
Abstract
Background
Glycogen Storage Disease Type Ia (GSDIa) is a rare genetic metabolic disorder characterized by hypoglycemia, hepatomegaly, growth failure, and possible seizures/death. Patients frequently consume cornstarch to maintain blood glucose. Evidence demonstrating the impact of GSDIa on health-related quality of life (HRQoL) is lacking. This study aims to understand the burden of GSDIa by obtaining utility values for economic appraisals.
Methods
A targeted literature review and interviews with experts (n = 4) and caregivers (n = 4) informed the development of health state vignettes describing different GSDIa severities by age and level of hypothetical treatment (i.e., gene therapy) response. Health states reflecting caregivers’ experiences were also developed. A convenience sample of the UK general public completed a time trade-off (TTO) exercise. Scores conceptually varied from 0 (dead) to 1 (full health). States were also rated using a visual analog scale (VAS) and the EQ-5D-5L. Data were descriptively summarized.
Results
One hundred participants completed the exercise (male: 48%; mean age: 42 years). Scores were lowest for the adolescent pre-treatment state (TTO = 0.38). Large increments in HRQoL were observed for the response (adult: TTO = 0.86; child: TTO = 0.84) and complete response (adult and child: TTO = 0.94) hypothetical treatment response states. Caregiver values were lowest for the pre-treatment state (TTO = 0.57) and highest for the complete response state (TTO = 0.95). VAS and EQ-5D-5L scores followed a similar pattern.
Conclusion
This study found an HRQoL burden on GSDIa patients and caregivers, with potential large improvement from a hypothetical treatment. These findings may be useful for families, clinicians, regulatory agencies, and in therapy economic evaluations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
There is a health-related quality-of-life burden on patients with glycogen storage disease type Ia (GSDIa) and on caregivers of patients with GSDIa. |
A hypothetical GSDIa treatment could provide a large improvement in quality of life for both patients and caregivers. |
1 Introduction
Glycogen storage disease type Ia (GSDIa), a major GSD subtype caused by deficiency of glucose-6-phosphatase (G6Pase) catalytic activity [1], is a rare genetic metabolic disorder with an estimated incidence rate of 1 in 100,000 [2]. The most common clinical symptoms of GSDIa relate to hypoglycemia, including seizures, hepatomegaly, and growth failure. If poorly managed, the condition can also result in impaired cognitive and motor development, progression of liver and kidney manifestations to organ failure, and death [2]. Patients are also at an increased risk of other long-term complications, such as osteoporosis, hypertension, malignancies, and neurocognitive disorders.
There are currently no approved drug therapies for GSDIa. The condition can be managed with dietary measures including frequent feeding of complex carbohydrate-rich foods and frequent consumption of cornstarch throughout the day and night, which can cause several gastrointestinal side effects [3]. Dietary management does not treat the underlying mechanism of disease or reduce risks of long-term complications such as osteoporosis, renal disease, hypertension, and neurocognitive disorders, all of which can occur in even well-managed patients [4,5,6,7]. Some patients are fitted with a nasogastric or G-tube to help maintain blood glucose levels during the night [2]. The symptomatic burden and strict feeding schedule have a profound impact on health-related quality of life (HRQoL) in both patients and caregivers. Caregivers of people with GSDIa and GSDIb have been shown to report impaired HRQoL compared with healthy controls [8].
There is very little published evidence demonstrating the impact of GSDIa on HRQoL. This study aims to understand the burden of the disease and its management on patients’ and caregivers’ HRQoL. This study was designed to develop health state vignettes and levels of hypothetical treatment response based on available evidence for different stages of GSDIa and to evaluate both using time-trade off (TTO) interviews with the general public. This report describes the development of the health state vignettes and subsequent utility weights. In addition, the study attempts to assess the impact on a primary caregiver of a child with GSDIa.
2 Methods
2.1 Study Design
The first phase of this study aimed to develop vignettes for patient and caregiver health states based on a review of the literature and qualitative data from clinicians and caregivers. The second phase used the TTO interview method with a convenience sample of the UK general public to generate utilities for each health state.
