
Abstract
Background
Low magnesium and vitamin D levels negatively affect individuals’ health.
Aims
We aimed to investigate the association of magnesium status with grip strength and fatigue scores, and evaluate whether this association differs by vitamin D status among older participants undergoing geriatric rehabilitation.
Methods
This is a 4-week observational study of participants aged ≥ 65 years undergoing rehabilitation. The outcomes were baseline grip strength and fatigue scores, and 4-week change from baseline in grip strength and fatigue scores. The exposures were baseline magnesium tertiles and achieved magnesium tertiles at week 4. Pre-defined subgroup analyses by vitamin D status (25[OH]D < 50 nmol/l = deficient) were performed.
Results
At baseline, participants (N = 253, mean age 75.7 years, 49.4% women) in the first magnesium tertile had lower mean grip strength compared to participants in the third tertile (25.99 [95% CI 24.28–27.70] vs. 30.1 [95% CI 28.26–31.69] kg). Similar results were observed among vitamin D sufficient participants (25.54 [95% CI 22.65–28.43] kg in the first magnesium tertile vs. 30.91 [27.97–33.86] kg in the third tertile). This association was not significant among vitamin D deficient participants. At week 4, no significant associations were observed between achieved magnesium tertiles and change in grip strength, overall and by vitamin D status. For fatigue, no significant associations were observed.
Conclusions
Among older participants undergoing rehabilitation, magnesium status may be relevant for grip strength, particularly among vitamin D sufficient individuals. Magnesium status was not associated with fatigue, regardless of vitamin D status.
Study registration
Clinicaltrials.gov, NCT03422263; registered February 5, 2018.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Magnesium is an essential mineral, which is involved in numerous enzymatic reactions in the body, such as DNA, RNA and protein synthesis, cell growth and reproduction, and cellular energy production and storage [1, 2]. Specifically, magnesium is required for adenosine triphosphate (ATP) synthesis and activation and produces energy for muscle contraction and relaxation. In addition to its critical role for many bodily functions, magnesium is also involved in the regulation, synthesis, and metabolism of vitamin D [3,4,5,6]. In fact, low levels of serum magnesium have been associated with vitamin D deficiency [7,8,9,10]. Similar to magnesium, vitamin D is involved in the regulation of muscle contraction and energy metabolism [11, 12].
Hypomagnesemia affects approximately 15% of the general population [13] and 25% of hospital inpatients [14], and may contribute to reduced muscle strength. Prevalence of poor muscle strength has been estimated at 48–57% in acute stroke patients [15], 56% in hip fracture patients [16] and 20% in patients with congestive heart failure [17]. Furthermore, prevalence of fatigue in patients with various health conditions requiring rehabilitation, such as heart failure [18], cerebrovascular disease [19], and musculoskeletal conditions [20], is considerably higher compared to the general population.
Given the key role of magnesium and vitamin D in muscle energy metabolism, and the increased prevalence of poor muscle strength, fatigue and low serum magnesium levels in patients with medical conditions requiring rehabilitation, an association between these independent variables cannot be excluded. Indeed, several studies support this association for vitamin D in older adults [12, 21], however, fewer studies have examined serum magnesium levels. One cross-sectional study among 1138 community-dwelling, generally healthy older adults found that baseline magnesium levels were positively associated with hand grip strength, lower extremity strength and muscle power [22]. Fatigue has been described as a symptom of magnesium deficiency [23], however, studies on the association of magnesium status and fatigue among older adults are lacking.
In summary, to the best of knowledge, no study has assessed the association between magnesium levels and muscle strength or fatigue among older rehabilitation patients to date. Furthermore, no studies have examined whether this association is modified by vitamin D status. The aim of the present study was therefore to investigate the association of magnesium status with grip strength and fatigue scores, and to evaluate whether this association differs by vitamin D status among older participants undergoing a 4-week rehabilitation program.
Methods
Study design and population
This is a 4-week observational study using data from the PUSH (Performance Under SGLT-2-Inhibitors in Humans, NCT03422263) study. The detailed study protocol has been published [24]. The PUSH study was a 4-week, prospective, observational study among participants with or without type 2 diabetes (T2D), SGLT2i treatment-naïve and with established atherosclerotic cardiovascular disease or at high risk for cardiovascular disease. Furthermore, participants had to be community-dwelling, aged ≥ 40 years and referred to inpatient rehabilitation clinic because of cerebrovascular disease, congestive heart failure or musculoskeletal conditions. Eligible participants were divided into 3 groups: (1) participants with inadequately controlled T2D, who were newly prescribed SGLT2i treatment as part of the study; (2) participants with controlled T2D who did not require new antidiabetic medication; (3) participants without T2D and no treatment. All three study groups underwent a 4-week rehabilitation program (exercise therapy). The study was conducted at the Berner Klinik Montana, Switzerland, between January 2018 and September 2020. For the purpose of the present study, a subsample of PUSH participants aged ≥ 65 years, who were recruited between January 2018 and July 2020, were included and baseline and 4-week follow-up data were used.
