
Abstract
Since the first outbreak of Coronavirus Disease-2019 (COVID-19) in January 2020, the medical community has been pursuing effective countermeasures. Early in the pandemic, several small clinical and in vitro studies from France and China reported on the efficacy of chloroquine (CQ) and hydroxychloroquine (HCQ) against SARS-CoV-2 infections, which generated global attention towards these decades-old antimalarials (AM) and heralded numerous studies investigating their role in treating COVID-19. Despite several observational studies early in the pandemic affirming their beneficial role in treating COVID-19, 12 clinical studies reported no mortality benefits for CQ/HCQ in COVID-19 patients. The excitement over CQ/HCQ was ultimately quenched after three large randomized clinical trials, the COALITION-I trial in Brazil, the RECOVERY trial in the United Kingdom (UK), and the SOLIDARITY trial from World Health Organization (WHO) consistently reported no beneficial effects for CQ/HCQ in hospitalized COVID-19 patients. While initial studies suggested that CQ/HCQ might have a role in treating the early phases of infection, the results from three rigorously designed studies investigating their role in non-hospitalized COVID-19 patients were equivocal and inconsistent. Here we review the major social events related to the therapeutic use of CQ/HCQ in COVID-19, and the data from selected clinical studies evaluating their efficacy in hospitalized and non-hospitalized COVID-19 patients along with the major safety concerns.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Following the initial attention given to chloroquine/hydroxychloroquine (CQ/HCQ) at the start of the COVID-19 pandemic, multiple observational studies presented data on mortality benefits and side effects of these medications. |
There is overwhelming evidence that CQ/HCQ do not have significant efficacy against SARS-CoV-2 infections. |
This paper reviews the data regarding the use of CQ/HCQ in hospitalized and non-hospitalized COVID-19 patients along with the major safety concerns. |
This information may help practitioners guide their patients as they treat them for COVID-19. |
Digital Features
This article is published with digital features, including a summary slide to facilitate understanding of the article. To view digital features for this article go to https://doi.org/10.6084/m9.figshare.14465826.
Introduction
Antimalarials (AM), including chloroquine (CQ) and hydroxychloroquine (HCQ) are some of the key medications used by rheumatologists; however, their recent notoriety with the ongoing pandemic has given practitioners pause [1]. The initial excitement for a potential treatment of coronavirus disease 2019 (COVID-19) [2, 3] was soon replaced by challenges including drug shortages [4, 5] and pushback from the medical community questioning the safety of medications [6, 7] that rheumatologists have long known to be safe.
CQ, a decades-old antimalarial agent and disease-modifying antirheumatic drug (DMARD), modulates inflammation through interference with lysosomal function, autophagy, and inhibition of Toll-like receptors (TLRs) signaling via endosome acidification [8]. Its derivative, HCQ, was found to have more potent immunomodulatory and antiviral properties as well as a better safety profile [9, 10]. Multiple in vitro studies showed the activity of CQ/HCQ against different subtypes of coronaviruses, including severe acute respiratory syndrome coronavirus (SARS-CoV-1) and Middle East respiratory syndrome coronavirus (MERS-CoV) [11, 12]. HCQ was proposed as a treatment for COVID-19 based on its in vitro SARS-CoV-2 antiviral activity [13, 14]. Subsequently, two preliminary clinical studies from China [15, 16] and France [2] reported that CQ and HCQ were associated with improved clinical outcomes and accelerated viral clearance in COVID-19 patients, which fueled further exploration into the therapeutic role of CQ/HCQ in combating COVID-19. However, following its rise to worldwide attention, the role of CQ/HCQ in COVID-19 looms in a mist of equivocal benefit and potential toxicity.
The current publication reviews the major social and political events related to AM use in COVID-19 and summarizes selected data on AM use among hospitalized and non-hospitalized COVID-19 patients.
