
Abstract
Introduction
Psoriatic arthritis (PsA) is a complex, progressive, and often debilitating disease. Despite recent advances in treatment, numerous unmet needs in patient care persist. Rheumacensus is a multistakeholder, pan-European initiative designed to identify ways to elevate the standard of care (SoC) and treatment ambition for patients with PsA, using the perspectives of three key stakeholder groups: patients, healthcare professionals (HCPs) and payors.
Methods
Rheumacensus followed three phases: an insights-gathering workshop to identify current unmet needs in PsA and an area of focus for the project, a modified Delphi process to gain consensus on improvements within the agreed area of focus, and a Consensus Council (CC) meeting which used consensus statements as inspiration to generate ‘Calls to Action’ (CTA)—practical measures which, if implemented, could elevate the SoC for patients with PsA.
Results
The Rheumacensus CC consisted of four patient representatives, four HCPs and four payors. All 12 members completed all three Delphi e-consultations. The shared area of focus that informed the Delphi process was “patient empowerment through education on the disease and treatment options available, to enable patient involvement in management”. Four key themes emerged from the Delphi process: patient empowerment, patient knowledge and sources of education, patient–HCP consultations, and optimal initial treatment. Statements within these themes informed 12 overarching CTA, which focus on the need for a multistakeholder approach to implementing a paradigm shift towards patient-centred care and improved outcomes for patients with PsA.
Conclusion
Rheumacensus has identified shortcomings in the current SoC for patients with PsA and provides a foundation for change through practical CTA. It is hoped that all stakeholders will now take practical steps towards implementing these CTA across Europe to elevate the SoC for patients with PsA.
Plain Language Summary
Inequalities in the care patients with psoriatic arthritis (PsA) receive can be mainly explained by poorly coordinated management due to a lack of disease and treatment knowledge. This report is about a programme called Rheumacensus which has the overall aim of improving the standard of care (SoC) for patients with PsA. Rheumacensus brings together the points of view of three key groups involved in the care of people with PsA: patients, payors and healthcare professionals (HCPs) from across Europe. Together, these three groups agreed to focus on patient empowerment through education on the disease and treatment options as a way to raise the SoC. Through a series of exercises—to agree on the current SoC and what needs to be improved—and group discussions, four themes were established which were used by the groups to help them suggest ‘Calls to action’ (CTA). The CTAs were ideas of how improvements could be made or what needs to be done to improve the care patients receive. The four themes were (1) patient empowerment, (2) patient knowledge, (3) patient–HCP consultation and (4) optimal initial treatment. In total, 12 CTAs were developed across these themes that provide direction and practical next steps which patients, payors and HCPs could take to drive change and make a real difference to patients by improving their care.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Several barriers to best practice care in psoriatic arthritis (PsA) exist, preventing patients from achieving optimal outcomes. Rheumacensus is a multidisciplinary, pan-European initiative involving 12 stakeholders evenly representing three key stakeholder groups: patients, healthcare professionals (HCPs) and payors. | |
Stakeholder leads identified a shared area of focus which informed the rest of the programme: patient empowerment through education on the disease and treatment options available, to enable patient involvement in management. | |
A modified Delphi process was used to gain multistakeholder consensus on statements based on insights around the shared area of focus, giving rise to four areas of management requiring improvement (themes): patient empowerment, patient knowledge and sources of education, patient–HCP consultations and optimal initial treatment. | |
Consensus statements were used to inspire ‘Calls to Action’ per theme, designed to bridge the gap between the current and desired care which, if implemented, would contribute to an elevation in the standard of care for patients with PsA. | |
The key areas of action that require change in PsA care focused on many aspects of patient empowerment, including the need to provide support throughout a patient’s treatment journey, signposting them to patient organisations and incorporating shared decision-making and personalised treatment approaches into care. |
Introduction
Psoriatic arthritis (PsA) is an inflammatory arthritis characterised by musculoskeletal and dermatological manifestations. It affects between 6% and 41% of patients with psoriasis [1,2,3]. PsA is a progressive and potentially debilitating disease affecting peripheral and axial joints, entheses and other organs [1, 3, 4]. Symptoms include pain, stiffness, fatigue, diminished physical function and, if untreated, permanent structural joint damage [1, 3,4,5]. Spontaneous remission seldom occurs, meaning appropriate long-term treatment is required to maintain health-related quality of life (HR-QoL) [1, 6]. Evidence suggests the greatest impact on HR-QoL comes from the broader spectrum of PsA manifestations, e.g. comorbidities, fatigue, sleep disturbance, anxiety, depression and the inability to work [5]. Higher total medical costs, arising from increased medication use and hospital visits, are incurred by patients with PsA compared to those with psoriasis alone [7].
