
Abstract
A four-session program of mindfulness and cognitive behavioral therapy (M-CBT) is a low-intensity treatment module for individuals with high cost/probability bias and social anxiety symptoms. We tested its effectiveness with 23 patients with social anxiety disorder. The patients completed a set of questionnaires that evaluated social anxiety symptoms, cost/probability bias, fear of negative evaluation from others, self-focused attention, trait mindfulness, depressive symptoms, cognitive reappraisal, and suppression at pretreatment, the time before each session of treatment, post-treatment, and follow-up. Linear mixed-effects models showed that the M-CBT was effective for social anxiety symptoms, cost/probability bias, fear of negative evaluation from others, self-focused attention, trait mindfulness, depressive symptoms, and cognitive reappraisal. The M-CBT also produced significant pre-post-improvements in social anxiety symptoms and cost bias with high effect sizes (social anxiety symptoms: d = 1.04–1.06, cost bias: d = 0.82–1.02). These results suggest that M-CBT is effective for treating social anxiety symptoms and cost bias. This study demonstrates that M-CBT is feasible and acceptable for social anxiety disorder. It may comprise a treatment module for those who do not respond to traditional cognitive behavioral therapy. Trial registration number: University Hospital Medical Information Network (UMIN CTR) UMIN000043720, Registered 23 Mar 2021.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Social anxiety disorder (SAD) is a marked and intense fear of social situations in which one may be scrutinized by others (American Psychiatric Association, 2013). SAD is highly comorbid with other anxiety and depressive disorders and is associated with significant impairment in social, educational, and occupational functioning, as well as a poorer quality of life (Acarturk et al., 2008; Stein & Kean, 2000). The most well-known and effective psychological treatment for SAD is cognitive behavioral therapy (CBT; Mayo-Wilson et al., 2014). However, many patients do not achieve clinically significant improvements even with CBT (Springer et al., 2018), and there is significant room for improvement in the treatment.
CBT programs for social anxiety target not only social anxiety but also its maintaining factors. Previous research has demonstrated that self-focused attention, cost/probability bias, and avoidance behavior are factors that maintain SAD (Clark & Wells, 1995; Hofmann & Otto, 2008; Rapee & Heimberg, 1997). According to the cognitive behavioral models of SAD (Clark & Wells, 1995; Hofmann & Otto, 2008; Rapee & Heimberg, 1997), self-focused attention plays a central role in maintaining SAD. Self-focused attention is defined as the perception of internal self-related information, including body state, thoughts, feelings, and behaviors in threatening social situations (Bögels et al., 1996; Noda et al., 2021a); it involves focusing on oneself as if through the eyes of the audience (Heimberg et al., 2014). Heightened self-focused attention positively affects cost/probability bias and contributes to the exacerbation of avoidance behavior and social anxiety (Clark & Wells, 1995; Hofmann & Otto, 2008; Rapee & Heimberg, 1997). Cost/probability bias refers to the specific negative bias in SAD. Cost bias pertains to exaggerated cost (negative valence) associated with negative social events (Foa et al., 1996); it refers to the tendency to view one’s own performance as catastrophic and believe that the worst is to come. Probability bias pertains to exaggerated estimates regarding the occurrence of negative social events (Foa et al., 1996) and refers to the tendency to predict a high likelihood of negative social consequences or events. Cost/probability bias exacerbates avoidance behavior and social anxiety (Heimberg et al., 2014; Hofmann & Otto, 2008). Avoidance behavior, which refers to actions taken to avoid situations or activities that promote fear or anxiety, increases social anxiety (Okajima et al., 2009).
Particularly, it has been suggested that reducing the cost bias enhances the effect of CBT on social anxiety (Shirotsuki et al., 2014). Foa et al. (1996) also indicated that reducing cost bias has a significant impact on improving SAD. Moscovitch et al. (2012) compared the outcomes of responders and non-responders in CBT. The responders showed significant improvement in cost bias after CBT, while non-responders did not. From these aforementioned studies, it was considered that cost bias is an important predictor in improving social anxiety.
It has been suggested that enhancing trait mindfulness may improve cost bias and SAD. Mindfulness is defined as “paying attention in a particular way—on purpose, in the present moment, and nonjudgmentally” (Kabat-Zinn, 1994, p. 4). Cardaciotto et al. (2008) found that awareness (the continuous monitoring of external stimuli and internal experience) and acceptance (a non-reactive stance toward one’s own experience) are the core components of mindfulness. Trait mindfulness is negatively correlated with social anxiety, self-focused attention, cost/probability bias, and avoidance behavior (Schmertz et al., 2012; Noda et al., 2022). Mindfulness training (MT) is an intervention technique aimed at enhancing trait mindfulness. Intervention programs built with MT as the primary intervention technique or with mindfulness as the core theory are called mindfulness-based interventions (MBIs). MBIs include mindfulness-based stress reduction (MBSR), mindfulness-based cognitive therapy (MBCT), and mindfulness- and acceptance-based group therapy (MAGT) for SAD (Liu et al., 2021). MBIs have been effective in improving social anxiety and its influencing factors (Desnoyers et al., 2017; Goldin et al., 2016; Kocovski et al., 2013; Koszycki et al., 2007; Piet et al., 2010). It has also been shown that the improvement of trait mindfulness by MBIs predicts a reduction in social anxiety (Kocovski et al., 2015). Noda et al., (2022) indicated that trait mindfulness plays a role in improving cost bias and social anxiety in the following three ways: (1) trait mindfulness affects self-focused attention, probability bias, cost bias, avoidance behavior, and social anxiety directly; (2) trait mindfulness affects cost bias via self-focused attention and probability bias; and (3) trait mindfulness affects avoidance behavior and social anxiety via cost bias.
Noda et al. (2021b) developed a four-session program of mindfulness and cognitive behavioral therapy (M-CBT) as a low-intensity treatment module for individuals with high cost/probability bias and social anxiety. The program is 90–120 min per session and is conducted in groups. Furthermore, Noda (2020) tested its effectiveness on cost bias and social anxiety with individuals who have high social anxiety in a randomized controlled trial. The results showed that the group receiving M-CBT, compared to the control group, improved significantly in cost/probability bias in the negative cognition generated when paying attention to others; fear of negative evaluation from others; depressive symptoms; trait mindfulness; and happiness (determined by a global, subjective assessment of whether one is a happy or an unhappy person). Despite the program being constructed in four sessions, high effect sizes were produced in these outcomes. However, the efficacy of M-CBT for SAD has not been studied.
