
Abstract
Fast, precise, and low-cost diagnostic testing to identify persons infected with SARS–CoV-2 virus is pivotal to control the global pandemic of COVID-19 that began in late 2019. The gold standard method of diagnostic recommended is the RT-qPCR test. However, this method is not universally available, and is time-consuming and requires specialized personnel, as well as sophisticated laboratories. Currently, machine learning is a useful predictive tool for biomedical applications, being able to classify data from diverse nature. Relying on the artificial intelligence learning process, spectroscopic data from nasopharyngeal swab and tracheal aspirate samples can be used to leverage characteristic patterns and nuances in healthy and infected body fluids, which allows to identify infection regardless of symptoms or any other clinical or laboratorial tests. Hence, when new measurements are performed on samples of unknown status and the corresponding data is submitted to such an algorithm, it will be possible to predict whether the source individual is infected or not. This work presents a new methodology for rapid and precise label-free diagnosing of SARS-CoV-2 infection in clinical samples, which combines spectroscopic data acquisition and analysis via artificial intelligence algorithms. Our results show an accuracy of 85% for detection of SARS-CoV-2 in nasopharyngeal swab samples collected from asymptomatic patients or with mild symptoms, as well as an accuracy of 97% in tracheal aspirate samples collected from critically ill COVID-19 patients under mechanical ventilation. Moreover, the acquisition and processing of the information is fast, simple, and cheaper than traditional approaches, suggesting this methodology as a promising tool for biomedical diagnosis vis-à-vis the emerging and re-emerging viral SARS-CoV-2 variant threats in the future.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
After reaching the status of a pandemic, the new coronavirus variant 2 (SARS-CoV-2), the etiological agent of the 2019 coronavirus infectious disease (COVID-19), has infected more than two hundred million individuals and caused over five million deaths worldwide (https://covid19.who.int). In order to mitigate the effects of the related morbidity of COVID-19, there is a substantial need for improved population-scale testing solutions to early identify infection and thus allow adequate tracking [1]. New diagnosis techniques that are fast, accurate, and low-cost will not only help the management of the current crisis, but also serve as a baseline for the development of multiplex technology that will be useful in the response to future epidemics. Presently, most diagnostic methods involve sampling and testing different fluids like nasopharyngeal cell lysate, saliva, or blood.
Infections of SARS-CoV-2 in the initial stage are currently identified using real-time quantitative polymerase chain reaction (RT-qPCR) assays, considered the Gold Standard method, which may require up to 3 days after infection for a reliable positive signal [2]. In addition, RT-qPCR tests require between 3 to 4 h to be concluded [3] and are hardly used on a daily basis due to their elevated cost, shortages in biomarkers, and key reagents.
Intermediate stage or past infections are investigated using serum-based testing methods such as enzyme-linked immunosorbent assays (ELISAs), lateral flow immunoassays (LFIAs), or chemiluminescent immunoassays (CLIAs). These tests normally detect a significant and measurable concentration of immunoglobulin G (IgG) and immunoglobulin M (IgM) antibodies in blood samples. However, the build-up of such antibodies in the blood is slow, thus concentrations of IgG and IgM are measurable by these methods only after 2 weeks of infection [4]. Sensitive and specific serological methods are not fast, requiring 4 to 6 h to be completed [3]. Moreover, since most infections become apparent only upon symptom onset, the current methods of testing are unlikely to identify pre-symptomatic carriers. It is estimated that as many as 50% of individuals infected with SARS-CoV-2 are asymptomatic, hampering early-stage interventions that reduce transmission [5, 6]. There is also a large number of unreported infection cases and COVID-19-related deaths [7].
In this regard, appropriate clinical samples are essential to produce reliable results for the diagnosis of infection with SARS-CoV-2. For primary diagnostic assessment for current SARS-CoV-2 infection, the Center for Disease Control and Prevention (CDC) recommends collecting and testing an upper respiratory specimen, which includes sputum, bronchoalveolar lavage, and tracheal aspirate samples [8]. Considering that the virus does not produce or poorly induces viremia, it is essential to search for the virus in the local infection milieu. As such, fast, accurate and inexpensive methods for the early detection of SARS-CoV-2 in sputum, bronchoalveolar lavage, and tracheal aspirate samples in real time are urgently needed.