Despite the progressive and debilitating nature of the disease and the necessity for appropriate treatment, it is well established that the standard of PsA care is suboptimal. The quality of care that patients receive varies considerably across Europe, but common unmet needs are recognised universally [8].
Given that PsA is a complex, heterogeneous disease affecting many body systems, multidisciplinary management is required for optimal care [1, 9]. Guidelines recommend effective communication between rheumatologists and dermatologists [1, 10], through combined clinics [1, 11, 12]. However, input from specialist nurses, psychologists, clinical pharmacists and patient organisations can also be valuable components of individualised, holistic care [9]. Currently, management pathways are not well defined, leading to variable access to care and suboptimal treatment approaches [1, 8, 9]. Another factor affecting quality of care is a disparity between treatment targets set by physicians, which focus on disease activity outcomes, and the expectations of patients, who value improvements in physical and social functioning, and work productivity [4, 13].
Misaligned treatment satisfaction between patient and physician is linked to greater impairment of work productivity and higher disease burden [14]. Treatment adherence is also a problem, with rates as low as 57.7% [15]. Since PsA impacts many aspects of a patient’s life, treatment recommendations and targets must go beyond simply addressing the musculoskeletal symptoms [4]. Encouraging self-reported patient insights facilitates patient involvement [13], and should include reporting of factors such as pain, fatigue, psychological well-being and treatment satisfaction [5, 13]. Fortunately there has been a shift towards more holistic patient-centric healthcare in recent years [16]. However, practical challenges remain such as overcoming traditional attitudes and the complexity of a multidisciplinary approach [9, 16].
Rheumacensus is a programme that aims to explore the different ways in which the standard of care (SoC) and treatment ambition for patients with PsA can be elevated from the perspective of three important stakeholders: patients, healthcare professionals (HCPs) and payors. Herein, we outline findings of a Delphi exercise undertaken to gain consensus on the current SoC and potential improvements. Additionally, we report ‘Calls to Action’ (CTA) inspired by consensus statements, intended to highlight the actions required by stakeholders to elevate the SoC.
Methods
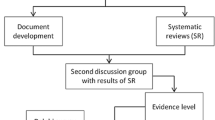
The Rheumacensus programme is a multistakeholder, pan-European initiative designed to identify challenges in the current management of PsA and axial spondyloarthritis (axSpA) and ultimately generate CTA which, if implemented, could improve the overall SoC and treatment ambition for people with these conditions (Fig. 1). The results of the axSpA workstream are published elsewhere [https://doi.org/10.1007/s40744-024-00663-4].

Process of the Rheumacensus PsA programme. *Twelve participants were recruited and contracted; six were female and six were male. All 12 CC participants completed all three Delphi e-consultations. †Two patient representatives, one payor and two HCPs were unable to attend the meeting but provided their CTA after the meeting. CC Consensus Council, CTA ‘Calls to Action’, HCP healthcare professional, PsA psoriatic arthritis, SoC standard of care
Twelve experts with a prominent level of engagement and experience in PsA (e.g. those involved in clinical trials, authors of manuscripts on PsA, treating patients with PsA, involved in funding PsA medications, are a member of a patient organisation or a patient with PsA) were recruited to participate in the PsA Rheumacensus Consensus Council (CC) from a range of different countries across Europe. The CC consisted of three equally represented stakeholder groups: patient representatives, HCPs (rheumatologists, a dermatologist and a nurse) and payors, each with a nominated group lead (Table S1). The aim was to ensure diversity with panellists from different countries and healthcare systems and equal representation of gender as far as possible while recruiting experts with adequate experience of PsA to contribute to the programme.
