
Abstract
Perioperative opioid stewardship programs aim to harness the benefits of opioid analgesia for managing acute post-surgical pain whilst mitigating potential harm. Healthcare worker stakeholders are vital for the effective program introduction and continuation. However, their perceptions of program barriers and promotors are underexplored. We conducted twenty semi-structured interviews with healthcare workers across three health services that introduced a perioperative opioid stewardship program. The participants included specialist pain medicine physicians, anaesthetist managers, pain nurses, pharmacists and Junior Medical Officers. Interviews were transcribed and coded both inductively and deductively against the Consolidated Framework of Implementation Research. Key themes from the data were reviewed, refined and reported. Participants were generally aware of perioperative opioid stewardship principles but senior clinicians reported greater specific program knowledge. Adherence to the discharge opioid prescription guideline was promoted by hospital leadership endorsement and workflow integration. A universal barrier to program adherence was inadequate resourcing. Lack of role clarity was a barrier to patient discharge opioid education. Hospital-community prescriber communication was variable but generally limited to written discharge summaries rather than a comprehensive, personalised approach. Introducing an Electronic Medical Record was universally seen as an opportunity to promote better program integration and sustainment. This study deepens our current understanding of the drivers of observed perioperative opioid stewardship program outcomes from the perspective of healthcare worker stakeholders. The findings could be used to optimise existing programs or to guide the implementation of new programs to achieve effective clinical change.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Opioids are a mainstay of post-surgical analgesia for moderate to severe pain. However, opioid-related harm is a significant concern both acutely (Roxburgh et al., 2011; Blanch et al., 2014; Roxburgh & Burns, 2017; Brat et al., 2018) and due to persistent use after intended short-term therapy (Macintyre et al., 2014; Chou et al., 2015; Shah et al., 2017; Suckling et al., 2022). Analgesic stewardship programs are designed to ensure that patients most likely to benefit receive appropriate opioid therapy whilst mitigating the potential harms. The Australian Commission for Safety and Quality in Health Care clinical care standard for the use of opioids in acute pain was released in May 2022 (Australian Commission on Safety and Quality in Health Care, 2022). These standards define practice expectations based on the best evidence for patients accessing health care in Australia and so provide the impetus for hospitals to implement opioid stewardship programs. Therefore, understanding the factors likely to drive or hinder opioid stewardship programs is a health service priority.
Recent international multidisciplinary consensus guidelines on perioperative opioid harm reduction provide a best practice framework (Levy et al., 2021). However, the barriers, promotors and factors impacting the introduction and sustainability of perioperative opioid stewardship programs are underexplored. Healthcare workers play a crucial role in opioid stewardship programs. A US study has reported the barriers and promotors of a perioperative opioid stewardship program anticipated by healthcare workers before program implementation (Coughlin et al., 2019). However, post-implementation evaluation of such programs from the perspective of healthcare worker stakeholders warrants investigation. Perioperative opioid stewardship targets multiple levels of organisations with established complex workflows and interdisciplinary interactions. Therefore, these programs must be nuanced and adapted to the local context to be effective (Alexander & Hearld, 2012; Tomoaia-Cotisel et al., 2013). An opioid stewardship program may fail to comprehensively or enduringly optimise practice due to the low efficacy of the intervention, its implementation, acceptability, or sustainability, or the interplay of these factors (Alexander & Hearld, 2012).
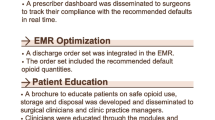
We introduced a perioperative opioid stewardship program at three metropolitan health services in Melbourne, Australia (Allen et al., 2023). This program targeted surgical patients other than day cases and comprised guidance for discharge opioid and adjunct analgesia, patient education, prescriber education and hospital-community care provider communication. Junior medical officers (JMOs) performed 95% of the discharge opioid prescribing, and there was a reduction in post-surgical discharge opioid prescribing after implementing the program (Allen et al., 2023). We also found improvements in patient-reported medication handling in the post-stewardship program cohort compared to the baseline cohort (Allen et al., 2020, 2023). However, some suboptimal practices persisted, including low rates of opioid disposal and poor communication, with only a 17% incidence of a hospital-community prescriber letter being used. Maintaining our program in the busy healthcare environment has been challenging, and similar studies have reported difficulties sustaining program changes over time (Stanley et al., 2022).
When we introduced our perioperative opioid stewardship program, we did not systematically evaluate its implementation or impact on usual workflows at the health services; we only assessed the quantitative impact on opioid prescribing and management. The current study sought to address these gaps. Specifically, we designed this study to explore clinicians’ impressions in the participating health services regarding the barriers to and promotors of successful implementation in their workplace. We also sought their insights into the factors influencing program sustainability and suggestions for future optimisation.
