
Abstract
While there are a number of systematic reviews on school-based mental health programs, there appears to be heterogeneity in their overall findings and conclusions, possibly due to the tendency to combine evidence from primary school and high school programs. To investigate the evidence for the effectiveness of targeted (for specific groups) and universal (for all students) mental health programs delivered in secondary schools, a systematic review of systematic reviews was conducted. A systematic search for reviews published from 2015 included outcomes for depression and anxiety—the most common mental health conditions—and quality appraisal of original studies in majority secondary school settings. A total of 395 references were screened and 14 systematic reviews were included. Of reviews that were assessed in full, most were excluded for not clearly separating studies in secondary school settings from primary school settings. Findings were generally positive but heterogenous in terms of quality and long-term outcomes. Interventions were mainly based on cognitive behavioural therapy (CBT), with results showing that targeted interventions are generally effective in the short-term for both anxiety and depression, while universal programs may be effective in some situations, typically in the short term and when programs were CBT-based; where reviews focused on universal resilience programs there were no significant effects. The overview shows a need for systematic reviews focused on secondary school settings, which consider contextual and individual factors that can influence the implementation and effectiveness of programs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Depression and anxiety are amongst the most common mental illnesses affecting adolescents and have been associated with social, school and family problems, poor physical health, and costs for individuals, families, and communities (Bitsko et al., 2018). Early intervention and prevention efforts for depression and anxiety aimed at adolescents have become a high priority in many parts of the world, reflected in global research and public health campaigns (UNICEF, 2022), as well as the expansion of mental health services focused on youth aged 12–25 years (Rocha et al., 2015). While the evidence for early intervention continues to accumulate, there exists a paradox where adolescents experience some of the highest levels of mental health issues yet have the lowest levels of mental health service access of any age group (McGorry & Mei, 2018). This has driven an interest in strategies to support the mental health and wellbeing of young people outside of health systems. One increasingly common strategy is the use of school-based mental health programs. There have now been several systematic reviews published on school-based mental health programs, with mixed conclusions about effectiveness. Most of these reviews, however, have combined research from across primary and secondary school settings, ignoring developmental differences between these age groups as well as contextual factors between primary and secondary education settings. The present overview of reviews seeks to address this gap by summarising the range of existing evidence for high school based universal and selective mental health programs targeting depression and anxiety.
Secondary school years capture a key developmental period for mental health, with global epidemiological data indicating that half of all lifetime mental disorders begin by 18 years of age (Solmi et al., 2022). It is increasingly recognised that secondary schools are uniquely placed as settings for effective intervention in youth mental health as they offer a unique opportunity to reach a large number of adolescents and overcome common barriers to help-seeking and mental health service access such as stigma, physical location and cost. Indeed, young people spend more time at school than in any other institution. The World Health Organization (WHO) acknowledges that schools are well-positioned to support adolescent mental health by providing a setting for large-scale implementation of interventions, across a range of social contexts (WHO, 2012). In light of this, school-based mental health programs have proliferated in recent years. School-based mental health programs vary widely in terms of intervention type, delivery, the provision of ongoing support and involvement of young people. For the purposes of the present review, these programs are broadly classified into two types: mental health promotion programs and mental illness prevention programs. Mental health promotion programs are those which focus on positive development and wellbeing, such as social inclusion, social and emotional skills, and problem-solving. Mental illness prevention programs are those which focus on preventing the development of common mental disorders, such as anxiety and depression. This review will focus on prevention programs for depression and anxiety, due to the prevalence of these conditions amongst adolescents and their far-reaching and significant consequences.
School-based prevention programs can be classified into two main approaches: universal approaches and targeted approaches (Zbukvic et al., 2020). Universal approaches involve all students, regardless of their experience, identity, or level of risk for developing a mental disorder. Targeted “selective” approaches are aimed at particular groups of young people who are identified as having a higher risk of developing a mental disorder—for example, students who live with parents experiencing mental ill-health, or students with a neurodevelopmental condition. Targeted “indicated” approaches are aimed at students who are already experiencing identifiable symptoms below the threshold typically associated with a diagnosable mental disorder. The current overview will present the evidence from systematic reviews focused on universal and/or targeted prevention programs in secondary schools, to help build knowledge about which program type may be most effective for addressing anxiety and depression in adolescents.
There has been much research to date on school-based mental health programs and several systematic reviews have now been published on the topic. However, overall, there appears to be heterogeneity in their findings and conclusions. This may be due to differences in methodological factors such as program type, delivery mode, implementing personnel (e.g., teachers, mental health clinicians, etc.), and outcomes investigated. Mixed findings may also be because many reviews do not separately consider the evidence from primary school and high school programs. Given that the prevalence of common mental illnesses increases substantially in adolescence as compared to childhood, reviews and meta-analyses that conflate the findings from primary and secondary school programs are ignoring critical developmental considerations that may help to clarify whether and why school-based programs are effective in different age groups (Younger, 2016). Overviews of systematic reviews—or, umbrella reviews—involve systematic review and synthesis of the evidence from multiple, existing systematic reviews in a given area. They are a relatively recent approach to evidence synthesis, and are considered particularly helpful for providing insight into the overall state of the evidence in situations where a number of systematic reviews have already been published evaluating interventions for a particular outcome (Hunt et al., 2018). While several systematic reviews on school based mental health programs targeting depression and anxiety have now been conducted, the present review represents the first known umbrella review of this area.
Current Study
The existing evidence from systematic reviews presents mixed findings for the effectiveness of school based mental health programs addressing anxiety and depression, possibly due to combining findings across primary and secondary school populations. To address this, the current study aimed to provide an overview of systematic reviews of research specifically in secondary schools. The present overview identified the overall evidence for different program types, strengths and limitations of the evidence, and opportunities for future research. The research was guided by the overarching research question: What is the evidence for secondary school-based programs for improving depression and anxiety outcomes in young people (aged 12–18 years)?
Methods
This overview is presented using the preferred reporting items for overviews of reviews (PRIOR) (Gates et al., 2022). An internal protocol was developed to document the search strategy, eligibility criteria, data extraction and synthesis procedures. The search strategy was pragmatically designed to originally produce an “Evidence Summary” from key findings (Zbukvic et al., 2020). The review was not registered, but the published “Evidence Summary” provides a record of the purpose and key methods used to produce the review. For the present article, only systematic reviews were included; no supplementary primary studies or grey literature were searched or obtained, and all included articles were assessed for quality and risk of bias. Data collection forms and data extracted from the included studies can be provided by the corresponding author on request.