The protocol of the PUSH study was approved by the Cantonal Ethical Commission of Bern, Switzerland (BASEC-ID 2017–01724). The research was carried out in accordance with the principles as outlined in the Declaration of Helsinki, and all participants gave written informed consent.
Clinical assessments
Baseline evaluation was performed within the first two days of rehabilitation admission by clinicians, certified nurses, physiotherapists or occupational therapists. The following data were collected: age, sex, body mass index (BMI), comorbidities, use of walking aids, and main reason for admission. Of these, there were three: ischemic or hemorrhagic stroke, congestive heart failure, or musculoskeletal conditions such as chronic back pain, arthritis including arthroplasty or prosthesis surgery, traumatic injuries (e.g., joint dislocations, fractures, sprains, tendon tears) or repetitive stress injuries (e.g., tendinitis). Comorbidities were assessed using the age-adjusted Charlson comorbidity index (CCI). Scoring of the questionnaire was performed by the same, single investigator at baseline and week 4 according to standard scoring rules. The total CCI score is derived by summing the assigned weights for all comorbid conditions. Higher scores indicate higher level of comorbidities and greater risk of mortality [25].
The use of supplements and medication (e.g., diuretics) was assessed and recorded by the treating physician at baseline and week 4.
Outcomes
Grip strength of the dominant hand was measured in kilograms, using a manual hydraulic dynamometer (JAMAR Hand Dynamometer®). The average of three consecutive measures was used for analysis [26,27,28]. Grip strength is a well-validated test [29, 30] and often used to characterize overall limb muscle strength, especially in older adults [31,32,33].
Subjective fatigue was assessed using the Fatigue Scale for Motor and Cognitive functions (FSMC), a 20-item questionnaire with a total of 100 points developed as a measure of cognitive and motor fatigue [34]. Higher scores indicate a higher level of fatigue. For global fatigue, the total FSMC score and for motor fatigue, the motor fatigue subscale were used. The motor fatigue subscale consists of 10 items and had a maximum score of 50 points [35].
Blood biomarkers
Fasting venous blood samples were collected from each participant at baseline and at week 4. Serum magnesium, calcium, and creatinine levels were analyzed within 2 h from sample collection at an external laboratory using Roche Diagnostics Cobas 8000 analyzer with a module (c502) for all three markers (Roche Diagnostics, Mannheim, Germany). This is a colorimetric endpoint method whereby the concentration is measured photometrically. The intra- and inter-assay coefficients of variation in the lab were 2.7% and 1.8% for magnesium. The creatinine measures were used to calculate estimated glomerular filtration rate (eGFR) using the 2012 CKD-EPI formula [36, 37].
Serum 25-hydroxy-Vitamin D (25[OH]D) levels were also analyzed within 2 h from sample collection at an external laboratory. A Roche Diagnostics Cobas 8000 analyzer with a module (e801) for 25(OH)D total assay (Roche Diagnostics, Mannheim, Germany) was used, which is a competitive electrochemiluminescence protein binding assay intended for the quantitative determination of total 25(OH)D in human serum and plasma [38]. The intra- and inter-assay coefficients of variation were 2.9% and 5.1% for vitamin D. Following the Endocrine Society clinical practice guideline, vitamin D deficiency was defined as a 25(OH)D measurement of < 50 nmol/l and vitamin D sufficiency as 25(OH)D measurement of ≥ 50 nmol/l [39].
Statistical analysis
Baseline characteristics are described overall and by tertiles of serum magnesium status at baseline. Categorical variables are presented as frequencies and percentages. Continuous variables are presented as mean and standard deviation (SD). Differences in baseline characteristics between magnesium tertiles were assessed by using χ2 test for categorical variables, and ANOVA for continuous variables.
Separate multivariable linear regression models were used to examine the association of tertiles of magnesium (tertile 1 as the reference group) with each outcome (grip strength, global fatigue scores, and motor fatigue scores) at baseline.
In the longitudinal analyses, separate multivariable linear regression models were used to examine the association of achieved tertiles of magnesium (tertile 1 as the reference group) at week 4 with change from baseline at week 4 for each outcome (grip strength, global fatigue scores, and motor fatigue scores).
All models were adjusted for the treatment group of the original PUSH study (diabetic patients with SGLT2 inhibitor treatment, diabetic patients without SGLT2 inhibitor treatment, non-diabetic patients) [24], sex [40], main reason for admission to rehabilitation (ischemic or hemorrhagic stroke, congestive heart failure or musculoskeletal conditions), and the following baseline covariates: age, BMI, CCI, vitamin D status, and walking aid. For the longitudinal analyses, models were further adjusted for duration of rehabilitation, vitamin D status at week 4, baseline magnesium tertiles, and baseline measure of the outcome.
Pre-defined subgroup analyses by vitamin D status were performed to investigate to what extent vitamin D status would impact the association between tertiles of magnesium status and the three outcomes at baseline and after 4 weeks of follow-up using the same methods and adjustments as described above.
