, CNN, VGG and EfficientNet addressed to diagnosis, only one work of U-Net and other of DenseNet have the purpose of outcome. The LR was used in 6 papers, and only one treat Diagnosis with clinical and laboratory data, all the others 5 are about outcome (1 is Image CT data, 2 are clinical and laboratory data, 1 is clinical, laboratory and image CT data).
5 Limitations
This review presents some limitations related to the selected keywords that adopted general terms, not considering specific names of IA/ML techniques. Research using AI/ML is increasing relentlessly, particularly COVID-19 context. So, a specific time was adopted, considering the period before the dissemination of vaccines, in which there was an intense search for patterns that would help in the diagnosis and outcome of the disease. Only papers with AI/ML approaches for the diagnosis or outcome of patients with COVID-19 were considered. Maybe some relevant studies were lost, but the search focused on efficient AI/ML models to identify papers with these objectives. As emphasized by Abd-Alrazaq et al. [18] the restriction of works in English may not have been considered significant works written in other languages.
6 Conclusion
In this systematic literature review, we investigate AI’s main scope and contributions to the diagnosis and outcomes of COVID-19, considering the beginning of the pandemic, which was a period dedicated to the exploration of AI-based techniques aimed at identifying some patterns that mapped relationships between clinical data and images with diagnoses and outcomes. This search began by collecting 839 articles, and after going through all the steps of the selection criteria, it grouped 64 selected studies that were analyzed in this systematic review. In both contexts, medical imaging analyses, whether chest X-Ray, chest CT or ultrasound, were used, especially in the case of studies aimed at diagnosis. Among the imaging exams, the use of chest CT stands out. However, clinical and laboratory data were used more frequently in papers involving outcome.
Generally, a sensitive point for models based on DL is the quantity of data available for training the models. Specifically, for works related to semantic segmentation of medical images, there is a need for manual annotation of the images of the areas of interest in the images. This work is expense and arduous due to its high complexity and needing experienced doctors to generate an accurate annotation of the medical image. To overcome this problem, the authors use transfer learning and data-augmentation techniques to mitigate this restriction [55, 62, 66, 69, 70, 76, 77].
For structured data (clinical and laboratory data), which generally have many attributes, close to 60% of the papers used some technique to reduce the data elements by selecting or compressing the data.
It is important to emphasize that the results obtained with image processing or clinical and laboratory data are, in many cases, above 95% of accuracy, indicating that AI techniques are valuable for decision making in a more sensitive area such as healthcare. However, one of the biggest challenges in the area seems to be the lack of explanation offered by the results found by the models. In this sense, one can point out that explainable artificial intelligence [101] has been growing to fill this gap.
Combining the terms CNN, the most frequent network model in this systematic review, Covid-19 and considering the 2022 year, a quick search was performed on Scholar-Google. More than 1000 papers were listed. This fact reinforces the importance of more specific systematic reviews considering the AI/ML techniques.
This work provides medical and AI researchers with a broad overview of AI contributions involving any type of data to the development of research to combat COVID-19, aiming to inspire new work to continue maximizing the advantages of AI with small or large databases to combat this pandemic. Finally, it is important to stress that in the initial of the disease was thought to affect mainly the lungs. Today it is known that it is a systemic disease that affects other organs and physiological systems [102]. In this context, new challenges arise for the automation of diagnoses and outcomes, integrating, in addition to images, clinical, and laboratory data. Although most patients recovered, several long-lasting symptoms were described and named “long-term COVID-19 syndrome” [103]. In this case, AI/ML models can be exploited from patient data to identify the potential to develop such a syndrome early and provide rehabilitation support more quickly. Other topics that can be further explored from an AI point of view are related to the diagnosis of Covid-19 in pediatric patients and the prediction of the duration of hospitalization in COVID-19 patients, considering ML models with a high level of accuracy [104].
Availability of Data and Materials
The data and materials used can be found in the references of this work.