Search Strategy
Literature was identified using the “Evidence Finder” (https://www.orygen.org.au/Training/Evidence-Finder), a publicly available living database and search engine jointly developed by Orygen and headspace (National Youth Mental Health Foundation). The “Evidence Finder” is a comprehensive repository of peer-reviewed systematic reviews and controlled trials evaluating prevention and treatment approaches for common mental ill-health conditions with a peak onset during adolescence/early adulthood (12–25 years). These conditions include anxiety, depression, bipolar, psychosis, eating disorders, substance-use, and suicide/self-harm. The systematic searching and screening methodology used to create and maintain the Evidence Finder is detailed in published studies (De Silva et al., 2018; Hetrick et al., 2018). Reproducible searches are run annually in MEDLINE, Embase and PsycINFO databases. Retrieved records are screened against pre-defined eligibility criteria, and included studies are coded within the database to support searching according to condition or disorder category, stage of illness, intervention type, and study design. By July 2022, more than 480,000 articles had been retrieved and screened, and over 5000 unique studies included in the Evidence Finder database, covering publication dates 1980 to 30 June 2021. The “Evidence Finder” tool has been used as a searchable information source underpinning published systematic reviews, scoping reviews and evidence mapping reviews (e.g., Bell et al., 2022; Pascoe et al., 2021).
For the present study, the team responsible for maintaining the Evidence Finder (SC, AB) conducted searches in the database for records with study design coded as “systematic review” AND “school” in the title, abstract, keyword or label fields. The original search was run in February 2019 and updated in July 2021 and again in August 2022, identifying records published to 30 June 2021. To ensure coverage of more recently published literature an additional search was conducted in August 2022 of unscreened records retrieved for the Evidence Finder annual update for the period 1 July 2021 to 30 June 2022 (see Appendix for Evidence Finder search strategy). The Evidence Finder’s anxiety and depression search retrievals were searched using the following terms in title, abstract, keyword, and label fields: school AND (systematic review OR (metaanalys OR meta-analys OR meta analys)). Combined, the searching procedure provides coverage for records published from 1980 through to 30 June 2022.
Titles and abstracts of retrieved records were then searched in EndNote using the terms “anxiety” or “depression”. Retrieved articles were screened for eligibility by abstract, using the eligibility criteria. Abstract and full text screening of articles was conducted by IZ, RA, SC, LM, VP and MT working independently using the eligibility criteria, with final eligibility for inclusion confirmed through discussion at team meetings. Where there was any hesitation or disagreement about whether a review should be included, this was resolved via discussion.
Eligibility Criteria
Inclusion criteria were: systematic reviews of controlled trials published in English focused on school-based interventions targeting prevention of, or reduction in, depression and anxiety symptoms, with at least half the participant population (i.e., program recipients) comprising secondary school-aged young people (i.e., 12- to 18-year-olds). The co-primary outcomes were anxiety and depression symptoms and could be measured using any tool and at any time-point. School-based interventions were defined as programs delivered in secondary school settings, either in-curriculum or outside of usual classes (regardless of whether school staff or others delivered the intervention). No restriction was placed on intervention type (e.g., psychosocial, lifestyle interventions) or on comparison condition. Systematic reviews were defined as using a systematic search strategy with or without meta-analysis. Reviews were required to be published from 2015 onwards to focus on recent evidence and limit primary trial overlap, based on the assumption that literature included in recent reviews would cover much of the literature included in previously published reviews.
Exclusion criteria was based on (i) evidence type (articles were excluded if they were non-systematic reviews, primary quantitative research studies, policy evaluations, editorials, conference papers, protocols, theses and book chapters), (ii) participants (reviews were excluded if the mean age of participants was outside of 12–18 years or if less than half the studies were identifiable as being conducted with secondary school age young people age 12–18 years) (iii) interventions (reviews were excluded if they described studies of interventions that did not target depression, anxiety or mental health and/or if they less than half the studies were delivered in a school-based setting) and (iv) outcomes (reviews were excluded if primary outcomes of studies included alcohol or other drug use, psychosis, suicidality, physical health or academic outcomes). Reviews were also excluded if they described interventions delivered in specialist secondary schools. Where a review was later updated, the original review was excluded from results.
Data Extraction and Synthesis
Six authors extracted data from included publications (IZ, LM, MT, RA, SC, VP) using a structured template spreadsheet. Extracted data included: author, year of publication, title of publication, country/countries where primary research was conducted, aims, methodology, findings, conclusions, caveats and biases, and other comments. Results were collated into tables and synthesized into written summaries based on the approach to prevention (targeted, universal), with results classified as statistically significant/non-statistically significant and further by standardized effect size and 95% confidence interval (CI) or credible interval (CrI). Effect sizes were further described according to results of included articles. Results were classified by time-point (immediately post-intervention or follow-up) and intervention type where relevant. A table providing an overview of the characteristics of all included reviews was produced, including details of participants, interventions, analysis and reported results (Table 1). A summary table was produced showing the proportion of the statistically significant positive effects compared to null effects by intervention type and time-point (Table 2). The time-points for this summary information were set to immediately post intervention, 0–6 months post intervention, 6–12 post intervention and 12 + months post intervention.
Risk of Bias
Risk of bias summaries across the primary trials included in each systematic review was extracted by LM, MT, SC and VP. An established four-item checklist for overviews of systematic reviews was used to assess potential bias both within and across included systematic reviews (Ballard & Montgomery, 2017). The four items include: (1) overlap, (2) rating of confidence from the AMSTAR 2 checklist, (3) date of publication, and (4) match between the scope of the included review and the overview itself. Each of these items are described in detail below.
It is also important to assess overlap in the use of the primary studies across multiple systematic reviews, as high overlap can contribute to biased results. The corrected covered area (CCA) is a comprehensive and validated measure of overlap that has been used in a previous review of reviews of school-based interventions (Levinson et al., 2019). The CCA is calculated based on three variables: the number of “index” primary trials (r), the number of total trials (including any multiple counts) (N), and the number of systematic reviews (c) in the overview. Each “index” trial represents the first time a primary trial is included in an overview. CCA overlap scores are interpreted as slight (0–5), moderate (6–10), high (11–15) or very high (> 15). The CCA formula is as follows:
The AMSTAR 2 checklist was used to evaluate the quality of included systematic reviews (Shea et al., 2017). The checklist includes 16 items assessing methodological quality. All SRs were assessed by one reviewer (LM, MT or VP) and a second reviewer (SM) duplicated the appraisal of 20% of SRs, with 93% agreement and only minor disagreements that had no impact on confidence grades. It is recommended that review authors determine which of 16-items from the AMSTAR 2 checklist are critical and non-critical for their review and use these to grade included systematic reviews (Shea et al., 2017). Based on this recommendation grades of confidence for each review were produced based on critical flaws and non-critical weaknesses (see Table 3).