Methods
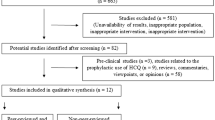
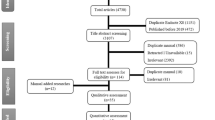
The NCBI PubMed database was searched for publications using the following search string: “(Chloroquine OR Hydroxychloroquine) AND (2019 novel Coronavirus disease OR COVID-19 OR SARS-CoV-2 OR novel Coronavirus infection OR 2019-ncov infection OR Coronavirus disease 2019 OR Coronavirus disease-19 OR 2019-ncov disease OR COV OR Coronavirus). Google was used to search for preprint publications, abstracts and relevant news items. Results were limited to January 2020 through March 2021. The search was limited to the publications written in English, Chinese, Spanish, Italian, and French, with the article type being either an observational study or a clinical trial. The eligibility criteria were as follows: (1) included ≥ 5 people infected with SARS–CoV‐2; (2) included patients with COVID-19 confirmed by either laboratory results or clinical symptoms; (3) focused on the effects of CQ/HCQ against SARS-CoV-2; (4) was published after January 1, 2020; (5) was original research; (6) had one of the following outcomes: death, ventilator-free days, escalation of care (intensive care unit transfer), length of hospital stay, symptom resolution, viral clearance; (7) had low risk of bias based on the risk of bias tools [17]. Articles that did not fulfill these inclusion criteria, did not present primary data, had insufficient data, or description of the methodology were excluded from the review. Two reviewers working independently (WT and ADA) evaluated eligibility based on review of the abstracts and titles. Disagreements regarding eligibility were resolved by consensus discussion. A limitation of the study is that databases other than NCBI PubMed were not searched. Of the 120 articles retrieved, 77 articles clearly did not address the topic of interest and were excluded. Subsequently, the remaining 43 selected articles were reviewed in full. Additional relevant publications cited in the articles collected were also examined. In total, 26 observational studies and clinical trials were ultimately included. This article is a review of previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Hydroxychloroquine in the Management of COVID-19: A Snapshot of Big Events
Gautret et al. conducted the first clinical study in 20 patients and concluded that HCQ had efficacy against SARS-CoV-2 infection [2], which attracted attention both scientifically and politically. During a press conference on March 21st, the 45th President of the United States declared that HCQ was a “game changer” for COVID-19 treatment. One week later, the Food and Drug Administration (FDA) issued an emergency authorization to allow off-label use of CQ/HCQ for the treatment of hospitalized COVID-19 patients based on “limited in vitro and anecdotal clinical data” [3]. Shortly after, the American Thoracic Society released an interim guidance on COVID-19 management and suggested the use of CQ/HCQ in hospitalized COVID-19 patients who had evidence of pneumonia on a case-by-case basis [18]. Meanwhile, the Infectious Disease Society of America (IDSA) guidance recommended the use of HCQ and azithromycin (AZ) for COVID-19 patients, preferably in clinical trial settings [19]. Safety questions regarding the use of CQ/HCQ in COVID-19 patients emerged and rapidly accumulated, specifically a growing concern for prolongation of QT interval and subsequent life-threatening cardiac arrhythmias. As a result, on April 24th, the FDA cautioned against the use of CQ/HCQ for COVID-19 outside of the hospital setting or a clinical trial due to this increased risk of arrhythmias [6]. Following the RECOVERY trial results showing no mortality benefits for HCQ in hospitalized COVID-19 patients [20], the FDA ultimately revoked the emergency use authorization of CQ/HCQ in COVID-19 on June 15th with the conclusion that “the drug is unlikely to be effective, and potential risks outweigh the benefits” [7].
On June 17th, the WHO announced termination of patient enrollment in the SOLIDARITY trial’s HCQ arm because the interim results showed that HCQ did not reduce mortality in hospitalized COVID-19 patients [21, 22]. Consequently, countries that had once recommended HCQ for COVID-19 treatment, including France, Italy, and Belgium, all moved to stop HCQ use in hospitalized patients. However, the Spanish Agency for Medicines and Health Products (AEMPS), unlike other European nations, continued to use HCQ for SARS-CoV-2 treatment, probably due to a lack of security alerts from the clinical studies underway in Spain [23]. Likewise, China continues to allow the off-label use of HCQ as an anti-viral agent in the early course of COVID-19, especially for patients who are at high risk for severe illness (Fig. 1) [24].

Snapshot of big events related to the use of HCQ in COVID-19
Hydroxychloroquine Against COVID-19: Molecular Basis
SARS-CoV-2 binds to the angiotensin-converting enzyme-2 (ACE-2) receptor on the surface to enter host cells via its spike protein, the most immunogenic part of the virus [25]. Subsequent recognition and presentation of viral antigens activate both innate and adaptive immunity and lead to release of a large amount of pro-inflammatory cytokines and chemokines, including TNF, interferon-gamma, IL-1, IL-6, IL-18, and IL-33 [26, 27]. This inflammatory process becomes exaggerated in some patients and produces a “cytokine storm” that rapidly progresses to acute respiratory distress, coagulopathy, multi-organ failure, and death [28, 29].
The potential role of CQ/HCQ against SARS-CoV-2 infection is postulated based on its anti-viral and immunomodulatory properties. The exact molecular mechanism of its antiviral activity remains unclear, but it has been proposed that CQ/HCQ interferes with the entry of SARS-CoV-2 into host cells. CQ/HCQ accumulates in lysosomes and raises the pH level of endosomes that SARS-CoV-2 utilizes for entry and exit [30]. In addition, CQ/HCQ may reduce terminal glycosylation of ACE-2 receptors, dampening effective virus-receptor binding [31]. On the other hand, the immunomodulatory property of CQ/HCQ could inhibit production of cytokines and modulate the subsequent “cytokine storm”. CQ/HCQ can raise the pH of endosomal compartments and hence inhibit the activities of lysosomes and autophagosomes that are both involved in the antigen presentation process, which eventually lead to less T and B cell activation and subsequent production of cytokines. In addition, the rise in endosomal pH also affects TLR signaling by inhibiting TLR–ligand interactions and hence further reduce cytokine formation [8].