This manuscript is formed of the opinions of the authors themselves. There was no need to collect any type of patient data. Therefore, the approval of an ethics committee was not required. Consent was obtained from all participants (or stakeholders).
A virtual workshop with the stakeholder group leads took place in June 2022 (via Zoom) to capture real-world insights into the unmet needs in the management of PsA from each stakeholder perspective (Table S2) and prioritise those with the greatest impact on the current SoC while avoiding duplication of existing initiatives [17]. After capturing the unmet needs per stakeholder, discussion revealed that patient-centred, holistic care was a key theme for both patients and payors and underpinned many of the other unmet needs identified, whilst HCPs focused on clinical considerations (e.g. shorter referral times). After reflecting on whether the topics could be addressed by a programme such as Rheumacensus, the shared area of focus was refined and agreed by all the stakeholder leads—patient empowerment through education on the disease and treatment options available, to enable patient involvement in management.
A modified Delphi method was used to explore the agreed area of focus of patient empowerment from the perspective of all three stakeholders with the aim of gaining consensus across stakeholders on the current state of patient empowerment, the need for change and the desired state/action. Three rounds of Delphi e-consultations were distributed to all participants to complete anonymously via Microsoft Forms between September 2022 and January 2023. These comprised statements with multiple-choice answers for level of agreement (strongly agree, agree, disagree, or strongly disagree) to assess consensus (defined as at least 75% of participants selecting ‘agree’ or ‘strongly agree’), and ‘complete the sentence’ and free-text questions to gather further insights. Each successive Delphi round was refined on the basis of feedback from participants from the previous round. All 12 members of the CC took part in this process and completed all three rounds of the Delphi.
Following the Delphi e-consultations, four themes were identified: patient empowerment, patient knowledge and sources of education, patient–HCP consultation, and optimal initial treatment that related to different aspects of the focus area. A narrative per theme was then created by further distilling the statements into the insights they provided relating to the current situation, need for change and desired state/action. This was done to summarise the outcome of the Delphi process to set the scene for the CC meeting where key consensus statements that reflected the desired state/action were used to inspire CTA. Not all the statements that achieved consensus were needed in the narratives. Statements were omitted if they did not add further detail to the narrative to ensure narratives were concise. Statements were also omitted from the narratives if they specifically related to how a change should be implemented and will be considered when the Rheumacensus programme moves into the implementation stage. The purpose of the CC meeting was to generate CTA—practical ideas that if addressed through the implementation of novel initiatives would contribute to an elevation in the SoC of patients with PsA.
The virtual PsA CC meeting took place via Zoom in March 2023. The meeting lasted 3.5 hours and was attended by eight of the 12 CC members, with Andrea Tomasini attending on behalf of Antonella Celano as a patient representative. For each theme in turn, the narrative was presented and then consensus statements that described the desired SoC were used to stimulate the generation of CTA. This was done in breakout rooms to separate participants into their respective stakeholder groups (patient representatives, HCPs, payors). Participants proposed and discussed CTA based on what they must do to address the statements presented. Then each stakeholder group presented their ideas to all the CC members so they could be discussed. Participants who were unable to attend were provided with a workmat containing an example CTA to complete and return via email to ensure their ideas were captured. Following the meeting, overarching CTA that all stakeholders could play a part in addressing were generated and agreed by the CC members (Fig. 1).
Results
Shared Area of Focus
The stakeholder leads workshop identified a shared area of focus requiring improvement in PsA management which informed the rest of the programme—patient empowerment through education on the disease and treatment options available, to enable patient involvement in management. See supplementary materials (Table S2) for more information.
Participants
Participants of the PsA CC were recruited on the basis of their expertise and experience in PsA (Fig. 1; Table S1).
Themes and Narratives
Following the Delphi process, four key themes emerged that the consensus statements could be divided into.