Emerging optical methods have been proposed for the detection of virus diseases [9]. Such methods usually detect labeled samples or use laser-based expensive and complex measurement techniques [9]. However, efforts to implement fast and sensitive diagnostic approaches have emerged in response to the current health crisis, as key steps to control the pandemic as well as part of reopening strategies [10]. Although the combination of RT-qPCR and serological tests such as ELISA are ideal for an accurate diagnosis, the detection of antibodies is particularly relevant during later transmission [11]. Thus, a fast and label-free methodology for COVID-19 diagnosis during the first days after infection is desirable.
Here, we report the use of a patent-pending [12,13,14] label-free optical spectroscopic method of straightforward operation, combined with machine learning (ML) processing of the acquired spectroscopic data, as a new diagnostic method of SARS-CoV-2. Using inactivated nasopharyngeal swab samples from RT-qPCR tested individuals, as well as inactivated tracheal aspirate from intubated patients, we show that this patent-pending multiplex method can be used to detect diseased individuals in less than 15 min, with elevated accuracy, and at a very low cost.
Methods
Study design and overview
We investigated whether optical spectroscopy data of nasopharyngeal swab and tracheal aspirate samples could be effectively used to detect SARS-CoV-2 infection with the aid of machine learning methods and without the use of biomarkers, in a fast and accurate way. Figure 1 shows an overview of the study process, divided into four steps: participant recruitment, collection of nasopharyngeal swab or tracheal aspirate samples, optical spectroscopy, and machine learning modeling.

Overview of the study process. a Enrollment. b Collection of nasopharyngeal swab or tracheal aspirate samples. c Optical spectroscopy measurements. d The algorithm was trained to predict the probability of a patient by COVID-19
Participant recruitment
The samples used in this research were collected from nasopharynx swabs of 152 patients suspected of SARS-CoV-2 infection, from asymptomatic individuals and from mildly symptomatic non-hospitalized patients. In addition, tracheal aspirate samples from 12 healthy patients and 12 critically ill COVID-19 patients, aged from 18 to 80 years old, 14 males and 10 females, under mechanical ventilation at the Intensive Care Unit of Risoleta Tolentino Neves Hospital were also studied.
The use of these samples was approved by the Ethical Committee (CAAE: 32,113,420.6.0000.5149; 1,686,320.0.0000.5149) from Universidade Federal de Minas Gerais (UFMG). Sensitive information was duly anonymized. All procedures followed ethical guidelines in accordance with Brazilian national regulations.
Collection of nasopharyngeal swab samples
Nasopharyngeal and oropharyngeal swab samples were collected from participants by inserting a rayon swab with a plastic shaft into the nostril, parallel to the palate, and gently scraped for a few seconds to absorb secretions. Another swab was shafted into the tonsils for sample collection. Next, the swabs were immediately merged into a sterile tube containing 2 mL of guanidine isothiocyanate solution. RNA extracted from all samples was tested by RT-qPCR using probes for viral and human genes. RT-qPCR was performed at the Vaccine Technology Center (CTVacinas) of the Universidade Federal de Minas Gerais to allow a definitive diagnosis of SARS-CoV-2 infection. Ground truth categorization of swab samples into negative (78) versus positive (74) SARS-CoV-2 infection was based on PCR results. Further details of the RT-qPCR results can be found in the Supplementary Information.
Collection of tracheal aspirate samples
Tracheal aspirate (TA) samples (2–10 mL) were collected during the early morning routine of COVID-19 patients. All patients included in the study tested positive for SARS-CoV-2 by RT-qPCR targeting the E gene. Only secretive productive patients were included in the study. Samples were aspirated into sterile tracheal secretion collectors and immediately processed in a biosecurity level 3 laboratory.
Optical spectroscopy measurements
For the optical measurements, each nasopharyngeal swab or tracheal aspirate sample was thawed and homogenized by spinning for 1 min, at room temperature and 1200 rpm. Next, 10 µL of the sample was deposited on a 22 mm × 22 mm glass #1½ coverslip (Corning, USA) and covered with a second coverslip. The sandwich samples were studied by ellipsometry in the 245–1690 nm wavelength range, with incidence angle varying from 45 to 70° in 5-degree steps. The measurements were repeated in 9 different regions of approximately 3 mm × 6 mm of each slide, organized as a 3 × 3 rectangular mesh, in order to account for possible spatial inhomogeneities across the samples.
Development of the machine learning model
The measured data was used to train a machine learning model to identify SARS-CoV-2 infected patients. This model was specifically trained to predict the infection status for each of the distinct positions read from the individual slides. The patient’s final diagnosis was defined by the average infection probability of all positions in the slide. An average probability below 0.5 meant a negative diagnostic, being positive otherwise.