Hydroxychloroquine Against SARS-CoV-2: In Vitro Studies
Several in vitro studies suggested potential roles for CQ/HCQ in SARS-CoV-2 infections. Wang et al. first demonstrated that CQ functioned at both entry and post-entry stages of SARS-CoV-2 infection in Vero E6 cells, an epithelial cell line used to studying viral growth, with a 90% maximal effective concentration (EC90) value of 6.9 μM, consistent with plasma levels in rheumatoid arthritis (RA) patients treated with CQ 500 mg daily [14]. Later, Liu et al. evaluated the antiviral effect of HCQ and CQ against SARS-CoV-2 infection in vitro and found that the 50% cytotoxic concentration (CC50) of HCQ (CC50 = 249.50 μM) and CQ (CC50 = 273.20 μM) were similar [10]. Yao et al. further evaluated the 50% maximal effective concentration (EC50) of both drugs in SARS-CoV-2-infected Vero cells and found that HCQ (EC50 = 0.72 μ) was lower than CQ (EC50 = 5.47 μM). Based on pharmacokinetic (PBPK) models, they suggested administration of oral HCQ for SARS-CoV-2 infection using a loading dose of 400 mg twice daily followed by a maintenance dose of 200 mg twice daily for 4 days [9].
Hydroxychloroquine in Hospitalized COVID-19 Patients
In April 2020, a small randomized clinical trial conducted in China involving 48 patients with moderate COVID-19 first reported that both CQ and HCQ shortened the time to clinical recovery (TTCR), which was defined as the number of days from randomization to clinical recovery [16]. Shortly after, another open-label non-randomized clinical trial conducted in France, albeit limited by its small sample size (a total of 36) and overall study design, concluded that HCQ treatment was associated with faster viral clearance in COVID-19 patients and this effect was increased by AZ [2]. This clinical study attracted the attention of physicians and researchers around the world and encouraged the launch of a number of observational studies, which produced inconsistent results. Four observational studies, two from Spain [32, 33], one from China [34], and one from the US [35] reported an association between administration of HCQ and lower mortality in hospitalized COVID-19 patients. However, a number of other observational studies conducted in the hospital settings reported no mortality benefit with AM use [36,37,38,39,40,41,42,43]. Many of these studies have been limited by multiple methodology issues and design flaws including lack of randomization, limited sample size, poorly defined outcomes, and multiple confounders. A systematic review and meta-analysis of antirheumatic disease therapies for the treatment of COVID-19 reviewed 14 studies for HCQ and five studies for CQ conducted before August 2020 and concluded that HCQ use was not associated with a mortality benefit in people with COVID-19 [44].
Of note, three large randomized clinical trials failed to show an association between HCQ use and decreased mortality. The RECOVERY trial in the UK announced its early closure of the HCQ arm after an interim analysis found that among patients hospitalized with COVID-19, those who received HCQ did not have lower death rates at day 28 compared to those who received standard care [20]. In addition, this trial reported that patients in the HCQ group, if not intubated at baseline, had a higher occurrence of invasive mechanical ventilation and death. The COALITION-I trial in Brazil [45], another large multicenter randomized controlled trial involving a total of 504 patients with confirmed mild-to-moderate COVID-19 disease revealed that the use of HCQ, either alone or with AZ, did not improve 15-day ordinal clinical-status outcome as compared to standard care. Moreover, QT prolongation and elevation of hepatic enzymes were more commonly reported in the HCQ-only group and in the combination therapy group as compared with the control group. More recently, the WHO released the interim results of its high-profile SOLIDARITY trial that includes a total of 1863 patients in the HCQ arm, which, similar to the two aforementioned trials, showed no difference regarding in-hospital mortality at any time in the HCQ group versus controls [risk ratio (RR) 1.19; 95% confidence interval (CI), 0.89–1.59]. A recent meta-analysis involving a total of 32,934 participants from 17 clinical studies concluded that HCQ did not decrease mortality (RR 0.83; 95% CI 0.65–1.06) while the combination of HCQ/AZ was associated with increased mortality (RR 1.27; 95% CI 1.04–1.54) [46]. Similarly, two earlier meta-analyses identified no difference in virologic cure, death, or clinical worsening of disease between COVID-19 patients treated with HCQ and standard care [47, 48].