2.2 Institutional Review Board (IRB) Approval
The study protocol was assessed using the United Kingdom Health Research Authority decision tool for ethics review requirements (http://www.hra-decisiontools.org.uk/ethics/). This decision tool indicated that the protocol did not need National Health Service Research Ethics Committee review, but another type of ethics committee review was recommended. Thus, all study materials were submitted to the Western Institutional Review Board (WIRB) in the United States for ethical review. WIRB reviewed the study materials and determined the study was exempt from ethical review on 21 September 2020 (WIRB Submission Number: 2643053-44684192).
2.3 Targeted Literature Review
A targeted literature review was conducted in April 2020 to identify published research on the symptoms and impact of GSDIa for patients and caregivers. Findings from this review informed the initial development of the vignettes and any interview discussion guides. The primary search was conducted in MEDLINE and Embase using free-text words in the title and abstract. There were no restrictions on study type or publication date. The full search string can be found in Table 1. Studies were included if the sample included GSDIa patients and reported findings on disease symptoms, impact on physical function, or HRQoL. The primary search was supplemented by study sponsor materials, including peer-reviewed publications, data from patient advocacy group meetings, and a review of the grey literature that included websites such as those from the Association for Glycogen Storage Disease UK and Metabolic Support UK.
2.4 Health State Development
The patient health states were categorized into four levels: (1) pre-treated sedentary, (2) pre-treated active, (3) hypothetical treated response, and (4) hypothetical treated complete response. The health states were also categorized by patient age (children [8–12 years], adolescents [13–17 years] and adults [≥ 18 years]) to reflect differing feeding requirements and HRQoL impact. As the differences in HRQoL impact between adolescent patients and other age groups is greatest in the most severely affected patients, adolescent-specific health states were created for the pre-treated sedentary level. The caregiver health states aimed to describe caregivers of (1) pre-treated sedentary children and (2) children who have completely responded to treatment. Only two caregiver states were selected to limit the number of vignettes presented to respondents and to capture the impact of states assumed to have the most and least severe HRQoL impact.
The content of the vignettes was informed by a targeted review of studies with individuals with GSDIa and/or their caregivers, internal data on file, and interviews with GSDIa clinicians and caregivers as described in the following section. Based on the findings of the literature review and input from the study sponsor, draft vignettes were developed describing the HRQoL impact initially for nine patient health states and two caregiver health states. The development of the caregiver vignettes was also informed by evidence identified in the literature review describing the HRQoL impact for caregivers of children with GSDIa. The number of health states was expanded based on feedback gathered from experts and caregivers. The final 15 health states are summarized in Tables 2 and 3. The full health states are available in Appendix 1: Final health state vignettes (see electronic supplementary material [ESM]). Additional details on the development of the health states can be found in the results section.
2.5 Expert and Caregiver Interviews
The draft vignettes were reviewed for content validity by clinical experts and caregivers of people with GSDIa between June 2020 and October 2020. Clinicians were identified through recent research publications in GSDIa and were recruited via email by the study team. Caregivers were identified through contacts at a patient advocacy group. The patient advocacy group shared information about the study with potential participants and, if interested, potential participants were instructed to contact the study team. Caregivers who provided informed consent were invited to take part in the interview. Participants were interviewed via video conference calls (Zoom) using a structured interview guide. Semi-structured interviews were conducted with four caregivers and four clinicians/experts in GSDIa, including two pediatric metabolic consultants from the UK, one pediatric research scientist from the US, and another UK consultant specializing in adult care. The objective of the expert interviews was to ensure clinical accuracy of the vignettes and to identify any missing content or differences between patient groups (such as adolescents that may need to be reflected in a separate vignette). Experts were shown the draft vignettes during the video teleconference and asked to provide feedback.
The caregiver interviews explored the HRQoL of patients and caregivers and included a review of the vignettes. Participants were all adult caregivers or parents of a patient with GSDIa, were able to speak and read English fluently, and able to understand the study. Participants received an honorarium for their time. The draft vignettes were amended using an iterative approach when inaccuracies or a lack of clarity were highlighted by clinicians or caregivers. Other changes to the content of the vignettes were made until a consensus was reached.
2.6 Health State Valuation
2.6.1 Participants
A sample of the UK general public was recruited by four interviewers using convenience sampling, including snowball sampling, and via the interviewers’ personal social networks. Recruitment aimed to produce a broadly representative sample in terms of age, sex, and ethnicity.