Given our study aims and design we planned to undertake framework analysis of the program implementation. We selected the Consolidated Framework of Implementation Research (CFIR) as it addresses the context in which the change occurs and its effect on the implementation, which aligned with our study aims (Damschroder et al., 2009). The CFIR is best used for people who hold sway over implementation outcomes through having power (e.g., through leadership) or being the end-users, which is well aligned to our target study population. We used version 1 of CFIR as our analysis was near completion at the time of the release of CFIR version 2 (Damschroder et al., 2022). CFIR version 1 has the domains of intervention characteristics, outer setting, inner setting, characteristics of individuals and implementation process (Damschroder et al., 2009). These domains encompass the relevant factors for the perioperative opioid stewardship program.
Design and Methods
The necessary ethics and governance approvals (MH_HREC_2020.26/17,092,020) were obtained before the study commenced. We conducted a qualitative study using semi-structured one-on-one interviews with clinicians participating in perioperative opioid stewardship programs.
Three publicly funded, university-affiliated metropolitan health services in Melbourne, Australia, share an Electronic Medical Record (EMR) and have introduced our perioperative opioid stewardship program. The study recruited clinicians practising at the target health services when the program was introduced. We designed this study to commence after the perioperative opioid stewardship program had been in place for at least one year in each health service. However, with the onset of the COVID-19 pandemic, commencement was delayed, so the programs had been active in the target health services for over 18 months when recruitment commenced. The COREQ checklist (Tong et al., 2007) for the study design and reporting is Supplementary File 1.
Recruitment
We invited at least four potential participants from each health service to interview. The invitation was via an email containing information on the study intent and participant requirements. No response was received to four invitations, and all consenting participants completed the study. No reimbursement was offered for participation. The breadth of role representation was achieved by initial purposive sampling from the following groups of clinicians: specialist pain medicine physicians, anaesthetist managers (e.g., heads of service or department), pain nurses, pharmacists and JMOs. Snowball recruitment was then employed, with participants invited to nominate further potential participants at the end of their interview. The recruitment target was 16 to 20 participants to achieve data saturation, (Guest et al., 2006) accounting for the subgroupings of clinical roles and health services sampled (Romney et al., 1986).
Data Collection
Before the interviews, we invited each health service’s head of anaesthesia or pain medicine to complete a survey, collecting details of the stewardship program components introduced and local adaptations (Supplementary file 2). We used the responses to adjust the standard interview protocol for each health service participant. We piloted the interview guide (components in Table 1, complete guide supplementary file 3) with two clinicians in relevant disciplines before study commencement.
A single investigator (MLA) conducted semi-structured interviews after obtaining written consent from study participants. This investigator had qualitative research methodology training, including online semi-structured interviews. The investigator had previous professional interactions with several of the study participants, both clinically and through introducing the perioperative opioid stewardship program at some health services. The interviews occurred at a date and time nominated by participants. The interview guide gave the structure, but additional questions were asked to clarify or extend the concepts raised. All interviews were conducted over videoconference (Zoom, 2022) and were audio-visually recorded. The audio files underwent automated transcription (Sonix Inc., 2022).
During and immediately following each interview, contemporaneous field notations were made. The transcripts were reviewed and compared to the original audio file and field notes, with corrections and bracketed insertions of definitions and redaction of identifying segments made where necessary by a single investigator (MLA). All participants were offered the opportunity to review their interview transcript before analysis. Minor edits were made in response to feedback from a few participants, with no change to the core content.
Coding and Analysis
The interview data were imported into NVivo software (Lumivero, 2022) to assist with analysis. Qualitative evaluative action research underlies this study of the perioperative opioid stewardship program. We used a template analysis approach for data analysis (King, 2012; Brooks & King, 2014; Keith et al., 2017). This allowed us to analyse our large dataset efficiently without losing richness. Prespecified contextual factors were the health service and the clinical role of the study participants. Coding was deductive with the full CFIR (Damschroder et al., 2009) represented in the NVivo node hierarchy from the outset of analysis. In addition to the deductive coding, we also performed inductive coding with the generation of new themes and subthemes emerging where the CFIR constructs did not apply to the study data.
Two study investigators (MLA and KS) coded all interview transcripts. A contingency escalation pathway to the senior researcher (JMN) for adjudication of discrepancies arising during analysis was predetermined but not required. The coders independently coded four interviews deductively against the complete CFIR constructs using the operations guide definitions (CFIR guide, 2009; Damschroder & Lowery, 2013). The analytic approach needed the coders to interpret and classify the study data when coding, considering the data segments’ overt and semantic meanings. Co-coding to multiple constructs was permitted. They then reviewed their initial independent coding for consistency, discussing and resolving discrepancies. They defined the initial study codebook by formulating supplementary context-specific definitions for the CFIR and non-CFIR constructs for use in coding the remainder of the study data.
After completing individual coding for each clinical role, the inter-coder discussion was repeated for all transcripts. Additionally, the transcripts coded early in the analysis were re-reviewed at the end of the coding to account for learning effects. The coders agreed that data saturation had been reached with no new themes emerging. Once coding was complete, the investigators conducted a construct review for the CFIR coding template and non-CFIR inductively coded constructs. Both coding investigators examined the data coded at each domain and its constructs. The classification was discussed, and un-coding or re-coding was performed until we obtained a final agreed study data set. Once coding and construct review were completed, the key themes were reviewed and refined into the final themes. Table 2 contains the final codebook for the CFIR and non-CFIR domains and study context-specific definitions.