The checklist includes date of publication, to ensure results are up to date. Systematic reviews published in the last five years (e.g., 2017 onwards) were considered up to date. The final item is the match between the scope of the overview and the primary trials within included systematic reviews. In this overview, only systematic reviews with a minimum of 50% of their primary trials fulfilling inclusion criteria for age/setting (secondary school) were included. Systematic reviews with a higher proportion of primary studies fulfilling the inclusion criteria were considered a better match.
Results
Results of the Search
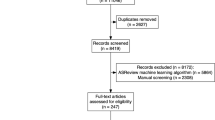
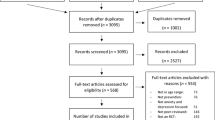
The original search (February 2019) retrieved 145 reviews, of which six were included (Bastounis, 2016; Caldwell et al., 2019; Dray, 2017; Ferreira-Vorkapic, 2015; Sancassiani, 2015; Werner-Seidler, 2017). The updated searches (July 2021, August 2022) resulted in the retrieval and screening of an additional 37 reviews and the inclusion of an additional four articles. A supplementary search (August 2022) within the unscreened search retrievals identified for the 2021–2022 Evidence Finder update resulted in retrieval and screening of an additional 231 reviews and inclusion of an additional five articles (Bradshaw et al., 2021; Fulambarkar et al., 2022; Kambara & Kira, 2021; Karukivi et al., 2021; Werner-Seidler et al., 2021). Twenty-five reviews were assessed in full but not included because the age group did not meet criteria (Cordier et al., 2021), the settings of included studies were not majority secondary school (Bennett, 2015; Cristea, 2015; Erford, 2015; James, 2015; Labelle, 2015; Oldham-Cooper, 2017; Townshend, 2016) or could not be confirmed as majority secondary school setting (Ahlen, 2015; Hetrick, 2015; Hetrick, 2016; Stockings, 2016), outcomes did not include depression or anxiety (Bennett, 2015; Das, 2016; Labelle, 2015; Lee et al., 2017; Meekums, 2015; O'Dea, 2015; Weaver, 2015; Zalsman, 2016), studies were not quality-appraised (Bernecker, 2017; Nanthakumar, 2018), or the record was an abstract not a review paper article (Chahar, 2015; Cowen, 2014; Galling, 2018). One review was updated in the time that searches were conducted so the original review has been excluded from results (Werner-Seidler, 2017). Figure 1 provides an overview of the exclusion and inclusion of reviews.

Flow diagram for inclusion and exclusion of reviews
Study Characteristics
In total, fourteen systematic reviews were included that considered findings for school-based mental health programs with outcomes for anxiety and/or depression (Bastounis, 2016; Bradshaw et al., 2021; Caldwell et al., 2019; Dray, 2017; Feiss et al., 2019; Ferreira-Vorkapic, 2015; Fulambarkar et al., 2022; Gee et al., 2020; Hugh-Jones et al., 2021; Kambara & Kira, 2021; Karukivi et al., 2021; Ma et al., 2020; Sancassiani, 2015; Werner-Seidler et al., 2021). Table 1 provides an overview of all included reviews with key findings for depression and anxiety outcomes, number of included studies and participants, program and intervention types, and comparison conditions. The majority of studies focused on CBT-based interventions, but reviews included research on a range of interventions including health promotion, life and social skills, resilience programs, yoga-based programs, interpersonal therapy-based programs, emotion regulation and other psychological and physical health-based interventions. Most significant findings related to reviews of majority CBT-based programs. Where reviews focused on universal resilience programs, there were no significant effects. All reviews included studies with a range of comparison conditions including no intervention, waitlist, attention control, and many compared to usual curriculum.
Description of Review Findings
Although the present overview only included systematic reviews of research majority conducted in secondary school settings, most reviews combined findings from across secondary and primary school participants or settings. Out of fourteen reviews, four focused on studies specifically in secondary school settings (Feiss et al., 2019; Fulambarkar et al., 2022; Kambara & Kira, 2021; Karukivi et al., 2021). Of those four, two reviews examined the effectiveness of universal programs and found no significant effects overall for either anxiety or depression outcomes (Fulambarkar et al., 2022; Kambara & Kira, 2021) while two reviews that examined targeted indicated programs found significant effects for anxiety and depression outcomes for CBT-based programs up to 12 months (Kambara & Kira, 2021; Karukivi et al., 2021) and one review that combined findings from universal and targeted programs found significant effects in the short- but not long-term (Feiss et al., 2019). Three reviews conducted separate (Caldwell et al., 2019; Dray, 2017) or sub-analyses (Werner-Seidler et al., 2021) with adolescent age groups. From these findings, there was weak evidence for CBT-based programs as a universal intervention for anxiety and depression up to 12 months, and no evidence for effectiveness beyond a year (Caldwell et al., 2019), while another review found no significant evidence for universal programs in secondary settings (Dray, 2017). These reviews also produced some limited evidence for CBT-based programs as a targeted intervention for both anxiety and depression, but where results were combined for universal and targeted interventions in a review focused on secondary school, effects were limited to the first 3 months post-intervention (Feiss et al., 2019). No reviews compared the effectiveness of targeted or universal approaches in primary vs secondary school settings, however, one review conducted subgroup analysis and found no difference between effect sizes by age (Werner-Seidler et al., 2021). That review found small effect sizes for universal and targeted programs overall across multiple time-points beyond 12 months after intervention. When compared using subgroup analyses, there were no significant differences between universal and targeted programs for anxiety, while for depression there were significantly smaller effect sizes for universal programs compared to targeted in the short term, though these were not maintained at follow-up (Werner-Seidler et al., 2021).
For reviews that combined results from research with primary and secondary school students without separate analyses, there was mixed evidence for universal programs. For depression outcomes, some reported significant effects (Ferreira-Vorkapic, 2015; Ma et al., 2020) while others reported no effect (Bastounis, 2016; Sancassiani, 2015). Likwise for anxiety, there was some evidence for effectiveness of universal programs short term (Ferreira-Vorkapic, 2015) while others found no effect (Bastounis, 2016; Sancassiani, 2015). There were reasonably consistent positive findings for targeted programs from reviews that combined results from primary and secondary settings in the short-term, however these were not maintained beyond 6–12 months (Gee et al., 2020; Hugh-Jones et al., 2021; Ma et al., 2020).
Overall, there was more evidence available for universal than targeted interventions, and only a small number of reviews directly compared these approaches. Table 2 provides a summary of the overarching findings across reviews and shows that evidence was strongest for the efficacy of targeted interventions for both depression and anxiety, particularly directly after the intervention, with greater heterogeneity in longer term effects. In contrast, universal programs were found to be effective in less than half of the reviews on anxiety, and just over one-third for depression, with less support again for the efficacy of such programs long term.