2.6.2 Time Trade-Off Method
The TTO interview approach was used to value the patient and caregiver vignettes. The TTO method is a recognized interview technique for valuing health states, and was used in the current study to generate health state utilities for each patient and caregiver health state [19, 20]. This approach is designed to establish the point that the respondent considers 10 years in the target health state equivalent to living in full health for X number of years for each health state. Time in full health was varied using a ‘ping pong’ approach, whereby the time in full health that participants were comparing with the target health state was switched back and forth (i.e., from 9 years to 1 year) at 6-month intervals [19, 20]. Full health was used as the upper anchor in the valuation exercises for both patient and caregiver health states.
If participants indicated that they would rather be dead than live any time in a health state, then this indicated that the participant believed the state to be worse than dead. In such cases, states were then assessed using the lead-time TTO approach during which participants were asked to choose between (1) living in full health for 10 years followed by 10 years in the health state or (2) living for 20 years in full health. The point of indifference was then determined in the same way.
2.6.3 Data Collection
Interviews were conducted in November 2020 by trained interviewers using online video calls (Skype or Zoom). Prior to the TTO interview, participants were provided with information about the study and asked to sign a consent form if they were eligible (aged ≥ 18 years, resident of the UK, able to read and write English, able to have a video call using Skype or Zoom, did not care for a child with a serious condition, and willing to provide informed consent to take part in the study). Participants were also asked to complete a brief background questionnaire and the EQ-5D-5L [21] to measure their current health status.
In preparation for the online interview, participants were asked to either print the vignettes or display them on one screen (monitor/laptop/tablet) and conduct the online video chat on a second screen (e.g., phone/tablet/laptop/monitor), so that the interviewer and participant could see each other at all times. To initiate the interviews, participants were asked to read the patient vignette introductory text which asked them to imagine they were living with a metabolic disorder that affected their ability to regulate blood sugar levels. For the caregiver vignettes, specific introductory text was provided which asked participants to imagine themselves as someone who is the primary caregiver/parent of a 10-year-old sedentary child with GSD1a. This text made reference to the corresponding patient’s health state to contextualize the caregiver burden (e.g., cornstarch/feeding requirements, symptoms, impacts on everyday activities). Both caregiver vignettes explicitly described how the caregiver was affected and were framed in the first person (e.g., “You frequently feel tired…”). In the TTO and VAS valuation tasks, the caregiver vignettes were evaluated against a vignette described as ‘full health’, which made no explicit reference to caregiving but stated simply that the participant was in a state of full health. Participants were thought to assume that the full-health state meant that they had no health burden associated with caring for a child. Participants were blinded to the descriptive titles of all health states.
Given the large number of vignettes, the health states were split into two sets so participants did not value all health states. Participants were then instructed to look at the patient vignettes one by one and asked to imagine themselves in the health state. They were then asked to rank the severity of each vignette from 0 (worst possible state) to 100 (full health) on a visual analogue scale (VAS). This included rating the ‘dead’ vignette (described as ‘You are dead’), allowing participants to indicate if they considered any of the vignettes to be worse than dead. Interviewers randomized the order that participants rated the vignettes. After the VAS exercise, participants completed the TTO interview for each vignette. As described above, the point of indifference was recorded as the utility value. Following the TTO interview, participants were asked to complete the EQ-5D-5L questionnaire to rate each vignette (i.e., imagining themselves in the health state and then completing the EQ-5D-5L to assess that state). This approach for valuing vignettes is recommended by the Decision Support Unit (DSU) in their guidance for measuring and valuing HRQoL when EQ-5D data collected directly from patients are unavailable [22]. Specifically, participants were asked to imagine themselves in each health state. Participants were then asked to consider each question in the EQ-5D and provide an answer that they felt best fits the description being valued. Respondents were not made aware of the age of the person described in the patient vignettes so that it did not influence their valuation. Research has shown that describing the age of the person in the vignette can have a large framing effect on valuations [23, 24]. Indeed, adults find it challenging to imagine themselves as a child for a number of reasons. Once all the patient vignettes had been valued, the VAS, TTO, and EQ-5D-5L tasks were repeated for the caregiver vignettes using the same approach.
2.7 Analysis
Socio-demographic information and participant EQ-5D-5L results were summarized descriptively. VAS ratings for each vignette were rescaled such that the value for the dead state was fixed at zero and all other values varied between 100 and the worse health state. The following formula was used to rescale the data:
In this equation, Vʹ is the rescaled VAS value, V is the original VAS value and \({V}_{\mathrm{Dead}}\) is the value given to the Dead state.