Model design was performed in three stages: feature treatment/model type selection, training with data augmentation, and model tuning. Throughout, model quality was assessed by accuracy, precision, recall, F1, and ROC-AUC scores in a test set, determined at the patient level. F1 was chosen as the reference metric for optimization.
In the first stage of model design, the pipeline consisted of the following sequential steps: manual variable selection, manual feature selection, scaling preprocessing, methods of outlier detection and removal, automatic feature selection, and model type selection. These steps aimed to recognize the variables, features, and preprocessing procedures that would yield the best models. For manual variable selection, we considered the variables related to experimental design. The angles of incidence were tried individually (45, 50, 55, 60, 65, and 70°) and combined (all angles). Four windows of wavelength were tried: below 380 nm, between 380 and 1000 nm, above 1000 nm, and the whole range (all wavelength). Due to concerns of rapid sample degradation, as well as the will to speed up the procedure in a clinical setup, three combinations of positions were tried: positions 1–3, 1–5, and 1–9 (all positions). For manual feature selection, we used combinations of the measured ellipsometry features: angles Ψ and Δ, depolarization, intensity, and the real and imaginary parts of the complex reflectance ratio ρ = tan Ψ eiΔ. The scaling step is introduced to express all measures in a comparable scale; the methods tested were MinMaxScaler, StandardScaler, QuantileTransformer and RobustScaler, as implemented by the Python package Scikit-Learn v0.24 [15]. The outlier detection methods tested were PCA, LOF, KNN, COPOD, and IForest, with contamination rates in the range of 1 to 12.5%, as implemented by the Python package PyOD v0.8.7 [16]. Automatic feature selection was performed to rank the features according to their discriminative power. The methods tested in this step were ExtraTreesClassifier (both by Gini and entropy criteria), PCA, and LDA, as implemented by Scikit-Learn v0.24. After the features were ordered accordingly, we tried the top “n” features from a range of 20 to 500. For model type, we tested implementations of logistic regression, support vector machine, gradient boosting classifier and deep neural network (multi-layer perceptron classifier), by Scikit-Learn v0.24, and XGBoost Classifier by Python package XGBoost v1.4.0 [17].
In the second stage of model design, we tested the top performing models identified so far with a technique of data augmentation presented in [18]. The main idea of the method is to create synthetic training data by mixing the original measurements; more data tends to increase the power of generalization of the model. The synthetic data in this study was generated by averaging two measurements, making sure that only measurements from the same class and position would be mixed. The original data was also kept in the training set. The test set consisted only of original measurements.
The third and last stage consisted of tuning further the best performing models by adjusting the parameters specific to each model type. We performed an exhaustive search, tweaking some of the adjustable parameters according to each model documentation, relying once again on the data augmentation setup.
Throughout the model design protocol, models were trained with a training set and evaluated with a test set. Even though models were trained on individual positions in the slides, we made sure that the same slide would not be present in the training and test set at the same time, therefore, preventing data leakage at the patient level. These sets were generated by randomly splitting all the measurements available in a stratified fashion, reserving 20% of the patients to the test set. All metrics reported are an average of 10 such splits, produced as follows: at first, all available slides were shuffled then split into 5 folds with roughly the same size, then, this process was repeated, yielding the 10 folds reported. Therefore, each of the 2 sets of 5 splits covered the whole dataset, and each patient was evaluated twice by the same model, trained with different patients each time.
Results
Machine learning model
Figure 2 depicts the steps of data preparation related to feature selection, prior to model implementation, for the nasopharyngeal swabs. The solid lines in panels a, b, and c are the mean spectra of the physical property denoted in the y-axis, at a particular angle, measured at the wavelengths denoted in the x-axis, for all the positions in the slides. The shadow areas are the corresponding standard deviation, and the readings are separated by infection status (color coded). Each position of the slide is represented by a set of data as exemplified in Fig. 2a; such a set contains readings for 9 different physical properties (Ψ, Δ, depolarization (depol), intensity, real part of ρ, imaginary part of ρ, sin(Δ), cos(Δ), tan(Ψ)), 6 different angles (45–70°) and 674 different wavelengths, making a total of 9 × 6 × 674 = 36,396 features available as a starting point for the development of the algorithm. After the manual selection of features, each position is represented by 198 features (Fig. 2b), which contain data for one single angle (55°), one single physical property (depolarization), and a sub-range of wavelengths (above 1000 nm). Figure 2c represents the remaining features after the automatic feature selection and data scaling, where the wavelengths are ordered by their importance given by the method chosen for feature selection. At this point, 166 features remain: 166 selected wavelengths from the depolarization spectra at 55°. Figure 2d is a PCA representation of the same data shown in Fig. 2c; some patients of the same status cluster together, but not all healthy and infected individuals are clearly discriminated by the data alone. The machine learning model is responsible for this final step in the classification task.