In summary, these findings suggest that HCQ is not effective in the treatment of hospitalized COVID-19 patients. While HCQ has both anti-inflammatory and anti-viral properties against COVID-19, the weak immunomodulatory effects might be inadequate to halt progression of disease and associated cytokine storm in severely ill patients. This could explain the lack of mortality benefit in hospitalized COVID-19 patients.
Hydroxychloroquine in Non-Hospitalized COVID-19 Patients
Multiple studies have explored the role of HCQ earlier in the clinical course of COVID-19. Some observational studies have suggested benefit. For example, a recently published observational study in New Jersey (USA) reported an association between exposure to HCQ and a decreased rate of hospitalization from COVID-19 [odds ratio (OR) 0.53; 95% CI 0.29–0.95] among 1274 outpatients with documented SARS-CoV-2 infection [49]. However, randomized controlled trials have not shown benefit. A double-blind, randomized, placebo-controlled study across the USA and Canada including 423 symptomatic non-hospitalized, laboratory-confirmed COVID-19 patients failed to detect a significant change in symptom severity over 14 days between patients receiving HCQ or placebo within 5 days of symptom onset using a ten-point visual analogue scale. Of note, the trial reported more medication-adverse effects in the HCQ group versus placebo group (43% versus 22%, P < 0.001) [50]. A similar multi-center, open-label study in Catalonia enrolled and randomized 293 patients to either treatment with HCQ for 1 week or no antiviral treatment. Results showed that there was no difference between the two groups in terms of mean viral load reduction at day 3 or 7, risk of hospitalization or time to complete resolution of symptoms [51]. However, it should be pointed out that these studies enrolled younger and healthier patients with lower risk of hospitalization, which might render these trials under-powered to detect significant differences. A pre-print meta-analysis that included 5577 patients from five randomized controlled clinical trials concluded that HCQ use in outpatients reduces the incidence of the composite outcome of SARS-CoV-2 infection, hospitalization, and death, while serious adverse events were not reported and cardiac arrhythmias were rare [52].
A total of 270 clinical studies investigating the role of CQ/HCQ in COVID have been registered around the world according to the search result from the US National Library of Medicine. Among them, 54 studies were completed, 51 studies were terminated, suspended, or withdrawn, and 111 studies are active or recruiting.
Scientific and clinical enthusiasm for HCQ as a potential therapy for COVID-19 resulted in a temporary HCQ shortage early in the pandemic, which inevitably affected the population of patients with rheumatic diseases. A survey by Systemic Lupus International Collaborating Clinics (SLICC) in May 2020 showed that 55% of the clinics in different countries and continents were confronted with HCQ shortages among patients with SLE during the pandemic. The number and proportion of the patients affected corresponded to a median of 40 [interquartile range (IQR) 15–90] patients per physician representing 15% (IQR 5–35%) of their respective SLE populations [4]. As a result, the COVID-19 Global Rheumatology Alliance issued a joint statement to call on prioritizing HCQ for the treatment of lupus and other evidence-bases rationales, and to emphasize wise and conservative use of HCQ for COVID-19 until emergence of more reliable data, which was also supported by Lupus Foundation of America (LFA) [5].
Hydroxychloroquine: Safety Concerns in COVID-19 Patients
Cardiotoxicity is the most serious concern in patients treated with CQ/HCQ, including conduction defects such as bundle branch block and atrioventricular heart block [53], cardiomyopathy resulting in heart failure, and sudden cardiac arrest [54]. Its use has also been associated with QTc prolongation that potentiates fatal arrhythmias such as torsades de pointes and ventricular arrhythmias. The mechanism underlying the QTc prolongation is the blockade of a voltage-gated potassium channel central to the delayed rectifier potassium current (IKr) that lengthens ventricular repolarization [55]. The incidence of these cardio-toxic effects in CQ/HCQ users pre-COVID is exceedingly rare and there is no indication for surveillance or monitoring in patients treated with CQ/HCQ for rheumatological indications.
The risks of cardiotoxicity from CQ/HCQ might be amplified in COVID-19 patients for several reasons. First of all, severe cardiovascular complications, including arrhythmias, acute cardiac injury, and shock have been frequently described in COVID-19 patients. A case series in Wuhan, China, describing clinical characteristics of 138 hospitalized COVID-19 patients reported arrhythmia (16.7%), acute cardiac injury (7.2%), and shock (8.7%) as common cardiovascular complications [56]. Another case series of 21 severely ill patients in the USA reported that seven patients (33%) developed cardiomyopathy [57]. Furthermore, other risk factors for cardiovascular events were prevalent in COVID-19 patients, including elevated interleukin-6 levels [58], co-administration of other QT-prolonging drugs (e.g., AZ) [36], and electrolyte imbalance such as hypokalemia [59].