The EQ-5D-5L rating for each state was scored using a mapping function for the EQ-5D-5L and scores reflected UK preference weights [25]. As a scenario analysis, EQ-5D-5L ratings were also scored using US preference weights. VAS, TTO, and EQ-5D-5L data were summarized descriptively using means and standard deviations. Unpaired t-tests were used to explore differences between equivalent child and adolescent health states and between health states representing the US and UK standard of care.
3 Results
3.1 Development of the Health State Vignettes
3.1.1 Targeted Literature Review
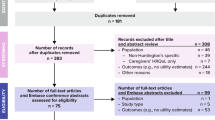
A total of 50 studies met the eligibility criteria for full-text review. A further 18 studies were excluded after full-text review, leaving 32 studies for consideration. A flow diagram showing the identification of papers is shown in Fig. 1.

Flow diagram showing the identification of studies
The impacts of GSDIa reported in the literature were summarized in relation to key dimensions of HRQoL. Where possible, findings were summarized by age (childhood, adolescence, and adulthood). The review highlighted that GSDIa is associated with significant symptomatic burden and currently can only be managed through a strict and taxing dietary regimen, including frequent cornstarch consumption. Frequent feeding is essential to avoid hypoglycemic episodes, but it does not address the underlying disease or prevent progressive complications. Hypoglycemia can induce a number of symptoms including sweating, seizures, headache, rapid breathing, and shakiness [11,12,13]. For severe episodes, patients may need to be hospitalized [12, 14]. Furthermore, patients can experience a range of longer-term complications, including hepatic and renal complications, osteoporosis, anemia, stunted growth, anxiety and depression, delayed puberty, learning disabilities, and psychosocial issues [11, 15, 16]. GSD patients experience greater levels of internalizing problems (e.g., anxiety and depression) and social issues compared with healthy controls [8]. The frequent consumption of cornstarch can lead to obesity, insulin resistance, and reduced appetite, resulting in nutrient deficiencies [26, 27]. Some complications emerge more frequently in the second and third decades of life, such as osteoporosis, hepatocellular carcinoma, and anxiety or depression [4, 12, 16, 17]. Impacts to daily life include restricted physical activity because of an increased injury risk due to hepatomegaly [9], and patients may tire more quickly compared with their peers [9].
The feeding regimen also places considerable burden on caregivers of GSDIa patients. Caregivers spend a significant amount of time planning and organizing nutrition and cornstarch requirements [9, 12]. Nocturnal feeds can result in sleep disturbances and fatigue for both patients and caregivers [12, 28]. There is considerable fear and anxiety over missing cornstarch doses or meals [12], and meal times can be particularly stressful for both patients and caregivers [18]. Patients and caregivers also worry about current management approaches becoming less effective over time [9, 12].
3.1.2 Expert Interview Findings
Overall, the experts (n = 4) felt that the vignettes captured the major impacts of GSDIa. Differences in the standard of care between the UK/Europe and the US were identified. Experts highlighted that nearly all children, adolescents, and even some adult patients are continually tube fed through the night in the UK and Europe, while most are woken for feeds during the night in the US. This regional management difference could differentially impact patient and caregiver HRQoL. Caregivers of children who are tube fed through the night experience considerable anxiety due to the risk of equipment failing and a serious hypoglycemic event occurring as a result. Because of these management differences, separate vignettes for the pre-treated health states for children, adolescents, and caregivers were developed to represent the differences between Europe (EU) and US current management resulting in three additional patient vignettes and one additional caregiver state. The 15 total health states are outlined below.
-
Pre-treated sedentary (US child, EU child, EU adolescent, US adolescent, adult, EU caregiver, US caregiver).
-
Pre-treated active (US child, EU child, and adult).
-
Treated responder (child and adult).
-
Treated complete responder (child, adult, and caregiver).
In addition, clinicians highlighted some missing impacts (e.g., limited independence for adolescents, restricted alcohol intake in adults, and emergency feeding routine), some irrelevant impacts/symptoms (e.g., joint pain, constipation) and recommended revising of some content (e.g., normalizing diet and feeding frequency for treated states). Clinicians reviewed and approved the final vignettes. The feedback and relevant modifications to the draft vignettes are summarized in Appendix 2: Clinician comments and health state description modifications (see ESM).