Transformation of the data along the processing steps. a Representation of the measured data. b Data after manual feature selection. c Data after automatic feature selection and scaling. d PCA of the data at the end of feature selection
For these samples, the feature that delivered the best scores is depolarization, measured at an angle of 55°, at wavelengths above 1000 nm, and at all positions of a slide. They were scaled by the RobustScaler method. Outlier detection and removal were performed by the iForest method with a contamination rate of 10%. Samples from the test set were not evaluated for the presence of outliers, meaning that outliers were removed only from the training set. Automatic feature selection was guided by the ExtraTreesClassifier with Gini criterion, and 166 features were fed into the model. The model that yielded the best F1 score was an implementation of the MLPClassifier, from the Python package Scikit-Learn v0.24 [15], which is used to design neural networks. It contained two hidden layers with 100 neurons each. All layers were activated by the ReLU function. The solver used was SGD, with alpha of 1E-5, momentum of 0.95, and constant learning rate. This setup yielded a model able to diagnose patients with an accuracy of 85.0% (standard deviation 6.0%), F1 of 85.9% (5.4%), precision of 79.1% (7.2%), recall of 90.4% (5.4%), and ROC-AUC of 0.900 (0.045).
In the case of the tracheal samples, four features were used: Ψ, Δ, depolarization, and intensity, measured at an angle of 70°, at all wavelengths, at positions 1–3. The best scaling method was Robust Scaler, and outliers were removed by the KNN method with a contamination rate of 2.5%. Automatic feature selection was guided by the ExtraTreesClassification with Gini criterion, and the model performed best using 568 features. Due to the lower number of samples, the best results were achieved prior to the data augmentation phase. The best model was an implementation of the LogisticRegression classifier with standard parameters, as implemented by the Scikit-Learn v0.24 package [15]. The accuracy at the patient level was 97.2% (standard deviation of 5.5%), F1 was 97.2% (5.7%), precision was 96.4% (7.4%), recall was 97.2% (8.3%), and ROC-AUC was 1.0.
In the configuration of 9 measured positions and only one measured angle, we estimated a 7-min interval to carry out the measurement and classification of one sample, and less than 15 min for the overall time of the diagnosis process of one patient, including the collection of the nasopharyngeal swab samples, preparation of the sample to be measured, the optical measurements, and the AI processing of the data. The measurement and classification of the tracheal aspirate are even faster, since only 3 positions of the slide are necessary to be measured.
Discussion
The rapid spreading of the new SARS-CoV-2 virus worldwide has shown the necessity and impact of governmental restrictions, such as lockdowns, to prevent the increase in cases and the collapse of health centers [19]. Likewise, this pandemic revealed the urgent need for fast, precise, and well-timed diagnostic systems to identify and manage the treatment of infected individuals, thus hampering the effects of COVID-19. Up to now, the most applied diagnostic methods encompass RT-qPCR assay at the early stage of infection, through samples collected from nasopharyngeal and oropharyngeal swabs, and ELISA at a later stage of infection by evaluating the patient’s sera [20]. Although the elevated sensitivity of the current available tests, false positive and false negative results may occur depending on the time of infection and the quantity of viral load. For example, it may be challenging to find viral RNA in some samples due to the quality of transport and manipulation. Radiological methods such as chest computed tomography or thoracic radiography also have demonstrated remarkable signs of COVID-19 disease; however, they cannot be used for disease screening [21].
New methodologies for massive testing are available by applying LFA through different approaches, mainly using nanomaterials. Among them, an electrochemical immunoassay based on a graphene electrode was functionalized with anti-spike antibodies for the rapid detection of the SARS-CoV-2 virus via the spike surface protein [22]. Another study has proposed three-dimensional assembly of electrodes of reduced-graphene-oxide (rGO) nanoflakes immobilized with specific viral antigens integrated with a microfluidic device [23]. In addition, a rapid electrochemical detection of SARS-CoV-2 antibodies using a commercially available impedance sensing platform was also proposed, which contains sensing electrodes coated with SARS-CoV-2 spike protein and exposes samples to an anti-SARS-CoV-2 monoclonal antibody [24]. However, these technologies possess some drawbacks difficult to overcome such as automation and integration of microfluidics as well as the avoidance of nonspecific biomolecule adhesion in their systems.