We then mapped these domains and themes to the opioid stewardship program components and classified them as promoting or barrier factors. Our final analysis phase explored the participant’s suggestions for program optimisation or reflections on future program implementation at their health service, mapped to the program components. Participants could choose to receive a summary of the study findings, but their feedback was not recorded or included in the study reporting.
Results
Twenty semi-structured interviews were conducted between 29/10/2021 and 30/5/2022. The range of interview duration was 19 min to 44 min (mean 30 min). Interview invitations were sent to 16 potential participants, and all accepted and completed the interview. Snowball recruitment was used from these initial participants, and in many cases, the other interview subjects suggested those who had already been invited. However, eight additional potential participants were proposed, and four (50%) consented and completed the interview. The other four (50%) potential participants did not respond to the invitation. Table 3 shows the participant distribution by sex, health services and clinical roles for those who completed a study interview.
Barriers and facilitators, based on CFIR, are described for the four pillars of the opioid stewardship program, as well as reflections on the implementation of the program overall. For each component of the opioid stewardship program and the implementation and sustainment phases, the domains and themes were classified as barriers or promotors Illustrative quotations for implementing the program components, organised as barriers or promoting factors and with key themes indicated, are presented in Supplementary file 4. Supplementary file 5 includes selected quotations from stakeholder participants for program sustainability and optimisation and contains the relevant study themes. Below, we describe the main study findings related to the four opioid stewardship program components and the program implementation, sustainability and optimisation with the main themes bracketed.
Discharge Prescription Guideline
Guideline adherence was facilitated by integration into workflow and endorsement of leadership. JMO participants reported overt support for a discharge prescription guideline integrated into their workflow (Planning quality). Top-down expression of the acceptability of the proposed change was advocated to increase compliance by the JMOs (Implementation climate). However, consideration of how work is performed and not increasing burden was also expressed as essential (Resourcing). The dual goals of desiring to conduct optimal evidence-based practice and to please the senior staff in their unit were acknowledged. Pain specialists also noted this tension in educating JMOs and expressed it as a potential barrier to program uptake and sustainment (Change leaders). Hospital C participants related a highly data-driven approach to clinical change (Patient needs and resources).
Participants expressed minimal concern about the content of locally adapted discharge opioid prescription guidelines, regardless of their clinical role or health service. This was variably attributed to effective stakeholder consultation, an evidence-based data-driven approach and minimal burden due to effective workflow integration (Planning quality). However, some patient population specific concerns about certain medications were raised, commonly concerning atypical opioids in obstetric patients and non-steroidal anti-inflammatory drugs in comorbid patients (Patient needs and resources).
Patient Education
Lack of role clarity and resourcing impacted negatively on patient education regarding discharge opioid use and handling. There was a general lack of role clarity regarding direct patient education (Planning quality). JMOs have less of a role in patient education regarding post-discharge opioid use and handling than participants in other clinical positions (Prespecified factor: Clinical role). Resourcing was a significant barrier to patient education identified by pain specialists and nurses (Resourcing). However, various opportunities in the patient journey were identified to improve opioid education (Planning quality). At Hospital C, patient opioid education was reported to be routinely performed in the preadmission clinic, facilitated by an elective surgical caseload. In the hospitals with a more significant burden of acute care, the Acute Pain Service had a more substantial role in education in the postoperative period (Implementation climate). Resourcing in terms of access to pain specialists and nurses and the inpatient load were barriers to accomplishing patient education (Resourcing). Pharmacists had an established role in patient medication education and found the program materials valuable (Knowledge and Beliefs).
Provider Education
Provider knowledge of the program was impacted by position in the hospital hierarchy, but a sense of lack of resources transcended this. Awareness of the perioperative opioid stewardship program among the participants was generally suboptimal (Planning quality). The JMOs understood the program’s concepts and importance. However, it was uncommon for them to know that a perioperative opioid stewardship program had been introduced (Prespecified factor: Clinical role). The pain specialists and nurses involved in staff education for the program raised concerns such as staff turnover and workload. Concern about inadequate resourcing was a matter of crucial relevance raised by all health services stakeholders (Resourcing) and negatively impacted attempts to sustain the program. Examples of this included pain specialists delivering education sessions for their health services during non-work days or multiple times a year; pharmacists educating colleagues and attending program meetings outside of their official role in their organisation; and pain nurses supporting various clinical roles in the hospital (JMOs, graduate nurses, pharmacy interns) regarding opioid stewardship without any additional staffing. For the JMOs, the daily workload was a barrier to attending formal education sessions and, consequently, to awareness of and compliance with the opioid stewardship program (Implementation climate). A key promoter of program integration into everyday work at all seniorities and across all roles was the perception of importance to the organisational, or unit, leadership. A vital program driver was the desire to meet the goals of the next level in the health service hierarchy – JMOs seeking approval from their registrars and consultants in particular, but also managers assisting with hospital executive goals (Leadership engagement).