The purpose of this study was to assess the feasibility and initial effectiveness of the four-session program in M-CBT for SAD. M-CBT sessions consisted mainly of MT and cognitive restructuring. As it was suggested that reducing cost bias predicts improvement in SAD (Foa et al., 1996; Moscovitch et al., 2012; Shirotsuki et al., 2014), it is essential to enhance the effects of cognitive restructuring in SAD treatment. The three stages of cognitive restructuring were shown to be (a) identify negative thoughts that occur before, during, or after anxiety-provoking situations; (b) evaluate the accuracy of these thoughts from an objective viewpoint; and (c) derive rational alternative thoughts based on the acquired information (Heimberg, 2002). Cognitive restructuring is also important to distance oneself from one’s thoughts and regard them as psychological events rather than reality (Beck et al., 1979). MT increases the ability to distance thoughts, cognitive flexibility, and cognitive reappraisal skills (Carmody et al., 2009; Desrosiers et al., 2013). Also, MT impacts cognitive reappraisal skills via the enhancement of trait mindfulness (Garland et al., 2015). Cognitive restructuring post-MT contributes toward increasing thinking flexibility and noticing unhelpful thoughts (Barlow et al., 2011). Noda and Shirotsuki (2017) suggested that cognitive restructuring post-MT may facilitate more constructive thoughts, since MT promotes the awareness of thoughts. Based on the above studies, MT is expected to enhance the effects of cognitive restructuring in SAD treatment. Thus, we hypothesized that the combination of MT and cognitive restructuring is a highly effective intervention for improving cost bias and the clinical symptoms of SAD. To address this hypothesis, this research was conducted as a pilot study in which M-CBT was administered to patients with SAD in a single-arm trial.
Although only several studies have examined the effectiveness of MBIs for SAD, Liu et al.’s (2021) meta-analysis report shows some promising results. Goldin et al. (2016) conducted the MBSR on patients with SAD and discovered high therapeutic efficacy. The MBSR program, developed by Kabat-Zinn (1990) and aimed primarily at enhancing well-being, consisted of 12 sessions lasting 2.5 h in Goldin et al.’s study (2016). Piet et al. (2010) practiced MBCT with patients with SAD. MBCT was originally developed as an intervention to prevent the recurrence of depression and was based on MBSR (Segal et al., 2002); however, it is used as a treatment for several mental illnesses other than depression. Piet et al. (2010) demonstrated the effectiveness of the MBCT in groups of eight weekly 2-h sessions on SAD. MAGT, developed by Fleming and Kocovski (2007), is a program based on CBT and acceptance and commitment therapy (ACT) theory, consisting of mindfulness and ACT exercises (including exposure). MAGT involves a group and includes 12 weekly 2-h sessions; it has shown high therapeutic efficacy for SAD (Kocovski et al., 2009). Meanwhile, M-CBT is a low-intensity treatment module with fewer sessions than the MBI described above; it targets the improvement of cost bias in predicting treatment effects for SAD. Developing a program with fewer sessions than the traditional MBI program could make it easier to use in combination with other treatment modalities and reduce the financial burden and inconvenience of receiving treatment. Accumulating evidence for the efficacy of M-CBT could provide new treatment options for patients with SAD and provide a treatment that is better tailored to the patient’s conditions.
Methods
Participants and Procedure
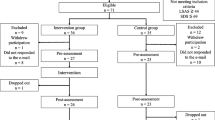
The participants were outpatients who suffered mainly from social anxiety attending an outpatient clinic in Tokyo, specializing in treating depression and anxiety. The inclusion criteria were having SAD (based on the criteria from the Diagnostic and Statistical Manual of Mental Disorders, 5th ed, DSM-5; American Psychiatric Association (2013), assessed by the Mini-International Neuropsychiatric Interview for DSM-5 (MINI; Sheehan et al., 1998) and being 18 years and older. The exclusion criteria were having a current psychotic disorder, current manic episode, high suicide risk, severe physical illness, or significant cognitive impairment. Patients (N = 30) who requested to participate in the study were individually spoken to about it and considered if they met the inclusion criteria. The MINI assessments were administered by a clinical psychologist in person. All participants met the SAD diagnosis and participation criteria, and written informed consent was obtained before their enrollment. However, six patients withdrew from participating prior to the M-CBT implementation due to work, relocation, or scheduling conflicts. Of the 24 participants, 18 completed all sessions (five sessions), five attended four sessions, and one dropped out. Figure 1 documents the participants’ flow, and the 23 participants’ clinical characteristics from the MINI diagnoses are displayed in Table 1.

Participants’ flowchart
Of the 23 patients, 15 had comorbidities, such as current major depressive episode, current panic disorder, current post-traumatic stress disorder, alcohol use disorder in the past 12 months, current anorexia nervosa, current bulimia nervosa, current binge eating disorder, and current generalized anxiety disorder. Only eight patients with SAD did not have comorbid mental disorders currently. Ten patients had received CBT in the past, and 21 patients were receiving pharmacological therapy, such as aripiprazole (8.70%), atomoxetine hydrochloride (8.70%), brexpiprazole (4.35%), duloxetine hydrochloride (13.04%), escitalopram oxalate (34.78%), ethyl loflazepate (13.04%), etizolam (4.35%), quetiapine fumarate (8.70%), lurasidone hydrochloride (13.04%), risperidone (8.70%), sertraline hydrochloride (8.70%), sulpiride (8.70%), trazodone hydrochloride (4.35%), venlafaxine hydrochloride (17.39%), and vortioxetine hydrobromide (4.35%), for their clinical symptoms. Three patients had received mindfulness-based stress reduction, and 21 patients had received MT (mean, 179.13 h ± 273.06). The average duration of treatment for patients at the clinic was 751.96 (± 860.79) days.
This study was registered in the UMIN Clinical Trial Registration System (UMIN: 000043720) and conducted with the approval of the Research Ethics Committee of the Faculty of Human Sciences, Musashino University (Approval Number: 202013).