Plasmonic biosensors have encouraged the development of novel approaches to achieve the effective coverage of the biological receptor while confirming the affinity and specificity of targeted viral nucleic acids, proteins, or whole virus [25]. Localized surface plasmon resonance (LSPR) has already been proposed to detect other viruses of medical interests such as dengue and Zika virus [26]. Besides, other strategies using gold nanoparticles (AuNPs) serological fast tests to identify the presence of IgM and/or IgG immunoglobulins are commercially available [27] and single-walled carbon nanotube (SWCNT)-based field-effect transistor (FET) semiconducting to detect the presence of SARS-CoV-2 antigens in clinical nasopharyngeal samples was assessed [28]. Nevertheless, most fast tests available have shown a considerable lack of specificity [29].
A more sophisticated biosensing platform was suggested by using a reverse transcription recombinase polymerase amplification (RT-RPA) coupled with clustered regularly interspaced short palindromic repeats (CRISPR-Cas12a) for the SARS-CoV-2 detection. This methodology utilizes DNA-modified gold nanoparticles (AuNPs) as a universal colorimetric readout and can specifically target the ORF1ab and N regions of the SARS-CoV-2 genome [30]. However, it is expensive and unlikely to be commercially available at large scale.
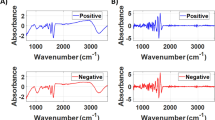
On the other hand, suggested spectroscopic techniques have demonstrated useful importance for rapid, accurate, and relatively cost-effective methods for virus detection but also for infection checking and follow-up [31, 32]. For instance, surface-enhanced Raman spectroscopy (SERS) [33], COVID-19 salivary Raman fingerprint [34], and a superfast, reagent-free, and non-destructive approach of attenuated total reflection Fourier-transform infrared (ATR-FTIR) spectroscopy [35] have already shown reliability for diagnostic applications.
The ability of monitoring potential virus mutations is essential, especially in identifying SARS-CoV-2 variants that are known to change their RNA sequence. The use of spectroscopic techniques combined with artificial intelligence models will allow detection and probably monitor and detect any changes related to this virus [36]. AI has been employed in health care fields for several proposals ranging from the prediction of disease spread trajectory to the development of diagnostic and prognostic models [37] by developing algorithms to analyze possible predictions for overall prognosis for COVID-19 patients [38]. Moreover, a machine-learning model that predicts a positive SARS-CoV-2 infection in a RT-PCR test based on symptoms was already established [39].
Despite all recent advances in diagnosis methods of SARS-CoV-2 above mentioned, there is an urgent need to develop a reagent-free, scalable, low-cost, sensitive, and specific assay for rapid detection of SARS-CoV-2 within minutes, or ideally in seconds, at the early stage of infection. Here, we have demonstrated the use of a label-free optical spectroscopy method of simple operation, combined with ML processing of the acquired raw spectroscopy data as an innovative method for SARS-CoV-2 infection detection in inactivated samples of nasopharyngeal swab and tracheal aspirate. Our methodology was validated by RT-qPCR and is applicable not only in the case of patients with mild symptoms or asymptomatic in the first stage of infection, but also to critically ill COVID-19 patients under mechanical ventilation in intensive care units. Spectroscopic data from the samples, carrying information about the dielectric properties of the sample over a broad spectral range, was acquired. Software was specifically developed to manipulate the data and process them via an artificial intelligence algorithm. Both the spectroscopic technique and the software are patent pending at this moment. One of the advantages of the present method is that the samples are not labeled or processed after collection. The samples can be measured right after collection or after several weeks of storage at − 20 °C. The volume of sample required for the test is relatively small, limited to 10 µL and dropped in between regular glass cover slides for measurements. Since the samples are inactivated at the moment of the collection, there is a very low biological risk associated with the preparation, manipulation, measurement, and later discard of the slides. The simplicity and automation of the measurements and data processing procedures avoid the necessity of highly qualified personnel. These characteristics ensure the low cost of our method. In general, the performance scores of different diagnostic tests are not comparable. Most of the scores depend on the cut-off point selection, as in the case of accuracy, selectivity, and sensitivity, for example. Other scores as the area under the receiver operating characteristic (AUC) are independent of the cut-off point selection but affected by asymmetries in the population of tested samples. However, just to put in perspective the results of our method (sensitivity of 90.4% and 97.2% for nasopharyngeal swab samples and tracheal aspirate samples, respectively), we should mention that SARS-CoV-2 detection with nasopharyngeal swabs by RT-PCR has been reported with a sensitivity of 77% [40], 63% [41], 79% [42], and 73% [43]. In addition, a processing time of less than 15 min, which can be reduced with further automation of the process, accuracy and sensitivity compatibles with the above-mentioned methods of COVID-19 diagnosis, make this solution optimal for contributing to the diagnosis of emerging infectious diseases and future pandemics of public health importance.
