
Abstract
Illness scripts describe the mental model used by experienced clinicians to store and recall condition-specific knowledge when making clinical decisions. Studies demonstrate that novice clinicians struggle to develop and apply strong illness scripts. We developed the Integrated Illness Script and Mechanism of Disease (IIS-MOD) map framework to address this challenge.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The term “illness script” describes the mental model by which a clinician organizes, stores, and retrieves from long-term memory key concepts and their relationships to clinical problems (i.e., diseases, conditions, or syndromes) [1]. Experienced clinicians draw from a repertoire of scripts to drive purposeful clinical data gathering, compare and contrast diagnostic hypotheses, and direct initial management decisions [2]. Scripted knowledge of each condition is organized into three main components: Enabling Conditions (predisposing epidemiologic and structural factors that influence a patient’s probability of the disease), Fault (the underlying pathophysiological insult), and Clinical Consequences (the patient’s chief concern, signs, and symptoms to which the Fault gives rise) [1, 2]. Importantly, research demonstrates that how a clinician “encapsulates” relevant information within these components facilitates or hinders accurate and efficient information retrieval during clinical decision-making [1].
The development of a holistic, organized knowledge base and a strong foundation of core illness scripts is a principal goal of health professions training. Initially, clinical learners must rely heavily on basic science understanding of core concepts and underlying pathophysiological mechanisms (e.g., the Fault) to slowly reason through clinical hypotheses and competing diagnoses. Not surprisingly, effective cognitive integration of basic and clinical science knowledge has been shown to enhance diagnostic accuracy of novice clinicians [3, 4]. However, left to their own devices’ learners will make connections, but seldom do they make the correct connections between biomedical knowledge and clinical features [3, 4]. The problem is further compounded by the difficulty basic science and clinical faculty face in “unpacking” their own deeply interconnected and encapsulated knowledge while teaching and collaborating [1].
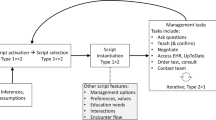
We developed the model of an Integrated Illness Script (IIS) and related Mechanism of Disease (MOD) map to address these challenges and accelerate the development and effective use of scripts by faculty and learners (Fig. 1). The IIS provides support for inductive reasoning from the observed features back through the relevant mechanisms and basic science concepts to the originating insult. The MOD map, on the other hand, provides a holistic and deductive visual representation of the clinical path: from the original insult, through the causal mechanisms and their corresponding concepts, to the resulting clinical features seen at presentation. The Overview section of the IIS provides a brief clinical definition, a description of the initiating pathophysiological insult, and a concise summary of the most salient basic science concepts impacted by the underlying disease. The Epidemiology section describes risk factors and their underlying mechanisms, highlighting pathology and genetics concepts. The Key Clinical Features articulate the most common presenting clinical findings as well as the basic science causal mechanisms that explain why each feature occurs in the condition. Links to core basic science concepts underlying the mechanisms are included (www.aquifersciences.org). The MOD map flows consistent with the manner a basic scientist would explain the occurrence of a given feature in a known disease and provides an integrated scientific view of the condition. In each section, annotated references are provided to supply supporting evidence for emerging and cutting-edge concepts and mechanisms.

Integrated Illness Script (IIS) and Mechanism of Disease (MOD) map for asthma
The structure of the IIS-MOD map was created through an iterative multidisciplinary and multi-institutional consensus process of leading clinical and basic science educators and validated through multiple national workshops over a 3-year period. The design was advanced by six nationally selected pilot schools with teams of basic science and clinical educators and senior medical students working in rapid cycle prototypes to create content for fifty exemplar IIS-MOD maps. To date, six medical schools are utilizing the IIS and MOD map models as pedagogical tools to educate learners at all levels.
For novice learners, the IIS and MOD map can provide a cognitively integrated framework with which to develop, apply, and elaborate basic science knowledge in a manner that supports emerging clinical decision-making skills. For experienced basic science and clinical faculty, the IIS and MOD map facilitate the difficult task of “unpacking” and making transparent deeply encapsulated knowledge to learners and collaborating colleagues. Importantly, the development and use of the IIS have enabled more effective collaborative instructional design and teaching between scientists and clinicians, and between scientists across disciplines. We believe the use of IIS-MOD maps has the potential to enhance curriculum development, teaching, and learning and to advance the value and safety of patient care by both novice and experienced clinicians.
References
Schmidt HG, Boshuizen HPA. On acquiring expertise in medicine. Educ Psychol Rev. 1993;5(3):205–21.
Bowen JL. Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. 2006;355:2217–25.
Baghdady M, Carnahan H, Lan EWN, Woods NN. Integration of basic sciences and clinical sciences in oral radiology education for dental students. J Dent Educ. 2013;77(6):757–63.
Kulasegaram KM, Manzone JC, Ku C, Skye A, Wadey V, Woods NN. Cause and effect: testing a mechanism and method for the cognitive integration of basic science. Acad Med. 2015;90(11):s63–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest. Aquifer, Inc. is a federally recognized non-profit health professions education organization, and therefore, I have no commercial or financial interest to disclose. Aquifer’s courses are developed and maintained by faculty and student contributors, and in partnership with other national health professions education organizations and sustained by subscriptions. Leslie Fall, Jackie Short, and Amy Wilson-Delfosse receive salary support from Aquifer. The remaining authors receive an honorarium for their contributions.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fall, L.H., English, R., Fulton, T.B. et al. Thinking Slow More Quickly: Development of Integrated Illness Scripts to Support Cognitively Integrated Learning and Improve Clinical Decision-Making. Med.Sci.Educ. 31, 1005–1007 (2021). https://doi.org/10.1007/s40670-021-01293-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40670-021-01293-z