1. Patient Empowerment
Discussion Points
Consensus was reached on 23 statements relating to patient empowerment (Table S3). One of these statements was also used in the “patient knowledge and sources of education” narrative. Stakeholders aligned on the following definition of patient empowerment: patient empowerment is the process by which people are supported to gain sufficient knowledge, to enable them to be as actively involved as they want to be in making decisions that shape their health.
Stakeholders agreed that the level of empowerment is currently low to moderate among patients with PsA with scope for improvement, but added that there is large inter-patient variation, with some patients being very active in managing their condition. Improvements in patient empowerment could affect HCP–patient communications and treatment decisions, and ultimately lead to more ambitious treatment goals and better outcomes. However, it was also observed that patients with low empowerment may have unrealistically high expectations of treatment.
To achieve improved patient empowerment, patient education through high-quality educational materials is needed, as well as improved communication between payors, patients, and HCPs (Table 1). All stakeholders agreed that policy makers have a role in improving care. Stakeholders did not reach consensus when it came to the statement, “patient organisations should provide high-quality educational materials to HCPs” with some of those who disagreed arguing that, conversely, it should be HCPs educating patient organisations. Table 2 contains the overarching CTA and associated stakeholder-specific discussions for the theme of patient empowerment. Overarching CTA were derived from the CTA specific for each stakeholder group (Tables S4–S6) which were inspired by the consensus statements marked with a superscript dagger symbol in Table 1 and generated at the CC meeting.
2. Patient Knowledge and Sources of Education
Discussion Points
Nineteen statements relating to patient knowledge and sources of education reached consensus (Table S7). The statement “patients with PsA are already sufficiently knowledgeable about their disease” did not reach consensus with some who disagreed describing patient knowledge as “low” or “basic”. However, stakeholders agreed that patients should be given the opportunity, educational materials, and encouragement to learn about their disease and treatment options. Open-ended questions revealed that stakeholders felt patients need to have a more holistic understanding of their PsA including self-management options, psychosocial influences, oral health, comorbidities, menopause, family planning and treatment options at different life stages.
Consensus was not reached on the statement that the internet is the main source of low-quality educational resources about PsA for patients; however, a refined statement that “the internet is a source of both high- and low-quality education about PsA and the available treatment options” did achieve consensus. Despite the perception that information on the internet was of variable quality, almost all stakeholders said this is where patients get disease information from. When asked about the characteristics of high-quality educational materials, stakeholders cited the following: up-to-date information; open access, includes the patient perspective; includes imagery; is available in different formats and in a patient’s native language; uses accessible language; and is endorsed by a scientific organisation. Stakeholders agreed that HCPs are key to providing high-quality education to patients with PsA, but this is challenged by a lack of time during consultations; as a compromise, patient organisations were identified as playing a valuable role in directing patients to high-quality material.
The knowledge and sources of education narrative highlighted suboptimal patient knowledge of PsA (Table 3). There was consensus that patients must be sufficiently knowledgeable about their disease and available interventions to be included in making treatment decisions. Feedback from those who disagreed suggested that a great deal of knowledge was not necessary, although poorer decisions are likely to be made by less knowledgeable patients. To achieve a sufficient level of knowledge, patients need support to identify easily accessible, high-quality, neutral information on all aspects of PsA. Table 4 contains the overarching CTA and associated stakeholder-specific discussions for the theme of patient knowledge and sources of education. See Tables S8–S10 in the supplementary materials for the CTA per stakeholder.
3. Patient–HCP Consultations
Discussion Points
Consensus was achieved on 18 statements relating to patient–HCP consultations (Table S11). The statement “HCPs recognise the full burden of PsA on patients” did not reach consensus; however, all stakeholders agreed that HCPs should ask questions to establish the full burden of PsA on all aspects of the patient’s life, rather than relying on the patient to proactively volunteer information. The statement that “patients with PsA are always routinely involved in treatment decisions” was very far from reaching consensus—involvement varies greatly between clinics and traditional, paternalistic HCP–patient relationships often remain. Therefore, the statement was refined to “many patients are not aware that they have an option to be involved in treatment decisions”, achieving almost complete agreement (92%).