3.1.3 Caregiver Interview Findings
Caregivers had experience caring for their children between 4 and 42 years old with GSDIa. Patient vignettes were believed to be accurate; however, cornstarch volumes were considered to be too high across all patient states. In practice, cornstarch consumption can vary among patients and does not necessarily align with generic guidelines. The text describing the volume of cornstarch was simplified to phrases such as ‘a large amount’ or ‘you do not need to consume a cornstarch drink’. The severities described for impacts on social activity, anxiety, physical activity, and sleep disturbance (in EU states) were also revised based on caregiver recommendations. Impacts considered irrelevant were removed from the vignettes, including impacts on learning disability and stature in the child states. There was consensus among experts and caregivers that due to improvements in the management of GSD1a, current child patients are generally unaffected if patients are adequately managed. Adult patients may still be shorter than average so this was retained in the adult health states.
Caregiver vignettes were also believed to be accurate. Some missing impacts (e.g., inability to work and spend time with other children) were identified and subsequently added to the health states. Some statements were also revised based on caregiver feedback to emphasize the organization required to manage the feeding schedule and the impact on usual/social activities, sleep disturbances, and anxiety/worry. All modifications to the vignettes are summarized in Appendix 3: Caregiver comments and health state description modifications (see ESM).
3.2 Health State Valuation
3.2.1 Sample Characteristics
The characteristics of the participants who took part in the TTO valuation interviews, together with data for age, sex, and ethnicity from the most recent UK census (2011) are shown in Table 4. The present sample was largely similar to the UK census data according to age, sex, and ethnicity. The prevalence of long-term conditions was lower than that observed in the latest UK opinions and lifestyle survey conducted in 2013 [29]. Indeed, participants also had fewer problems across all dimensions of the EQ-5D compared with recent population data from England [30].
3.2.2 Health State Results
Table 5 shows the mean TTO weights, VAS ratings, and EQ-5D derived weights for patient health states. The results show a significant HRQoL burden for patients with GSDIa and their caregivers. Mean TTO ratings for child patient states ranged from 0.48 (pre-treated sedentary US) to 0.94 (child complete responder, EU/US). Similar differences between levels of severity/treatment response were observed for adult patient states (pre-treated sedentary EU/US: 0.59 vs complete responder, EU/US: 0.94). However, TTO scores were lowest for the adolescent pre-treatment state (adolescent pre-treated sedentary, US: 0.38). For both child and adult health states, large gains in HRQoL were observed for vignettes describing treated patients with a response and a complete response. There was also evidence suggesting that the perceived burden is greater for adolescents compared with children and adults. EQ-5D values were significantly lower for adolescent states when compared with equivalent child states (p < 0.001). A similar pattern of results was observed for the TTO weights, but differences were not statistically significant (p = 0.071–0.113). The burden was also greater for patients receiving the standard of care in the US (i.e., receiving cornstarch orally through the night) versus the UK (i.e., tube feeding through the night), with some statistically significant differences observed in EQ-5D values (p = 0.007–0.197) and TTO weights (p = 0.013–0.057).
Overall, the mean scores for the EQ-5D proxy evaluation show a similar pattern and range as the TTO weights, but the EQ-5D values were consistently lower than the corresponding TTO weights. Mean VAS ratings also show a similar pattern to the TTO weights and EQ-5D values.
Table 6 presents the utility ratings for the caregiver health states. Mean caregiver TTO weights ranged from 0.57 (pre-treated sedentary, EU) to 0.95 (complete responder, EU/US). The utility ratings showed a similar pattern to the patient health states, with large gains in HRQoL for caregivers of patients with a complete response. No statistically significant differences were observed between US and UK standard-of-care caregiver states (p > 0.05).
EQ-5D ratings were also scored according to US preference weights (Appendix 4. EQ-5D utility ratings for patient and caregiver health state vignettes using US EQ-5D value sets, see ESM). The ratings were consistently higher using the US preference weights, but the overall pattern of results was the same when using the UK preference weights.
4 Discussion
This report describes work to estimate health state utilities related to GSDIa. These findings may be useful for families affected by GSDIa, clinicians, and regulatory agencies, but the study was primarily designed to support economic analyses and to quantify HRQoL for this rare disease. This study used the vignette methodology with a convenience sample of the UK general public to value different GSDIa health states using the TTO approach, the VAS, and a proxy rated EQ-5D-5L. Results were largely consistent across the three measures, although EQ-5D values were consistently lower than the corresponding TTO weights, a finding that has been observed in previous studies and may reflect that the TTO task requires participants to trade life-years in their decisions, which may be difficult for some respondents [31].