Concerns about cardiotoxicity among patients with COVID-19 receiving CQ/HCQ emerged early in the pandemic. An analysis of a large multinational registry of COVID-19 patients treated with CQ/HCQ reported increased frequency of ventricular arrhythmias and received substantial coverage in the lay press, but the publication was subsequently retracted due to concerns about the authenticity of the data [60, 61]. A small study of high- (600 mg twice daily for 10 days) versus low-dose (450 mg twice on day 1 and once daily for 4 days) CQ among hospitalized patients with COVID-19 was stopped early based on greater QTc prolongation (instance of QTc greater than 500 ms, 18.9% versus 11.1%) and higher mortality (mortality through day 13, 39.0% versus 15.0%) among patients in the high-dose group, and other small studies raised similar concerns regarding QTc prolongation [45, 62]. However, the SOLIDARITY and RECOVERY trials did not suggest significant cardiotoxicity associated with HCQ [20, 63].
A recent study involving two prospective rheumatoid arthritis (RA) cohorts (n = 307) and one retrospective SLE cohort (n = 374) demonstrated that QTc length did not significantly differ in HCQ users compared to non-HCQ users even after adjusting for potential clinical confounders (e.g., age, sex, race, disease activity, concurrent medication use), and HCQ was not a significant predictor of prolonged QTc > 440 ms or > 500 ms. Moreover, QTc > 500 ms was not associated with arrhythmias or deaths in SLE. The study also reported that use of HCQ combined with QTc-prolonging medication was associated with a comparable QTc length compared to HCQ alone (434 ms versus 433 ms) [64]. These results from RA and SLE patients challenges the concern that HCQ use induces QTc prolongation and predisposes recipients to arrhythmias among rheumatic disease patients.
Conclusions
CQ/HCQ have gained significant scientific and political attention as several in vitro experiments and small clinical studies reported their efficacy against SARS-CoV-2 infection early in the beginning of the pandemic. However, the overwhelming evidence from large epidemiological studies and clinical trials is that CQ/HCQ do not have significant mortality benefits in hospitalized COVID-19 patients. Studies investigating their role in the early phases of infection are equivocal and inconsistent, and thus unable to support benefits for outpatients with COVID-19. In addition, cardiotoxicity, especially the prolongation of QTc, raised the major concerns.
Rheumatologists on the front lines in the fight against COVID-19 embraced the re-purposing of antimalarials and were disappointed in the lack of efficacy noted across studies. Of course, dose, timing, serum concentrations, and treatment duration all are important in the evaluation of efficacy of AMs and some of the studies did not account for these critical issues. Although highly effective vaccines have been developed, there continue to be limitations in vaccine availability and the emergence of SARS-CoV-2 variants. Therefore, effective treatments for COVID-19 remain essential. We can only hope that CQ and HCQ will be returned to their rightful and dignified place in the care of rheumatology patients, where their efficacy and safety are above all controversy.
References
Kim AHJ, Sparks JA, Liew JW, Putman MS, Berenbaum F, Duarte-Garcia A, et al. A rush to judgment? Rapid reporting and dissemination of results and its consequences regarding the use of hydroxychloroquine for COVID-19. Ann Intern Med. 2020;172(12):819–21.
Gautret P, Lagier JC, Parola P, Hoang VT, Meddeb L, Mailhe M, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int J Antimicrob Agents. 2020;56(1):105949.
Hinton DM. Food and Drug Administration: Emergency Use Authorization For Use of Chloroquine Phosphate or Hydroxychloroquine Sulfate Supplied From the Strategic National Stockpile for Treatment of 2019 Coronavirus Disease 2020. https://www.fda.gov/media/136534/download. Accessed 2 Mar 2021.
Mendel A, Bernatsky S, Askanase A, Bae SC, Clarke AE, Costedoat-Chalumeau N, et al. Hydroxychloroquine shortages among patients with systemic lupus erythematosus during the COVID-19 pandemic: experience of the Systemic Lupus International Collaborating Clinics. Ann Rheum Dis. 2021;80(2):1–2.
Lupus Foundation of America (LFA). Global Experts Agree: Hydroxychloroquine (Plaquenil) Must Be Protected for People with Lupus 2020. https://www.lupus.org/news/global-experts-agree-hydroxychloroquine-plaquenil-must-be-protected-for-people-with-lupus. Accessed 2 Mar 2021.
FDA. FDA cautions against use of hydroxychloroquine or chloroquine for COVID-19 outside of the hospital setting or a clinical trial due to risk of heart rhythm problems 2020. https://www.fda.gov/drugs/drug-safety-and-availability/fda-cautions-against-use-hydroxychloroquine-or-chloroquine-covid-19-outside-hospital-setting-or. Accessed 2 Mar 2021.