Discharge Communication
Hospital-community prescriber communication was variable but generally limited to written discharge summaries rather than a comprehensive, personalised approach. We found that the reported communication from hospital to community varied substantially with health service and clinician assessment of the needs of their patients. Generally, participants said that routine surgical patients did not have hospital-community prescriber communication beyond the hospital discharge summary. Commonly, it was expressed that this approach was likely adequate for most patients. For more complex patient situations, communication with community prescribers varied between including information on the discharge summary, a customised pain service letter and a phone call (Discharge communication). However, several participants expressed concerns about this aspect of opioid stewardship being inadequately executed (Patient needs and resources).
Program Implementation
Perioperative opioid stewardship program implementation is impacted by perceived relevance, health service organisation and case mix. Inadequate resourcing was a universal barrier identified by those in all clinical roles across all participating health services (Resourcing). For pain medicine specialists and nurses, pharmacists and JMOs at Hospitals A and C, competing workload demands resulted in a lack of capacity to drive or execute the program despite universal recognition of its importance. Hospital B’s pharmacists and pain nurses expressed the view that suboptimal perioperative opioid use was uncommon in their patients. However, pain specialists at Hospital B held the opposing view (Patient needs and resources; prespecified factors: clinical role and health service).
Organisational level reflections were commonly expressed by the anaesthetist department leads, managers, and pain specialists but not those in other positions. Participants working at Hospital A expressed some difficulties with hospital management in attempting to introduce program components such as clinical guidelines and patient education materials (Leadership Engagement). The large size of the organisation, its multiple autonomous departments and the distinct workflows interfacing with the program were also perceived as barriers (Compatibility). Those at Hospital C reported that being a smaller organisation and having close relationships between the surgical and pain clinicians were promoters of effective change (Culture). Mainly serving a young and healthy patient population whose care was amenable to standardisation was identified as a promoter by the Hospital B participants (Patient needs and resources). However, their sizeable surgical caseload relative to hospital size and pain clinician staffing was reported to hinder engagement (Compatibility). An additional concern regarding perioperative opioid stewardship programs was the potential for harm with undue restriction of analgesia with worse long-term patient pain outcomes (Patient needs and resources).
The idealised characteristics of the program leader included helpful features such as enthusiasm, expertise and understanding of the local organisational culture. Undesirable features for program leaders included using “external fixers”, perceiving an ulterior motive for the change and having a confrontational interpersonal style (Change leaders). The value ascribed to these traits was consistent for participants across all health services and clinical roles.
Sustainability and Optimisation
The participants made many suggestions about sustaining, improving and extending the perioperative opioid stewardship program components in their workplace. Integration into the usual workflow was a promoter of program sustainment identified by participants in all clinical roles (Prespecified factor: clinical role). If the action to accomplish a program component was outside of routine duties and required explicit recall and effort, then it was less likely to be sustained over time (Reflecting and evaluating). Many participants identified the EMR as a significant opportunity to embed the program into everyday work and to assist with increasing efficiency (Electronic Medical Record; Compatibility). Some program components were reportedly much more accessible after the EMR’s introduction (Reflecting and evaluating; Electronic Medical Record). Hospital-community prescriber communication, patient education and adherence to the discharge prescription guideline were commonly reported to be most amenable to EMR support.
Discussion
Our study evaluated perioperative opioid stewardship program implementation components, overall and individually, by garnering the perspectives of healthcare worker stakeholders across three different health services. Additionally, we obtained their insights into program sustainment and suggestions for program improvements that would be feasible in their work environments.
The intervention characteristics domain of the CFIR did not emerge as an essential study theme. This was likely because the perioperative opioid stewardship intervention was introduced with core pillars to be adapted to the individual health service workflows by the local program lead. Therefore, external imposition, adaptability, complexity and presentation considerations were suited to local requirements whilst remaining within the whole program framework. Evaluation of the implementation soon after the program introduction may have better captured these negotiations. However, our evaluation was more distant, and the dominant findings related to the ongoing program work and reflections for future iterations.
Inner setting CFIR constructs emerged as particularly important for assessing the implementation of perioperative opioid stewardship programs across our three target health services. This is consistent with a previous report of a weight management program introduced across five sites where inner setting factors best explained the variation in reported implementation success (Damschroder & Lowery, 2013). In our study, within the CFIR inner setting domain, the themes of compatibility, implementation climate and resourcing were strongly represented across the health services and clinical roles. When participants reported the program elements positively across these factors, it was a promoter of both program implementation and sustainment. The inverse was true when these themes were reported negatively as barriers. Program resourcing was a barrier to implementation and sustainment reported across the health services and clinical roles. As has been found by others undertaking program evaluation (Damschroder & Lowery, 2013), leadership engagement was linked to resourcing. In our study, this relationship was perceived as so important that a commonly suggested strategy to optimise the program was to improve top-down endorsement as a driver of enhanced engagement and compliance.