Our study has some limitations. The fact that nasopharyngeal swab RT-PCR sensitivity varies throughout the disease course [40] limits the external validity of our findings. A future systematic follow-up study is necessary to understand the evolution of the performance scores of our methods during the disease course. It is also possible that other pre-clinical conditions could influence the classification outcome of our method. Further studies are necessary to understand the role of infection by common diseases that produces clinical conditions like COVID-19.
Conclusion
There is a massive demand for alternative methods to detect new cases of COVID-19 as well as to investigate the epidemiology of the disease. In many countries, the importation of commercial kits poses a significant impact on their testing capacity and increases the costs for the public health system [11]. Decentralization of diagnostic testing and other technology transfer activities should be prioritized to improve accessibility in remote or isolated areas and reduce costs for the public health system [44]. Our approach demonstrates an accurate, simple, fast, label-free and cost-effective methodology for SARS-CoV-2 diagnosis.
Data Availability
All data generated or analysed during this study are available upon request.
References
Seshadri DR, Davies EV, Harlow ER et al (2020) Wearable sensors for COVID-19: a call to action to harness our digital infrastructure for remote patient monitoring and virtual assessments. Front Digit Health 2:8. https://doi.org/10.3389/fdgth.2020.00008
Sethuraman N, Jeremiah SS, Ryo A (2020) Interpreting diagnostic tests for SARS-CoV-2. J Am Med Assoc 323:2249–2251. https://doi.org/10.1001/jama.2020.8259
Kumar R, Nagpal S, Kaushik S et al (2020) COVID-19 diagnostic approaches: different roads to the same destination. VirusDis 31:97–105. https://doi.org/10.1007/s13337-020-00599-7
Cheng MP, Papenburg J, Desjardins M et al (2020) Diagnostic testing for severe acute respiratory syndrome–related Coronavirus 2: a narrative review. Ann Intern Med 172:726–734. https://doi.org/10.7326/M20-1301
Arons MM, Kelly RN, Hatfield M et al (2020) Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N Engl J Med 382:2081–2090. https://doi.org/10.1056/NEJMoa2008457
He X, Lau EHY, Wu P et al (2020) Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med 26:672–675. https://doi.org/10.1038/s41591-020-0869-5
Versiani AF, Sousa RG, Monteforte PT et al (2021) A required isolation index to support the health system during the pandemic of Covid-19 in Minas Gerais, Brazil. IEEE Lat Am Trans 19:961–969
Center for Disease Control and Prevention (2022). Interim guidelines for collecting and handling of clinical specimens for COVID-19 testing. https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html. Accessed 22 Oct 2022
Masson JF (2017) Surface plasmon resonance clinical biosensors for medical diagnostics. ACS Sens 2:16–30. https://doi.org/10.1021/acssensors.6b00763
Carvalho AF, Rocha RP, Gonçalves AP et al (2021) The use of denaturing solution as collection and transport media to improve SARS-CoV-2 RNA detection and reduce infection of laboratory personnel. Brazilian Journal of Microbiology. Braz J Microbiol 52:531–539. https://doi.org/10.1007/s42770-021-00469-4
Bagno FF, Sergio SAR, Figueiredo MM et al (2021) Development and validation of and enzyme-linked immunoassay kit for diagnosis and surveillance of COVID-19 https://doi.org/10.1101/2021.06.23.21259392
Amaral PHR, González JC, Andrade LM, Silva MIN (2020) Processo para classificação de células quanto a infecção por agentes virais e usos. Instituto Nacional da Propriedade Industrial. BR1020200249932. https://busca.inpi.gov.br/pePI/servlet/PatenteServletController?Action=detail&CodPedido=1597522&SearchParameter=BR1020200249932%20%20%20%20%20%20&Resumo=&Titulo=. Accessed 20 Oct 2022