FDA. Coronavirus (COVID-19) Update: FDA Revokes Emergency Use Authorization for Chloroquine and Hydroxychloroquine 2020. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-chloroquine-and. Accessed 2 Mar 2021.
Schrezenmeier E, Dorner T. Mechanisms of action of hydroxychloroquine and chloroquine: implications for rheumatology. Nat Rev Rheumatol. 2020;16(3):155–66.
Yao X, Ye F, Zhang M, Cui C, Huang B, Niu P, et al. In vitro antiviral activity and projection of optimized dosing design of hydroxychloroquine for the treatment of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Clin Infect Dis. 2020;71(15):732–9.
Liu J, Cao R, Xu M, Wang X, Zhang H, Hu H, et al. Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell Discov. 2020;6:16.
Keyaerts E, Vijgen L, Maes P, Neyts J, Van Ranst M. In vitro inhibition of severe acute respiratory syndrome coronavirus by chloroquine. Biochem Biophys Res Commun. 2004;323(1):264–8.
de Wilde AH, Jochmans D, Posthuma CC, Zevenhoven-Dobbe JC, van Nieuwkoop S, Bestebroer TM, et al. Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture. Antimicrob Agents Chemother. 2014;58(8):4875–84.
Andreani J, Le Bideau M, Duflot I, Jardot P, Rolland C, Boxberger M, et al. In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect. Microb Pathog. 2020;145:104228.
Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020;30(3):269–71.
Gao J, Tian Z, Yang X. Breakthrough: chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci Trends. 2020;14(1):72–3.
Chen Z, Hu J, Zhang Z, Jiang S, Han S, Yan D, et al. Efficacy of hydroxychloroquine in patients with COVID-19: results of a randomized clinical trial. medRxiv. 2020.
Sterne JAC, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
Wilson KC, Chotirmall SH, Bai C, Rello J. COVID‐19: Interim Guidance on Management Pending Empirical Evidence. From an American Thoracic Society‐led International Task Force 2020. https://www.thoracic.org/covid/covid-19-guidance.pdf. Accessed 2 Mar 2021.
Bhimraj A, Morgan RL, Shumaker AH, Lavergne V, Baden L, Cheng VC, et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin Infect Dis. 2020; ciaa478.
Group RC, Horby P, Mafham M, Linsell L, Bell JL, Staplin N, et al. Effect of hydroxychloroquine in hospitalized patients with COVID-19. N Engl J Med. 2020;383(21):2030–40.
WHO. WHO Director-General's opening remarks at the media briefing on COVID-19–25 May 2020 2020. https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---25-may-2020. Accessed 2 Mar 2021.
WHO. WHO discontinues hydroxychloroquine and lopinavir/ritonavir treatment arms for COVID-19 2020. https://www.who.int/news/item/04-07-2020-who-discontinues-hydroxychloroquine-and-lopinavir-ritonavir-treatment-arms-for-covid-19. Accessed 2 Mar 2021.
Pais E. Spain will continue to use hydroxychloroquine against the coronavirus despite the French ban and the doubts of the WHO 2020. https://elpais.com/sociedad/2020-05-27/sanidad-apuesta-por-seguir-usando-e-investigando-la-hidroxicloroquina-frente-al-coronavirus.html. Accessed 2 Mar 2021.
National Health Commission of the People’s Republic of China. COVID-19 Treatment Guideline, the 8th Edition 2020. http://www.nhc.gov.cn/yzygj/s7653p/202008/0a7bdf12bd4b46e5bd28ca7f9a7f5e5a/files/a449a3e2e2c94d9a856d5faea2ff0f94.pdf. Accessed 2 Mar 2021.
Shang J, Wan Y, Luo C, Ye G, Geng Q, Auerbach A, et al. Cell entry mechanisms of SARS-CoV-2. Proc Natl Acad Sci USA. 2020;117(21):11727–34.
Channappanavar R, Perlman S. Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. Semin Immunopathol. 2017;39(5):529–39.
Teijaro JR. Cytokine storms in infectious diseases. Semin Immunopathol. 2017;39(5):501–3.
Sarzi-Puttini P, Giorgi V, Sirotti S, Marotto D, Ardizzone S, Rizzardini G, et al. COVID-19, cytokines and immunosuppression: what can we learn from severe acute respiratory syndrome? Clin Exp Rheumatol. 2020;38(2):337–42.
Li X, Geng M, Peng Y, Meng L, Lu S. Molecular immune pathogenesis and diagnosis of COVID-19. J Pharm Anal. 2020;10(2):102–8.
Yang ZY, Huang Y, Ganesh L, Leung K, Kong WP, Schwartz O, et al. pH-dependent entry of severe acute respiratory syndrome coronavirus is mediated by the spike glycoprotein and enhanced by dendritic cell transfer through DC-SIGN. J Virol. 2004;78(11):5642–50.