Materials
Screening Measure
We administered a structural interview through screening indicators prior to inclusion in the study.
Clinician-Administered Structured Interview
The MINI 7.0.2 (Sheehan et al., 1998) was used to assess mental disorders based on DSM-5.
Treatment Outcomes
We assessed the following measures as treatment outcomes at eight time points: before the intervention, before each session, after the intervention, and at a one-month follow-up.
Primary Outcomes
The severity of SAD symptoms was assessed by the Japanese version of Liebowitz Social Anxiety Scale (LSAS; Asakura et al., 2002), which is a self-report scale that measures social anxiety and avoidance behavior in anxiety-provoking social situations (Liebowitz, 1987). The scale consists of 24 items, each rated on a four-point scale from 0 (none on the social anxiety scale and never on the avoidance behavior scale) to 3 (severe in the social anxiety scale and usually on the avoidance behavior scale). The total score was used as a criterion for clinical symptoms of SAD and ranged from 0 to 144 (social anxiety 72, avoidance behavior 72), with higher scores indicating greater social anxiety symptoms. Also, we used the Speech Cost/Probability bias Scale (SCPS; Noda et al., 2017) to assess cost and probability bias. The scale consists of 11 items, each rated on a five-point scale from 1 (not at all in the cost bias scale and I don’t think so at all in the probability bias scale) to 5 (very much in the cost bias scale and I very much think so in the probability bias scale). The total score ranges from 11 to 55, with higher scores indicating greater cognitive bias.
Secondary Outcomes
The short version of the Japanese Fear of Negative Evaluation Scale (SFNE; Sasagawa et al., 2004) was used to assess fear of negative evaluation from others, which is one of the diagnostic criteria of SAD. The SFNE contains 12 items rated on a five-point scale from 1 (not at all) to 5 (very much). The total score ranges from 12 to 60, with higher scores indicating a greater fear of negative evaluation from others. The Japanese version of the Self-Focused Attention Scale (SFA; Noda et al., 2021a) was used to assess self-focused attention, which is a core maintaining factor of SAD. It consists of 11 items, including six for the arousal factor and five for the behavior factor. Each item is rated on a five-point scale from 0 (not at all) to 4 (very much), and the total score ranges from 0 to 44, with higher scores indicating greater self-focused attention.
Additional Outcomes
The Japanese version of Five Facet Mindfulness Questionnaire (FFMQ; Sugiura et al., 2012) was used to assess trait mindfulness. It includes 39 items and consists of five subscales: “observing (eight items),” “acting with awareness (eight items),” “nonjudging (seven items),” “nonreactivity (eight items),” and “describing (eight items).” The total score of the five subscales represented trait mindfulness. Each item is rated on a five-point scale from 1 (never or very rarely true) to 5 (very often or always true), and the total score ranges from 39 to 195, with higher scores indicating greater trait mindfulness. The Japanese version of the Self-rating Depression Scale (SDS; Fukuda & Kobayashi, 1973) was used to assess depressive symptoms. The SDS contains 20 items rated on a four-point scale from 1 (a little of the time) to 4 (most of the time). The total score ranges from 20 to 80, with higher scores indicating greater depressive symptoms. The Japanese version of Emotion Regulation Questionnaire (ERQ; Yoshizu et al., 2013) was used to assess emotion regulation such as cognitive reappraisal and suppression. The cognitive reappraisal subscale consists of six items and the suppression subscale consists of four items, each rated on a seven-point scale from 1 (strongly disagree) to 7 (strongly agree). The total score of the cognitive reappraisal subscale ranges from 6 to 42, and the suppression subscale ranges from 4 to 28, with higher scores indicating greater emotion regulation.
Therapy Protocol
The four-session program of M-CBT protocol was developed by Noda et al., (2021b). The original M-CBT program was conducted as four 90–120-min sessions in a group format (of three to eight participants per group). The protocol in this study added a half-day retreat (150 min) to that program. The program comprised of MT, cognitive restructuring, psychoeducation, and sharing. The therapy protocol is presented in Table 2. The purpose of Session 1 was to discover the factors that increased one’s social anxiety, consisting of mindful yoga, developing a treatment plan, psychoeducation, sitting meditation, and sharing. First, mindful yoga was performed to relieve tension in the group. The treatment plan was explained to participants, and they engaged in a motivational exercise in which goals and expectations of the treatment were discussed. They were informed of the maintaining mechanisms of social anxiety, particularly the role of negative thoughts in increasing social anxiety, rumination, cost bias, and probability bias, deriving an individual personal model using these definitions. Subsequently, the concept of mindfulness and how it helps reduce negative thoughts and social anxiety were explained. After the psychoeducation, sitting meditation with a focus on breathing, body sensation, feeling, and thoughts was conducted. The therapist led the participants to bring awareness to the present moment and recognize physical, cognitive, and emotional responses. Finally, participants shared what they had discovered about themselves (especially emotional, physiological, and cognitive experiences) with the other group members, throughout the session. The purpose of Session 2 was to identify the factors that were causing one’s social anxiety, consisting of mindful yoga, psychoeducation, imagery meditation, and sharing. First, mindful yoga was performed to relieve tension in the group and participants learned about social anxiety and mindfulness through psychoeducation. The mental responses to anxiety-provoking situations, including thoughts (rumination, cost bias, and probability bias), emotions, physical sensations, and avoidance behaviors, were explained to the participants. In the mindfulness practice, the participants performed imagery meditation. They imagined anxiety-provoking situations and tried to notice their response patterns during sitting meditation. The therapist prompted participants to identify negative thoughts that increased their social anxiety and to become aware of their response patterns. Finally, the participants shared what they had noticed, identified, and learned (especially emotional, physiological, and cognitive experiences) throughout the session. The purpose of Session 3 was to observe the factors that were causing one’s social anxiety, focusing on mindfulness practices to confront and let go of negative thoughts that increased social anxiety using developing an anxiety hierarchy list and personal version of cognitive behavioral models, imagery meditation, and sharing. In order to identify the anxiety-provoking situations, the participants made the anxiety hierarchy list. Furthermore, they made the cognitive behavioral model constructed with four variables (thoughts, emotions, physical sensations, and avoidance behaviors) before the mindfulness practice. Participants imagined anxiety-provoking situations and attempted to notice their negative thoughts and other responses. The therapist ensured that the participants did not criticize or suppress the thoughts, but observed them and experienced the process of waiting for them to disappear. Participants’ experience with the mindfulness practices was shared. The fourth session was a half-day retreat. Mindful yoga, body scan, mindful walking, and sitting meditation were performed to enhance mindfulness. The purpose of Session 5 was to let go of the factors that were causing one’s social anxiety. It was designed to help participants acquire the skills to think objectively rather than subjectively using imagery meditation, cognitive restructuring, loving-kindness meditation, and sharing. First, through mindfulness practice using imagery of the anxiety-provoking situations, the therapist prompted the participants to notice negative thoughts and other responses in threatening situations. Second, cognitive restructuring using a thought record was conducted to enhance one’s skill of looking at things from different perspectives instead of just subjective ones. The therapist ensured that participants gained skills that would allow them to employ realistic and constructive thoughts, while accepting the negative ones that come from subjective perspectives. Finally, a loving-kindness meditation was implemented and experiences were shared.