Abbreviations
- AD3D0MIL:
-
Attention-based deep 3D multiple instance learning
- AFS-DF:
-
Adaptive feature selection guided deep forest
- AI:
-
Artificial intelligence
- AlexNet:
-
Is the name of a convolutional neural network (CNN) architecture, designed by Alex Krizhevsky
- ANN:
-
Artificial neural network
- AUC:
-
Area under the ROC curve
- CNN:
-
Convolution neural networks
- CNNLSTM:
-
Convolutional neural network long-short time memory
- CNNRNN:
-
Convolutional neural networks recurrent neural networks
- ConvLSTM:
-
Convolutional long short-term memory
- COVID-19:
-
Coronavirus disease 2019
- CT:
-
Computed tomography
- DeepLabv3:
-
The third version of the system of semantic image segmentation task
- DenseNet121:
-
Densely connected CNN with 121 layers, an architecture of convolutional neural network
- DenseNet201:
-
Densely connected CNN with 201 layers, an of convolutional neural network
- DL:
-
Deep learning
- DNA:
-
Deoxyribonucleic acid (abbreviated)
- EfficientNet:
-
Are a family of models based on deep learning scaled up very effectively
- GAN:
-
Generative adversarial network
- Grad-CAM:
-
Gradient-weighted class activation mapping
- H1n1:
-
Flu that is known popularly as Swine flu
- ImageNet:
-
T is an image database organized according to the WordNet hierarchy (currently only the nouns), in which each node of the hierarchy is depicted by hundreds and thousands of images
- InceptionV3:
-
Is a convolutional neural network for assisting in image analysis and object detection
- KNN:
-
K-nearest neighbor
- LR:
-
Logist regression
- LSTM:
-
Long-short time memory
- MERS:
-
Middle east respiratory syndrome
- MH-CovidNet:
-
Is the name given by its authors to the proposed methodology that joins deep learning algorithms and meta-heuristic algorithms
- ML:
-
Machine learning
- nCOVNet:
-
Deep learning neural network-based method
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- ReLu:
-
Rectified linear unit activation function
- ResNet:
-
Residual neural network
- ResNet50:
-
Is a convolutional neural network that is 50 layers deep
- RF:
-
Decision tree-based algorithms
- RNA:
-
Ribonucleic acid (abbreviated)
- RNN:
-
Recurrent neural networks
- ROC:
-
Receiver operating characteristic
- SARS:
-
Severe acute respiratory syndrome
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- SVM:
-
Decision tree, support vector machine
- U-Net:
-
Is a convolutional neural network that was developed for biomedical image segmentation
- VGG:
-
Is a classical convolutional neural network architecture, stands for visual geometry group
- VGG-16:
-
Is a convolutional neural network model with 16 layers
- WHO:
-
World Health Organization
- XGboost:
-
Method that seeks to improve the performance of gradient boosting by optimizing
References
Verma, S., Manjunath, S.M., Ettishree, A.S., Srivastava, M., Sahoo, K.K., et al.: Coronavirus: An emergency for healthcare professionals. J. Fam. Med. Prim. Care 9(4), 1815 (2020). https://doi.org/10.4103/jfmpc.jfmpc46220
World Health Organization.: “WHO Statement on the Second Meeting of the International Health Regulation (2005) Emergency Committee Regulating the Outbreak of the Novel Corona Virus (2019-nCOV)”. https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov). Accessed 30 Jan 2020
Rajendran, D.K., Rajagopal, V., Alagumanian, S., Santhosh Kumar, T., Sathiya Prabhakaran, S.P., et al.: Systematic literature review on novel corona virus SARS-CoV-2: a threat to human era. Virus Dis. 31(2), 161–173 (2020). https://doi.org/10.1007/s13337-020-00604-z
Salian, V.S., Wright, J.A., Vedell, P.T., Nair, S., Li, C., et al.: COVID-19 transmission, current treatment, and future therapeutic strategies. Mol. Pharm. 18(3), 754–771 (2021). https://doi.org/10.1021/acs.molpharmaceut.0c00608
Mullard, A.: COVID-19 vaccine development pipeline gears up. Lancet 395(10239), 1751–1752 (2020)
Ouassou, H., Kharchoufa, L., Bouhrim, M., Daoudi, N.E., Imtara, H., et al.: The pathogenesis of coronavirus disease 2019 (COVID-19): evaluation and prevention. J. Immunol. Res. (2020). https://doi.org/10.1155/2020/1357983