The JMOs, as the predominant discharge opioid prescribers, provided crucial insights into how the program was implemented, especially regarding the discharge prescription guidance and integration with existing workflows. Regardless of health service, their work demands were high, so compatibility was essential to program execution. Their explicit knowledge of the program and its components was low, potentially indicating gaps in the program provider’s engagement or education delivery. Nevertheless, the program principles of limiting and individualising opioid prescribing and maximising adjunct analgesia were embedded in their accounts of routine practice. This was evidenced by the post-program cohort finding that 78% of discharge prescribing was guideline-compliant (Allen et al., 2023). The co-prescription of paracetamol to 91% and anti-inflammatory drugs to 64% of the cohort was consistent with accounts, particularly from pain specialists, that paracetamol was acceptable, but there was some resistance to anti-inflammatory drugs at the health services. Guideline compliance, including adjunct co-prescribing, could be further optimised by EMR order set review and alignment with the program recommendations. The suggestions of JMOs of ensuring program usability and that senior staff endorse the program present opportunities for future interventions.
Our study identified that hospital-community prescriber communication was challenging due to no clear workflow intervention point, a time-pressured work context, and differing processes between health services. An additional reported barrier to this component being effectively implemented was the perception of JMOs that their consultants did not value the time they spent on this task. The EMR was introduced to the health services after the perioperative opioid stewardship program. Participants across health services and clinical roles made many suggestions for optimising hospital-community communication by harnessing the capability of the EMR. This represents a significant opportunity to improve on this poorly integrated program component.
Using the EMR to optimise perioperative opioid practice, as suggested by our participants, is supported by an evidence base in medication stewardship and addiction treatment. In a primary care quality improvement study for alcohol screening, EMR support improved compliance and patient blood pressure management (Rose et al., 2008). This suggests that the EMR may have potential as a support tool for preadmission opioid screening as an extension of the current program. Antimicrobial stewardship is better established than opioid stewardship, but these programs face similar challenges and opportunities. In antimicrobial stewardship, EMR support for multiple program components has been advocated, with the alteration of prescriber behaviour a key target (Parzen-Johnson et al., 2021). The EMR can improve antimicrobial prescriber behaviour with intervention from suggestions (e.g., best practice advisories) to restrictions (e.g., hard stops). Our participants suggested these as potential program optimisations, and proof-of-concept in antimicrobial stewardship programs adds credence to their application to opioid stewardship. An ongoing primary care trial aims to avoid opioid analgesia in opioid naïve patients and to taper opioid therapy in those with high opioid use through EMR interventions (Vock et al., 2022). A similar study in a hospital inpatient setting would be a welcome extension to our work.
A US study has reported the potential barriers to implementing an opioid stewardship program from the healthcare provider’s perspective (Coughlin et al., 2019). Their program comprised similar components to ours, including patient and prescriber education. Commonalities with our study included findings that time and resource constraints were a significant concern for effective implementation (Coughlin et al., 2019). However, they found significant concerns for patient satisfaction scores and remuneration implications (External policy and incentives). Our study was conducted in state-funded Australian hospitals, where most patients receive free care, highlighting the importance of local context program evaluation. Additionally, the US program evaluation was conducted before implementation, so the conclusions were based on potential issues that stakeholders envisaged, whilst ours explored the impediments clinicians experienced in introducing and sustaining the program.
Clinical practice guidelines make evidence-based or expert consensus recommendations to reduce individual practitioner variation and nudge towards current best practices. Perioperative opioid stewardship has benefited from the release of relevant local (Australian and New Zealand College of Anaesthetists, 2022) and international (Clarke et al., 2020; Hyland et al., 2021; Levy et al., 2021a, b) guidelines. However, diffusion of innovation, even if acceptable and easily integrated into practice, takes time. Health policy and regulation are potent levers for clinical change that can more rapidly shift practice. The Australian opioid analgesic stewardship in acute pain clinical care standard (Australian Commission on Safety and Quality in Health Care, 2022) was released at the end of the data collection period for our study. Therefore, the impact on perioperative practice from the healthcare worker’s perspective was not fully captured and could be investigated in future work.
The insights we gained from our study findings inform strategies that may be used to overcome the barriers and capitalise on the promotors of successful opioid stewardship program implementation. We found the health service’s overall workload and capacity to undertake the proposed change were significant factors that could act as barriers or promotors of success. Allocating clear responsibilities for program components and securing the necessary resources at the outset to accomplish the required work was critical for successful implementation. Planning the intervention to align with evidence-based practice and local factors through early stakeholder consultation was also crucial. Facility leadership endorsement of workflow changes from the outset supported successful implementation. It was essential for the uptake by more junior staff that their immediate superiors were committed to the program. Additionally, proactive integration of changes into the usual workflow to minimise burden was vital. While our insights have been derived from the implementation of the perioperative opioid stewardship program, it’s important to note that many of the findings are not program-specific. Therefore, the strategies outlined above may apply to various clinical change programs.