Homework
Participants were given homework designed to integrate the practices of each session into their daily lives. Homework assignments for Session 1 included sitting meditation, informal mindfulness practice, and diary of daily happiness. Participants were given a meditation guide that included videos of guided sitting meditation and instructed them to meditate for at least 20 min each day at home. Participants were also briefed on practices for living mindfully in their daily lives and were encouraged to complete these practices every day. The diary of daily happiness is intended to help participants become aware of the small happiness they experience in their daily lives. Participants were asked to describe pleasant events; their thoughts, feelings, and physical sensations at the time; and their thoughts when they looked back on the events. Homework assignments for Session 2 included sitting or imagery meditation; informal mindfulness practice; and diary of thoughts, emotions, behaviors, and physical reactions when interacting with others. The goal of the video with guided imagery meditation given to participants was to help them become aware of how they react in an anxiety-provoking situation. Participants in the informal mindfulness practice selected one daily activity to be mindful of each day of the following week: eating breakfast slowly and savoring it; walking slowly and consciously; and lying on their back and just feeling their body before going to bed. The purpose of the interpersonal and social interaction diary was to help participants become more aware of their responses. Participants were asked to describe events related to interacting with others; their thoughts, feelings, and physical sensations at the time; and their thoughts when they looked back on the events. Homework assignments for Session 3 included sitting meditation or imagery meditation, informal mindfulness practice, and diary of communication with others. Participants received a video with guided imagery meditation that was aimed at helping them observe their response in an anxiety-provoking situation and experience the process of waiting for their response to pass. Participants were also briefed on practices for living mindfully when faced with unpleasant or difficult situations and were encouraged to perform these practices every day. Participants were asked to describe situations in which they communicated with others; their thoughts, feelings, physical sensations, and behaviors at the time; what makes communicating with others difficult; and what they have learned from that communication. Homework assignments for the half-day retreat included sitting meditation or imagery meditation and informal mindfulness practice. Participants were encouraged to work on these homework assignments in the same way as in Sessions 1, 2, and 3. Homework assignments for Session 4 included sitting meditation, imagery meditation or loving-kindness meditation, and informal mindfulness practice. A video with instructions for a loving-kindness meditation was given to participants. Participants in the informal mindfulness practice selected one daily activity to be mindful of throughout the week when faced with unpleasant or difficult situations (noticing their emotions without reacting to them and instead of pushing the unpleasant or depressing experiences to the back of their minds, just feeling the experience and waiting for it to end).
Place and Therapist
The M-CBT was conducted at a clinic in Tokyo. Participants could freely borrow a yoga mat and zafu (cushion). The program was conducted using PowerPoint. A therapist who is both a certified public psychologist and a clinical psychologist led all of the group sessions. The therapist has more than 5 years of clinical experience practicing psychotherapy in clinical settings, more than 5 years of experience in mindfulness practice, and more than 2 years of clinical experience practicing MT in clinical settings. For CBT, the therapist was supervised by a clinical psychologist with more than 10 years of clinical experience, and for MT, by an MBSR teacher with more than 10 years of clinical experience.
Statistical Analyses
Two sets of analyses were conducted: one for patients, including those who attended at least 80% of the sessions (intent-to-treat (ITT) sample), and the other for the sample of patients who completed all sessions (completer sample). Eighteen of the 23 participants included in ITT analyses completed all sessions of the program, and five participated in four sessions. The effectiveness of M-CBT was analyzed with linear mixed-effects models. If the main effects of time were significant, multiple comparisons were performed using the Bonferroni method. A priori power calculations by G*Power showed that a sample of at least 16 participants was required to detect a moderate effect size (f = 0.25) (alpha = 0.05, power = 0.80). Cohen’s d was calculated to examine the effect size between the pre- and post-test and follow-up test. We used the statistical software SPSS version 28.0 (IBM Corp., Armonk, NY, USA) for linear mixed models and effect sizes.
Missing Data
In the ITT and completer samples, two patients had the same timing for the pre-test and the test before the first session. Thus, their test scores were the same. In the ITT sample, a patient had a missing value in the FFMQ on the test before the fourth session. Since the scores in this item on the test before the third and fifths session were the same, we substituted the same score for that item on the test before the third session based on the last observation carried forward. Other missing values were complemented and analyzed by linear mixed-effects models.