Research Support Foundation of the State of São Paulo: “Inteligência artificial contra a Covid-19”. https://revistapesquisa.fapesp.br/inteligencia-artificial-contra-a-covid-19. Accessed 15 Apr 2020
Giger, M.L.: Machine learning in medical imaging. J. Am. Coll. Radiol. 15(3), 512–520 (2018). https://doi.org/10.1016/j.jacr.2017.12.028
Erickson, B.J., Korfiatis, P., Akkus, Z., Kline, T.L.: Machine learning for medical imaging. Radiographics 37(2), 505–515 (2017). https://doi.org/10.1148/rg.2017160130
Choy, G., Khalilzadeh, O., Michalski, M., Do, S., Samir, A.E., et al.: Current applications and future impact of machine learning in radiology. Radiology 288(2), 318 (2018). https://doi.org/10.1148/radiol.2018171820
Santos, M.K., Ferreira Ju´nior, J.R., Wada, D.T., Tenório, A.P.M., Nogueira-Barbosa, M.H., et al.: Inteligência artificial, aprendizado de máquina, diagnóstico auxiliado por computador e radiomica: avanços da imagem rumo à medicina de precisão. Radiol. Bras. 52, 387–396 (2019). https://doi.org/10.1590/0100-3984.2019.0049
Li, L., Qin, L., Xu, Z., Yin, Y., Wang, X., et al.: Artificial intelligence distinguishes COVID-19 from community acquired pneumonia on chest CT. Radiology (2020). https://doi.org/10.1148/radiol.2020200905
Bullock, J., Luccioni, A., Pham, K.H., Lam, C.S.N., Luengo-Oroz, M.: Mapping the landscape of artificial intelligence applications against COVID-19. J. Artif. Intell. Res. 69, 807–845 (2020)
Goel, K., Shefali, A.: Novel coronavirus (2019-NCOV): impact of global pandemic and predictive analysis using machine learning. Int. J. Eng. Appl. Sci. Technol. 5(3), 2455–2143 (2020). https://doi.org/10.33564/IJEAST.2020.v05i03.059
Sharma, A., Rani, S., Gupta, D.: Artificial intelligence-based classification of chest X-ray images into COVID-19 and other infectious diseases. Int. J. Biomed. Imaging 2020, 1–10 (2020). https://doi.org/10.1155/2020/8889023
Jiao, Z., Choi, J.W., Halsey, K., Tran, T.M.L., Hsieh, B., Wang, D., Bai, H.X.: Prognostication of patients with COVID-19 using artificial intelligence based on chest x-rays and clinical data: a retrospective study. Lancet Dig. Health 3(5), e286–e294 (2021). https://doi.org/10.1016/S2589-7500(21)00039-X
Dogan, O., Tiwari, S., Jabbar, M.A., Guggari, S.: A systematic review on AI/ML approaches against COVID-19 outbreak. Complex Intell. Syst. 7(5), 2655–2678 (2021). https://doi.org/10.1007/s40747-021-00424-8
Abd-Alrazaq, A., Alajlani, M., Alhuwail, D., Schneider, J., Al-Kuwari, S., Shah, Z., Hamdi, M., Househ, M.: Artificial intelligence in the fight against COVID-19: scoping review. J. Med. Internet Res. 22(12), e20756 (2020). https://doi.org/10.2196/20756
Islam, M.N., Inan, T.T., Rafi, S., Akter, S.S., Sarker, I.H., Islam, A.K.M.N.: A systematic review on the use of AI and ML for fighting the COVID-19 pandemic. IEEE Trans. Artif. Intell. 1(3), 258–270 (2020). https://doi.org/10.1109/TAI.2021.3062771
Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G., PRISMA Group: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann. Intern. Med. 151(4), 264–269 (2009). https://doi.org/10.1371/journal.pmed.1000097
Islam, M.Z., Islam, M.M., Asraf, A.: A combined deep CNN- LSTM network for the detection of novel coronavirus (COVID-19) using X-ray images. Inform. Med. Unlocked 20, 100412 (2020). https://doi.org/10.1016/j.imu.2020.100412
Echtioui, A., ZouchW, G.M., Mhiri, C., Hamam, H.: Detection methods of COVID-19. SLAS Technol. 25(6), 566–572 (2020). https://doi.org/10.1177/2472630320962002
Nour, M., Cömert, Z., Polat, K.: A novel medical diagnosis model for COVID-19 infection detection based on deep features and Bayesian optimization. Appl. Soft Comput. 97, 106580 (2020). https://doi.org/10.1016/j.asoc.2020.106580
Sedik, A., Iliyasu, A.M., Abd El-Rahiem, B., Abdel Samea, M.E., Abdel-Raheem, A., et al.: Deploying machine and deep learning models for efficient data-augmented detection of COVID-19 infections. Viruses 12(7), 769 (2020). https://doi.org/10.3390/v12070769