In order to explore the potential effect modification of rehabilitation reason, we tested the interaction between magnesium tertiles and rehabilitation reason for the three different outcomes cross-sectionally and prospectively by adding the respective interaction terms in the models described above. We found no indication of effect modification by rehabilitation reason for any of the exposures and outcomes (Supplemental Table 4). Therefore, no subgroup analysis by rehabilitation reason was performed.
All analyses were carried out using SAS version 9.4 (SAS Institute, Cary, NC). Statistical significance was set at P value of < 0.05, and reported P values are 2-sided.
Results
Population characteristics
A total of 253 study participants with a mean age of 75.7 years (SD 6.3) were included, of which 125 (49.4%) were women (Table 1). Overall, mean BMI was 28.4 kg/m2 (5.7), mean CCI was 5.9 (1.4), mean 25(OH)D levels were 48.3 (20.8) nmol/l, mean estimated glomerular filtration rate (eGFR) was 74.9 (24.0) ml/min and mean ionized calcium levels were 1.3 (0.1) mmol/L. More than half of participants had vitamin D deficiency (53.4%) and 59.8% of participants used walking aids. Most participants were referred to rehabilitation due to ischemic or hemorrhagic stroke (37.6%), followed by congestive heart failure (32.8%) and musculoskeletal disorders (29.6%). Ninety (35.7%) participants had diabetes at baseline (defined as HbA1c ≥ 6.5%) and 76 (30.2%) participants took calcium supplements, 169 (66.8%) took vitamin D supplements and 116 (46%) took diuretics at baseline.
At baseline, there were no differences between magnesium tertiles in age, sex, BMI, use of walking aid, main reason for rehabilitation admission, 25(OH)D levels, and vitamin D status (Table 1). There was a statistically significant difference between magnesium tertiles for mean CCI. Participants in the first magnesium tertile had higher mean CCI than participants in the second and third tertiles (6.4, 5.7, and 5.6, respectively, P < 0.001).
Cross-sectional analysis
Association of magnesium tertiles with grip strength and fatigue scores at baseline
At baseline, magnesium tertiles were associated with grip strength (Table 2; Fig. 1), with statistically significant lower grip strength in the first magnesium tertile when compared to the second and third tertiles, even after controlling for relevant confounders (mean grip strength [95% CI]; T1: 25.99 [24.28, 27.70] kg; T2: 28.82 [27.11, 30.52] kg; T3: 29.98 [28.26, 31.69] kg).

Adjusted1 mean grip strength (95% CI) at baseline by tertiles of magnesium. 1Adjusted means are least square means (LSM) and 95% CI from multivariable linear regression models. P values are from the pairwise comparison between the tertiles with tertile 1 as the reference group. Models were adjusted for treatment group of the original PUSH study, sex, reason for admission to rehabilitation, and baseline covariates: age, BMI, Charlson comorbidity index, vitamin D status (deficiency defined as 25[OH]D < 50 nmol/l), and use of walking aids
There were no statistically significant associations between magnesium tertiles and global fatigue scores at baseline (Table 2) in the unadjusted and adjusted models. There was, however, a statistically significant association between magnesium tertiles and motor fatigue. On average, participants in the first magnesium tertile had lower fatigue scores compared to the second tertile in the unadjusted model (mean score [95% CI]; T1 27.96 [25.83, 30.09], T2: 31.00 [28.79, 33.21]). After adjusting for confounders, this association was no longer statistically significant (Table 2).
Association of magnesium with grip strength and fatigue scores according to vitamin D status at baseline
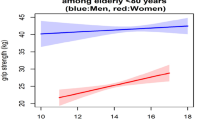
In a subgroup analysis according to participants' vitamin D status, magnesium tertiles were statistically significantly associated with grip strength among participants with vitamin D sufficiency (Fig. 2). On average, mean grip strength was lower in the first magnesium tertile compared to the third tertile (mean grip strength [95%CI]; T1 25.55 [22.65, 28.43] kg; T3: 30.91 [27.97, 33.86] kg), after controlling for potential confounders. Among participants with vitamin D deficiency, no statistically significant association was observed (Online Resource 1, Supplemental Table 5).

Adjusted1 mean grip strength (95% CI) at baseline by tertiles of magnesium according to vitamin D status. 1Adjusted means are least square means (LSM) and 95% CI from multivariable linear regression models. P values are from the pairwise comparison between the tertiles with tertile 1 as the reference group. Models were adjusted for treatment group of the original PUSH study, sex, reason for admission to rehabilitation, and baseline covariates: age, BMI, Charlson comorbidity index, and use of walking aids
There were no statistically significant differences across magnesium tertiles and global or motor fatigue at baseline (Online Resource 1, Supplemental Table 5) when stratified according to vitamin D status.
Prospective analysis
Out of the 253 participants included at baseline, 238 had serum magnesium level measurements at week 4 and were included in the prospective analyses. Participants were followed for a median time of 29 days. At week 4, mean serum magnesium levels were 0.84 (SD 0.09) mmol/L and mean serum 25(OH)D levels were 53.20 (SD 19.14) nmol/l. Overall mean change from baseline at week 4 in grip strength, fatigue scores, and motor fatigue scores were 0.54 kg, −7.19, −3.99, respectively.