Our study effectively mapped the components of the perioperative opioid stewardship program to the CFIR domains and themes in a framework template analysis, considering both barriers and promoting factors. The CFIR targets individuals who influence the implementation’s outcome and is widely used in implementation science. From the methodology we successfully used in this study, when the CFIR is to be applied for framework analysis, consideration should be given to exploring the study participants’ suggestions for optimising and sustaining the intervention. This approach successfully leverages the end-user insights into the implementation and efficiently gathers inputs for program maintenance and modification. This is a valuable extension to standard CFIR-guided framework analysis.
Strengths
Our study addressed an important topic with limited existing evidence and included representatives from the target clinical roles and across the different health services. The clinician participants illuminated the impact of the perioperative opioid stewardship program on complex health service workflows. These insights contextualise the findings from the post-program patient cohort study (Allen et al., 2023). The sample size was sufficient for exploring barriers and promotors from various perspectives and for achieving thematic saturation. Further, the CFIR was well suited to our evaluation. We considered our prespecified contextual factors and all of the CFIR constructs whilst maintaining the flexibility for novel themes to emerge from the dataset. Seeking participant reflections on sustaining and improving the program was a novel and valuable inclusion. The rigorous methodology and general findings may be widely applied to the implementation and sustainment of other clinical programs.
Limitations
Interviews were conducted by a single investigator (MLA) who was involved in the perioperative opioid stewardship program development and had previous professional interactions with several of the study participants. This preexisting relationship could have constrained participants from providing candid negative responses about the program. Whilst this investigation into the implementation of an opioid stewardship program in three Australian health services adds to our knowledge base, the themes that have emerged may not necessarily be generalised beyond the practice context, which is a known limitation of qualitative analysis. The interviews were conducted more distantly from the program introduction than planned initially due to the COVID-19 pandemic and its disruption of health service workflows and research activity. This may have limited participants’ recall of the critical barriers and promoters for program implementation. However, the revised timeframe presented an opportunity to consider program sustainment comprehensively. In our study, only health service employees were recruited, so the patient perspective on perioperative opioid stewardship programs remains unexplored and warrants investigation.
Conclusions
Opioid stewardship programs are an essential mechanism for harnessing the benefits of adequate analgesia and mitigating harm in the perioperative period. However, they occupy a precarious location in clinical practice as restriction of discharge analgesia without reasonable rescue contingencies could leave patients with poor pain control. This study adds to the literature by increasing our understanding of promoters and barriers to implementing and sustaining opioid stewardship measures from the perspective of healthcare worker stakeholders. The insights from this study provide targets for future program optimisation and a starting point for promoting effective clinical change. Whilst healthcare workers are critical stakeholders in the clinical change process, the roles of patient consumers and the impact of health policy and regulation are areas for further investigation into perioperative opioid stewardship programs in Australia.
Data Availability
The datasets generated and analysed during the current study are not publicly available per the conditions of the ethics approval for this project. Still, they may be available from the corresponding author on reasonable request and subject to the local Office for Research approval.
References
Alexander, J. A., & Hearld, L. R. (2012). Methods and metrics challenges of delivery-system research. Implementation Science, 7(1), 15. https://doi.org/10.1186/1748-5908-7-15.
Allen, M. L., Kim, C. C., Braat, S., Jones, K., Winter, N., Hucker, T. R., Chia, A., Lang, C., Brooks, S. L., & Williams, D. L. (2020). Post-discharge opioid use and handling in surgical patients: A multicentre prospective cohort study. Anaesthesia and Intensive Care, 48(1), 36–42. https://doi.org/10.1177/0310057X19895019.
Allen, M. L., De Silva, A. P., Braat, S., Jones, K., Chia, A., Hucker, T. R., Brooks, S. L., Hogg, M., Lee, C. W., Williams, D. L., & Kim, C. C. (2023). Post-surgical discharge opioid prescribing, use and handling after introduction of a stewardship program. Anaesthesia and Intensive Care, 51(4), 239–253. https://doi.org/10.1177/0310057X231160800.
Australian Commission on Safety and Quality in Health Care (2022). Opioid analgesic stewardship in acute pain clinical care standard - acute care edition. https://www.safetyandquality.gov.au/standards/clinical-care-standards/opioid-analgesic-stewardship-acute-pain-clinical-care-standard.
Australian and New Zealand College of Anaesthetists (2022). PS41(G) Position statement on acute pain management, Faculty of Pain Medicine, ANZCA. Retrieved 28th Feburary 2023 from https://www.anzca.edu.au/getattachment/558316c5-ea93-457c-b51f-d57556b0ffa7/PS41(G)-Position-statement-on-acute-pain-management-2022-PILOT#page=.
Blanch, B., Pearson, S. A., & Haber, P. S. (2014). An overview of the patterns of prescription opioid use, costs and related harms in Australia. British Journal of Clinical Pharmacology, 78(5), 1159–1166. https://doi.org/10.1111/bcp.12446.