Stakeholders did not reach consensus on who should have the final say on treatment decisions (the patient or physician). Discussion centred around the need for a trusting relationship and good communication, which led to 100% agreement that in the event of a disagreement on a treatment decision, “efforts should be made to reach a shared decision through further discussion”.
The patient–HCP consultations statements that were used to form the narrative (Table 5) indicated that improvements in patient–HCP consultations would require improved communication from HCPs and individualised treatment based on shared decision-making (SDM). All stakeholders agreed that patients should be educated on what they are entitled to in terms of their level of involvement in treatment decisions. It was agreed that HCPs need support to enable them to communicate effectively with patients about the full burden of their PsA. Table 6 contains the overarching CTA and associated stakeholder-specific discussions for the theme of patient–HCP consultations. See Tables S12–S14 in the supplementary materials for the CTA per stakeholder.
4. Optimal Initial Treatment
Discussion Points
Nine consensus statements relating to optimal initial treatment reached consensus (Table S15). Stakeholders reached consensus that currently payors prioritise cost considerations of PsA treatments across the population over individual patient outcomes; often guidelines dictate that drugs must be tried in a particular order in all patients, meaning those who physicians consider ideal for biologics must try and fail on other medications first (Table 7). However, feedback revealed that in Germany the physician is free to choose a treatment for a specific patient provided it is within the approved indication and it is the most economical option (e.g. a biosimilar before a reference biologic if it is less expensive). Stakeholders agreed that prioritising cost considerations over optimal initial treatment for patients with PsA can negatively affect treatment decisions and lead to poor patient outcomes. However, the need for healthcare systems to consider costs because of limited budgets was acknowledged.
In an open-ended question, one participant cited cost as the main barrier preventing patients from accessing optimal treatment initially; conversely another reported that optimal initial treatment is not costly—highlighting the need for health economic data to provide evidence for the most cost-effective treatment. Table 8 contains the overarching CTA and associated stakeholder-specific discussions for the theme of optimal initial treatment. See Tables S16–S17 in the supplementary materials for the CTA per stakeholder.
Discussion
The Rheumacensus programme is unique in that it is a multistakeholder, pan-European initiative to identify challenges in the current management of PsA from the perspectives of three key stakeholders: patients, HCPs, and payors. By reaching consensus on the current situation, identifying potential improvements, and proposing CTA, Rheumacensus provides a framework to drive key stakeholders to elevate the SoC and treatment ambition for patients with PsA.
The initial stakeholder leads workshop provided real-world insights into the unmet needs in PsA management, identifying the shared area of focus for the programme, which informed the modified Delphi process: patient empowerment through education on the disease and treatment options available, to enable patient involvement in management.
Grouping consensus statements into four key themes allowed for the construction of narratives which help to provide a summary of the current management gaps and the desired state/action. The themes underpin the main area of focus—patient empowerment, patient education and sources of information, patient–HCP consultations, and optimal initial treatment. They are interconnected and overlapping, with statements relating to the need to improve knowledge of the disease and treatment options, and the need for individualised treatment choices appearing in multiple narratives.
The resulting CTA summarised in Table 9, inspired by key consensus statements that described the desired state/action, are designed to drive key stakeholders to elevate the SoC for patients. They cover the need for patients to be empowered and educated through the correct support and appropriate materials; and highlight the importance of individualised treatment and SDM. Ultimately, findings underscore the need for effective communication and education across all stakeholders to improve patient care.
The benefits of patient empowerment and involvement in care are widely recognised, and SDM is actively recommended by the European Alliance of Associations for Rheumatology guidelines for the management of PsA [10]. When patients are empowered and knowledgeable about their disease, the treatments available to them and their role in their care, they can participate in informed decisions [18]. Effective communication between the HCP and patient is another key factor contributing to patient empowerment and SDM. The treatment of PsA should be individualised on the basis of the needs and goals of each patient; honest, open and clear dialogue between the patient and HCP is essential to align on treatment goals and personal values, set expectations and agree on a treatment decision [4]. Patients who participate in their treatment decisions report higher levels of satisfaction with their care; have more realistic expectations about benefits and harms of treatments; are more likely to adhere to monitoring and treatment plans and can have improved health outcomes [19].