Padma, T., Kumari, C. U.: Deep learning based chest x-ray image as a diagnostic tool for covid-19. In: 2020 International Conference on Smart Electronics and Communication (ICOSEC), pp. 589–592 (2020). https://doi.org/10.1109/ICOSEC49089.2020.9215257
Karar, M.E., Hemdan, E.E.D., Shouman, M.A.: Cascaded deep learning classifiers for computer-aided diagnosis of COVID-19 and pneumonia diseases in X-ray scans. Complex Intell. Syst. 7(1), 235–247 (2021). https://doi.org/10.1007/s40747-020-00199-4
Albahli, S.: Efficient GAN-based chest radiographs (CXR) augmentation to diagnose coronavirus disease pneumonia. Int. J. Med. Sci. 17(10), 1439 (2020). https://doi.org/10.7150/ijms.46684
Abraham, B., Nair, M.S.: Computer-aided detection of COVID-19 from X-ray images using multi-CNN and Bayesnet classifier. Biocybern. Biomed. Eng. 40(4), 1436–1445 (2020). https://doi.org/10.1016/j.bbe.2020.08.005
Fu, L., Li, Y., Cheng, A., Pang, P., Shu, Z.: A novel machine learning- derived radiomic signature of the whole lung differentiates stable from progressive COVID-19 infection: a retrospective cohort study. J. Thorac. Imaging 35(6), 361 (2020). https://doi.org/10.1097/RTI.0000000000000544
Abdulaal, A., Patel, A., Charani, E., Denny, S., Mughal, N., et al.: Prognostic modeling of COVID-19 using artificial intelligence in the United Kingdom: model development and validation. J. Med. Internet Res. 22(8), e20259 (2020). https://doi.org/10.2196/20259
Ma, X., Ng, M., Xu, S., Xu, Z., Qiu, H., et al.: Development and validation of prognosis model of mortality risk in patients with COVID-19. Epidemiol. Infect. (2020). https://doi.org/10.1017/S0950268820001727
Bai, H.X., Wang, R., Xiong, Z., Hsieh, B., Chang, K.: Erratum: Artificial intelligence augmentation of radiologist performance in distinguishing COVID-19 from pneumonia of other origin at chest CT (Radiology (2020) 296 3 (E156-E165)). Radiology (2020). https://doi.org/10.1148/radiol.2020201491
Ko, H., Chung, H., Kang, W.S., Kim, K.W., Shin, Y., et al.: COVID- 19 pneumonia diagnosis using a simple 2D deep learning framework with a single chest CT image: model development and validation. J. Med. Internet Res. 22(6), e19569 (2020). https://doi.org/10.2196/19569
Bridge, J., Meng, Y., Zhao, Y., Du, Y., Zhao, M., et al.: Introducing the GEV activation function for highly unbalanced data to develop COVID-19 diagnostic models. IEEE J. Biomed. Health Inform. 24(10), 2776–2786 (2020). https://doi.org/10.1109/JBHI.2020.3012383
Wu, D., Gong, K., Arru, C.D., Homayounieh, F., Bizzo, B., et al.: Severity and consolidation quantification of COVID-19 from CT images using deep learning based on hybrid weak labels. IEEE J. Biomed. Health Inform. 24(12), 3529–3538 (2020). https://doi.org/10.1109/JBHI.2020.3030224
Roy, S., Menapace, W., Oei, S., Luijten, B., Fini, E., et al.: Deep learning for classification and localization of COVID-19 markers in point-of-care lung ultrasound. IEEE Trans. Med. Imaging 39(8), 2676–2687 (2020). https://doi.org/10.1109/TMI.2020.2994459
Canayaz, M.: MH-COVIDNet: diagnosis of COVID-19 using deep neural networks and meta-heuristic-based feature selection on X-ray images. Biomed. Signal Process. Control 64, 102257 (2021). https://doi.org/10.1016/j.bspc.2020.102257
McRae, M.P., Dapkins, I.P., Sharif, I., Anderman, J., Fenyo, D., et al.: Managing COVID-19 with a clinical decision support tool in a community health network: Algorithm development and validation. J. Med. Internet Res. 22(8), e22033 (2020). https://doi.org/10.2196/22033
Zhang, H.T., Zhang, J.S., Zhang, H.H., Nan, Y.D., Zhao, Y., et al.: Automated detection and quantification of COVID-19 pneumonia: CT imaging analysis by a deep learning-based software. Eur. J. Nucl. Med. Mol. Imaging 47(11), 2525–2532 (2020). https://doi.org/10.1007/s00259-020-04953-1
Qjidaa, M., Ben-Fares, A., Mechbal, Y., Amakdouf, H., Maaroufi, M. et al.: Development of a clinical decision support system for the early detection of COVID-19 using deep learning based on chest radiographic images. In: 2020 International Conference on Intelligent Systems and Computer Vision (ISCV), pp. 1–6. IEEE (2020). https://doi.org/10.1109/ISCV49265.2020.9204282