Brat, G. A., Agniel, D., Beam, A., Yorkgitis, B., Bicket, M., Homer, M., Fox, K. P., Knecht, D. B., McMahill-Walraven, C. N., Palmer, N., & Kohane, I. (2018). Postsurgical prescriptions for opioid naive patients and association with overdose and misuse: Retrospective cohort study. Bmj, 360, j5790. https://doi.org/10.1136/bmj.j5790.
Brooks, J., & King, N. (2014). Doing template analysis: Evaluating an end of life care service. In. Sage research methods cases. https://doi.org/10.4135/978144627305013512755.
CFIR guide (2009). 2009 CFIR constructs. Retrieved 13th June, 2023 from https://cfirguide.org/constructs-old/.
Chou, R., Turner, J. A., Devine, E. B., Hansen, R. N., Sullivan, S. D., Blazina, I., Dana, T., Bougatsos, C., & Deyo, R. A. (2015). The effectiveness and risks of long-term opioid therapy for chronic pain: A systematic review for a National Institutes of Health Pathways to Prevention Workshop. Annals of Internal Medicine, 162(4), 276–286. https://doi.org/10.7326/M14-2559.
Clarke, H. A., Manoo, V., Pearsall, E. A., Goel, A., Feinberg, A., Weinrib, A., Chiu, J. C., Shah, B., Ladak, S. S. J., Ward, S., Srikandarajah, S., Brar, S. S., & McLeod, R. S. (2020). Consensus statement for the prescription of pain medication at discharge after elective adult surgery. Can J Pain, 4(1), 67–85. https://doi.org/10.1080/24740527.2020.1724775.
Coughlin, J. M., Shallcross, M. L., Schafer, W. L. A., Buckley, B. A., Stulberg, J. J., Holl, J. L., Bilimoria, K. Y., & Johnson, J. K. (2019). Minimizing opioid prescribing in surgery (MOPiS) Initiative: An analysis of implementation barriers. Journal of Surgical Research, 239, 309–319. https://doi.org/10.1016/j.jss.2019.03.006.
Damschroder, L. J., & Lowery, J. C. (2013). Evaluation of a large-scale weight management program using the consolidated framework for implementation research (CFIR). Implementation Science, 8(1), 51. https://doi.org/10.1186/1748-5908-8-51.
Damschroder, L. J., Aron, D. C., Keith, R. E., Kirsh, S. R., Alexander, J. A., & Lowery, J. C. (2009). Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement Sci, 4(1), 50. https://doi.org/10.1186/1748-5908-4-50.
Damschroder, L. J., Reardon, C. M., Widerquist, M. A. O., & Lowery, J. (2022). The updated consolidated framework for implementation research based on user feedback. Implement Sci, 17(1), 75. https://doi.org/10.1186/s13012-022-01245-0.
Guest, G., Bunce, A., & Johnson, L. (2006). How many interviews are enough? An experiment with data saturation and variability. Field Methods, 18(1), 59–82.
Hyland, S. J., Brockhaus, K. K., Vincent, W. R., Spence, N. Z., Lucki, M. M., Howkins, M. J., & Cleary, R. K. (2021). Perioperative pain management and opioid stewardship: A practical guide. Healthcare (Basel), 9(3). https://doi.org/10.3390/healthcare9030333.
Keith, R. E., Crosson, J. C., O’Malley, A. S., Cromp, D., & Taylor, E. F. (2017). Using the Consolidated Framework for Implementation Research (CFIR) to produce actionable findings: A rapid-cycle evaluation approach to improving implementation. Implementation Science, 12(1), 15. https://doi.org/10.1186/s13012-017-0550-7.
King, N. (2012). Doing template analysis. In G. Symon, & C. Cassell (Eds.), Qualitative organizational research: Core methods and current challenges (1 ed.). SAGE Publications, Inc. https://doi.org/10.4135/9781526435620.
Levy, N., Lord, L. J., & Lobo, D. N. (2021). UK recommendations on opioid stewardship. Bmj, 372, m4901. https://doi.org/10.1136/bmj.m4901.
Levy, N., Quinlan, J., El-Boghdadly, K., Fawcett, W. J., Agarwal, V., Bastable, R. B., Cox, F. J., de Boer, H. D., Dowdy, S. C., Hattingh, K., Knaggs, R. D., Mariano, E. R., Pelosi, P., Scott, M. J., Lobo, D. N., & Macintyre, P. E. (2021b). An international multidisciplinary consensus statement on the prevention of opioid-related harm in adult surgical patients. Anaesthesia, 76(4), 520–536. https://doi.org/10.1111/anae.15262.
Lumivero (2022). Version 12 for Mac. https://lumivero.com/products/nvivo/.
Macintyre, P. E., Huxtable, C. A., Flint, S. L., & Dobbin, M. D. (2014, Sep). Costs and consequences: A review of discharge opioid prescribing for ongoing management of acute pain. Anaesthesia and Intensive Care, 42(5), 558–574. https://doi.org/10.1177/0310057X1404200504.