The overarching CTA for each theme highlights what is required to bridge the gap between the current and desired state/action in PsA (Table 9), while the stakeholder-specific CTA (see supplementary materials) provide stakeholders with implementable actions in their role that could contribute towards achieving the overarching CTA. Many of the overarching CTA touch on different aspects of patient empowerment. Therefore, implementing one CTA may synergistically influence CTA for another theme. The CTA are broad-ranging, and some are readily actionable. For example, HCPs can attempt to better understand the patient’s lived experience during consultations and can begin to further involve patients in SDM with minimal investment of time and money. Progress is already being made in this area, as the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) and a member of the Rheumacensus CC recognise the importance of facilitating effective consultations between HCPs and patients to ensure a shared management approach to care and are currently driving an educational initiative to address these factors [20]. Other CTA will take longer and be more costly and difficult to implement as they involve changes to systems and processes, and the development of new educational materials.
Rheumacensus has provided additional insights into the unmet needs in PsA. A report from the GRAPPA 2016 annual meeting identified ten key challenges throughout the PsA patient journey [8], which previously inspired a separate initiative [17], and care was taken not to duplicate this work. Like Rheumacensus, this previous initiative had the overall objective of improving patient care, but focussed on four key areas aligned to the ten unmet needs identified by GRAPPA: reducing time to diagnosis, improving multidisciplinary collaboration, optimising disease management, and improving disease monitoring [17]. Similarly, action points were proposed in a review paper outlining prospects for the future in PsA [21], some of which overlap with the Rheumacensus CTA. For example, the authors call for a range of methods to be harnessed to communicate disease education, and for novel tools to be developed for the assessment of patient outcomes. The Rheumacensus programme differs from these existing initiatives with a patient-centric emphasis reflected in the shared area of focus (patient empowerment) which was decided at the outset, as well as the inclusion of patient representatives. It also provides actions for payors generated by payors themselves, reflecting its multidisciplinary nature. Furthermore, Rheumacensus identified shared challenges in PsA care across eight European countries, whereas the GRAPPA report gathered insights from seven centres around the world (USA, Canada, Germany, Argentina, UK, South Africa, and Hong Kong) [8]. While Rheumacensus had a more focussed geography, the CTA are widely applicable owing to some similarities in healthcare systems across Europe, which may differ greatly across continents.
One of the main strengths of Rheumacensus is the inclusion of three key stakeholder groups involved in the front-line management of PsA: patients, HCPs, and payors, representing eight countries across Europe—setting the programme apart from others in PsA. Generating agreement across multiple stakeholder types might increase the chances of creating initiatives that all stakeholders find helpful, potentially increasing their chance of success. On the other hand, representation was limited to 12 stakeholders representing eight countries and this may have introduced some bias into the recommendations. Other limitations of Rheumacensus include the subjective grouping of consensus statements and CTA, although this was necessary to provide narrative summaries of the current and desired states for all aspects explored in the Delphi process. Furthermore, statements that were omitted often informed implementation and will therefore be considered when creating initiatives aimed at addressing CTA. A further limitation was that some stakeholders were unable to attend the virtual CC meeting, so some additional insights might not have been captured. However, CTA were provided in writing post-meeting and a separate meeting was held with one lead stakeholder as requested to ensure the perspectives of all stakeholders were captured. The Delphi e-consultations were completed by stakeholders independently and the sponsor did not take an active part in the CC meeting.
Conclusion
The Rheumacensus programme has added to current understanding of the SoC for patients with PsA. It has identified key unmet needs and proposed CTA to bridge the gaps in care, largely focussed on patient empowerment. Rheumacensus has set the foundation for change, and it is hoped that all stakeholders will now take practical steps towards implementing these CTA across Europe to elevate the SoC and treatment ambition for patients with PsA.
Data Availability
All data generated or analysed during this study are included in this published article/as supplementary information files.
References
Baum EW, Schwartzman S. ALIGN PsA: advancing a multidisciplinary approach in PsA. Semin Cutan Med Surg. 2018;37(6s):S125–34.