Yan, T., Wong, P.K., Ren, H., Wang, H., Wang, J., et al.: Automatic distinction between COVID-19 and common pneumonia using multi-scale convolutional neural network on chest CT scans. Chaos Solitons Fractals 140, 110153 (2020). https://doi.org/10.1016/j.chaos.2020.110153
Dey, N., Rajinikanth, V., Fong, S.J., Kaiser, M.S., Mahmud, M.: Social group optimization–assisted Kapur’s entropy and morphological segmentation for automated detection of COVID-19 infection from computed tomography images. Cogn. Comput. 12(5), 1011–1023 (2020). https://doi.org/10.1007/s12559-020-09751-3
Zhang, K., Liu, X., Shen, J., Li, Z., Sang, Y., et al.: Clinically applicable AI system for accurate diagnosis, quantitative measurements, and prognosis of COVID-19 pneumonia using computed tomography. Cell 181(6), 1423–1433 (2020). https://doi.org/10.1016/j.cell.2020.04.045
Sun, L., Mo, Z., Yan, F., Xia, L., Shan, F., et al.: Adaptive feature selection guided deep forest for covid-19 classification with chest CT. IEEE J. Biomed. Health Inform. 24(10), 2798–2805 (2020). https://doi.org/10.1109/JBHI.2020.3019505
Ahamad, M.M., Aktar, S., Rashed-Al-Mahfuz, M., Uddin, S., Lio, P., et al.: A machine learning model to identify early stage symptoms of SARS- Cov-2 infected patients. Expert Syst. Appl. 160, 113661 (2020). https://doi.org/10.1016/j.eswa.2020.113661
Ardakani, A.A., Acharya, U.R., Habibollahi, S., Mohammadi, A.: COVIDiag: a clinical CAD system to diagnose COVID-19 pneumonia based on CT findings. Eur. Radiol. 31(1), 121–130 (2020). https://doi.org/10.1007/s00330-020-07087-y
Toraman, S., Alakus, T.B., Turkoglu, I.: Convolutional cap-snet: a novel artificial neural network approach to detect COVID-19 disease from X-ray images using capsule networks. Chaos Solitons Fractals 140, 110122 (2020). https://doi.org/10.1016/j.chaos.2020.110122
Yue, H., Yu, Q., Liu, C., Huang, Y., Jiang, Z., et al.: Machine learning-based CT radiomics method for predicting hospital stay in patients with pneumonia associated with SARS-CoV-2 infection: a multicenter study. Ann. Transl. Med. 8, 14 (2020). https://doi.org/10.1101/2020.02.29.20029603
Chen, X., Zhenqiu, L.: Early prediction of mortality risk among severe COVID-19 patients using machine learning (2020). https://doi.org/10.1101/2020.04.13.20064329
Li, L., Qin, L., Xu, Z., Yin, Y., Wang, X., et al.: Using artificial intelligence to detect COVID-19 and community-acquired pneumonia based on pulmonary CT: evaluation of the diagnostic accuracy. Radiology 296(2), E65–E71 (2020). https://doi.org/10.1148/radiol.2020200905
Alakus, T.B., Turkoglu, I.: Comparison of deep learning approaches to predict COVID-19 infection. Chaos Solitons Fractals 140, 110120 (2020). https://doi.org/10.1016/j.chaos.2020.110120
Cai, W., Liu, T., Xue, X., Luo, G., Wang, X.: CT quantification and machine-learning models for assessment of disease severity and prognosis of COVID- 19 patients. Acad. Radiol. 27(12), 1665–1678 (2020). https://doi.org/10.1016/j.acra.2020.09.004
Ardakani, A.A., Kanafi, A.R., Acharya, U.R., Khadem, N., Mohammadi, A.: Application of deep learning technique to manage COVID-19 in routine clinical practice using CT images: results of 10 convolutional neural networks. Comput. Biol. Med. 121, 103795 (2020). https://doi.org/10.1016/j.compbiomed.2020.103795
Pathak, Y., Shukla, P. K., Tiwari, A., Stalin, S., Singh, S.: Deep transfer learning based classification model for COVID-19 disease. IRBM (2020). https://doi.org/10.1016/j.irbm.2020.05.003
Rahaman, M.M., Li, C., Yao, Y., Kulwa, F., Rahman, M.A.: Identification of COVID-19 samples from chest X-Ray images using deep learning: a comparison of transfer learning approaches. J. Xray Sci. Technol. 28(5), 821–839 (2020). https://doi.org/10.3233/XST-200715
Amyar, A., Modzelewski, R., Li, H., Ruan, S.: Multi-task deep learning based CT imaging analysis for COVID-19 pneumonia: classification and segmentation. Comput. Biol. Med. 126, 104037 (2020). https://doi.org/10.1016/j.compbiomed.2020.104037