Across reviews, facilitators included health workers and doctors, researchers, school counsellors, teachers, psychologists, graduate students, and other trained instructors. There was no evidence for different outcomes between mental health professionals or teachers in two reviews (Bastounis, 2016; Caldwell et al., 2019), while another review found that interventions were more effective, especially at longer term follow ups, when delivered by mental health professionals (Ma et al., 2020). Another review found that indicated interventions delivered by teachers had no impact on depression or anxiety symptoms (Gee et al., 2020). The original and updated review published by one group suggested a slight preference for external personnel over school staff, though the earlier review found no significant difference between groups for anxiety outcomes, and across both reviews’ findings were not maintained at longer-term follow-up (Werner-Seidler et al., 2021; Werner-Seidler, 2017). Digital and face-to-face approaches also appear to be similar in terms of effectiveness, although there is less evidence currently available for digital interventions (Caldwell et al., 2019; Gee et al., 2020; Werner-Seidler et al., 2021). Most studies in included reviews were conducted English-speaking countries including Australia, Canada, and the USA.
Quality Appraisal of Included Systematic Reviews
The CCA was found to be 5.98%, which represents a moderate overlap between the 14 systematic reviews covering 319 studies. Detailed explanations and calculations for the CCA can be found in the Appendix. Table 3 presents the checklist for quality appraisal of included reviews. The majority of reviews were of moderate to high quality, although there was one low and three critically-low quality reviews. Of note, out of the four reviews that focused on secondary school programs, two were of critically low quality and two moderate quality. A detailed overview of the AMSTAR 2 review rating checklist and quality appraisal of primary studies can be found in the Appendix. Table 4 shows the target outcome of each included systematic review along with the results for other 3 items from the checklist for assessing risk of bias in overviews of reviews. All but three of the systematic reviews were considered up to date by AMSTAR criteria of published in the last five years. The proportion of included relevant primary studies targeting secondary school age young people ranged from 50 to 100%, with four reviews including 100% relevant studies.
Discussion
There have now been several systematic reviews of school-based mental health programs aimed at anxiety and depression published without clear conclusions for effectiveness, possibly due to combining findings from primary and secondary school settings without considering the developmental differences between age groups, or the heightened period of vulnerability for the emergence of anxiety and depression symptoms during secondary school years. This umbrella review sought to address this issue by undertaking a developmentally focused examination of existing evidence for programs delivered in secondary schools specifically. The current umbrella review included fourteen systematic reviews of research on school-based universal or targeted interventions for depression or anxiety, with findings from generally high-quality reviews suggesting that programs can be effective short-term but benefits may diminish over time.
Overall, the results of the present review show that targeted school-based interventions are generally effective at reducing depression and anxiety symptoms in young people, especially at the time of intervention, while universal programs show greater heterogeneity in results. Regardless of intervention or program type, evidence for the long-term efficacy of school-based interventions for depression and anxiety is still mixed and highly variable. It is not clear which programs may be most suitable for secondary school students, as most reviews combined findings from across age groups and settings. The combined results provide some basis for integrating universal or targeted interventions for anxiety and depression into school health and wellbeing programs. However, the heterogeneity in findings and quality across the reviews limits strong conclusions. In particular, limitations in the participant cohorts, study designs, and program implementation strategies leave a number of questions and opportunities for future investigation.
Evidence for Different Program and Facilitator Types
The present overview provides a summary of the different program and facilitator types that have been evaluated in school-based mental health programs. Consistent with previous research, results suggest that targeted programs may be more effective than universal programs (Werner-Seidler et al., 2021). Although it appears that targeted approaches may be more effective than universal, it is essential to acknowledge that the direct comparison of different program types is threatened by confounding factors, particularly symptom levels at baseline. Universal programs include all individuals in a cohort, regardless of mental health needs, whereas targeted interventions focus on those who have greater mental health support needs and therefore have greater potential for improvement relative to universal programs. Such design characteristics make it difficult to effectively compare universal and targeted programs, and may lead to less positive conclusions about the efficacy of universal interventions than are warranted (Feiss et al., 2019). Overall, while findings from the present overview helps to paint a picture of the evidence for school-based programs targeting secondary school students, they also help to show where there are current gaps in the literature and opportunities for future research.
Programs studied in the included reviews were primarily cognitive behavioural therapy-based. While these programs appear to be the most effective targeting depression and anxiety, such conclusions can only be made tentatively as more research on non-CBT programs is needed. There was mixed evidence for the impact of facilitators across the reviews, with most delivered by mental health professionals or teachers. Taken together, the reviews suggest that interventions may be more effective when delivered by mental health professionals rather than teachers, especially for indicated interventions. Results also suggested similar effectiveness for programs delivered in person compared to online, however the research in this area was limited. At least one randomized controlled trial is currently underway focused on understanding the effectiveness of online app-based interventions for mental health delivered in secondary school settings, which will add to the evidence in this area (Werner-Seidler et al., 2020). From the present findings, it is not clear under what conditions specific facilitators and delivery methods can have the greatest impact.
Future research designs should consider the need to understand how, why, and when secondary school programs can be most effective. The importance of separating research in primary and secondary school settings is relevant here too, with major differences in learning environment, processes and structures that can all impact implementation, which can in turn influence the reach and impact of programs (Pearson et al., 2015). Although not the focus of the current review, an understanding of the evidence for cost-effectiveness will also help with decision-making about future investment in universal and/or targeted school-based mental health programs. The field of implementation science offers frameworks to help capture factors that may influence implementation in school settings, as well as cost and efficiency outcomes, which can build relevant knowledge to support decision-makers (Moir, 2018).
Developmental Considerations
The present overview aimed to understand the evidence for secondary school mental health programs by including systematic reviews where it was possible to identify that at least 50% of primary studies were conducted in a secondary school setting or with secondary school age adolescents. All but one included > 60% studies with secondary school age children, suggesting the majority of primary studies in included reviews aligned with the overview scope. However, the mixture of findings from primary and secondary school studies in most included reviews means that results should still be interpreted with some caution. While more recent reviews (e.g., Werner-Seidler et al., 2017, 2021) have addressed this to some extent using sub-group analyses, there is a clear need for systematic reviews that focus on each age group and setting. The present overview offers a step in this direction, presenting the evidence from systematic reviews of majority secondary school-based research.