Ogdie A, Weiss P. The epidemiology of psoriatic arthritis. Rheum Dis Clin North Am. 2015;41(4):545–68.
Gladman DD, Antoni C, Mease P, Clegg DO, Nash P. Psoriatic arthritis: epidemiology, clinical features, course, and outcome. Ann Rheum Dis. 2005;64(Suppl 2):ii14–7.
Garrido-Cumbrera M, Hillmann O, Mahapatra R, et al. Improving the management of psoriatic arthritis and axial spondyloarthritis: roundtable discussions with healthcare professionals and patients. Rheumatol Ther. 2017;4(2):219–31.
Haugeberg G, Michelsen B, Kavanaugh A. Impact of skin, musculoskeletal and psychosocial aspects on quality of life in psoriatic arthritis patients: a cross-sectional study of outpatient clinic patients in the biologic treatment era. RMD Open. 2020;6(1):e001223.
Ritchlin CT, Colbert RA, Gladman DD. Psoriatic arthritis. N Engl J Med. 2017;376(10):957–70.
Feldman SR, Zhao Y, Shi L, Tran MH, Lu J. Economic and comorbidity burden among moderate-to-severe psoriasis patients with comorbid psoriatic arthritis. Arthritis Care Res (Hoboken). 2015;67(5):708–17.
Favier G, Gladman DD, Merola JF, Armstrong AW, Boehncke WH, Helliwell PS. Benchmarking care in psoriatic arthritis—the QUANTUM report: a report from the GRAPPA 2016 annual meeting. J Rheumatol. 2017;44(5):674–8.
Betteridge N, Boehncke WH, Bundy C, Gossec L, Gratacós J, Augustin M. Promoting patient-centred care in psoriatic arthritis: a multidisciplinary European perspective on improving the patient experience. J Eur Acad Dermatol Venereol. 2016;30(4):576–85.
Gossec L, Baraliakos X, Kerschbaumer A, et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheum Dis. 2020;79(6):700–12.
Koren J, Lambert JLW, Thomsen SF, McAteer H, Fabbrocini G, Corazza V, et al. Elevating the standard of care for patients with psoriasis: “calls to action” from epicensus, a multistakeholder pan-European initiative. Dermatol Ther (Heidelb). 2023;13(1):245–68.
Luelmo J, Gratacós J, Moreno Martínez-Losa M, et al. A report of 4 years of experience of a multidisciplinary unit of psoriasis and psoriatic arthritis. Reumatol Clin. 2014;10(3):141–6.
Sacristán JA, Dilla T, Díaz-Cerezo S, Gabás-Rivera C, Aceituno S, Lizán L. Patient-physician discrepancy in the perception of immune-mediated inflammatory diseases: rheumatoid arthritis, psoriatic arthritis and psoriasis. A qualitative systematic review of the literature. PLoS One. 2020;15(6):e0234705.
Furst DE, Tran M, Sullivan E, et al. Misalignment between physicians and patient satisfaction with psoriatic arthritis disease control. Clin Rheumatol. 2017;36(9):2045–54.
Adebajo AO, Akintayo RO. Patient educational needs and challenges in psoriatic arthritis. Curr Opin Rheumatol. 2021;33(4):356–62.
van der Veen S, Evans N, Huisman M, Welch Saleeby P, Widdershoven G. Toward a paradigm shift in healthcare: using the international classification of functioning, disability and health (ICF) and the capability approach (CA) jointly in theory and practice. Disabil Rehabil. 2023:45(14):2382–89.
Helliwell PS, Favier G, Gladman DD, et al. Best-practice indicators in psoriatic disease care. J Rheumatol Suppl. 2019;95:38–45.
Aslani P. Patient empowerment and informed decision-making. Int J Pharm Pract. 2013;21(6):347–8.
Krist AH, Tong ST, Aycock RA, Longo DR. Engaging patients in decision-making and behavior change to promote prevention. Stud Health Technol Inform. 2017;240:284–302.
GRAPPA. GRAPPA Career Boost eLearning. Effective clinical communication for improved outcomes 2023. https://elearn.grappanetwork.org/.