Utility data are required by decision makers, such as the National Institute for Health and Care Excellence (NICE), to understand the burden of disease and to assess the cost effectiveness of treatments. Utilities are typically assessed with a preference-based measure like the EQ-5D, providing decision makers with a degree of standardization to support interpretation of the data. However, as noted earlier, capturing utility data in ultra-rare conditions can be challenging given the difficulties with recruiting and collecting data in these hard-to-reach populations.
The vignette methodology relies heavily on the accuracy of health state descriptions. To ensure the vignettes accurately describe GSDIa health states, multiple data sources were employed in their development with the intention that each vignette element was supported by at least two data sources. The literature review provided detailed information regarding the nature of the condition, wide-ranging impacts of the condition, and daily management requirements, all of which informed the development of the initial health state descriptions. These descriptions were subsequently revised based on feedback from caregivers and clinical experts. Clinicians approved the final vignettes after the modifications were made. Combining multiple sources of information and iterative feedback in vignette development was intended to improve vignette content validity. The impacts of GSDIa on daily life captured in the vignettes are also consistent with findings from a recent survey including 27 adult GSDIa patients from Germany [32], providing further evidence to support the content validity of the vignettes.
The present findings highlight the impact of GSDIa on HRQoL at different ages and levels of a hypothetical treatment response. Notably, participants were not informed about the age of patients described by the vignettes. Previous studies have shown that participants are generally less willing to trade years of life when imagining child health states, resulting in higher utilities for child health states compared with adult health states [23, 24].
To our knowledge, no previous studies have estimated utility values in GSDIa. Recent research has used the TTO approach to estimate utilities in Pompe disease (GSD type II). This condition has a very different symptomatic burden, including severe muscular and respiratory impairments [33]. TTO values for the adult health states were comparable between these studies, with a consistently lower perceived burden for adult health states. The larger disutility for child health states may be due to the more intense feeding routine and the increased urgency for medical attention due to illness or missed feeds. In the present study, the perceived burden was greatest for adolescent patient states, plausibly because of the increased psychological impact, particularly around self-consciousness, body image, and lack of independence. Our data also suggest that the perceived burden may be different for the EU versus US standard of care, but given the small sample size these differences should be interpreted with caution. Similarly, Simon et al., observed a large disutility for parents of children with Pompe disease, particularly in those with moderate to severe symptoms [33].
Some important limitations should be considered when interpreting our study results. The vignette methodology could be criticized because the results are highly dependent on the accuracy of the descriptions of each health state. It is possible that the descriptions may be too severe or that they underemphasize HRQoL impacts. For example, the health state describing a complete treatment response was largely hypothetical because currently such a state is not seen clinically. To support the content of the vignettes, the study used multiple sources of information, including a targeted literature review and feedback from experts and caregivers to support content validity. It is possible that the views of the caregivers and clinicians with whom we spoke may not be representative of the views of the wider expert community. It should also be considered that the TTO data were collected from a relatively small convenience sample which may not be entirely representative of the UK general population. Although the characteristics of the present sample broadly aligned with the UK census data, fewer long-term conditions and health problems across EQ-5D dimensions were reported compared with recent population data [29, 30]. Lastly, it is worth noting that the caregiver states also referenced how the child was affected in order to provide context. It is possible that this affected how people viewed and valued the caregiver states.
This study benefitted from utility ratings using the EQ-5D and TTO methodology. The TTO has historically been the standard approach for assessing vignettes [20]. However, there is increasing interest in using a proxy assessment of vignettes using the EQ-5D. By presenting both TTO scores and EQ-5D values for the same states, modellers and decision makers can decide which they interpret to be most appropriate.
5 Conclusion
This study demonstrates the perceived burden of GSDIa to patients and caregivers and potential improvements in HRQoL following a successful hypothetical treatment for GSDIa in a convenience sample from the UK general public.
References
Bali DS, Chen YT, Austin S, Goldstein JL. Glycogen storage disease type I. Seattle: University of Washington; 2016.
Parikh NS, Ahlawat R. Glycogen Storage disease type I (Von Gierke disease). Tampa: StatPearls, StatPearls Publishing; 2019.