The developmental differences between primary school age (5–11 years) and secondary school age (12–18 years) are significant, particularly in relation to mental health prevention and treatment needs. These age groups show differences in cognitive abilities, neurobiology, relationships with peers and family; there are also significant differences that come following puberty in terms of romantic relationships, exploration of sexuality and gender, and bodily changes, as well as new social pressures related to academic performance and working towards independent living, all of which can impact and be impacted by mental health and wellbeing (National Academies of Sciences, 2019; Pfeifer & Allen, 2021). These developmental differences have been proposed to explain the rise in rates of mental ill-health between childhood and adolescence. It is perhaps not surprising that targeted programs show stronger evidence for effectiveness in this age group compared to findings for universal programs, where targeted programs can both address the specific needs of adolescents (e.g., peer pressure, academic stress) as well as being more likely to produce positive impacts on symptoms if starting from a higher baseline. Results of the present overview showed that some reviews combining results for primary and secondary school settings reported positive results for universal programs, whereas reviews focused specifically on secondary school did not. It is possible that universal programs may be more suitable and effective for primary school students, which may be confounding results for reviews that combined age groups and settings. This may be due to depression and anxiety symptoms being more amenable to universal intervention earlier in life, or it may be related to differences between settings making implementation more effective. Future research could help to disentangle these questions. The mixed and weaker effects for long-term effects for school-based programs overall may also be interpreted through a developmental lens, considering the rapid and significant changes that occur for adolescent over periods of one year or more. It may be the case that targeted programs benefit from being delivered regularly across secondary school years, however, further research is needed to support this approach.
Limitations of Overview Review Methodology
Overviews of systematic reviews can provide a comprehensive summary of the existing evidence on a topic, but also come with limitations (Ballard & Montgomery, 2017). Overviews are unlikely to include the most recent primary studies due to the time lag between study publication and inclusion in systematic reviews. Therefore, it is possible that more recent studies have addressed the identified research gaps in this study. Additionally, scope mismatch, or when the scope of included systematic reviews is not directly aligned with the overview, can also pose a problem, as conclusions may be based on studies that do not fully address the scope of the overview. Finally, overlap of primary studies between included systematic reviews can bias results and conclusions of overviews. The current study used a CCA analysis, demonstrating a moderate level of overlap in primary studies. Critically, overviews can also only provide conclusions that are accurate when the included reviews are of a high standard. Four of the reviews in this overview were critically low- or low-quality confidence based on the AMSTAR 2 checklist, which included two of the four reviews focused on secondary school research, with the rest of either moderate (n = 7) or high confidence (n = 3). Given the stringency of the checklist, this suggests that overall quality of the included reviews is relatively good (Levinson et al., 2019), however the poor quality found for secondary school research casts some doubt on the conclusions that can be drawn from those reviews. Results of the present overview must be considered in light of these limitations and strengths. The present study is among the first umbrella reviews focused on adolescent research, summarizing the state of knowledge in the area of secondary school-based mental health interventions (Levesque, 2016).
Additional Limitations and Strengths
A limitation of the research included in this overview relates to study settings and the generalizability of findings. Most studies in included reviews were conducted in high income countries such as Australia, Canada, and the USA, limiting generalizability to other socio-economic and cultural contexts. Understanding the impact of these differences is crucial, as one review found that found that programs delivered in lower socioeconomic status secondary school settings were less effective than in high or mixed socioeconomic schools (Caldwell et al., 2019). Similarly, assessing the effectiveness and acceptability of school-based interventions for depression and anxiety for those from culturally and linguistically diverse and LGBTQI + communities, is vital. Such groups often face unique stressors and barriers to help seeking that can exacerbate mental health problems, and may require tailored or adapted interventions to best support their needs (Brown et al., 2016). Future research and systematic reviews must consider the contextual and individual factors that can influence the implementation and effectiveness of school-based programs. Those responsible for program design, implementation, and evaluation should aim to capture inclusive data about student identity and background, and to assess programs delivered in a range of settings. Where the evidence is limited, designers and facilitators should adapt school-based mental health programs according to relevant guidelines and models to ensure culturally responsive practice (Yohannan & Carlson, 2019).
Another limitation of included research relates to study design and outcome measures. While long-term outcomes were mixed overall, interpretation is somewhat limited by long-term impacts not being consistently measured by the same tools. The development of meaningful, appropriate youth mental health measures and outcomes is an area of research focus that will help with future school-based mental health program evaluation and research (Thapa Bajgain et al., 2023). Consensus on measures and study designs will help to promote consistency across the field and enhance opportunities to identify the key mechanisms that could be leveraged to improve program delivery and efficacy. Consistency in the measures used to assess mental health outcomes would also support comparison between approach and program types. Without such information, policy makers, researchers, and leaders in school health are limited by the evidence-base in terms of recommendations for implementation. Most studies compared programs with “non-active” comparison conditions, for instance where students experience the usual curriculum. This makes it difficult to determine in this review whether positive effects relate to the components of programs thought to be beneficial for mental health, such as cognitive restructuring or mindfulness, or whether positive effect relate to indirect effects like additional one-on-one attention for students from facilitators. These sorts of issues related to control conditions are already a criticism of depression prevention trials in wider youth settings. In addition, limited studies included measures of positive mental health or wellbeing. The dual continua model suggests that positive mental health and mental ill-health operate on two spectrums rather than a single continuum (Iasiello et al., 2020). When studies only measure one of these spectrums they may fail to provide a complete picture of the impact of the intervention. Future studies could benefit from adding measures of physical, social or educational functioning. It would also be beneficial to draw upon multiple perspectives by including teachers or parents’ perspectives on the interventions, as the existing evidence is based primarily on student self-report. Future research should aim to tease apart the effectiveness of active program components to better current understandings around which elements of programs are most effective.
The current overview is also limited by the fact that it did not include and compare findings from research in primary school settings to those from secondary school settings. Results presented here provide an umbrella view of research in secondary school settings, which can be helpful for guiding future research and for informing guidance for decision-makers about different program and facilitator types. It would be valuable for future reviews to critically compare and contrast research from across primary, secondary, and indeed tertiary education settings, to fully address developmental and contextual considerations that may influence program effectiveness.
A key strength of the present article was the attempt to answer a question that had not yet been addressed through an overview regarding the effectiveness of school-based programs targeting anxiety and depression in adolescents. Findings are highly relevant to the development of recommendations for decision-makers about secondary school-based mental health programs, where guidance is currently limited and not always evidence-based. The wide reach of secondary schools globally represents an opportunity for international collaboration in research and guideline development to support evidence-based decision making in this area.
Conclusion
Understanding the evidence for secondary school-based programs targeting anxiety and depression—two of the most common mental health challenges faced by young people—represents an important area for early intervention. To date, systematic reviews have tended to combine findings from research in primary and secondary school settings, producing unclear conclusions about program effectiveness for different developmental periods. This overview presents the results of systematic reviews of research focused on secondary school mental health programs. Overall, the findings are encouraging and indicate that secondary school settings may be an appropriate context for effective mental health interventions targeting depression and anxiety outcomes. Results showed that targeted interventions for depression and anxiety are generally effective in the short term, though evidence was less clear for long term outcomes; results for universal programs were heterogenous across short and long-term outcomes. Importantly, the majority of reviews identified for this overview combined findings from primary and secondary school settings and age groups, revealing a need for well-designed systematic reviews that focus on these groups separately. The identified gaps in the present review can inform future research including systematic reviews, as well as recommendations and guidance that can be the basis for improving youth mental health through school-based interventions.