González JC, Andrade LM, Amaral, PHR (2020) CanDLE Soft. Instituto Nacional da Propriedade Industrial. BR512020001043–1. https://busca.inpi.gov.br/pePI/servlet/ProgramaServletController?Action=detail&CodPedido=29120&SearchParameter=. Accessed 20 Oct 2022
González JC, Andrade LM, Amaral, PHR (2021) MLSerum. Coordenadoria de Transferência e Inovação Tecnológica – Universidade Federal de Minas Gerais. UFMG-CTIT 20210001. http://www.ctit.ufmg.br/. Accessed 20 Oct 2022
Pedregosa F, Varoquaux G, Gramfort A et al (2011) Scikit-learn: machine learning in python. J Mach Learn Res 12:2825–2830
Zhao Y, Nasrullah Z, Li Z (2019) PyOD: a python toolbox for scalable outlier detection. J Mach Learn Res 20:1–7
Chen T, Guestrin C (2016) XGBoost: A scalable tree boosting system. In: Krishnapuram B, Shah M (ed) Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining. ACM, New York. 785–794. https://doi.org/10.1145/2939672.2939785
Houston J, Glavin FG, Madden MG (2020) Robust classification of high-dimensional spectroscopy data using deep learning and data synthesis. J Chem Inf Model 60:1936–1954. https://doi.org/10.1021/acs.jcim.9b01037
Amaral PHR, Andrade LM, Fonseca FG et al (2020) Impact of COVID-19 in Minas Gerais, Brazil: excess deaths, sub-notified cases, geographic and ethnic distribution. Transbound Emerg Dis 68:2521–2530. https://doi.org/10.1111/tbed.13922
Yuan X, Yang C, He Q et al (2020) Current and perspective diagnostic techniques for COVID-19. ACS Infect Dis 6:1998–2016. https://doi.org/10.1021/acsinfecdis.0c00365
Adams HJA, Kwee TC, Yakar D et al (2020) Chest CT imaging signature of Coronavirus disease 2019 infection: in pursuit of the scientific evidence. Chest 158:1885–1895. https://doi.org/10.1016/j.chest.2020.06.025
Mojsoska B, Larsen S, Olsen DA et al (2021) Rapid SARS-CoV-2 detection using electrochemical immunosensor. Sensors 21:1–11. https://doi.org/10.3390/s21020390
Ali MA, Hu C, Jahan S et al (2020) Sensing of COVID-19 antibodies in seconds via aerosol jet nanoprinted reduced-graphene-oxide-coated 3D electrodes. Adv Mater 33:2006647. https://doi.org/10.1002/adma.202006647
Rashed MZ, Kopechek JA, Priddy MC et al (2021) Rapid detection of SARS-CoV-2 antibodies using electrochemical impedance-based detector. Biosens Bioelectron 171:112709. https://doi.org/10.1016/j.bios.2020.112709
Mauriz E (2020) Recent progress in plasmonic biosensing schemes for virus detection. Sensors 20:1–27. https://doi.org/10.3390/s20174745
Versiani AF, Martins EMN, Andrade LM (2020) Nanosensors based on LSPR are able to serologically differentiate dengue from Zika infections. Sci Rep 10:1–17. https://doi.org/10.1038/s41598-020-68357-9
Díaz-Badillo A, Muñoz LM, Morales-Gómez MC et al (2020) Diagnostic tests for COVID-19 detection: a hybrid methodology. Cir Cir 88:537–541. https://doi.org/10.24875/CIRU.M20000068
Shao W, Shurin MR, Wheeler SE et al (2021) Rapid detection of SARS-CoV-2 antigens using high-purity semiconducting single-walled carbon nanotube-based field-effect transistors. ACS Appl Mater Interfaces 13:10321–10327. https://doi.org/10.1021/acsami.0c22589
Low SL, Leo YS, Lai YL et al (2021) Evaluation of eight commercial Zika virus IgM and IgG serology assays for diagnostics and research. PLoS ONE 16:1–15. https://doi.org/10.1371/journal.pone.0244601
Zhang WS, Pan J, Li F et al (2021) Reverse transcription recombinase polymerase amplification coupled with CRISPR-Cas12a for facile and highly sensitive colorimetric SARS-CoV-2 detection. Anal Chem 93:4126–4133. https://doi.org/10.1021/acs.analchem.1c00013
Carvalho LFCS, Nogueira MS (2020) Optical techniques for fast screening – towards prevention of the coronavirus COVID-19 outbreak. Photodiagnosis Photodyn Ther 30:101765. https://doi.org/10.1016/j.pdpdt.2020.101765