Hackett S, Ogdie A, Coates LC. Psoriatic arthritis: prospects for the future. Therap Adv Musculosk Dis. 2022;14. https://doi.org/10.1177/1759720X2210867.
Acknowledgements
The authors would like to thank Antonella Celano (patient representative) for completing the Delphi e-consultations and Hedye van Ameijden (payor) for completing the Delphi e-consultations and providing CTA during the Rheumacensus PsA CC meeting—providing valuable insights to this programme.
Medical Writing.
Medical writing support was provided by Sophie Dent, Ogilvy Health, London, UK and funded by UCB Pharma.
Funding
The Rheumacensus programme and medical writing (including the development of the publication) were funded by UCB Pharma. The Rapid Service Fee and Open Access Fee for publication in Rheumatology and Therapy were also funded by UCB Pharma.
Author information
Authors and Affiliations
Contributions
The Delphi e-consultations were designed by Laura Harrington. Iris Verbinnen, Emilio Monte-Boquet, Detlev Parow, Fabienne Lacombe, Andrew Pothecary, Arno W.R. van Kuijk, Edita Müllerová, Andreas Pinter, Ulrike Erstling and Phillip S. Helliwell completed the Delphi e-consultations and participated in the PsA Rheumacensus CC meeting either virtually during the meeting or via email post-meeting. Andrea Tomasini (patient representative) did not complete the Delphi e-consultations but attended the CC meeting in place of Antonella Celano. All authors were fully responsible for all content and editorial decisions, were involved at all stages of manuscript development and have approved the final version.
Corresponding author
Ethics declarations
Conflict of Interest
Stakeholder leads (namely, Iris Verbinnen, Phillip S. Helliwell and Emilio Monte-Boquet) received an honorarium for their participation in the initial workshop and they and the other PsA CC members (Detlev Parow, Fabienne Lancombe, Andrew Pothecary, Arno W.R. van Kuijk, Edita Müllerová, Andreas Pinter, Ulrike Erstling and Andrea Tomasini) received an honorarium from UCB for their time to complete the Delphi e-consultations and to attend the PsA CC meeting or provide their input offline. UCB Pharma reviewed the manuscript to ensure scientific and medical clarity and accuracy only. Emilio Monte-Boquet has received grants/research support or participation in educational activities, research projects, scientific meetings (either attendance, speaking and/or delivering presentations) and advisory boards sponsored by Abbott/AbbVie, Amgen, Astellas, AstraZeneca, Baxalta, Bayer, Biogen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Chiesi, CSL Behring, Eisai, Fresenius, Galapagos, Gilead, GSK, Ipsen, Janssen, Leo Pharma, Lilly, MSD, Merck-Serono, Novartis, Pfizer, Roche, Sanofi, Shire, Takeda, Theramex, UCB and ViiV. Detlev Parow has received an honorarium for advisory boards from Boehringer-Ingelheim, Hexal and UCB. Iris Verbinnen, Ulrike Erstling, Andreas Pinter, Edita Müllerová, Fabienne Lacombe, Andrea Tomasini and Arno W.R. van Kuijk have nothing to disclose. Laura Harrington is an employee of Ogilvy Health. Phillip S. Helliwell has received speaker fees from Novartis and participated in an advisory board for Amgen. Andrew Pothecary has received honoraria for lectures and educational events from AbbVie and Galapagos, for lectures and advisory boards from UCB Pharma and for advisory boards from Vifor Pharma and Thornton & Ross Ltd. Andrew Pothecary has also previously undertaken an unpaid volunteer position as an Expert Advisor at National Rheumatoid Arthritis Society (UK).
Ethical approval
This manuscript is formed of the opinions of the authors themselves. There was no need to collect any type of patient data. Therefore, the approval of an ethics committee was not required. Consent was obtained from all participants (or stakeholders).
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Verbinnen, I., Monte-Boquet, E., Parow, D. et al. Elevating the Standard of Care for Patients with Psoriatic Arthritis: ‘Calls to Action’ from a Multistakeholder Pan-European Initiative. Rheumatol Ther 11, 795–815 (2024). https://doi.org/10.1007/s40744-024-00664-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-024-00664-3