References
Ahlen, J., Lenhard, F., & Ghaderi, A. (2015). Universal prevention for anxiety and depressive symptoms in children: A meta-analysis of randomized and cluster-randomized trials. Journal of Primary Prevention, 36(6), 387–403. https://doi.org/10.1007/s10935-015-0405-4
Bajgain, K. T., Amarbayan, M., Wittevrongel, K., McCabe, E., Naqvi, S. F., Tang, K., Aghajafari, F., Zwicker, J. D., & Santana, M. (2023). Patient-reported outcome measures used to improve youth mental health services: a systematic review. Journal of Patient-Reported Outcomes, 7(1), 14. https://doi.org/10.1186/s41687-023-00556-0
Ballard, M., & Montgomery, P. (2017). Risk of bias in overviews of reviews: A scoping review of methodological guidance and four-item checklist. Research Synthesis Methods, 8(1), 92–108. https://doi.org/10.1002/jrsm.1229
Bastounis, A., Callaghan, P., Banerjee, A., & Michail, M. (2016). The effectiveness of the Penn Resiliency Programme (PRP) and its adapted versions in reducing depression and anxiety and improving explanatory style: A systematic review and meta-analysis. Journal of Adolescence, 52, 37–48. https://doi.org/10.1016/j.adolescence.2016.07.004
Bell, I., Pot-Kolder, R. M., Wood, S. J., Nelson, B., Acevedo, N., Stainton, A., & Allott, K. (2022). Digital technology for addressing cognitive impairment in recent-onset psychosis: A perspective. Schizophrenia Research: Cognition, 28, 100247.
Bennett, K., Rhodes, A. E., Duda, S., Cheung, A. H., Manassis, K., Links, P., Mushquash, C., Braunberger, P., Newton, A. S., Kutcher, S., Bridge, J. A., Santos, R. G., Manion, I. G., McLennan, J. D., Bagnell, A., Lipman, E., Rice, M., & Szatmari, P. (2015). A youth suicide prevention plan for Canada: A systematic review of reviews. Canadian Journal of Psychiatry, 60(6), 245–257.
Bernecker, S. L., Coyne, A. E., Constantino, M. J., & Ravitz, P. (2017). For whom does interpersonal psychotherapy work? A systematic review. Clinical Psychology Review, 56, 82–93.
Bitsko, R. H., Holbrook, J. R., Ghandour, R. M., Blumberg, S. J., Visser, S. N., Perou, R., & Walkup, J. T. (2018). Epidemiology and impact of health care provider-diagnosed anxiety and depression among US children. Journal of Developmental and Behavioral Pediatrics, 39(5), 395–403. https://doi.org/10.1097/dbp.0000000000000571
Bradshaw, M., Gericke, H., Coetzee, B. J., Stallard, P., Human, S., & Loades, M. (2021). Universal school-based mental health programmes in low- and middle-income countries: A systematic review and narrative synthesis. Preventive Medicine, 143, 106317. https://doi.org/10.1016/j.ypmed.2020.106317
Brown, A., Rice, S. M., Rickwood, D. J., & Parker, A. G. (2016). Systematic review of barriers and facilitators to accessing and engaging with mental health care among at-risk young people. Asia-Pacific Psychiatry, 8(1), 3–22. https://doi.org/10.1111/appy.12199
Caldwell, D. M., Davies, S. R., Hetrick, S. E., Palmer, J. C., Caro, P., López-López, J. A., & Welton, N. J. (2019). School-based interventions to prevent anxiety and depression in children and young people: a systematic review and network meta-analysis. The Lancet Psychiatry, 6(12), 1011–1020. https://doi.org/10.1016/s2215-0366(19)30403-1
Chahar, A., Gulati, R., Sharma, J., Likhar, N., & Dang, A. (2015). Impact of community based therapy on children with mental health disorders: A health technology assessment. Value in Health, 18(3), 275.
Cordier, R., Speyer, R., Mahoney, N., Arnesen, A., Mjelve, L. H., & Nyborg, G. (2021). Effects of interventions for social anxiety and shyness in school-aged children: A systematic review and meta-analysis. PLoS ONE, 16(7), e0254117. https://doi.org/10.1371/journal.pone.0254117
Cowen, S. L. (2014). A meta-analysis of school-based depression prevention programs for children and adolescents. Brigham Young University.
Cristea, I. A., Mogoașe, C., David, D., & Cuijpers, P. (2015). Practitioner Review: Cognitive bias modification for mental health problems in children and adolescents: a meta-analysis. Journal of Child Psychology & Psychiatry & Allied Disciplines, 56(7), 723–734. https://doi.org/10.1111/jcpp.12383
Das, J. K., Salam, R. A., Lassi, Z. S., Khan, M. N., Mahmood, W., Patel, V., & Bhutta, Z. A. (2016). Interventions for adolescent mental health: An overview of systematic reviews. Journal of Adolescent Health, 59(4suppl), S49–S60. https://doi.org/10.1016/j.jadohealth.2016.06.020
De Silva, S., Bailey, A. P., Parker, A. G., Montague, A. E., & Hetrick, S. E. (2018). Open-access evidence database of controlled trials and systematic reviews in youth mental health. Early Intervention in Psychiatry, 12(3), 474–477. https://doi.org/10.1111/eip.12423
Dray, J., Bowman, J., Campbell, E., Freund, M., Wolfenden, L., Hodder, R. K., McElwaine, K., Tremain, D., Bartlem, K., Bailey, J., Small, T., Palazzi, K., Oldmeadow, C., & Wiggers, J. (2017). Systematic review of universal resilience-focused interventions targeting child and adolescent mental health in the school setting. Journal of the American Academy of Child & Adolescent Psychiatry, 56(10), 813–824.
Erford, B., Kress, V., Giguere, M., Cieri, D., & Erford, B. (2015). Meta-analysis: Counseling outcomes for youth with anxiety disorders. Journal of Mental Health Counseling, 37(1), 63–94.
Feiss, R., Dolinger, S. B., Merritt, M., Reiche, E., Martin, K., Yanes, J. A., Thomas, C. M., & Pangelinan, M. (2019). A systematic review and meta-analysis of school-based stress, anxiety, and depression prevention programs for adolescents. Journal of Youth and Adolescence, 48(9), 1668–1685.
Ferreira-Vorkapic, C., Feitoza, J. M., Marchioro, M., Simões, J., Kozasa, E., & Telles, S. (2015). Are there benefits from teaching yoga at schools? A systematic review of randomized control trials of yoga-based interventions. Evidence-Based Complementary & Alternative Medicine, 2015, 1.