Results
Linear Mixed-Effects Models
ITT Sample
Table 3 shows the means and standard deviations of the outcome indicators of the ITT sample and results of linear mixed-effects models. There were significant reductions in all primary outcomes (LSAS: F(7, 149.14) = 11.40, p < 0.01, LSAS-anxiety: F(7, 149.05) = 9.59, p < 0.01, LSAS avoidance: F(7, 149.10) = 9.10, p < 0.01, SCPS-cost bias total score: F(7, 149.04) = 14.84, p < 0.01, SCPS-cost bias in the negative cognition from one’s own performance: F(7, 149.10) = 12.35, p < 0.01, SCPS-cost bias in the negative cognition that occurs by paying attention to others: F(7, 149.05) = 11.13, p < 0.01, SCPS-probability bias total score: F(7, 149.07) = 20.11, p < 0.01, SCPS-probability bias in the negative cognition from one’s own performance: F(7, 149.08) = 16.39, p < 0.01, SCPS-probability bias in the negative cognition that occurs by paying attention to others: F(7, 149.11) = 14.47, p < 0.01). There were significant improvements in all secondary outcomes (SFNE: F(7, 149.05) = 11.99, p < 0.01, SFA total score: F(7, 149.07) = 5.01, p < 0.01, SFA-arousal: F(7, 149.10) = 4.11, p < 0.01, SFA-behavior: F(7, 149.04) = 4.70, p < 0.01). There were significant reductions in all additional outcomes (FFMQ: F(7, 149.05) = 13.57, p < 0.01, SDS: F(7, 149.12) = 10.36, p < 0.01, ERQ-cognitive reappraisal: F(7, 149.09) = 6.03, p < 0.01), except for ERQ-suppression: F(7, 149.04) = 0.56, p = 0.79).
Completer Sample
Table 4 shows the means and standard deviations of the outcome indicators of the completer sample and results of linear mixed-effects models. There were significant reductions in all primary outcomes (LSAS: F(7, 119.00) = 10.34, p < 0.01, LSAS-anxiety: F(7, 119.00) = 7.55, p < 0.01, LSAS-avoidance: F(7, 119.00) = 9.53, p < 0.01, SCPS-cost bias total score: F(7, 119.00) = 9.97, p < 0.01, SCPS-cost bias in the negative cognition from one’s own performance: F(7, 119.00) = 8.60, p < 0.01, SCPS-cost bias in the negative cognition that occurs by paying attention to others: F(7, 119.00) = 7.70, p < 0.01, SCPS-probability bias total score: F(7, 119.00) = 15.44, p < 0.01, SCPS-probability bias in the negative cognition from one’s own performance: F(7, 119.00) = 14.21, p < 0.01, SCPS-probability bias in the negative cognition that occurs by paying attention to others: F(7, 119.00) = 9.77, p < 0.01). There were significant improvements in all secondary outcomes (SFNE: F(7, 119.00) = 11.76, p < 0.01, SFA total score: F(7, 119.00) = 2.88, p < 0.01, SFA-arousal: F(7, 119.00) = 2.40, p < 0.05, SFA-behavior: F(7, 119.00) = 3.21, p < 0.01). There were significant reductions in all additional outcomes (FFMQ: F(7, 119.00) = 12.22, p < 0.01, SDS: F(7, 119.00) = 4.61, p < 0.01, ERQ-cognitive reappraisal: F(7, 149.09) = 6.03, p < 0.01), except for ERQ-suppression: F(7, 119.00) = 0.96, p = 0.47).
Effect Sizes
Effect sizes between the pre- and post-test and follow-up test are shown in Table 5. Significant effect sizes between the pre-and post-tests were shown for LSAS, SCPS-cost bias, SCPS-probability bias, SFNE, FFMQ, SDS, and ERQ-cognitive reappraisal in the ITT and completer samples (p < 0.05). Between the pre-test and follow-up, significant effect sizes were shown for LSAS, SCPS-cost bias, SCPS-probability bias, SFNE, SFA-arousal, FFMQ, SDS, and ERQ-cognitive reappraisal in the ITT and completer samples (p < 0.05).
Discussion
The purpose of this study was to examine the feasibility and initial effectiveness of the four-session program of M-CBT for SAD. The primary outcomes of this study were social anxiety symptoms, cost bias, and probability bias. The results of the linear mixed-effects models showed that the M-CBT was effective for social anxiety symptoms, cost bias, and probability bias. The multiple comparisons showed that there were significant improvements in these outcomes from the test before the fourth or fifth session. The M-CBT also produced significant pre-post- or follow-up improvements in social anxiety symptoms, as measured by the LSAS, with high effect sizes (d = 1.04 to 1.08). This was similar to the effect sizes of the MAGT, which had effect sizes of 1.00 for LSAS between pre- and post-test and follow-up (Kocovski et al., 2009). The MAGT meets once a week for 2-h sessions over a 12-week period. In Piet et al.’s study (2010), the effect size of MBCT was 0.90, measured by LSAS, which is similar to the effect size of the present study. The MBCT consisted of eight weekly 2-h sessions in groups, with more sessions than the M-CBT. Thus, the M-CBT would be equally effective for social anxiety symptoms when compared to other MBIs. This program consists of four sessions and a half-day retreat, which is fewer sessions than those required by MAGT and MBCT. Therefore, it may be more affordable and convenient than other interventions that treat SAD. High effect sizes were also obtained in the cost and probability bias (cost bias: d = 0.82 to 1.13, probability bias: d = 1.03 to 1.32). Cost bias is an important predictor in improving social anxiety symptoms (Foa et al., 1996); past findings showed that patients who did not respond to cost bias in traditional CBT did not have improved social anxiety symptoms (Moscovitch et al., 2012). The M-CBT targets cost bias, which is a maintaining factor of social anxiety symptoms. The results of this study indicate that the M-CBT is highly effective in treating cost bias and social anxiety symptoms. Therefore, the M-CBT may be expected to represent an effective treatment module for patients who do not respond to traditional CBT.
The secondary outcomes of this study were fear of negative evaluation from others and self-focused attention, which are core maintaining factors of social anxiety symptoms. In particular, the importance of reducing the fear of negative evaluation from others in the treatment of SAD has been emphasized (Mattick & Peters, 1988; Mattick et al., 1989). The results of linear mixed-effects models showed that M-CBT was effective at reducing fear of negative evaluation from others and self-focused attention. The multiple comparisons demonstrated significant improvements in the fear of negative evaluation from others in the test before the fourth or fifth session. High values were also obtained for the effect size (d = 0.94 to 1.22), suggesting a higher therapeutic effect than with MBCT (Piet et al., 2010; d = 0.50). In contrast, the effect sizes of M-CBT in self-focused attention were weak to moderate (d = 0.28 to 0.57). Baer (2009) suggested that enhanced trait mindfulness mediated the improvement in psychological functioning by cultivating an adaptive form of self-focused attention. Self-focused attention decreased through the attention training technique, which is associated with reduced anxiety, while self-focused attention increased through the brief mindfulness program, associated with decreased anxiety (Fergus et al., 2014). Noda et al. (2023) indicated that the enhanced awareness component of mindfulness increases self-focused attention, while the enhanced acceptance component of mindfulness decreases self-focused attention. Since this program targets both the awareness and acceptance components of mindfulness as intervention targets, it is suggested that the effects on self-focused attention may have been weak to moderate.