Vincent MJ, Bergeron E, Benjannet S, Erickson BR, Rollin PE, Ksiazek TG, et al. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol J. 2005;2:69.
Ayerbe L, Risco-Risco C, Ayis S. The association of treatment with hydroxychloroquine and hospital mortality in COVID-19 patients. Intern Emerg Med. 2020;15(8):1501–6.
Membrillo FJ, Ramírez-Olivencia G, Estébanez M, de Dios B, Herrero MD, Mata T, et al. Early hydroxychloroquine is associated with an increase of survival in COVID-19 patients: an observational study. Preprints. 2020.
Yu B, Li C, Chen P, Zhou N, Wang L, Li J, et al. Low dose of hydroxychloroquine reduces fatality of critically ill patients with COVID-19. Sci China Life Sci. 2020;63(10):1515–21.
Arshad S, Kilgore P, Chaudhry ZS, Jacobsen G, Wang DD, Huitsing K, et al. Treatment with hydroxychloroquine, azithromycin, and combination in patients hospitalized with COVID-19. Int J Infect Dis. 2020;97:396–403.
Rosenberg ES, Dufort EM, Udo T, Wilberschied LA, Kumar J, Tesoriero J, et al. Association of treatment with hydroxychloroquine or azithromycin with in-hospital mortality in patients with COVID-19 in New York State. JAMA. 2020;323(24):2493–502.
Ip A, Berry DA, Hansen E, Goy AH, Pecora AL, Sinclaire BA, et al. Hydroxychloroquine and tocilizumab therapy in COVID-19 patients—an observational study. PLoS ONE. 2020;15(8):e0237693.
Magagnoli J, Narendran S, Pereira F, Cummings TH, Hardin JW, Sutton SS, et al. Outcomes of hydroxychloroquine usage in united states veterans hospitalized with COVID-19. Med (NY). 2020;1(1):114–27 (e3).
Paccoud O, Tubach F, Baptiste A, Bleibtreu A, Hajage D, Monsel G, et al. Compassionate use of hydroxychloroquine in clinical practice for patients with mild to severe COVID-19 in a French university hospital. Clin Infect Dis. 2020; ciaa791.
Sbidian E, Josse J, Lemaitre G, Meyer I, Bernaux M, Gramfort A, et al. Hydroxychloroquine with or without azithromycin and in-hospital mortality or discharge in patients hospitalized for COVID-19 infection: a cohort study of 4642 in-patients in France. medRxiv. 2020.
Molina JM, Delaugerre C, Le Goff J, Mela-Lima B, Ponscarme D, Goldwirt L, et al. No evidence of rapid antiviral clearance or clinical benefit with the combination of hydroxychloroquine and azithromycin in patients with severe COVID-19 infection. Med Mal Infect. 2020;50(4):384.
Tang W, Cao Z, Han M, Wang Z, Chen J, Sun W, et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: open label, randomised controlled trial. BMJ. 2020;369:m1849.
Geleris J, Sun Y, Platt J, Zucker J, Baldwin M, Hripcsak G, et al. Observational study of hydroxychloroquine in hospitalized patients with COVID-19. N Engl J Med. 2020;382(25):2411–8.
Putman M, Chock YPE, Tam H, Kim AHJ, Sattui SE, Berenbaum F, et al. Antirheumatic disease therapies for the treatment of COVID-19: a systematic review and meta-analysis. Arthritis Rheumatol. 2020;73:36–47.
Cavalcanti AB, Zampieri FG, Rosa RG, Azevedo LCP, Veiga VC, Avezum A, et al. Hydroxychloroquine with or without azithromycin in mild-to-moderate COVID-19. N Engl J Med. 2020;383(21):2041–52.
Fiolet T, Guihur A, Rebeaud ME, Mulot M, Peiffer-Smadja N, Mahamat-Saleh Y. Effect of hydroxychloroquine with or without azithromycin on the mortality of coronavirus disease 2019 (COVID-19) patients: a systematic review and meta-analysis. Clin Microbiol Infect. 2021;27(1):19–27.
Singh AK, Singh A, Singh R, Misra A. Hydroxychloroquine in patients with COVID-19: a systematic review and meta-analysis. Diabetes Metab Syndr. 2020;14(4):589–96.
Sarma P, Kaur H, Kumar H, Mahendru D, Avti P, Bhattacharyya A, et al. Virological and clinical cure in COVID-19 patients treated with hydroxychloroquine: a systematic review and meta-analysis. J Med Virol. 2020;92(7):776–85.