Parzen-Johnson, S., Kronforst, K. D., Shah, R. M., Whitmer, G. R., Scardina, T., Chandarraju, M., & Patel, S. J. (2021). Use of the electronic health record to optimize antimicrobial prescribing. Clinical Therapeutics, 43(10), 1681–1688. https://doi.org/10.1016/j.clinthera.2021.09.009.
Romney, A. K., Weller, S. C., & Batchelder, W. H. (1986). Culture as consensus: A theory of culture and informant accuracy. American Anthropologist, 88(2), 313–338. http://www.jstor.org/stable/677564.
Rose, H. L., Miller, P. M., Nemeth, L. S., Jenkins, R. G., Nietert, P. J., Wessell, A. M., & Ornstein, S. (2008). Alcohol screening and brief counseling in a primary care hypertensive population: A quality improvement intervention. Addiction, 103(8), 1271–1280. https://doi.org/10.1111/j.1360-0443.2008.02199.x.
Roxburgh, A., & Burns, L. (2017). Accidental drug-induced deaths due to opioids in Australia, 2013. National Drug and Alcohol Research Centre. Retrieved 12th April 2021 from https://ndarc.med.unsw.edu.au/sites/default/files/ndarc/resources/OpioidDeaths_2013_Website_FINAL_0.pdf.
Roxburgh, A., Bruno, R., Larance, B., & Burns, L. (2011). Prescription of opioid analgesics and related harms in Australia. Medical Journal of Australia, 195(5), 280–284. https://doi.org/10.5694/mja10.11450.
Shah, A., Hayes, C. J., & Martin, B. C. (2017). Characteristics of initial prescription episodes and Likelihood of long-term opioid use - United States, 2006–2015. Mmwr. Morbidity and Mortality Weekly Report, 66(10), 265–269. https://doi.org/10.15585/mmwr.mm6610a1.
Sonix Inc (2022). https://Sonix.ai.
Stanley, B., Collins, L., Norman, A., Bonomo, A., & Bonomo, Y. (2022). Reducing opioid prescribing on discharge after orthopaedic surgery: Does a guideline and education improve prescribing practice 1 year later? Anz Journal of Surgery, 92(5), 1171–1177. https://doi.org/10.1111/ans.17557.
Suckling, B., Pattullo, C., Liu, S., James, P., Donovan, P., Patanwala, A., & Penm, J. (2022). Persistent opioid use after hospital discharge in Australia: A systematic review. Australian Health Review, 46(3), 367–380. https://doi.org/10.1071/ah21353.
Tomoaia-Cotisel, A., Scammon, D. L., Waitzman, N. J., Cronholm, P. F., Halladay, J. R., Driscoll, D. L., Solberg, L. I., Hsu, C., Tai-Seale, M., & Hiratsuka, V. (2013). Context matters: The experience of 14 research teams in systematically reporting contextual factors important for practice change. The Annals of Family Medicine, 11(Suppl 1), S115–S123.
Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19(6), 349–357. https://doi.org/10.1093/intqhc/mzm042.
Vock, D. M., Neprash, H. T., Hanson, A. V., Elert, B. A., Satin, D. J., Rothman, A. J., Short, S., Karaca-Mandic, P., Markowitz, R., Melton, G. B., & Golberstein, E. (2022). PRescribing interventions for chronic pain using the electronic health record (PRINCE): Study protocol. Contemporary Clinical Trials, 121, 106905. https://doi.org/10.1016/j.cct.2022.106905.
Zoom (2022). Zoom Video Communications Inc. https://zoom.us.
Acknowledgements
None.
Funding
No funds, grants or other support was received.
Open Access funding enabled and organized by CAUL and its Member Institutions
Author information
Authors and Affiliations
Contributions
MLA conceptualised and designed the study, wrote the protocol, obtained regulatory approvals, undertook recruitment and data collection, analysed and interpreted the data and wrote and revised the manuscript. KS analysed and interpreted the data and revised the manuscript. KL conceptualised and designed the study, revised the protocol and revised the manuscript. JAMN conceptualised and designed the study, revised the protocol and revised the manuscript. All authors have reviewed and approved the submitted version of the manuscript and are accountable for the entirety of the submission.
Corresponding author
Ethics declarations
Ethics Approval
The procedures used in this study adhere to the tenants of the Declaration of Helsinki. Before the study commenced, the necessary ethics and governance approvals were obtained from the Melbourne Health Office for Research (MH_HREC_2020.26/17092020).
Consent
Written informed consent for participation was obtained by all interview subjects, including for audio-visual recording and publication of de-identified data. Consent for the publication of de-identified data was obtained from participants. No individually identifiable data was included in the manuscript.
Competing Interests
The authors declare that they have no financial or non-financial interests to disclose.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Allen, M.L., Somasundaram, K., Leslie, K. et al. Perioperative Opioid Stewardship Program: Barriers and Promotors of Implementation and Sustainability. Glob Implement Res Appl (2024). https://doi.org/10.1007/s43477-024-00124-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s43477-024-00124-8