Panwar, H., Gupta, P.K., Siddiqui, M.K., Morales-Menendez, R., Singh, V.: Application of deep learning for fast detection of COVID-19 in X-rays using nCOVnet. Chaos Solitons Fractals 138, 109944 (2020). https://doi.org/10.1016/j.chaos.2020.109944
Zhang, R., Tie, X., Qi, Z., Bevins, N.B., Zhang, C., et al.: Diagnosis of coronavirus disease 2019 pneumonia by using chest radiography: Value of artificial intelligence. Radiology 298(2), E88 (2021). https://doi.org/10.1148/radiol.2020202944
Anastasopoulos, C., Weikert, T., Yang, S., Abdulkadir, A., Schmülling, L., et al.: Development and clinical implementation of tailored image analysis tools for COVID-19 in the midst of the pandemic: The synergetic effect of an open, clinically embedded software development platform and machine learning. Eur. J. Radiol. 131, 109233 (2020). https://doi.org/10.1016/j.ejrad.2020.109233
Fan, D.P., Zhou, T., Ji, G.P., Zhou, Y., Chen, G., et al.: Inf-net: automatic covid-19 lung infection segmentation from ct images. IEEE Trans. Med. Imaging 39(8), 2626–2637 (2020). https://doi.org/10.1109/TMI.2020.2996645
Di Castelnuovo, A., Bonaccio, M., Costanzo, S., Gialluisi, A., Antinori, A.: Common cardiovascular risk factors and in-hospital mortality in 3,894 patients with COVID-19: survival analysis and machine learning-based findings from the multicentre Italian CORIST Study. Nutr. Metab. Cardiovasc. Dis. 30(11), 1899–1913 (2020). https://doi.org/10.1016/j.numecd.2020.07.031
Qian, X., Fu, H., Shi, W., Chen, T., Fu, Y., et al.: M3 Lung-Sys: a deep learning system for multi-class lung pneumonia screening from CT imaging. IEEE J. Biomed. Health Inform. 24(12), 3539–3550 (2020). https://doi.org/10.1109/JBHI.2020.3030853
Hu, S., Gao, Y., Niu, Z., Jiang, Y., Li, L., et al.: Weakly supervised deep learning for covid-19 infection detection and classification from ct images. IEEE Access 8, 118869–118883 (2020). https://doi.org/10.1109/ACCESS.2020.3005510
Han, Z., Wei, B., Hong, Y., Li, T., Cong, J., et al.: Accurate screening of COVID-19 using attention-based deep 3D multiple instance learning. IEEE Trans. Med. Imaging 39(8), 2584–2594 (2020). https://doi.org/10.1109/TMI.2020.2996256
Xu, X., Jiang, X., Ma, C., Du, P., Li, X., et al.: A deep learning system to screen novel coronavirus disease 2019 pneumonia. Engineering 6(10), 1122–1129 (2020). https://doi.org/10.1016/j.eng.2020.04.010
Jain, G., Mittal, D., Thakur, D., Mittal, M.K.: A deep learning approach to detect Covid-19 coronavirus with X-ray images. Biocybern. Biomed. Eng. 40(4), 1391–1405 (2020). https://doi.org/10.1016/j.bbe.2020.08.008
Silva, P., Luz, E., Silva, G., Moreira, G., Silva, R., et al.: COVID-19 detection in CT images with deep learning: a voting-based scheme and cross-datasets analysis. Inform. Med. Unlocked 20, 100427 (2020). https://doi.org/10.1016/j.imu.2020.100427
Khanday, A.M.U.D., Rabani, S.T., Khan, Q.R., Rouf, N., Din, M.M.U.: Machine learning based approaches for detecting COVID-19 using clinical text data. Int. J. Inf. Technol. 12(3), 731–739 (2020). https://doi.org/10.1007/s41870-020-00495-9
Jaiswal, A., Gianchandani, N., Singh, D., Kumar, V., Kaur, M.: Classification of the COVID-19 infected patients using DenseNet201 based deep transfer learning. J. Biomol. Struct. Dyn. 39(15), 5682–5689 (2021). https://doi.org/10.1080/07391102.2020.1788642
Makris, A., Kontopoulos, I., Tserpes, K.: COVID-19 detection from chest X-ray images using deep learning and convolutional neural networks. In: 11th hellenic conference on artificial intelligence, pp. 60–66 (2020). https://doi.org/10.1145/3411408.3411416
Altan, A., Karasu, S.: Recognition of COVID-19 disease from X-ray images by hybrid model consisting of 2D curvelet transform, chaotic salp swarm algorithm and deep learning technique. Chaos Solitons Fractals 140, 110071 (2020). https://doi.org/10.1016/j.chaos.2020.110071
Brunese, L., Mercaldo, F., Reginelli, A., Santone, A.: Explainable deep learning for pulmonary disease and coronavirus COVID-19 detection from X-rays. Comput. Methods Progr. Biomed. 196, 105608 (2020). https://doi.org/10.1016/j.cmpb.2020.105608