Lukose J, Chidangil S, George SD (2021) Optical technologies for the detection of viruses like COVID-19: progress and prospects. Biosens Bioelectron 178:113004. https://doi.org/10.1016/j.bios.2021.113004
Saviñon-Flores F, Méndez E, López-Castaños M et al (2021) A review on SERS-based detection of human virus infections: influenza and coronavirus. Biosens 11:66. https://doi.org/10.3390/bios11030066
Carlomagno C, Bertazioli D, Gualerzi A (2021) COVID-19 salivary Raman fingerprint: innovative approach for the detection of current and past SARS-CoV-2 infections. Sci Rep 11:1–13. https://doi.org/10.1038/s41598-021-84565-3
Barauna VG, Singh MN, Barbosa LL et al (2021) Ultrarapid on-site detection of SARS-CoV-2 infection using simple ATR-FTIR spectroscopy and an analysis algorithm: high sensitivity and specificity. Anal Chem 93:2950–2958. https://doi.org/10.1021/acs.analchem.0c04608
Khan RS, Rehman IU (2020) Spectroscopy as a tool for detection and monitoring of Coronavirus (COVID-19). Expert Rev Mol Diagn 2:647–649. https://doi.org/10.1080/14737159.2020.1766968
Syeda HB, Syed M, Sexton KW et al (2021) Role of machine learning techniques to tackle the covid-19 crisis: systematic review. JMIR Med Inform 9:e23811. https://doi.org/10.2196/23811
Fernandes FT, Oliveira TA, Teixeira CE et al (2021) A multipurpose machine learning approach to predict COVID-19 negative prognosis in São Paulo, Brazil. Sci Rep 11:1–7. https://doi.org/10.1038/s41598-021-82885-y
Zoabi Y, Deri-Rozov S, Shomron N (2021) Machine learning-based prediction of COVID-19 diagnosis based on symptoms. npj Digit Med 4:1–5. https://doi.org/10.1038/s41746-020-00372-6
Clerici B, Muscatello A, Bai F, Pavanello D, Orlandi M, Marchetti GC, Castelli V, Casazza G, Costantino G, Podda GM (2021) Sensitivity of SARS-CoV-2 detection with nasopharyngeal swabs. Front. Public Health 8:593491. https://doi.org/10.3389/fpubh.2020.593491
Wang W, Xu Y, Gao R, Lu R, Han K, Wu G et al (2020) Detection of SARS-CoV-2 in different types of clinical specimens. JAMA 323:1843–1844. https://doi.org/10.1001/jama.2020.3786
Kucirka LM, Lauer SA, Laeyendecker O, Boon D, Lessler J (2020) Variation in false-negative rate of reverse transcriptase polymerase chain reaction–based SARS-CoV-2 tests by time since exposure. Ann Intern Med 173:262–267. https://doi.org/10.7326/m20-1495
Böger B, Fachi MM, Vilhena RO et al (2021) Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am J Infect Control 49:21–29. https://doi.org/10.1016/j.ajic.2020.07.011
EisBrenner T, Tipples G, Kuschak T, Gilmour M (2020) Laboratory response checklist for infectious disease outbreaks—preparedness and response considerations for emerging threats. Can Commun Dis Rep 46:311–21. https://doi.org/10.14745/ccdr.v46i10a01
Acknowledgements
We thank all Brazilian funding agencies CAPES-PNPD scholarship program, CNPq, and FAPEMIG.
Funding
Part of this work was supported by the Brazilian Ministry of Science, Technology, and Innovation (MCTI) through the “Rede Virus” initiative and the following individual projects: sub-rede Diagnóstico and sub-rede Laboratórios de Campanha. We also acknowledge the support of Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) though the grants APQ-00418–20, APQ-01499–21 and RED-00135–22, as well as the support of the Ministry of Education through the grant 23072.211119/2020.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Responsible Editor: Fernando R. Spilki
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ceccon, D.M., Amaral, P.H.R., Andrade, L.M. et al. New, fast, and precise method of COVID-19 detection in nasopharyngeal and tracheal aspirate samples combining optical spectroscopy and machine learning. Braz J Microbiol 54, 769–777 (2023). https://doi.org/10.1007/s42770-023-00923-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42770-023-00923-5