Association of achieved tertiles of magnesium levels with change from baseline in grip strength and fatigue
At week 4, there was no statistically significant difference in grip strength change across achieved magnesium tertiles in the unadjusted or adjusted models (Table 3).
For global fatigue, higher achieved tertiles of magnesium were associated with greater reduction in global fatigue scores at week 4 (mean change [95% CI]; T1: −4.06 [−7.21, −0.90]; T2: −8.89 [−12.00, −5.78]; T3: −8.87 [−12.06, −5.67]). After controlling for potential confounders, this association was no longer statistically significant. Similarly, higher achieved magnesium tertiles were associated with greater reduction in motor fatigue scores at week 4 in the unadjusted model (mean change [95% CI]; T1: −2.06 [−3.74, −0.38]; T2: −5.29 [−6.95, −3.63]; T3: −4.65 [−6.34, −2.96]). After controlling for potential confounders this association was, however, no longer statistically significant (Table 3).
Association of achieved tertiles of magnesium levels with change from baseline in grip strength and fatigue according to vitamin D status
After stratifying according to vitamin D status at week 4, no significant associations were found between achieved magnesium tertiles and mean change in grip strength in the unadjusted or adjusted models (Online Resource 1, Supplemental Table 6).
Among participants with vitamin D deficiency, a significantly greater reduction in the global fatigue scores at week 4 was observed in the third achieved magnesium tertile compared to the first achieved magnesium tertile in the unadjusted model (mean change [95% CI]; T1: −2.23 [−7.13, 2.67]; T3: −10.13 [−14.95, −5.31]). No significant association was observed in the adjusted model. Likewise, participants in the higher achieved magnesium tertiles had a greater reduction in motor fatigue scores at week 4 compared to the first achieved magnesium tertile in the unadjusted model (mean change [95% CI]; T1: −0.87 [−3.45, 1.71]; T2: −4.97 [−7.43, −2.51]; T3: −4.93 [−7.52, −2.35]). However, this association was not statistically significant in the adjusted model (Online Resource 1, Supplemental Table 6, Supplemental Fig. 4).
Discussion
In the present study, we investigated the cross-sectional association of serum magnesium status with grip strength and global and motor fatigue scores and evaluated whether this association differed by vitamin D status among older adults enrolled in the PUSH study, who were undergoing rehabilitation. Furthermore, we examined the prospective association between achieved serum magnesium status and vitamin D status and the changes from baseline in grip strength and fatigue scores after 4 weeks of rehabilitation. Results showed an association between serum magnesium status and grip strength at baseline, with higher tertiles of magnesium being associated with greater grip strength, overall and in the subgroup of vitamin D sufficient participants. Prospective analyses indicated an association between higher achieved serum magnesium tertiles and greater 4-week change in global and motor fatigue, but only in the unadjusted model.
Our findings align with the results from the InCHIANTI study, which reported an association between higher serum magnesium tertiles and greater physical performance, including grip strength, among older adults (i.e., grip strength over 18 months of follow-up [β = 2.0 ± 0.5, P = 0.0002]) [22]. Participants in the InCHIANTI study (N = 1138) were community-dwelling and slightly younger (mean age 67 years), but otherwise comparable to our study population. Other previous cross-sectional studies explored the associations between dietary magnesium intake, assessed by food frequency questionnaires, and a range of functional performance measurements, including grip strength [41,42,43]. One of these studies was the Tasmanian Older Adult Cohort Study among community-dwelling adults aged 50–79 years (N = 1099) [41]. Higher magnesium intake at baseline was associated with greater appendicular lean mass (ALM) at baseline and was a positive predictor of changes in ALM over 2.6 years (β = 0.07, P = 0.02), however, no associations with knee extensor strength was detected. Similarly, in a cross-sectional study among women aged 18–79 years, highest compared to lowest magnesium intake was associated with greater amounts of fat-free mass (extreme quintile difference: 2.6%, P < 0.001; N = 2570), and higher leg extension power (24.1%, P < 0.001; N = 1914), but not with grip strength (2.5%, P = 0.348; N = 949) [42].
The observation that the association between magnesium status and grip strength persists in the subgroup of vitamin D sufficient individuals but not in those with deficiency, supports a potential interaction effect between the two nutrients [8, 44, 45]. Adequate levels of both, magnesium and vitamin D, may be needed for optimal muscle strength [46,47,48]. We are not aware of any other, similar, cross-sectional studies which support the interaction effect of magnesium and vitamin D, however, interventional studies support our observation [8]. In a study of 180 individuals (40–85 years old) at risk for colorectal cancer, individualized magnesium supplementation, based on baseline intake, increased the 25(OH)D concentration when baseline 25(OH)D concentrations were 30 ng/mL compared to placebo (mean difference from baseline = 2.79 ng/mL, 95% CI 0.25, 5.34) [8].