The additional outcomes of this study were trait mindfulness, depressive symptoms, cognitive reappraisal, and suppression. The results of linear mixed-effects models showed that M-CBT was effective for trait mindfulness, depressive symptoms, and cognitive reappraisal. In the multiple comparisons, there were significant improvements in trait mindfulness from the test before the fourth session. In addition, strong effect sizes were calculated between the pre-and post-test and follow-up (d = − 0.82 to − 1.01), suggesting that M-CBT is helpful as a program to enhance trait mindfulness for SAD, as well as for individuals with high social anxiety (Noda, 2020). Furthermore, the M-CBT produced significant pre-post- or follow-up improvements in depressive symptoms, as measured by the SDS, with moderate to high effect sizes (d = 0.75 to 0.90). These values can be considered higher than the effect size of MBCT (Piet et al., 2010; d = 0.64), and similar to that of MAGT (Kocovski et al., 2009; d = 0.79 to 0.98), on depressive symptoms, as measured by the Beck Depressive Inventory. Furthermore, moderate to strong effect sizes were obtained between the pre- and post-test and follow-up (d = − 0.62 to − 0.81), suggesting that M-CBT contributes toward cognitive restructuring skills. However, the M-CBT did not show an effect on suppression and did not contribute to emotional release.
From the abovementioned findings, M-CBT is considered feasible and helpful as a low-intensity treatment program for SAD. However, there are some limitations to this study that need to be considered. First, further studies on the effectiveness of M-CBT with a larger sample size are needed. Although the sample size of this study exceeded the results of the priori power calculations (N = 16), it was still relatively small. This limits the evidence for the effectiveness of M-CBT. Second, there is the need to conduct a randomized controlled trial comparing M-CBT and a control group, such as a wait-list group. Although this study examined the efficacy of M-CBT in a single-arm trial and the results of the linear mixed-effects model showed its effectiveness, we cannot rule out the possibility that factors other than the intervention, such as the time course, could have affected the degree of symptom improvement. Third, it is necessary to compare the therapeutic effects of M-CBT with those of a cognitive behavioral group therapy consisting primarily of cognitive restructuring. We hypothesized that the combined use of MT with cognitive restructuring would enhance the therapeutic effect of cognitive restructuring and be a more effective intervention for cost bias and social symptoms than cognitive restructuring alone. However, since the treatment effects were not compared with a program consisting primarily of cognitive restructuring, the above hypotheses cannot be determined. Fourth, there is a need to compare the effectiveness of M-CBT with other MBIs. In the “Discussion” section, we compared the effect sizes between M-CBT and MBIs, but studies that assume a direct comparison of effects are warranted.
Despite these limitations, this study demonstrated that the four-session program of M-CBT is feasible and acceptable for patients with SAD. This finding supports the first phase of accumulating evidence for the use of mindfulness and cognitive restructuring in the treatment of SAD. Rigorous randomized controlled trials that address the limitations of this study should be conducted to accumulate evidence of this possibility. These findings would provide a rationale for therapists to combine CBT techniques and MBIs in clinical settings. If the effectiveness of M-CBT is validated, it may provide new treatment options for patients with SAD and lead to more tailored therapies for their conditions. As M-CBT is positioned as a low-intensity treatment module, it may be expected as a viable treatment option for patients with mild SAD, those with SAD who require additional intervention for cost bias, or those with other mental illnesses who need intervention for social anxiety symptoms.
Data Availability
Detailed data are available from the corresponding authors upon reasonable request.
Materials Availability
The program materials are available from the first author upon reasonable request.
Change history
22 July 2023
A Correction to this paper has been published: https://doi.org/10.1007/s41811-023-00178-w
Abbreviations
- ACT:
-
Acceptance and commitment therapy
- CBT:
-
Cognitive behavioral therapy
- ERQ:
-
Emotion Regulation Questionnaire
- FFMQ:
-
Five Facet Mindfulness Questionnaire
- ITT:
-
Intent to treat
- LSAS:
-
Liebowitz Social Anxiety Scale
- MAGT:
-
Mindfulness- and acceptance-based group therapy
- MBCT:
-
Mindfulness-based cognitive therapy
- MBIs:
-
Mindfulness-based interventions
- M-CBT:
-
Mindfulness and cognitive behavioral therapy
- MINI:
-
Mini-International Neuropsychiatric Interview for DSM-5
- MT:
-
Mindfulness training
- SAD:
-
Social anxiety disorder
- SCPS:
-
Speech Cost/Probability bias Scale
- SDS:
-
Self-rating Depression Scale
- SFA:
-
Self-Focused Attention Scale
- SFNE:
-
Short Fear of Negative Evaluation Scale
References
Acarturk, C., de Graaf, R., van Straten, A., ten Have, M. T., & Cuijpers, P. (2008). Social phobia and number of social fears, and their association with comorbidity, health-related quality of life and help seeking: A population-based study. Social Psychiatry and Psychiatric Epidemiology, 43(4), 273–279. https://doi.org/10.1007/s00127-008-0309-1
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders 5th ed. American Psychiatric Association.
Asakura, S., Inoue, S., Sasaki, F., Sasaki, Y., Kitagawa, N., Inoue, T., Denda, K., Ito, M., Matsubara, Y., & Koyama, T. (2002). Reliability and validity of the Japanese version of the Liebowitz social anxiety scale. Japanese Journal of Psychiatric Medicine, 44, 1077–1084.
Baer, R. A. (2009). Self-focused attention and mechanisms of change in mindfulness-based treatment. Cognitive Behaviour Therapy., 38, 15–20. https://doi.org/10.1080/16506070902980703
Barlow, D. H., Green, J. D., Fairholme, C. P., Elland, K. K., Boisseau, C. L., Allen, L. B., & Ehrenreich-May, J. T. (2011). Unified protocol for transdiagnostic treatment of emotional disorder: Therapist guide. Oxford University Press.