Fulambarkar, N., Seo, B., Testerman, A., Rees, M., Bausback, K., & Bunge, E. (2022). Review: Meta-analysis on mindfulness-based interventions for adolescents’ stress, depression, and anxiety in school settings: A cautionary tale. Child and Adolescent Mental Health. https://doi.org/10.1111/camh.12572
Galling, B., & Correll, C. (2018). Effectiveness of coordinated specialty care for early psychosis [conference abstract]. Schizophrenia Bulletin, 44(suppl1), S108. https://doi.org/10.1093/schbul/sby015.265
Gates, M., Gates, A., Pieper, D., Fernandes, R. M., Tricco, A. C., Moher, D., & Hartling, L. (2022). Reporting guideline for overviews of reviews of healthcare interventions: Development of the PRIOR statement. BMJ, 378, 070849. https://doi.org/10.1136/bmj-2022-070849
Gee, B., Reynolds, S., Carroll, B., Orchard, F., Clarke, T., Martin, D., & Pass, L. (2020). Practitioner Review: Effectiveness of indicated school-based interventions for adolescent depression and anxiety–a meta-analytic review. Journal of Child Psychology and Psychiatry, 61(7), 739–756.
Hetrick, S., Cox, G., & Merry, S. (2015). Where to go from here? An exploratory meta-analysis of the most promising approaches to depression prevention programs for children and adolescents. International Journal of Environmental Research & Public Health, 12(5), 4758–4795. https://doi.org/10.3390/ijerph120504758
Hetrick, S. E., Cox, G. R., Witt, K. G., Bir, J. J., & Merry, S. N. (2016). Cognitive behavioural therapy (CBT), third-wave CBT and interpersonal therapy (IPT) based interventions for preventing depression in children and adolescents. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD003380.pub4
Hetrick, S. E., O’Connor, D. A., Stavely, H., Hughes, F., Pennell, K., Killackey, E., & McGorry, P. D. (2018). Development of an implementation guide to facilitate the roll-out of early intervention services for psychosis. Early Intervention in Psychiatry, 12(6), 1100–1111. https://doi.org/10.1111/eip.12420PMID-28177191
Hugh-Jones, S., Beckett, S., Tumelty, E., & Mallikarjun, P. (2021). Indicated prevention interventions for anxiety in children and adolescents: A review and meta-analysis of school-based programs. European Child & Adolescent Psychiatry, 30(6), 849–860.
Hunt, H., Pollock, A., Campbell, P., Estcourt, L., & Brunton, G. (2018). An introduction to overviews of reviews: Planning a relevant research question and objective for an overview. Systematic Reviews, 7(39), 1–9.
Iasiello, M., van Agteren, J., & Cochrane, E. M. (2020). Mental health and/or mental illness: A scoping review of the evidence and implications of the dual-continua model of mental health. Evidence Base, 202(1), 1–45. https://doi.org/10.21307/eb-2020-001
James, A. C., James, G., Cowdrey, F. A., Soler, A., & Choke, A. (2015). Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD004690.pub4
Kambara, K., & Kira, Y. (2021). School-based intervention for depressive symptoms in upper secondary education: A focused review and meta-analysis of the effect of CBT-based prevention. Mental Health & Prevention. https://doi.org/10.1016/j.mhp.2021.200206
Karukivi, J., Herrala, O., Sateri, E., Tornivuori, A., Salantera, S., Aromaa, M., & Karukivi, M. (2021). The effectiveness of individual mental health interventions for depressive, anxiety and conduct disorder symptoms in school environment for adolescents aged 12–18-A systematic review. Front Psychiatry, 12, 779933. https://doi.org/10.3389/fpsyt.2021.779933
Labelle, R., Pouliot, L., & Janelle, A. (2015). A systematic review and meta-analysis of cognitive behavioural treatments for suicidal and self-harm behaviours in adolescents. Canadian Psychology/psychologie Canadienne, 56(4), 368–378. https://doi.org/10.1037/a0039159
Lee, R. S. C., Hermens, D. F., Scott, J., O’Dea, B., Glozier, N., Scott, E. M., & Hickie, I. B. (2017). A transdiagnostic study of education, employment, and training outcomes in young people with mental illness. Psychological Medicine, 47(12), 2061–2070. https://doi.org/10.1017/S0033291717000484
Levesque, R. J. R. (2016). Reviews in research on adolescence: Genres, trends, and challenges. Adolescent Research Review, 1(1), 3–13. https://doi.org/10.1007/s40894-015-0022-8
Levinson, J., Kohl, K., Baltag, V., & Ross, D. A. (2019). Investigating the effectiveness of school health services delivered by a health provider: A systematic review of systematic reviews. PLoS ONE, 14(6), e0212603. https://doi.org/10.1371/journal.pone.0212603
Ma, L., Zhang, Y., Huang, C., & Cui, Z. (2020). Resilience-oriented cognitive behavioral interventions for depressive symptoms in children and adolescents: A meta-analytic review. Journal of Affective Disorders, 270, 150–164.
McGorry, P. D., & Mei, C. (2018). Early intervention in youth mental health: Progress and future directions. Evidence Based Mental Health, 21(4), 182. https://doi.org/10.1136/ebmental-2018-300060
Meekums, B., Vicky Karkou, E., & Nelson, A. (2015). Dance movement therapy for depression. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD009895.pub2
Moir, T. (2018). Why is implementation science important for intervention design and evaluation within educational settings? Frontiers in Education. https://doi.org/10.3389/feduc.2018.00061
Nanthakumar, C. (2018). The benefits of yoga in children. Journal of Integrative Medicine, 16(1), 14–19. https://doi.org/10.1016/j.joim.2017.12.008
National Academies of Sciences, E., and Medicine. (2019). The promise of adolescence realizing opportunity for all youth. National Academies Press. https://doi.org/10.17226/25388
O’Dea, B., Calear, A. L., & Perry, Y. (2015). Is e-health the answer to gaps in adolescent mental health service provision? Current Opinion in Psychiatry, 28(4), 336–342. https://doi.org/10.1097/YCO.0000000000000170
Oldham-Cooper, R., & Loades, M. (2017). Disorder-specific versus generic cognitive-behavioral treatment of anxiety disorders in children and young people: A systematic narrative review of evidence for the effectiveness of disorder-specific CBT compared with the disorder-generic treatment, Coping Cat. Journal of Child and Adolescent Psychiatric Nursing, 30(1), 6–17.