To the best of our knowledge, this is the first cross-sectional study which examined the association of serum magnesium status with global or motor fatigue. We detected significant positive associations between mean change in global and motor fatigue score and achieved tertiles of serum magnesium levels in the unadjusted model. A similar, but not statistically significant pattern was observed in the adjusted model, which may suggest that other clinical characteristics are also relevant to fatigue in addition to magnesium status. Cross-sectional studies on the association of serum magnesium levels and fatigue in geriatric patients are lacking, however, evidence from interventional studies in various populations at risk for fatigue support our findings. For example, magnesium supplementation reduced fatigue in women suffering from breast cancer [49] and patients suffering from chronic fatigue syndrome [50]. Furthermore, 6 months of magnesium supplementation improved energy levels compared to placebo, measured by the Nottingham Health Profile Scores, among 32 young (mean age: ~ 36 years) adults (mean difference: −46.57, 95% CI −76.16, −16.98, P = 0.002) [51].
When considering vitamin D status, the association between achieved tertiles of magnesium levels and changes in global and motor fatigue score remained significant in vitamin D deficient individuals in the adjusted models. These results are in contrast to the observations for grip strength, where the positive association was only observed in vitamin D sufficient patients, and to previous studies, which have shown a negative association between vitamin D and fatigue in older adults [52, 53]. Further prospective studies with a larger sample size are needed to investigate the association between magnesium status, vitamin D status and fatigue in older adults.
Our findings that magnesium status is associated with grip strength are of clinical relevance since poor muscle strength is a major contributing factor for disability and frailty [54]. Furthermore, the risk of becoming frail increases with the number of micronutrient deficiencies [55]. Screening for magnesium deficiency may therefore be a relevant strategy for successful rehabilitation in geriatric populations at risk of frailty and disability.
The findings on magnesium status and fatigue are less clear and further studies are required. Chronic fatigue presents an important public health problem, and is a prevalent comorbidity of various health conditions such as cancer, rheumatic disorders or, more recently, COVID-19 [56,57,58,59,60,61,62]. The assessment of fatigue can be challenging due to its subjectivity, limited standardized assessment tools, and limited knowledge of its pathophysiological pathways. These limitations can contribute to a poor understanding and appreciation of its implications for older people in clinical practice [63]. Future studies on the association of fatigue and nutrient deficiencies may help to guide health care professionals in identifying the most appropriate nutritional recommendations and interventions in the future.
Some limitations of the present study should be acknowledged. First, this was a secondary analysis including older participants from the PUSH study, which was not designed to evaluate the association of magnesium status with grip strength and fatigue. Second, this is an observational study therefore causality cannot be inferred and residual confounding may have biased our results. Third, the follow-up time of four weeks was relatively short and further studies with longer follow-up periods and larger sample sizes are thus needed. Fourth, measuring actual magnesium status and assessing magnesium deficiency is complex, mostly because magnesium is an intracellular cation. Measuring serum concentrations is the clinical standard but often does not accurately reflect magnesium status in the body [64,65,66,67]. A validated, accurate and widely available clinical test is lacking. Fifth, generalizability of the study findings may be limited to older patients undergoing rehabilitation. And last, we did not adjust the p-values for multiple testing. Therefore, statistically significant associations may have occurred by chance.
Conclusions
Among older adults undergoing rehabilitation, higher tertiles of serum magnesium was cross-sectionally associated with greater grip strength overall and in individuals with vitamin D sufficiency, but not among individuals with vitamin D deficiency. The association between magnesium status and global and motor fatigue remains unclear and longitudinal studies are required to examine the role of magnesium alone, and in combination with vitamin D in individuals at risk for fatigue.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Volpe SL (2013) Magnesium in disease prevention and overall health. Adv Nutr 4:378S-S383. https://doi.org/10.3945/an.112.003483