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression. Guilford Press.
Bögels, S. M., Alberts, M., & de Jong, P. J. (1996). Self-consciousness, self-focused attention, blushing propensity and fear of blushing. Personality and Individual Differences, 21, 573–581. https://doi.org/10.1016/0191-8869(96)00100-6
Cardaciotto, L., Herbert, J. D., Forman, E. M., Moitra, E., & Farrow, V. (2008). The assessment of present-moment awareness and acceptance: The Philadelphia Mindfulness Scale. Assessment, 15(2), 204–223. https://doi.org/10.1177/1073191107311467
Carmody, J., Baer, R. A., Lykins, E. L. B., & Olendzki, N. (2009). An empirical study of the mechanisms of mindfulness in a mindfulness-based stress reduction program. Journal of Clinical Psychology, 65, 613–626. https://doi.org/10.1002/jclp.20579
Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In R. G. Heimberg, M. R. Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Social phobia: Diagnosis, assessment, and treatment (pp. 69–93). Guilford Press.
Desnoyers, A. J., Kocovski, N. L., Fleming, J. E., & Antony, M. M. (2017). Self- focused attention and safety behaviors across group therapies for social disorder. Anxiety Stress and Coping, 30, 441–455. https://doi.org/10.1080/10615806.2016.1239083
Desrosiers, A., Vine, V., Klemanski, D. H., & Nolen-Hoeksema, S. (2013). Mindfulness and emotion regulation in depression and anxiety: Common and distinct mechanisms of action. Depression and Anxiety, 30, 654–661. https://doi.org/10.1002/da.22124
Fergus, T. A., Wheless, N. E., & Wright, L. C. (2014). The attention training technique, self-focused attention, and anxiety: A laboratory-based component study. Behaviour Research and Therapy, 61, 150–155. https://doi.org/10.1016/j.brat.2014.08.007
Fleming, J. E., & Kocovski N. L. (2007; revised 2009, 2013). Mindfulness and acceptance-based group therapy for social anxiety disorder: A treatment manual. Retrieved from http://www.actonsocialanxiety.com/pdf/Treatment_Manual.pdf.
Foa, E. B., Franklin, M. E., Perry, K. J., & Herbert, J. D. (1996). Cognitive biases in generalized social phobia. Journal of Abnormal Psychology, 105, 433–439.
Fukuda, K., & Kobayashi, S. (1973). A study on a self-rating depression scale. Seishin Shinkeigaku Zasshi, 75, 673–679.
Garland, E. L., Hanley, A., Farb, N. A., & Froeliger, B. (2015). State mindfulness during meditation predicts enhanced cognitive reappraisal. Mindfulness, 6, 234–242. https://doi.org/10.1007/s12671-013-0250-6
Goldin, P. R., Morrison, A., Jazaieri, H., Brozovish, F., Heimberg, R., & Gross, J. J. (2016). Group CBT versus MBSR for social anxiety disorder: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 84, 427–437. https://doi.org/10.1037/ccp0000092
Heimberg, R. G. (2002). Cognitive-behavioral therapy for social anxiety disorder: Current status and future directions. Society of Biological Psychiatry, 51, 101–108. https://doi.org/10.1016/s0006-3223(01)01183-0
Heimberg, R. G., Brozovich, F. A., & Rapee, R. M. (2014). A cognitive-behavioral model of social anxiety disorder. In S. G. Hofmann & P. M. DiBartolo (Eds.), Social Anxiety: Clinical, Developmental and Social Perspectives (pp. 705–728). Elsevier. https://doi.org/10.1016/B978-0-12-394427-6.00024-8
Hofmann, S. G., & Otto, M. W. (2008). Cognitive behavioral therapy for social anxiety disorder. Routledge.
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. Delacorte Press.
Kabat-Zinn, J. (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. Hyperion.
Kocovski, N. L., Fleming, J., & Rector, N. A. (2009). Mindfulness and acceptance-based group therapy for social anxiety disorder: An open trial. Cognitive and Behavioral Practice, 16, 276–289. https://doi.org/10.1016/j.cbpra.2008.12.004
Kocovski, N. L., Fleming, J. E., Hawley, L. L., Huta, V., & Antony, M. M. (2013). Mindfulness and acceptance-based group therapy versus traditional cognitive behavioral group therapy for social anxiety disorder: A randomized controlled trial. Behaviour Research and Therapy, 51, 889–898. https://doi.org/10.1016/j.brat.2013.10.007
Kocovski, N. L., Fleming, J. E., Hawley, L. L., Ho, M. R., & Antony, M. M. (2015). Mindfulness and acceptance-based group therapy and traditional cognitive behavioral group therapy for social anxiety disorder: Mechanisms of change. Behaviour Research and Therapy, 70, 11–22. https://doi.org/10.1016/j.brat.2015.04.005
Koszycki, D., Benger, M., Shlik, J., & Bradwejn, J. (2007). Randomized trial of a meditation-based stress reduction program and cognitive behavior therapy in generalized social anxiety disorder. Behaviour Research and Therapy, 45, 2518–2526. https://doi.org/10.1016/j.brat.2007.04.011
Liebowitz, M. R. (1987). Social phobia. Modern Problems of Pharmacopsychiatry, 22, 141–173. https://doi.org/10.1159/000414022
Liu, X., Yi, P., Ma, L., Liu, W., Deng, W., Yang, X., Liang, M., Luo, J., Li, N., & Li, X. (2021). Mindfulness-based interventions for social anxiety disorder: A systematic review and meta-analysis. Psychiatry Research, 300, 113935. https://doi.org/10.1016/j.psychres.2021.113935
Mattick, R. P., & Peters, L. (1988). Treatment of severe social phobia: Effects of guided exposure with and without cognitive restructuring. Journal of Consulting and Clinical Psychology, 56, 251–260. https://doi.org/10.1037/0022-006X.56.2.251
Mattick, R. P., Peters, L., & Clarke, J. C. (1989). Exposure and cognitive restructuring for social phobia: A controlled study. Behavior Therapy, 20, 3–23. https://doi.org/10.1016/S0005-7894(89)80115-7
Mayo-Wilson, E., Dias, S., Mavranezouli, I., Kew, K., Clark, D. M., Ades, A. E., & Pilling, S. (2014). Psychological and pharmacological interventions for social anxiety disorder in adults: A systematic review and network meta-analysis. The Lancet Psychiatry, 1, 368–376. https://doi.org/10.1016/S2215-0366(14)70329-3
Moscovitch, D. A., Gavric, D. L., Senn, J. M., Santesso, D. L., Miskovic, V., Schmidt, L. A., & Antony, M. M. (2012). Changes in judgment biases and use of emotion regulation strategies during cognitive-behavioral therapy for social anxiety disorder: Distinguishing treatment responders from non-responders. Cognitive Therapy Research, 36, 261–271. https://doi.org/10.1007/s10608-011-9371-1
Noda, S., & Shirotsuki, K. (2017). The mechanism of mindfulness on social anxiety disorder and the intervention program. The Annual of Musashino University Clinical Psychology Center, 17, 37–44.