Kishnani PS, Austin SL, Abdenur JE, Arn P, Bali DS, Boney A, et al. Diagnosis and management of glycogen storage disease type I: a practice guideline of the American College of Medical Genetics and Genomics. Genet Med. 2014;16(11): e1.
Kim YM, Choi JH, Lee BH, Kim GH, Kim KM, Yoo HW. Predominance of the c.648G > T G6PC gene mutation and late complications in Korean patients with glycogen storage disease type Ia. Orphanet J Rare Dis. 2020;15(1):45.
Kaiser N, Gautschi M, Bosanska L, Meienberg F, Baumgartner MR, Spinas GA, et al. Glycemic control and complications in glycogen storage disease type I: Results from the Swiss registry. Mol Genet Metab. 2019;126(4):355–61.
Dambska M, Labrador EB, Kuo CL, Weinstein DA. Prevention of complications in glycogen storage disease type Ia with optimization of metabolic control. Pediatr Diabetes. 2017;18(5):327–31.
Martens DHJ, Rake JP, Navis G, Fidler V, Van Dael CML, Smit GPA. Renal function in glycogen storage disease type I, natural course, and renopreservative effects of ACE inhibition. Clin J Am Soc Nephrol. 2009;4(11):1741–6.
Storch E, Keeley M, Merlo L, Jacob M, Correia C, Weinstein D. Psychosocial functioning in youth with glycogen storage disease type I. J Pediatr Psychol. 2008;33(7):728–38.
Gill T, Gick J, Gribben J. Glycogen storage disease a parent/carers’ guide [Internet]. 2018. http://agsd.org.uk/wp-content/uploads/2019/01/Evelina-booklet-Oct-2018-2.pdf. Accessed 20 Mar 2023.
Shah KK, O’Dell SD. Effect of dietary interventions in the maintenance of normoglycaemia in glycogen storage disease type 1a: a systematic review and meta-analysis. J Hum Nutr Diet. 2013;26:329–39.
Özen H. Glycogen storage diseases: new perspectives. World J Gastroenterol. 2007;13(18):2541–53.
Ultragenyx: data on file. GSDIa Patient Advocacy: Patient and Caregiver Summary and Recommendations. 2019.
Endocrine Society’s 96th Annual Meeting and Expo, June 21–24, 2014 – Chicago, Endocrine Reviews, Volume 35, Issue Supplement, 1 August 2014, Pages i1–i1153, https://doi.org/10.1093/edrv/35.supp.1.
Hazlehurst J, Johnson J, Geberhiwot T, Newsome P, Webber J, Ghosh S. The chronic and acute management of glycogen storage disease type 1 causes difficulties both in diagnosing diabetes and managing glycaemic variability: a case report. Diabet Med. 2014;1(31):83.
Rake JP, Visser G, Labrune P, Leonard JV, Ullrich K, Smit GPA. Glycogen storage disease type I: diagnosis, management, clinical course and outcome. Results of the European Study on Glycogen Storage Disease Type I (ESGSD I). Eur J Pediatr Suppl. 2002;161:S20–34.
Baker L, Dahlem S, Goldfarb S, Kern EFO, Stanley CA, Egler J, et al. Hyperfiltration and renal disease in glycogen storage disease, type I. Kidney Int. 1989;35(6):1345–50.
Bindi V, Eiroa H. Retrospective study in glycogen storage disease type I (GSD I): a cohort from Garrahan Hospital. Abstracts presented at the 13th international congress of inborn errors of metabolism—ICIEM 2017. J Inborn Errors Metab Screen. 2017;5:232640981772229. https://doi.org/10.1177/2326409817722292.
Martinez CC, Tonon T, Nalin T, Refosco LF, de Souza CFM, Schwartz IVD. Feeding difficulties and orofacial myofunctional disorder in patients with hepatic glycogen storage diseases. JIMD Rep. 2019;45:21–7.
Griebsch I. Economic evaluation in health care: merging theory with practise. Int J Epidemiol. 2002;31(4):877–8.
Torrance GW. Measurement of health state utilities for economic appraisal. A review. J Health Econ. 1986;5(1):1–30.
Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res [Internet]. 2011 [cited 2021 May 11];20(10):1727–36. https://pubmed.ncbi.nlm.nih.gov/21479777/. Accessed 20 Mar 2023.