Institute of Medicine Standing Committee on the Scientific Evaluation of Dietary Reference I (1997) The National Academies Collection: Reports funded by National Institutes of Health. Dietary reference intakes for calcium, phosphorus, magnesium, vitamin D, and Fluoride. The National Academies Collection: reports funded by National Institutes of Health. National Academies Press (US), Washington (DC)
de Baaij JH, Hoenderop JG, Bindels RJ (2015) Magnesium in man: implications for health and disease. Physiol Rev 95:1–46. https://doi.org/10.1152/physrev.00012.2014
Glasdam SM, Glasdam S, Peters GH (2016) The importance of magnesium in the human body: a systematic literature review. Adv Clin Chem 73:169–193. https://doi.org/10.1016/bs.acc.2015.10.002
Romani AM (2011) Cellular magnesium homeostasis. Arch Biochem Biophys 512:1–23. https://doi.org/10.1016/j.abb.2011.05.010
Wolf FI, Trapani V (2008) Cell (patho)physiology of magnesium. Clin Sci (Lond) 114:27–35. https://doi.org/10.1042/CS20070129
Nielsen FH, Lukaski HC (2006) Update on the relationship between magnesium and exercise. Magnes Res 19:180–189
Dai Q, Zhu X, Manson JE et al (2018) Magnesium status and supplementation influence vitamin D status and metabolism: results from a randomized trial. Am J Clin Nutr 108:1249–1258. https://doi.org/10.1093/ajcn/nqy274
Deng X, Song Y, Manson JE et al (2013) Magnesium, vitamin D status and mortality: results from US National Health and Nutrition Examination Survey (NHANES) 2001 to 2006 and NHANES III. BMC Med 11:187. https://doi.org/10.1186/1741-7015-11-187
Uwitonze AM, Razzaque MS (2018) Role of magnesium in vitamin D activation and function. J Am Osteopath Assoc 118:181–189. https://doi.org/10.7556/jaoa.2018.037
Dzik KP, Kaczor JJ (2019) Mechanisms of vitamin D on skeletal muscle function: oxidative stress, energy metabolism and anabolic state. Eur J Appl Physiol 119:825–839. https://doi.org/10.1007/s00421-019-04104-x
McCarthy EK, Kiely M (2015) Vitamin D and muscle strength throughout the life course: a review of epidemiological and intervention studies. J Hum Nutr Diet 28:636–645. https://doi.org/10.1111/jhn.12268
Schimatschek HF, Rempis R (2001) Prevalence of hypomagnesemia in an unselected German population of 16,000 individuals. Magnes Res 14:283–290
Malinowska J, Malecka M, Ciepiela O (2020) Variations in magnesium concentration are associated with increased mortality: study in an unselected population of hospitalized patients. Nutrients. https://doi.org/10.3390/nu12061836
Simpson LA, Hayward KS, McPeake M et al (2021) Challenges of estimating accurate prevalence of arm weakness early after stroke. Neurorehabil Neural Repair 35:871–879. https://doi.org/10.1177/15459683211028240
Churilov I, Churilov L, MacIsaac RJ et al (2018) Systematic review and meta-analysis of prevalence of sarcopenia in post acute inpatient rehabilitation. Osteoporos Int 29:805–812. https://doi.org/10.1007/s00198-018-4381-4
Fülster S, Tacke M, Sandek A et al (2012) Muscle wasting in patients with chronic heart failure: results from the studies investigating co-morbidities aggravating heart failure (SICA-HF). Eur Heart J 34:512–519. https://doi.org/10.1093/eurheartj/ehs381%JEuropeanHeartJournal
Polikandrioti M, Kalafatakis F, Koutelekos I et al (2019) Fatigue in heart failure outpatients: levels, associated factors, and the impact on quality of life. Arch Med Sci Atheroscler Dis 4:e103–e112. https://doi.org/10.5114/amsad.2019.85406
Nadarajah M, Goh HT (2015) Post-stroke fatigue: a review on prevalence, correlates, measurement, and management. Top Stroke Rehabil 22:208–220. https://doi.org/10.1179/1074935714Z.0000000015
Wolfe F, Hawley DJ, Wilson K (1996) The prevalence and meaning of fatigue in rheumatic disease. J Rheumatol 23:1407–1417
Aspell N, Laird E, Healy M et al (2019) Vitamin D deficiency is associated with impaired muscle strength and physical performance in community-dwelling older adults: findings from the english longitudinal study of ageing. Clin Interv Aging 14:1751–1761. https://doi.org/10.2147/CIA.S222143
Dominguez LJ, Barbagallo M, Lauretani F et al (2006) Magnesium and muscle performance in older persons: the InCHIANTI study. Am J Clin Nutr 84:419–426. https://doi.org/10.1093/ajcn/84.1.419
Barbagallo M, Veronese N, Dominguez LJ (2021) Magnesium in aging health and diseases. Nutrients. https://doi.org/10.3390/nu13020463
Frundi DS, Kettig E, Popp LL et al (2022) Physical performance and glycemic control under SGLT-2-inhibitors in patients with type 2 diabetes and established atherosclerotic cardiovascular diseases or high cardiovascular risk (PUSH): Design of a 4-week prospective observational study. Front Cardiovasc Med 9:907385. https://doi.org/10.3389/fcvm.2022.907385
Charlson M, Szatrowski TP, Peterson J et al (1994) Validation of a combined comorbidity index. J Clin Epidemiol 47:1245–1251. https://doi.org/10.1016/0895-4356(94)90129-5
De Dobbeleer L, Beyer I, Hansen ÅM et al (2019) Grip work measurement with the jamar dynamometer: validation of a simple equation for clinical use. J Nutr Health Aging 23:221–224. https://doi.org/10.1007/s12603-019-1155-4