Noda, S., Osawa, S., & Shirotsuki, K. (2017). The development of the speech cost/probability bias. Japanese Journal of Cognitive Therapy, 10, 219–231.
Noda, S., Okawa, S., Shirotsuki, K., Sasagawa, T., & Bögels, S. M. (2021a). The Japanese self-focused attention scale: Factor structure, internal consistency, convergent and discriminant validity. Journal of Clinical Psychology, 77, 2011–2026. https://doi.org/10.1002/jclp.23133
Noda, S., Shirotsuki, K., & Nakao, M. (2021b). The four-session program of mindfulness and cognitive behavioral therapy for social anxiety. Journal of Musashino University of Cognitive Behavioral Therapy and Research, 10, 219–231.
Noda, S., Nishiuchi, M., & Shirotsuki, K. (2023). Awareness and acceptance in anxiety-provoking social situations and social anxiety: Development and initial validation of the social anxiety-awareness and acceptance scale. Japanese Psychological Research. https://doi.org/10.1111/jpr.12446
Noda, S., Shirotsuki, K., & Sasagawa, T. (2022). Self-focused attention, cost/probability bias, and avoidance behavior mediate the relationship between trait mindfulness and social anxiety: A cross-sectional study. Frontiers in Psychology, 13 , 942801. https://doi.org/10.3389/fpsyg.2022.942801
Noda, S. (2020). The development of mindfulness and cognitive behavioral therapy for social anxiety and examination of its effectiveness. (Unpublished doctoral dissertation). Musashino University, Tokyo, Japan.
Okajima, I., Kanai, Y., Chen, J., & Sakano, Y. (2009). Effects of safety behavior on the maintenance of anxiety and negative belief social anxiety disorder. International Journal of Social Psychiatry, 55, 71–81. https://doi.org/10.1177/0020764008092191
Piet, J., Hougaard, E., Hecksher, M. S., & Rosenberg, N. K. (2010). A randomized pilot study of mindfulness-based cognitive therapy and group cognitive-behavioral therapy for young adults with social phobia. Scandinavian Journal of Psychology, 51, 403–410. https://doi.org/10.1111/j.1467-9450.2009.00801.x
Rapee, R. M., & Heimberg, R. G. (1997). A cognitive-behavioral model of anxiety in social phobia. Behaviour Research and Therapy., 35, 741–756. https://doi.org/10.1016/s0005-7967(97)00022-3
Sasagawa, S., Kanai, Y., Muranaka, Y., Suzuki, S., Shimada, H., & Sakano, Y. (2004). Development of a short fear of negative evaluation scale for Japanese using item response theory. Japanese Journal of Behavior Therapy, 30, 87–98. https://doi.org/10.24468/jjbt.30.2_87
Schmertz, S. K., Masuda, A., & Anderson, P. L. (2012). Cognitive processes mediate the relation between mindfulness and social anxiety within a clinical sample. Journal of Clinical Psychology, 68, 362–371. https://doi.org/10.1002/jclp.20861
Segal, Z. V., Williams, J. M., & Teasdale, J. (2002). Mindfulness-based cognitive therapy for depression. Guilford Press.
Sheehan, D. V., Lecrubier, Y., Harnett-Sheehan, K., Amorim, P., Janavs, J., Weiller, E., & Dunbar, G. C. (1998). The Mini International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry, 59, 22–33.
Shirotsuki, K., Kodama, Y., & Nomura, S. (2014). The preliminary study of individual cognitive behavior therapy for Japanese patients with social anxiety disorder. Psychological Services, 11, 162–170. https://doi.org/10.1037/a0034781
Springer, K. S., Levy, H. C., & Tolin, D. F. (2018). Remission in CBT for adult anxiety disorders: A meta-analysis. Clinical Psychology Review, 61, 1–8. https://doi.org/10.1016/j.cpr.2018.03.002
Stein, M. B., & Kean, Y. M. (2000). Disability and quality of life in social phobia: Epidemiologic findings. American Journal of Psychiatry, 157(10), 1606–1613. https://doi.org/10.1176/appi.ajp.157.10.1606
Sugiura, Y., Sato, A., Ito, Y., & Murakami, H. (2012). Development and validation of the Japanese version of the Five Facet Mindfulness Questionnaire. Mindfulness, 3, 85–94. https://doi.org/10.1007/s12671-011-0082-1
Yoshizu, J., Sekiguchi, R., & Amemiya, T. (2013). Development of a Japanese version of emotion regulation questionnaire. Japanese Journal of Research on Emotions, 20, 56–62. https://doi.org/10.4092/jsre.20.56
Funding
Open Access funding enabled and organized by Projekt DEAL. This study is supported by the JSPS KAKENHI Grant Number JP20J10260 and the Sasakawa Scientific Research Grant from the Japan Science Society.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
The ethics committee of the first author’s affiliated university, Research Ethics Committee of the Faculty of Human Sciences, Musashino University, approved this study (Approval Number: 202013).
Consent for Publication
Written informed consent was obtained from all participants prior to their enrollment in the study.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised to correct the fifth's author name.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Noda, S., Honda, Y., Komatsu, C. et al. Low-Intensity Mindfulness and Cognitive Behavioral Therapy for Social Anxiety Disorder: Pilot Study. J Cogn Ther 16, 510–536 (2023). https://doi.org/10.1007/s41811-023-00173-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41811-023-00173-1