Rowen D, Brazier J, Wong R, Wailoo A. Measuring and valuing health-related quality of life when sufficient EQ-5D data is not available [Internet]. 2020. http://nicedsu.org.uk/wp-content/uploads/2021/07/DSU-hierarchy-of-evidence-report-310720-Final-for-website-1.pdf. Accessed 20 Mar 2023.
Dewilde S, Janssen MF, Lloyd AJ, Shah K. Exploration of the reasons why health state valuation differs for children compared with adults: a mixed methods approach. Value Health. 2022;25(7):1185–95.
Reckers-Droog V, Karimi M, Lipman S, Verstraete J. Why do adults value EQ-5D-Y-3L health states differently for themselves than for children and adolescents: a think-aloud study. Value Health. 2022;25(7):1174–84.
Van Hout B, Janssen MF, Feng Y, Kohlmann T, Busschbach J, Golicki D, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708–15.
Kishnani PS, Boney A, Chen YT. Nutritional deficiencies in a patient with glycogen storage disease type Ib. J Inherit Metab Dis. 1999;22(7):795–801.
Bhattacharya K. Dietary dilemmas in the management of glycogen storage disease type I. J Inherit Metab Dis. 2011;34(3):621–9.
Rousseau-Nepton I, Huot C, Laforte D, Mok E, Fenyves D, Constantin E, et al. Sleep and quality of life of patients with glycogen storage disease on standard and modified uncooked cornstarch. Mol Genet Metab. 2018;123(3):326–30.
Adult Health in Great Britain, 2013—Office for National Statistics [Internet]. [cited 2022 Sep 28]. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandlifeexpectancies/compendium/opinionsandlifestylesurvey/2015-03-19/adulthealthingreatbritain2013. Accessed 20 Mar 2023.
Mulhern B, Feng Y, Shah K, Janssen MF, Herdman M, van Hout B, et al. Comparing the UK EQ-5D-3L and English EQ-5D-5L Value Sets. Pharmacoeconomics [Internet]. 2018 [cited 2022 Sep 28];36(6):699. /pmc/articles/PMC5954043/.
Lloyd A, Daniel A, Slocomb T. PND107 utilities for X-linked myotubular myopathy to support cost effectiveness modelling. Value Health. 2020;1(23):S642.
Garbade SF, Ederer V, Burgard P, Wendel U, Spiekerkoetter U, Haas D, et al. Impact of glycogen storage disease type I on adult daily life: a survey. Orphanet J Rare Dis. 2021;16(1):1–10.
Simon NJ, Richardson J, Ahmad A, Rose A, Wittenberg E, D’Cruz B, et al. Health utilities and parental quality of life effects for three rare conditions tested in newborns. J Patient Rep Outcomes. 2019;3(1):4.
Acknowledgements
Ultragenyx Pharmaceutical Inc. funded this research. Jamie Ziobro of Ultragenyx Pharmaceutical Inc. provided medical writing assistance in the preparation of this manuscript for submission.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Eliza Kruger, Daniel Aggio, Hayley de Freitas, and Andrew Lloyd. The first draft of the manuscript was written by Daniel Aggio, Hayley de Freitas, and Andrew Lloyd, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data availability
Manuscript data are available as electronic supplementary material.
Compliance with ethical standards
Eliza Kruger is an employee and shareholder of Ultragenyx Pharmaceutical Inc. Daniel Aggio, Hayley de Freitas, and Andrew Lloyd are employees of Acaster Lloyd Consulting Ltd. This research was funded by Ultragenyx Pharmaceutical Inc.
Funding
This study was funded by Ultragenyx Pharmaceutical Inc.
Ethics approval
All study materials were submitted to the Western Institutional Review Board (WIRB) in the United States for ethical review. WIRB reviewed the study materials and determined the study was exempt from ethical review on 21 September 2020 (WIRB Submission Number: 2643053-44684192).
Consent to participate
All participants were provided with information about the study and asked to provide written informed consent prior to participation.
Consent for publication (from parents/participants)
All participants provided written informed consent for publication of the research results.
Code availability
Codes are available upon reasonable request to the corresponding author.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Kruger, E., Aggio, D., de Freitas, H. et al. Estimation of Health Utility Scores for Glycogen Storage Disease Type Ia. PharmacoEconomics Open 7, 627–638 (2023). https://doi.org/10.1007/s41669-023-00397-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41669-023-00397-z