Hamilton GF, McDonald C, Chenier TC (1992) Measurement of grip strength: validity and reliability of the sphygmomanometer and jamar grip dynamometer. J Orthop Sports Phys Ther 16:215–219. https://doi.org/10.2519/jospt.1992.16.5.215
Mathiowetz V, Weber K, Volland G et al (1984) Reliability and validity of grip and pinch strength evaluations. J Hand Surg Am 9:222–226. https://doi.org/10.1016/s0363-5023(84)80146-x
Jakobsen LH, Rask IK, Kondrup J (2010) Validation of handgrip strength and endurance as a measure of physical function and quality of life in healthy subjects and patients. Nutrition 26:542–550. https://doi.org/10.1016/j.nut.2009.06.015
Dodds RM, Syddall HE, Cooper R et al (2016) Global variation in grip strength: a systematic review and meta-analysis of normative data. Age Ageing 45:209–216. https://doi.org/10.1093/ageing/afv192
Bohannon RW, Magasi SR, Bubela DJ et al (2012) Grip and knee extension muscle strength reflect a common construct among adults. Muscle Nerve 46:555–558. https://doi.org/10.1002/mus.23350
Kuh D, Hardy R, Blodgett JM et al (2019) Developmental factors associated with decline in grip strength from midlife to old age: a British birth cohort study. BMJ Open 9:e025755. https://doi.org/10.1136/bmjopen-2018-025755
Bohannon RW (2019) Grip strength: an indispensable biomarker for older adults. Clin Interv Aging 14:1681–1691. https://doi.org/10.2147/CIA.S194543
Penner IK, Raselli C, Stocklin M et al (2009) The fatigue scale for motor and cognitive functions (FSMC): validation of a new instrument to assess multiple sclerosis-related fatigue. Mult Scler 15:1509–1517. https://doi.org/10.1177/1352458509348519
Sehle A, Mundermann A, Starrost K et al (2011) Objective assessment of motor fatigue in multiple sclerosis using kinematic gait analysis: a pilot study. J Neuroeng Rehabil 8:59. https://doi.org/10.1186/1743-0003-8-59
Inker LA, Schmid CH, Tighiouart H et al (2012) Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med 367:20–29. https://doi.org/10.1056/NEJMoa1114248
Inker LA, Eneanya ND, Coresh J et al (2021) New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med 385:1737–1749. https://doi.org/10.1056/NEJMoa2102953
Knudsen CS, Nexo E, Hojskov CS et al (2012) Analytical validation of the roche 25-OH vitamin D total assay. Clin Chem Lab Med 50:1965–1968. https://doi.org/10.1515/cclm-2011-0964
Holick MF, Binkley NC, Bischoff-Ferrari HA et al (2011) Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 96:1911–1930. https://doi.org/10.1210/jc.2011-0385
Wang YC, Bohannon RW, Li X et al (2018) Hand-grip strength: normative reference values and equations for individuals 18 to 85 years of age residing in the United States. J Orthop Sports Phys Ther 48:685–693. https://doi.org/10.2519/jospt.2018.7851
Scott D, Blizzard L, Fell J et al (2010) Associations between dietary nutrient intake and muscle mass and strength in community-dwelling older adults: the Tasmanian older adult cohort study. J Am Geriatr Soc 58:2129–2134. https://doi.org/10.1111/j.1532-5415.2010.03147.x
Welch AA, Kelaiditi E, Jennings A et al (2016) Dietary magnesium is positively associated with skeletal muscle power and indices of muscle mass and may attenuate the association between circulating C-reactive protein and muscle mass in women. J Bone Miner Res 31:317–325. https://doi.org/10.1002/jbmr.2692
Santos DA, Matias CN, Monteiro CP et al (2011) Magnesium intake is associated with strength performance in elite basketball, handball and volleyball players. Magnes Res 24:215–219. https://doi.org/10.1684/mrh.2011.0290
Huang W, Ma X, Chen Y et al (2022) Dietary magnesium intake modifies the association between vitamin D and systolic blood pressure: results from NHANES 2007–2014. Front Nutr 9:829857. https://doi.org/10.3389/fnut.2022.829857
Rosanoff A, Dai Q, Shapses SA (2016) Essential nutrient interactions: does low or suboptimal magnesium status interact with vitamin D and/or calcium status? Adv Nutr 7:25–43. https://doi.org/10.3945/an.115.008631
Kheyruri F, Sarrafzadeh J, Hosseini AF et al (2021) Randomized study of the effects of vitamin D and magnesium co-supplementation on muscle strength and function, body composition, and inflammation in vitamin D-deficient middle-aged women. Biol Trace Elem Res 199:2523–2534. https://doi.org/10.1007/s12011-020-02387-2
Ganapathy A, Nieves JW (2020) Nutrition and sarcopenia—what do we know? Nutrients. https://doi.org/10.3390/nu12061755
Cruz-Jentoft AJ, Dawson Hughes B, Scott D et al (2020) Nutritional strategies for maintaining muscle mass and strength from middle age to later life: a narrative review. Maturitas 132:57–64. https://doi.org/10.1016/j.maturitas.2019.11.007
Park H, Parker GL, Boardman CH et al (2011) A pilot phase II trial of magnesium supplements to reduce menopausal hot flashes in breast cancer patients. Support Care Cancer 19:859–863. https://doi.org/10.1007/s00520-011-1099-7
Bjorklund G, Dadar M, Pen JJ et al (2019) Chronic fatigue syndrome (CFS): suggestions for a nutritional treatment in the therapeutic approach. Biomed Pharmacother 109:1000–1007. https://doi.org/10.1016/j.biopha.2018.10.076