Mishra, A.K., Das, S.K., Roy, P., Bandyopadhyay, S.: Identifying COVID19 from chest CT images: a deep convolutional neural networks based approach. J. Healthc. Eng. (2020). https://doi.org/10.1155/2020/8843664
Zhou, L., Li, Z., Zhou, J., Li, H., Chen, Y.: A rapid, accurate and machine-agnostic segmentation and quantification method for CT-based COVID-19 diagnosis. IEEE Trans. Med. Imaging 39(8), 2638–2652 (2020). https://doi.org/10.1109/TMI.2020.3001810
Polsinelli, M., Cinque, L., Placidi, G.: A light CNN for detecting COVID-19 from CT scans of the chest. Pattern Recognit. Lett. 140, 95–100 (2020). https://doi.org/10.1016/j.patrec.2020.10.001
Oh, Y., Park, S., Ye, J.C.: Deep learning COVID-19 features on CXR using limited training data sets. IEEE Trans. Med. Imaging 39(8), 2688–2700 (2020). https://doi.org/10.1109/TMI.2020.2993291
Tsiknakis, N., Trivizakis, E., Vassalou, E.E., Papadakis, G.Z., Spandidos, D.A., et al.: Interpretable artificial intelligence framework for COVID-19 screening on chest X-rays. Exp. Ther. Med. 20(2), 727–735 (2020). https://doi.org/10.3892/etm.2020.8797
Khalifa, N. E. M., Taha, M. H. N., Hassanien, A. E., Taha, S. H. N. et al.: The detection of covid-19 in ct medical images: A deep learning approach. In: Big Data Analytics and Artificial Intelligence against COVID-19: Innovation Vision and Approach, pp. 73–90 (2020). https://doi.org/10.1007/978-3-030-55258-95
Mahmud, T., Rahman, M.A., Fattah, S.A.: CovXNet: a multi-dilation convolutional neural network for automatic COVID-19 and other pneumonia detection from chest X-ray images with transferable multi-receptive feature optimization. Comput. Biol. Med. 122, 103869 (2020). https://doi.org/10.1016/j.compbiomed.2020.103869
Wu, G., Zhou, S., Wang, Y., Lv, W., Wang, S.: A prediction model of outcome of SARS-CoV-2 pneumonia based on laboratory findings. Sci. Rep. 10(1), 1–9 (2020). https://doi.org/10.1038/s41598-020-71114-7
Yu, Z., Li, X., Sun, H., Wang, J., Zhao, T., et al.: Rapid identification of COVID-19 severity in CT scans through classification of deep features. Biomed. Eng. Online 19(1), 1–13 (2020). https://doi.org/10.1186/s12938-020-00807-x
Yoo, S.H., Geng, H., Chiu, T.L., Yu, S.K., Cho, D.C., et al.: Deep learning-based decision-tree classifier for COVID-19 diagnosis from chest X-ray imaging. Front. Med. 7, 427 (2020). https://doi.org/10.3389/fmed.2020.00427
Pan, P., Li, Y., Xiao, Y., Han, B., Su, M., et al.: Prognostic assessment of COVID-19 in ICU by machine learning methods: a retrospective study. J. Med. Internet Res. (2020). https://doi.org/10.2196/23128
Liu, C., Wang, X., Liu, C., Sun, Q., Peng, W.: Differentiating novel coronavirus pneumonia from general pneumonia based on machine learning. Biomed. Eng. Online 19(1), 1–14 (2020). https://doi.org/10.1186/s12938-020-00809-9
Fukushima, K.: Neocognitron. Scholarpedia 2(1), 1717 (2007). https://doi.org/10.4249/scholarpedia.1717
Hochreiter, S., Schmidhuber, J.: Long short-term memory. Neural Comput. 9(8), 1735–1780 (1997). https://doi.org/10.1162/neco.1997.9.8.1735
Van Timmeren, J.E., Cester, D., Tanadini-Lang, S., Alkadhi, H., Baessler, B.: Radiomics in medical imaging—“how-to” guide and critical reflection. Insights Imaging 11(1), 1–16 (2020). https://doi.org/10.1186/s13244-020-00887-2
Ding, C., Peng, H.: Minimum redundancy feature selection from microarray gene expression data. J. Bioinform. Comput. Biol. 3(2), 185–205 (2005). https://doi.org/10.1142/S0219720005001004
Tibshirani, R.: The lasso method for variable selection in the Cox model. Stat. Med. 16(4), 385–395 (1997). https://doi.org/10.1002/(SICI)1097-0258(19970228)16:4¡385::AID-SIM380¿3.0.CO;2-3
Myers, J.L., Well, A.D., Lorch Jr, R.F.: Research Design and Statistical Analysis, 3rd edn. Routledge, New York (2010). https://doi.org/10.4324/9780203726631
Abdi, H., Williams, L.J.: Principal component analysis. WIREs Comput. Stat. 2(4), 433–459 (2010). https://doi.org/10.1002/wics.101
Krizhevsky, A., Sutskever, I., Hinton, G.E.: Imagenet classification with deep convolutional neural networks. Advances in neural information processing systems, p. 25 (2012). https://proceedings.neurips.cc/paper/2012/file/c399862d3b9d6b76c8436e924a68c45b-Paper.pdf