Pascoe, M. C., Bailey, A. P., Craike, M., Carter, T., Patten, R. K., Stepto, N. K., & Parker, A. G. (2021). Single session and short-term exercise for mental health promotion in tertiary students: A scoping review. Sports Medicine - Open, 7(1), 72. https://doi.org/10.1186/s40798-021-00358-y
Pearson, M., Chilton, R., Wyatt, K., Abraham, C., Ford, T., Woods, H. B., & Anderson, R. (2015). Implementing health promotion programmes in schools: A realist systematic review of research and experience in the United Kingdom. Implementation Science, 10, 149. https://doi.org/10.1186/s13012-015-0338-6
Pfeifer, J. H., & Allen, N. B. (2021). Puberty initiates cascading relationships between neurodevelopmental, social, and internalizing processes across adolescence. Biological Psychiatry, 89(2), 99–108. https://doi.org/10.1016/j.biopsych.2020.09.002
Rocha, T.B.-M., Graeff-Martins, A. S., Kieling, C., & Rohde, L. A. (2015). Provision of mental healthcare for children and adolescents: A worldwide view. Current Opinion in Psychiatry, 28(4), 330.
Sancassiani, F., Pintus, E., Holte, A., Paulus, P., Moro, M. F., Cossu, G., Angermeyer, M. C., Carta, M. G., & Lindert, J. (2015). Enhancing the emotional and social skills of the youth to promote their wellbeing and positive development: A systematic review of universal school-based randomized controlled trials. Clinical Practice and Epidemiology in Mental Health, 11, 21–40.
Shea, B. J., Reeves, B. C., Wells, G., Thuku, M., Hamel, C., Moran, J., Moher, D., Tugwell, P., Welch, V., Kristjansson, E., & Henry, D. A. (2017). AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. https://doi.org/10.1136/bmj.j4008
Solmi, M., Radua, J., Olivola, M., Croce, E., Soardo, L., Salazar, G., de Pablo, J., Shin, Il., Kirkbride, J. B., Jones, P., Kim, J. H., Kim, J. Y., Carvalho, A. F., Seeman, M. V., Correll, C. U., & Fusar-Poli, P. (2022). Age at onset of mental disorders worldwide large-scale meta-analysis of 192 epidemiological studies. Molecular Psychiatry, 27, 281–295. https://doi.org/10.1038/s41380-021-01161-7
Stockings, E., Hall, W. D., Lynskey, M., Morley, K. I., Reavley, N., Strang, J., Patton, G., & Degenhardt, L. (2016). Substance use in young people 3: Prevention, early intervention, harm reduction, and treatment of substance use in young people. Lancet Psychiatry, 3(3), 280–296.
Townshend, K., Jordan, Z., Stephenson, M., & Tsey, K. (2016). The effectiveness of mindful parenting programs in promoting parents’ and children’s wellbeing: A systematic review. JBI Database of Systematic Reviews and Implementation Reports, 14(3), 139–178. https://doi.org/10.11124/JBISRIR-2016-2314
UNICEF. (2022). The Global Coalition for Youth Mental Well-being. UNICEF. Retrieved March 2023 from https://www.unicef.org/partnerships/coalition-youth-mental-wellbeing
Weaver, L. L., & Darragh, A. R. (2015). Systematic review of yoga interventions for anxiety reduction among children and adolescents. The American Journal of Occupational Therapy: Official Publication of the American Occupational Therapy Association. https://doi.org/10.5014/ajot.2015.020115
Werner-Seidler, A., Huckvale, K., Larsen, M. E., Calear, A. L., Maston, K., Johnston, L., Torok, M., O’Dea, B., Batterham, P. J., Susanne Schweizer, S., Skinner, R., Steinbeck, K., Ratcliffe, J., Oei, J. L., Patton, G., Wong, I., Beames, J., Wong, Q. J. J., Lingam, R., … Christensen, H. (2020). A trial protocol for the effectiveness of digital interventions for preventing depression in adolescents: The future proofing study. Trials, 21(1), 2. https://doi.org/10.1186/s13063-019-3901-7
Werner-Seidler, A., Perry, Y., Calear, A. L., Newby, J. M., & Christensen, H. (2017). School-based depression and anxiety prevention programs for young people: A systematic review and meta-analysis. Clinical Psychology Review, 51, 30–47. https://doi.org/10.1016/j.cpr.2016.10.005
Werner-Seidler, A., Spanos, S., Calear, A. L., Perry, Y., Torok, M., O’Dea, B., & Newby, J. M. (2021). School-based depression and anxiety prevention programs: An updated systematic review and meta-analysis. Clinical Psychology Review, 89, 102079. https://doi.org/10.1016/j.cpr.2021.102079
WHO. (2012, 2012). Adolescent mental health: mapping actions of nongovernmental organizations and other international development organizations. World Health Organization. https://apps.who.int/iris/handle/10665/44875
Yohannan, J., & Carlson, J. S. (2019). A systematic review of school-based interventions and their outcomes for youth exposed to traumatic events. Psychology in the Schools, 56(3), 447–464. https://doi.org/10.1002/pits.22202
Younger, D. S. (2016). Epidemiology of childhood and adult mental illness. Neurologic Clinics, 34(4), 1023–1033. https://doi.org/10.1016/j.ncl.2016.06.010
Zalsman, G., Hawton, K., Wasserman, D., van Heeringen, K., Arensman, E., Sarchiapone, M., Carli, V., Höschl, C., Barzilay, R., Balazs, J., Purebl, G., Kahn, J. P., Sáiz, P. A., Lipsicas, C. B., Bobes, J., Cozman, D., Hegerl, U., & Zohar, J. (2016). Suicide prevention strategies revisited: 10-year systematic review. The Lancet. Psychiatry, 3(7), 646–659. https://doi.org/10.1016/S2215-0366(16)30030-X
Zbukvic, I., Cooke, S., & Anderson, R. (2020). Evidence summary: A review of school-based mental health programs. Orygen. https://www.orygen.org.au/Training/Resources/Depression/Evidence-summary/A-review-of-secondary-school-based-mental-health-p/orygen-schools-evidence-summary-pdf.aspx?ext=
Acknowledgements
The authors would like to acknowledge all contributors to the “Evidence Summary” that inspired this article (see reference: Zbukvic et al., 2020).
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
IZ conceived of the study, participated in its design and coordination, interpretation of the data and drafted the manuscript; SM participated in the design and interpretation of the data and helped to draft the manuscript; SC participated in the interpretation of the data and helped to draft the manuscript; RA participated in the interpretation of the data and helped to draft the manuscript; VP participated in the interpretation of the data and helped to draft the manuscript; LM participated in the interpretation of the data and helped to draft the manuscript; AB participated in the collection and interpretation of the data and helped to draft the manuscript; RP participated in the interpretation of the data and helped to draft the manuscript; MT participated in the interpretation of the data and coordination helped to draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zbukvic, I., McKay, S., Cooke, S. et al. Evidence for Targeted and Universal Secondary School-Based Programs for Anxiety and Depression: An Overview of Systematic Reviews. Adolescent Res Rev 9, 53–73 (2024). https://doi.org/10.1007/s40894-023-00211-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40894-023-00211-1