Cox IM, Campbell MJ, Dowson D (1991) Red blood cell magnesium and chronic fatigue syndrome. Lancet 337:757–760. https://doi.org/10.1016/0140-6736(91)91371-z
Nowak A, Boesch L, Andres E et al (2016) Effect of vitamin D3 on self-perceived fatigue: a double-blind randomized placebo-controlled trial. Medicine 95:e5353. https://doi.org/10.1097/MD.0000000000005353
Pennisi M, Malaguarnera G, Di Bartolo G et al (2019) Decrease in serum vitamin D level of older patients with fatigue. Nutrients. https://doi.org/10.3390/nu11102531
Rantanen T, Guralnik JM, Foley D et al (1999) Midlife hand grip strength as a predictor of old age disability. JAMA 281:558–560. https://doi.org/10.1001/jama.281.6.558
Semba RD, Bartali B, Zhou J et al (2006) Low serum micronutrient concentrations predict frailty among older women living in the community. J Gerontol A Biol Sci Med Sci 61:594–599. https://doi.org/10.1093/gerona/61.6.594
Carfì A, Bernabei R, Landi F (2020) Persistent symptoms in patients after acute COVID-19. JAMA 324:603–605. https://doi.org/10.1001/jama.2020.12603
Davies K, Dures E, Ng WF (2021) Fatigue in inflammatory rheumatic diseases: current knowledge and areas for future research. Nat Rev Rheumatol 17:651–664. https://doi.org/10.1038/s41584-021-00692-1
El Sayed S, Shokry D, Gomaa SM (2021) Post-COVID-19 fatigue and anhedonia: a cross-sectional study and their correlation to post-recovery period. Neuropsychopharmacol Rep 41:50–55. https://doi.org/10.1002/npr2.12154
Mohandas H, Jaganathan SK, Mani MP et al (2017) Cancer-related fatigue treatment: an overview. J Cancer Res Ther 13:916–929. https://doi.org/10.4103/jcrt.JCRT_50_17
Liao S, Ferrell BA (2000) Fatigue in an older population. J Am Geriatr Soc 48:426–430. https://doi.org/10.1111/j.1532-5415.2000.tb04702.x
Loge JH, Ekeberg O, Kaasa S (1998) Fatigue in the general Norwegian population: normative data and associations. J Psychosom Res 45:53–65. https://doi.org/10.1016/s0022-3999(97)00291-2
Wijeratne C, Hickie I, Brodaty H (2007) The characteristics of fatigue in an older primary care sample. J Psychosom Res 62:153–158. https://doi.org/10.1016/j.jpsychores.2006.09.011
Azzolino D, Arosio B, Marzetti E et al (2020) Nutritional status as a mediator of fatigue and its underlying mechanisms in older people. Nutrients. https://doi.org/10.3390/nu12020444
Reinhart RA (1988) Magnesium metabolism. A review with special reference to the relationship between intracellular content and serum levels. Arch Intern Med 148:2415–20. https://doi.org/10.1001/archinte.148.11.2415
Saris NE, Mervaala E, Karppanen H et al (2000) Magnesium. An update on physiological, clinical and analytical aspects. Clin Chim Acta 294:1–26. https://doi.org/10.1016/s0009-8981(99)00258-2
Rude RK, Stephen A, Nadler J (1991) Determination of red blood cell intracellular free magnesium by nuclear magnetic resonance as an assessment of magnesium depletion. Magnes Trace Elem 10:117–121
Millart H, Durlach V, Durlach J (1995) Red blood cell magnesium concentrations: analytical problems and significance. Magnes Res 8:65–76
Acknowledgements
We thank the participants for their participation in and commitment to the PUSH study.
Funding
Open access funding provided by University of Zurich. The PUSH study was funded by the Berner Klinik Foundation, Bern, Switzerland. The foundation is a non-profit organization with a focus on clinical rehabilitation. External funding was neither sought nor endured from previous research projects in the institution. Partial financial support was received from the Baugarten Stiftung by the “Centre Grant for Aging Research in the Extension of Healthy Life Expectancy and the Prevention of Sarcopenia”.
Author information
Authors and Affiliations
Contributions
Conceptualization: DSF, EK; Methodology: DSF, CGRCM; Formal analysis and investigation: CGRCM, EK, MK-F; Writing—original draft preparation: EK and MK-F contributed equally as co-first authors. They performed the literature survey and the drafting of the article; Writing—review and editing: MK-F, CGRCM, HAB-F; Funding acquisition: DSF; Supervision: MK-F, CGRCM, HAB-F.
Corresponding author
Ethics declarations
Conflict of interest
Authors EK, MK-F, CDGRCM, HAB-F, DSF have no relevant financial or non-financial interests to disclose.
Statement of human and animal rights
This study was approved by the Cantonal Ethical Commission of Bern, Switzerland (BASEC-ID 2017–01724).
Informed consent
Informed consent was obtained from all participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kettig, E., Kistler-Fischbacher, M., de Godoi Rezende Costa Molino, C. et al. Association of magnesium and vitamin D status with grip strength and fatigue in older adults: a 4-week observational study of geriatric participants undergoing rehabilitation. Aging Clin Exp Res 35, 1619–1629 (2023). https://doi.org/10.1007/s40520-023-02450-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-023-02450-7