He, K., Zhang, X., Ren, S., Sun, J.: Deep residual learning for image recognition. In: Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, pp. 770–778 (2016). https://openaccess.thecvf.com/contentcvpr2016/papers/He Deep Residual Learning CVPR 2016 paper.pdf
Tan, M., Le, Q.: Efficientnet: rethinking model scaling for convolutional neural networks. In: International conference on machine learning, pp. 6105–6114 (2019). http://proceedings.mlr.press/v97/tan19a.html
Goodfellow, I., Bengio, Y., Courville, A.: Deep learning. MIT Press, Cambridge (2016)
Ronneberger, O., Fischer, P., Brox, T.: U-net: convolutional networks for biomedical image segmentation. In: International Conference on Medical Image Computing and Computer-Assisted Intervention, pp. 234–241 (2015). https://doi.org/10.1007/978-3-319-24574-428
Cortes, C., Vapnik, V.: Support-vector networks. Mach. Learn. 20(3), 273–297 (1995). https://doi.org/10.1007/BF00994018
Haykin, S., Network, N.: A comprehensive foundation. Neural Netw. 2, 41 (2004)
Ho, T. K.: Random decision forests. In: Proceedings of 3rd International Conference on Document Analysis and Recognition, vol. 1, pp. 278–282 (1995). https://doi.org/10.1109/ICDAR.1995.598994
Chen, T., Guestrin, C.: Xgboost: a scalable tree boosting system. In: Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, pp 785–794 (2016). https://doi.org/10.1145/2939672.2939785
Gunning, D., Stefik, M., Choi, J., Miller, T., Stumpf, S., et al.: XAI—explainable artificial intelligence. Sci. Robot. 4(37), eaay7120 (2019). https://doi.org/10.1126/scirobotics.aay7120
Ashraf, U.M., Abokor, A.A., Edwards, J.M., Waigi, E.W., Royfman, R.S., et al.: SARS-CoV-2, ACE2 expression, and systemic organ invasion. Physiol. Genom. (2021). https://doi.org/10.1152/physiolgenomics.00087.2020
Cau, R., Faa, G., Nardi, V., Balestrieri, A., Puig, J., Suri, J.S., SanFilippo, R., Saba, L.: Long-COVID diagnosis: from diagnostic to advanced AI-driven models. Eur. J. Radiol. 148, 110164 (2022). https://doi.org/10.1016/j.ejrad.2022.110164
Rostami, M., Oussalah, M.: A novel explainable COVID-19 diagnosis method by integration of feature selection with random forest. Inform. Med. Unlocked 30, 100941 (2022). https://doi.org/10.1016/j.imu.2022.100941
Funding
The authors thankfully acknowledge the financial support from the Brazilian research agencies. This work was funded by the National Council for Scientific and Technological Development—CNPq under Grant 308717/2020-1, the Coordination for the Improvement of Higher Education Personnel (CAPES)—Finance Code 001 and under grant 88881.506840/2020-01, and Carlos Chagas Filho Foundation for Research Support in the State of Rio de Janeiro (FAPERJ) under “Grant E43/2021—Terceira Chamada Emergencial de projetos para combater os efeitos da COVID—2021, processo E26/211.136/2021”.
Author information
Authors and Affiliations
Contributions
KF, RMEMC, VMBW proposed and designed the study. AGM, AMT, CCPC, FHC, LYM, and SHA described the search expressions and found the articles. They did the first review, data extraction, and classification. COF, KF, RC, RL, RMEMC, and VMBW conducted the step that confirmed the chosen selected studies. All authors prepared the tables and figures, drew up the final draft, and made a critical revision. Also, all authors wrote, read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Authors report no potential conflict of interest.
Ethics approval and consent to participate
Not applicable because this work is a systematic review based in works published in journals.
Consent for publication
Not applicable because this work is systematic review based in works published in journals.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mano, L.Y., Torres, A.M., Morales, A.G. et al. Machine Learning Applied to COVID-19: A Review of the Initial Pandemic Period. Int J Comput Intell Syst 16, 73 (2023). https://doi.org/10.1007/s44196-023-00236-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44196-023-00236-3