Ip A, Ahn J, Zhou Y, Goy AH, Hansen E, Pecora AL, et al. Hydroxychloroquine in the treatment of outpatients with mildly symptomatic COVID-19: a multi-center observational study. BMC Infect Dis. 2021;21(1):72.
Skipper CP, Pastick KA, Engen NW, Bangdiwala AS, Abassi M, Lofgren SM, et al. Hydroxychloroquine in nonhospitalized adults with early COVID-19: a randomized trial. Ann Intern Med. 2020;173(8):623–31.
Mitja O, Corbacho-Monne M, Ubals M, Tebe C, Penafiel J, Tobias A, et al. Hydroxychloroquine for early treatment of adults with mild COVID-19: a randomized-controlled trial. Clin Infect Dis. 2020; ciaa1009.
Ladapo JA, McKinnon JE, McCullough PA, Risch H. Randomized controlled trials of early ambulatory hydroxychloroquine in the prevention of COVID-19 infection, hospitalization, and death: meta-analysis. medRxiv. 2020.
Piette JC, Guillevin L, Chapelon C, Wechsler B, Bletry O, Godeau P. Chloroquine cardiotoxicity. N Engl J Med. 1987;317(11):710–1.
Page RL 2nd, O’Bryant CL, Cheng D, Dow TJ, Ky B, Stein CM, et al. Drugs that may cause or exacerbate heart failure: a scientific statement From the American Heart Association. Circulation. 2016;134(6):e32-69.
Traebert M, Dumotier B, Meister L, Hoffmann P, Dominguez-Estevez M, Suter W. Inhibition of hERG K+ currents by antimalarial drugs in stably transfected HEK293 cells. Eur J Pharmacol. 2004;484(1):41–8.
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan. China JAMA. 2020;323(11):1061–9.
Arentz M, Yim E, Klaff L, Lokhandwala S, Riedo FX, Chong M, et al. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State. JAMA. 2020;323(16):1612–4.
Aromolaran AS, Srivastava U, Ali A, Chahine M, Lazaro D, El-Sherif N, et al. Interleukin-6 inhibition of hERG underlies risk for acquired long QT in cardiac and systemic inflammation. PLoS ONE. 2018;13(12):e0208321.
Chen D, Li X, Song Q, Hu C, Su F, Dai J, et al. Assessment of hypokalemia and clinical characteristics in patients with coronavirus disease 2019 in Wenzhou, China. JAMA Netw Open. 2020;3(6):e2011122.
Rani S, Grover S, Mehra A, Sahoo S. Psychiatric implications of the use of hydroxychloroquine in COVID-19 patients. Indian J Pharmacol. 2020;52(3):229–31.
Mehra MR, Ruschitzka F, Patel AN. Retraction-Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis. Lancet. 2020;395(10240):1820.
Mercuro NJ, Yen CF, Shim DJ, Maher TR, McCoy CM, Zimetbaum PJ, et al. Risk of QT interval prolongation associated with use of hydroxychloroquine with or without concomitant azithromycin among hospitalized patients testing positive for Coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(9):1036–41.
Consortium WHOST, Pan H, Peto R, Henao-Restrepo AM, Preziosi MP, Sathiyamoorthy V, et al. Repurposed antiviral drugs for COVID-19-Interim WHO solidarity trial results. N Engl J Med. 2021;384(6):497–511.
Park E, Giles J, Perez-Recio T, Pina P, Depender C, Bathon J, et al. Hydroxychloroquine use was not associated with QTc length in a large cohort of SLE and RA patients [abstract]. Arthritis Rheumatol. vol 72, 2020.
Acknowledgements
Funding
The study and the journal’s Rapid Service Fee for this article were funded by the authors.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Authors’ Contributions
Wei Tang MD, Leila Khalili FNP, and Anca Askanase MD contributed to the concept and design of the manuscript. Wei Tang MD, Leila Khalili FNP, Cathy Guo, and Tommy Chen contributed to the data collection and statistical analysis of the manuscript. Wei Tang MD, Anca Askanase MD, Jon Giles MD, Yevgeniya Gartshteyn MD, Teja Kapoor MD, and Deborah Theodore MD contributed to the drafting of the manuscript.
Disclosures
Wei Tang MD, Leila Khalili FNP, Jon Giles MD, Yevgeniya Gartshteyn MD, Teja Kapoor MD, Cathy Guo, Tommy Chen, Deborah Theodore MD, and Anca Askanase MD have nothing to disclose.
Compliance with Ethics Guidelines
This article is a review of previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Data Availability
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Tang, W., Khalili, L., Giles, J. et al. The Rise and Fall of Hydroxychloroquine with the COVID-19 Pandemic: Narrative Review of Selected Data. Rheumatol Ther 8, 681–691 (2021). https://doi.org/10.1007/s40744-021-00315-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-021-00315-x